
Abstract
Introduction:
Reduction mammoplasty for bilateral asymmetric hypertrophy remains challenging due to variability in tissue distribution and difficulty in achieving predictable symmetry. This study proposes a numerical planning method that simplifies preoperative markings, minimises subjectivity and enhances reproducibility using fixed reference measurements.
Methods:
Patients with bilateral asymmetric macromastia and varying degrees of ptosis were planned for reduction using a superomedial pedicle–based technique. The upper breast border (UBB) was identified as the key primary landmark, from which the new nipple–areola complex (NAC) medial and lateral pillars were defined numerically at fixed measured points, eliminating the ambiguity during marking and making the process more objective and easily reproducible.
Results:
The numerical method provided consistent, symmetric and aesthetically balanced reductions. Defining the UBB simplified localisation of the NAC, improved prediction of skin excision patterns and maintained scar centrality. The approach decreased operative subjectivity and enhanced predictability of the final breast contour and upper pole fullness. Symmetry was achieved more reliably across various breast sizes, asymmetric as well as symmetric.
Conclusion:
Numerical planning in reduction mammoplasty introduces a system that standardises preoperative markings, optimises parenchymal resection and facilitates aesthetically pleasing symmetry in bilateral asymmetric hypertrophy. The use of UBB as a key landmark redefines surgical planning, emphasising preservation of form and predictable volume reduction. Longterm comparative studies are warranted to validate the stability and efficacy of this simplified, measurement-based approach.
Keywords
Introduction
Reduction mammoplasty, from its inception, has undergone numerous modifications, all directed towards a comprehensive goal of achieving an adequate reduction in volume while simultaneously preserving maximum functional and aesthetic outcomes with minimal scarring. There are multiple approaches to address skin and parenchyma which many able pioneers have popularised with the ideal expectation of ample parenchymal volume reduction in a symmetrical fashion and minimal scarring.
Breast asymmetry refers to variation in volume or shape between the breasts and is observed in approximately 25% of women.1,2 Although the female breasts are often not completely symmetric and whereas in the past small variations were accepted, contemporary culture, new body images and modern ideals of beauty have led people to believe that even small asymmetries in breast shape are not considered aesthetically pleasing. For these reasons, asymmetric breasts have become not just personal but also a social problem affecting the psychological wellbeing and quality of life of the patients.
Breast asymmetry can be classified based on the presenting form of asymmetry and volume discrepancy into unilateral hypoplasia/hypertrophy, unilateral hypertrophy with contralateral hypoplasia and bilateral asymmetric hypertrophy/hypoplasia. All these modalities need either a single or combination approach to achieve adequate symmetry.
Among all the types, bilateral asymmetric hypertrophy of the breast poses a serious challenge to the surgeon, as achieving symmetry post-reduction requires meticulous pre-surgical planning.
For a surgeon attempting reduction mammoplasty for asymmetric breasts, some form of uncertainty in terms of planning and execution with adequate excision is always experienced during their formative years. Even in the hands of experienced professionals, consistency and aesthetics can be challenging on a case-by-case basis. Planning in reduction mammoplasty still leaves a few ambiguities, posing challenges in delivering a standard result in consecutive cases. Breast tissue factors, such as parenchymal volume, degree of ptosis, breast footprint, skin envelope, shape and location of the nipple-areola complex (NAC), as well as phenotypic factors such as height, weight, body type and personal preference, all play a role. Among this multitude of variables, a breast surgeon may feel lost at times despite the best planning and intentions. This can lead to a significant amount of time per operation as a result of the back and forth in the attempt to achieve a good execution and meet patients’ expectations of a sound reduction and symmetry.
Overall, the general satisfaction of patients following a reduction mammoplasty is high; however, a surgeon must not cease to push the boundaries for betterment and predictability of surgical results.
