
Abstract
Leiomyosarcoma of the bone (LMSB) is a rare type of sarcoma characterized by smooth muscle differentiation arising within the bone. We present the case of a 38-year-old female patient diagnosed with LMSB in the left distal femur. Histological examination revealed spindle-shaped and pleomorphic cells, with no evidence of cartilage or bone matrix formation. Immunohistochemical analysis demonstrated the tumor cell were positive for Smooth Muscle Actin, Desmin, and H-caldesmon. The integration of clinical presentation, imaging, morphological, and immunohistochemical findings confirmed the diagnosis of high-grade leiomyosarcoma of the bone. Postoperative pathological analysis further validated this diagnosis. One year after surgery, the patient remains stable, with no signs of recurrence or metastasis. Diagnosing leiomyosarcoma of the bone is particularly challenging due to the limitations of core needle biopsy samples. However, immunohistochemical evidence of smooth muscle differentiation plays a critical role in establishing the diagnosis.
Background
Leiomyosarcoma can originate primarily in either bone or soft tissue. In bone, this type of tumor accounts for less than 0.7% of primary bone tumors and has a poor prognosis, with an overall survival rate of 35%. 1 The cause of leiomyosarcoma of the bone remains unclear. However, some hypotheses suggest that it originates from smooth muscle cells lining blood vessels, pluripotent mesenchymal stem cells in the bone, or is associated with a bone infarct.2,3
Case Report
A 38-year-old female patient presented with a solitary bone lesion in the left distal femur. Her past medical history was unremarkable. She reported mild pain in her left knee. X-ray imaging of the left femur revealed a lytic, destructive mass that had destroyed the cortex and extended into the surrounding soft tissue without appreciable mineralization (Figure 1). MRI showed a mass lesion measuring 46 × 38 × 34 mm at the lateral epicondyle of the femur, with evidence of cortical bone destruction (Figure 2). The lesion was predominantly located in the medullary cavity and extended into the soft tissue from the bone, with indistinct tumor margins. A total-body PET/CT showed no evidence of metastatic disease or other primary tumors (Figure 3). Accordingly, the clinical diagnosis suggested a malignant tumor, with differential diagnoses including osteosarcoma, chondrosarcoma, and giant cell tumor of the bone.
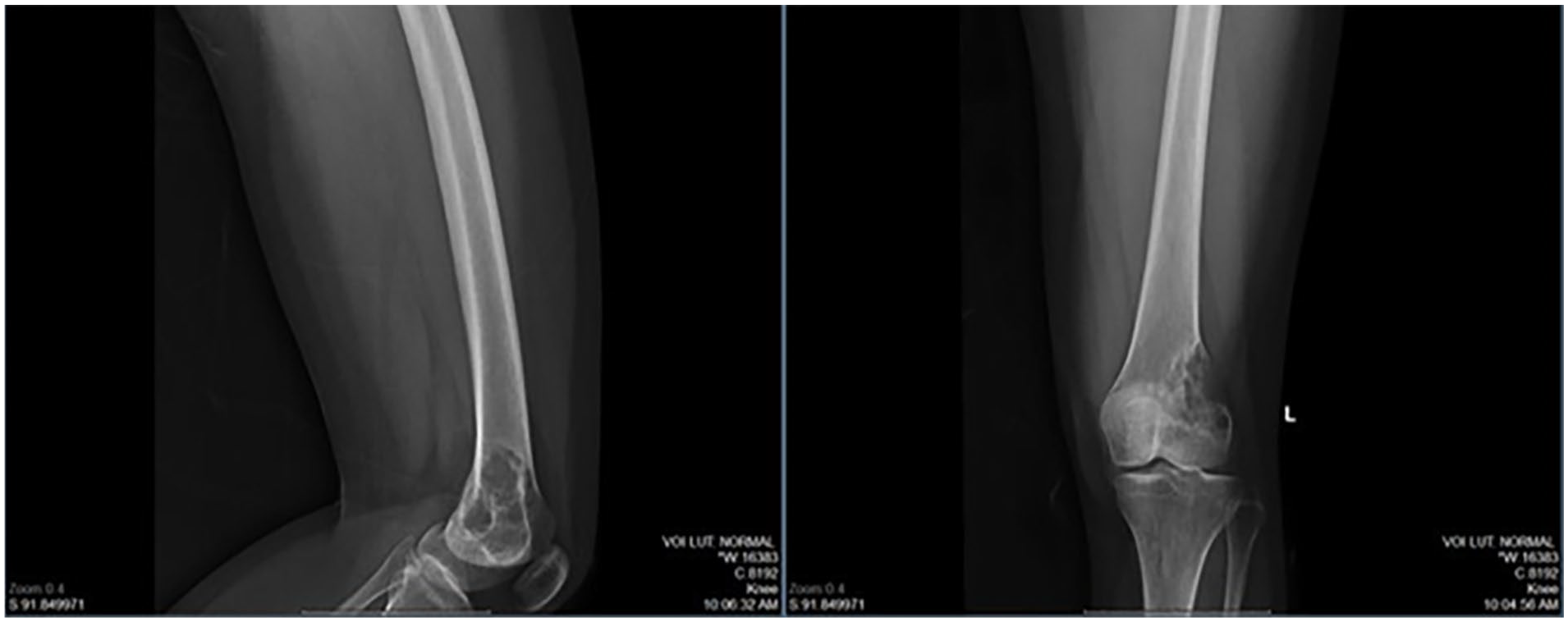
X-ray shows the lytic destructive mass at the left lateral epicondyle of the femur that destroyed the cortex and invaded soft tissue without appreciable mineralization.

MRI showing a large, heterogeneous mass with irregular borders.

PET/CT reveals no metastasis, only uptake at the primary site.
The patient underwent a core needle biopsy. Histopathological morphology revealed the presence of spindle-shaped tumor cells with plump, blunt-ended nuclei, marked nuclear pleomorphism, hyperchromasia, prominent nucleoli, numerous bizarre nuclei, a mitotic index of approximately 12 mitoses per 10 high-power fields (HPF), and a moderate amount of brightly eosinophilic fibrillar cytoplasm. No evidence of osteoid or chondroid matrix was observed. Immunohistochemical staining showed diffuse strong positivity for smooth muscle actin (SMA) and desmin, focal strong positivity for CKAE1/AE3, and negative reactions for S100, Myogenin, and SATB2 (Figure 5). These findings supported a diagnosis of high-grade LMS arising from the bone. After reviewing the patient’s clinical condition, the radiographic imaging, and the results of the biopsy, our multidisciplinary tumor board (MTB) concurred that the diagnosis was primary leiomyosarcoma of bone and surgery was deemed the preferred treatment option. Subsequently, the patient underwent wide resection to remove the lesion in the left distal femur.
Macroscopically showed a tan-white lesion measuring 50 × 45 × 30 mm and located in the center of the left distal femur, involving the metaphysis (Figure 4). Peripherally invades through the cortical bone into the soft tissue on the lateral aspects of the distal femur. Some areas of hemorrhage were present. Microscopically, the tumor cells were spindle-shaped with plump, blunt-ended nuclei, marked nuclear pleomorphism, hyperchromasia, prominent nucleoli, numerous bizarre nuclei, a mitotic index of approximately 12 mitoses per 10 high-power fields (HPF), and a moderate amount of brightly eosinophilic fibrillar cytoplasm. Some areas showed necrosis and hemorrhage. No evidence of osteoid or chondroid matrix was observed (Figure 5). Immunohistochemical stains were performed on the surgical specimens, revealing tumor cells with diffuse strong positivity for SMA, desmin, and h-caldesmon, and focal strong positivity for CKAE1/AE3. The cells were negative for S100 protein. The surgical margins were negative. These results once again confirmed the diagnosis of LMSB. The neoplasm was classified according to the Enneking staging system as a high-grade extracompartimental tumor, stage IIB.

Gross images, tan-white lesion measuring 50 × 45 × 30 mm and located in the center of the left distal femur, involving the metaphysis.