As famously quoted by Hall- Findlay EJ, ‘we cannot manage what we do not measure,’ 3 this study aims at taking a fresh perspective on the standard reduction mammoplasty technique, utilising superomedial pedicle, and attempts to further simplify the marking process, reducing the subjectivity of the steps and redirecting the planning towards a more predictable approach with measurements, thus increasing the consistency of the results. This article is an attempt to formulate certain guidelines for planning resection of parenchyma and skin in cases of breast asymmetry, aiming to achieve a more pleasing outcome for the patient and the surgeon while optimising volume reduction.
Inclusion Criteria: All patients presenting with complaints of bilateral asymmetric macromastia along with varying degrees of ptosis were included in the study. Patients with a preference for considering a periareolar approach or augmentation mastopexy (both parenchymal and implant-based) were excluded.
Methodology
After taking clinical pictures in all the standard views, all included patients were marked with arms by their side in a relaxed position. The primary author (SB) made all measurements and performed markings to avoid any bias. Data was collected for each patient in terms of demographic and anthropological parameters.
Keeping the superomedial pedicle as the basis, there are standard landmarks and measurements that help guide the planning for the procedure. To reiterate, the traditional marking
4
proceeds as follows:
After marking the vertical midline, the sternal notch and the inframammary folds are marked. The breast meridian is determined along the breast irrespective of the native nipple areola complex, thereby giving the ideal location of the future NAC. Measurements are taken for distances between the sternal notch and the nipple. The position of the new nipple is decided by placing it at almost the level of IMF and placing the areolar marking 2 cm above it on the breast meridian. Once the level is decided, a freehand or a stencil aided marking akin to a dome is made for the areola. The pillars are then marked by rotating the breast in either direction and marking vertically both lateral and the medial pillar along the breast meridian. A 5–7 cm mark is placed to define the length of the pillar followed by a gentle curvature meeting 2–3 cm above the present IMF as skin excision pattern. For the inferolateral and inferomedial parenchyma excision, extensions are marked from the end of pillars to medial and lateral extent of the IMF so that the parenchymal excision is in a wise pattern. The superomedial pedicle is finally marked, thus delineating the area of excision.
In due course of time, other landmarks and markings have been added, which have helped define the breast footprint more clearly.
5
These are:
Upper breast border: present as a junction between the chest wall and breast, this landmark helps in defining ‘high breasted’ or ‘low breasted’ patients. It also helps in positioning the nipple and predicting its change during the procedure. Clavicle to UBB: Although a more significant variable in case of augmentation surgeries, this variable has a low impact on reduction surgeries. UBB to Nipple: Like the above-mentioned variable, this distance is also more applicable in the augmentation surgeries. NAC – IMF: This distance invariably reduces as IMF is usually elevated in cases of supero-medial pedicle with vertical scar technique.
Although the method overall provides good guidance for reduction marking, a few points pose significant challenges in achieving adequate symmetric reduction and delivering consistently good results in different patients, despite the volume of reduction.
The unpredictability of technique in medium to large size breasts.
The ambiguity of pillar markings due to the extent of rotation of breasts not being standardised and proving to be difficult in case of macromastia, hence leading to suboptimal parenchymal removal.
Nipple position measurements, which may lead to inadequate reduction.
The downward pull of the tissue due to gravity can confound the actual position and markings on the skin, as the elastic recoil of the remaining offloaded tissue is not considered.
Lack of clarity in planning the skin excision limit.
The focus of what is to be removed is more dominant than what is to be saved.
Steep learning curve to give consistent results.