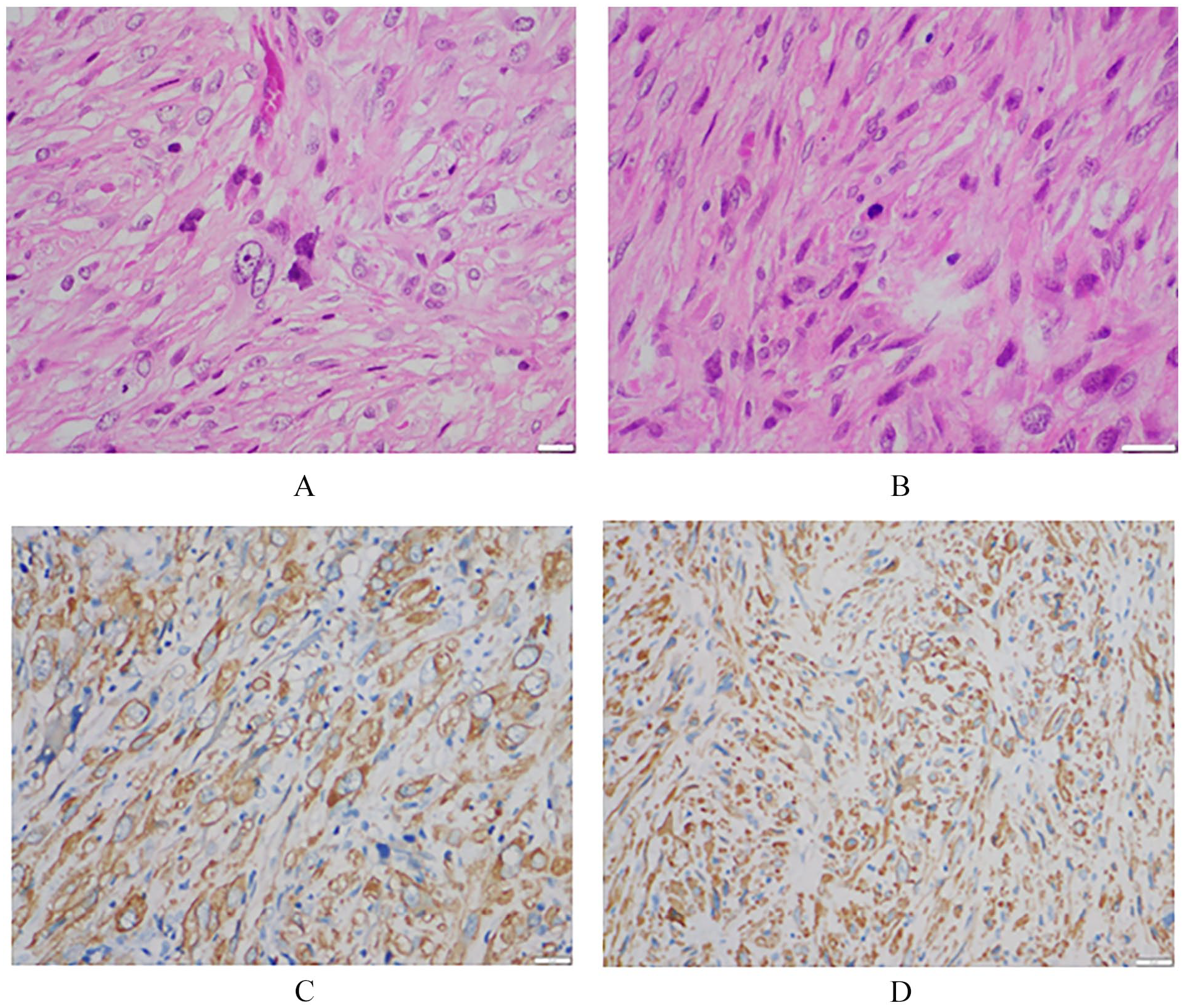
Microscopic images: (A and B) HE stain—The tumor cells exhibit spindle and pleomorphic characteristics with eosinophilic cytoplasm. Immunohistochemical stain shows strong diffuse positivity with smooth muscle actin (C) and H-caldesmon (D).
After surgery, the MTB decided against administering adjuvant chemotherapy or radiotherapy. The patient was closely monitored with clinical and radiological examinations, including MRI of the left femur and lung CT scans every 3 months. One year after surgery, the patient remains in stable health, showing no symptoms and continuing follow-up without evidence of recurrent or metastatic disease.
Discussion
Leiomyosarcoma is a malignant tumor with smooth muscle differentiation that primarily arises in the retroperitoneal soft tissue, gastrointestinal tract, and extremities. 4 However, primary leiomyosarcoma of the bone is a rarely encountered malignant disease, characterized by a high-grade destructive tumor and, unfortunately, a bleak prognosis with limited viable treatment options. Since its inaugural description by Evans and Sanerkin in 1965, 5 documented cases of this phenomenon have remained notably scarce. Some series, such as the one by Antonescu et al with 33 cases, 6 and the study by Mori et al with 48 cases, 7 along with various case reports in the literature,8,9 contribute to our understanding of this rare condition.
The cause of bone leiomyosarcoma can be classified as either spontaneous (de novo) or secondary, with the latter being associated with radiation exposure or a history of another bone tumor. 9 Remarkably, de novo leiomyosarcomas of bone are common in long bones, particulary around thearound the knee joint (64%), 6 whereas 50% of leiomyosarcomas in the craniofacial bones are secondary leiomyosarcoma to radiation exposure. 10 In our case, our patient had no history of exposure or special treatment that could explain the cause of this condition.
Diagnostic imaging typically reveals an osteolytic, radiolucent intramedullary mass with cortical destruction and infiltration into the surrounding soft tissue, as consistently observed in studies.6,8,11 This consistent imaging feature observed in leiomyosarcoma of the bone, as noted in our patient, serves as a noteworthy point for clinicians and radiologists when approaching differential diagnoses. Therefore, these characteristics provide valuable insights for clinicians encountering similar images.
Macroscopically, leiomyosarcoma of the bone manifests as an infiltrative, gray-tan, creamy tumor interspersed with focal areas of necrosis and cystic degeneration. Lesions exhibit a variable size range, spanning from 2 to 12 cm, with an average dimension of 6.1 cm. Remarkably, cortical penetration is observed in 95% of cases, while soft-tissue involvement is a prominent feature in 83% of lesions. 6 Histologically, the majority of cases depict a high-grade tumor characterized by spindle cells of varying sizes, nuclear pleomorphism, hyperchromasia, and prominent nucleoli. In contrast, low-grade tumors exhibit spindle cells with relatively abundant dense fibrillar cytoplasm, elongated nuclei, and minimal nuclear atypia. 12 Variants of Leiomyosarcoma of the bone include classic, pleomorphic, and epithelioid types, with no discernible evidence of osteoid or chondroid matrix.6,8 In immunohistochemistry, SMA emerges as the marker with the highest sensitivity and specificity, displaying positivity in all sarcoma cases. In contrast, HHF-35 exhibits lower sensitivity, a crucial insight into the nuanced diagnostic landscape of leiomyosarcoma of the bone, as highlighted in the literature.
In general, the treatment options for leiomyosarcoma are limited, and outcomes remain poor. Strong guidelines are available only for advanced or metastatic leiomyosarcoma of soft tissue, with no specific recommendations for leiomyosarcoma of the bone. 13 Based on current evidence in the literature, surgery remains the primary and pivotal approach. Radiation therapy has been shown to be effective in reducing recurrence and metastasis rates in soft tissue leiomyosarcoma, but there is no evidence supporting its efficacy in leiomyosarcoma of the bone.10,14,15 Systemic chemotherapy remains controversial, as there is no evidence to suggest it improves survival rates or reduces secondary metastasis. Consequently, it is typically reserved for cases with metastatic disease.10,16
Our patient presented with a tumor measuring 50 mm at its largest dimension, a negative surgical margin, and no evidence of metastasis at the time of diagnosis (as confirmed by PET/CT imaging), all of which are favorable prognostic factors for this condition. 10 These characteristics supported our decision to pursue the most suitable treatment strategy, which involved wide excision of the tumor and reconstruction with a megaprosthesis, followed by rigorous monitoring of other organs, particularly the lungs. Another reported case describes the treatment of leiomyosarcoma in the distal femur through surgery followed by chemotherapy. This approach was prompted by the presence of pathological bone fracture, which may have influenced the patient’s potential for metastasis. 17
Conclusion
Bone leiomyosarcoma is a rare malignancy, diagnosed through a combination of morphological analysis, immunophenotyping, imaging, and clinical findings. Given this, further studies and reports, including comprehensive case reports and multicenter collaborations, are needed to gather additional data on the treatment of this disease. Publishing this case could help disseminate and enhance the understanding of information related to LMSB, providing a valuable resource for diagnosing and treating similar cases.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Nguyen Van Khanh analyzed pathology and immunohistochemistry and wrote the manuscript. Tran Duy Thanh reviewed pathology and immunohistochemistry. Tran Duc Thanh conceived the original idea manuscript and operated the patient. Dang Minh Quang, Le The Hung, Nguyen Tran Quang Sang summed up data, operated the patient, and revised the manuscript. Tran Van Cong, Tran Tuyet Thanh Hai, Vu Hai Son, Nguyen Xuan Hung reviewed the manuscript. Tran Trung Dung operated the patient and reviewed the manuscript. All the authors read and approved the final manuscript.
Statement of Ethics
The procedures used in this study adhere to the tenets of the Declarations of Helsinki. Case reports are approved by the Joint Consultation for Approval of Surgery and are granted an exemption from requiring ethical approval at the Vinmec Healthcare System.
Consent for Publication
Informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the consent is available for review by the Editor-in-Chief of this journal.
Data Availability Statement
All relevant data are provided in the manuscript. Further inquiries can be directed to the corresponding author.