Modifications
The points that we put forward for numerical-based markings for a breast reduction of any size are as follows:
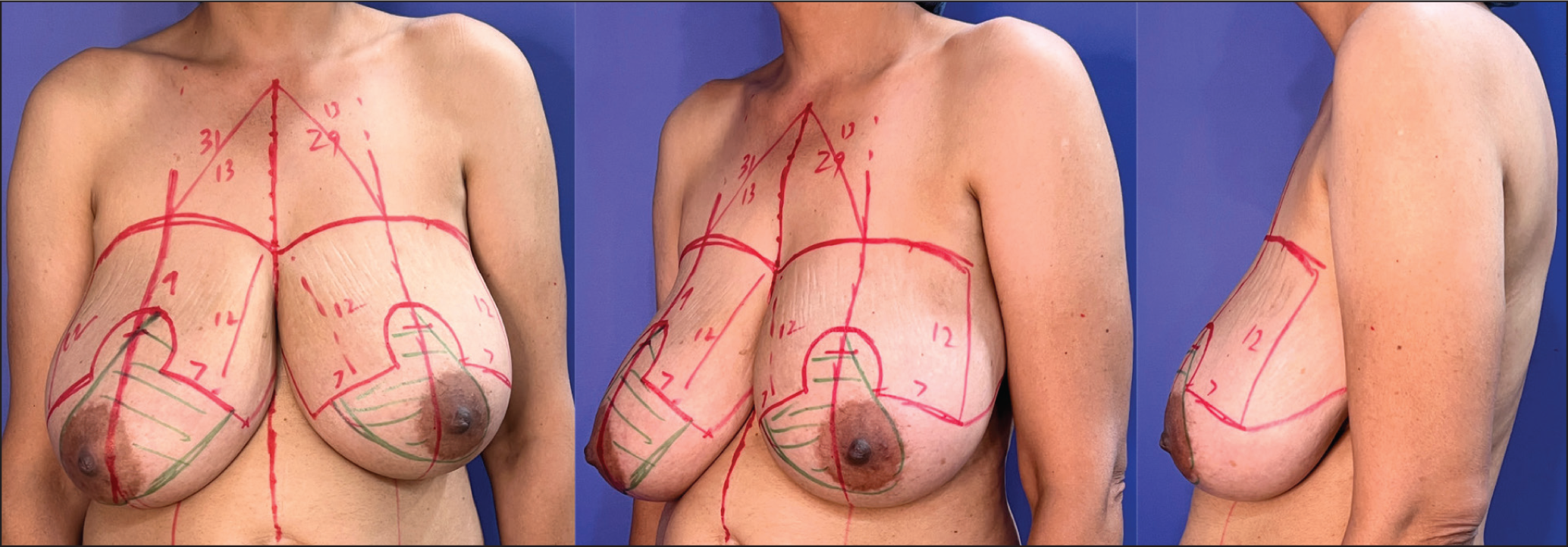
During the pre-operative examination, all asymmetries are assessed and explained to the patient, and the findings are documented in the medical records. The upper breast border is identified by tracing medially from the axillary fold. In larger breasts it can also be determined by folding the breasts superiorly. Breast meridian, midline, inframammary fold and anterior axillary line is also marked to complete the anatomical framing. The new nipple position is marked on the breast meridian at 8.5 cm-9.0 cm from the upper breast border. The dome of the nipple-areola complex is drawn either freehand (as by the senior author) or a stencil may be used to assist in keeping the measurement at approximately 13 cm. The horizontal distance between the ends of the dome is typically 5 cm. The marking of the lateral pillar on the skin is achieved by two reference points
Junction of anterior axillary line and upper breast border Lateral end of the neo nipple areolar complex dome. From the first point, a distance of 12 cm–13 cm is marked obliquely towards the inferior part of the dome. It is intersected by a marking from the second point at a distance of 7 cm. Similarly, for the medial pillar, a distance of 12 cm–13 cm is taken from the medial end of the upper breast border, obliquely directed at a distance of 7 cm from the medial end of the dome. In this way, we do not need to rotate the breasts for marking and have a symmetrically marked skin envelope, medially and laterally on both breasts. From the end of this skin marking at 7 cm, the Wise pattern can be marked by a line extending laterally and medially to meet the inframammary fold. In the event that a vertical scar is planned, the only change is the length of the pillar, which is maintained at 5 cm. The inferior marking then proceeds from this point towards the inframammary fold in the standard manner. Since we are keeping the medial and lateral pillars equidistant, the central placement of the scar is more predictable (Figure 1).
Markings for Reduction Mammoplasty Shown in Front (A), Oblique (B) and Lateral (C) Profile.
Results
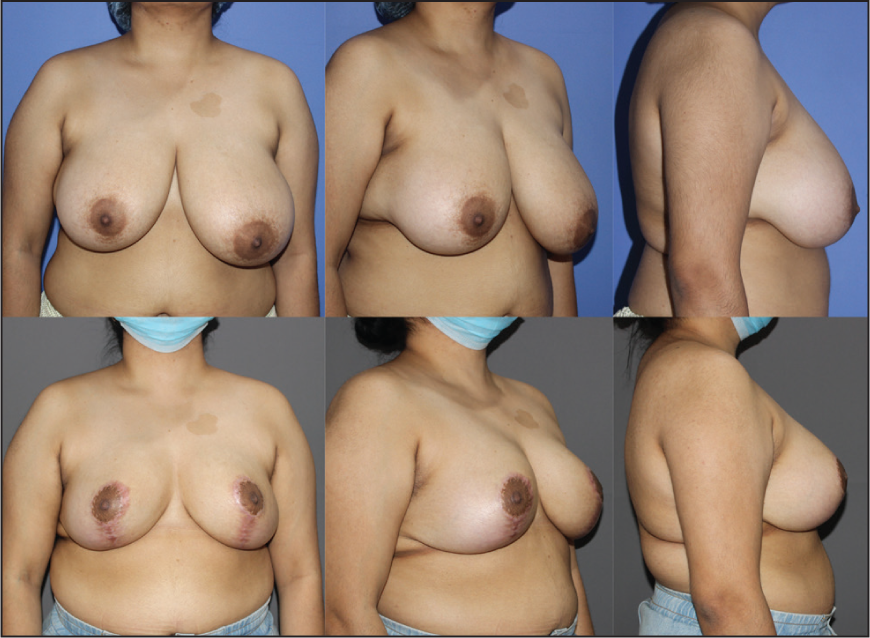
Preoperative Images A-C Show Asymmetry with a Larger Left Breast and Difference in the Direction and Level of NAC; Postoperative Images D-F Show Postoperative Result After 8 Weeks with Improved Symmetry and Repositioned NAC.
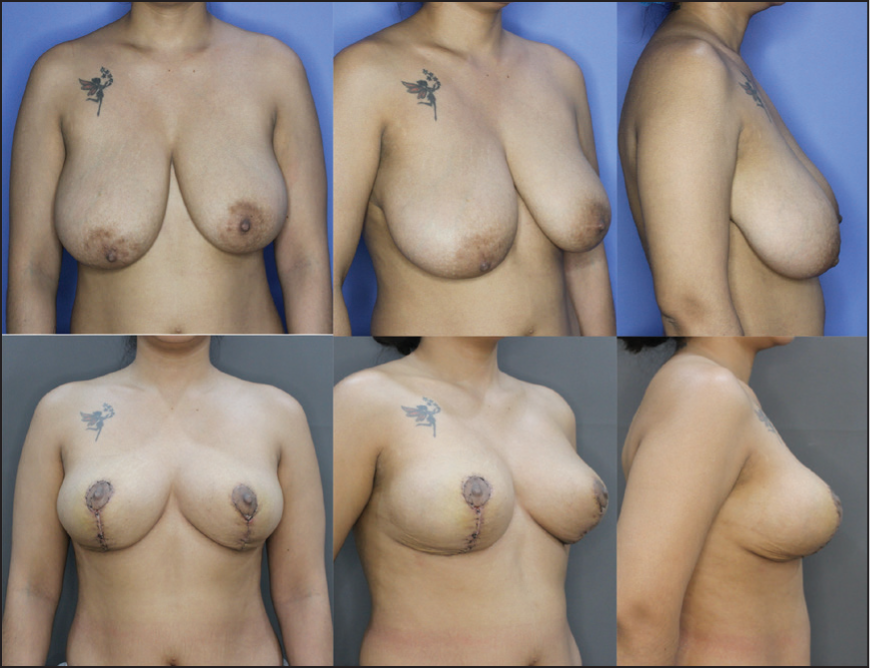
Preoperative Images A-C Show Asymmetry with Larger Right Breast and Difference in the Direction and Level of NAC; Postoperative Images D-F Show Postoperative Result After 8 Weeks with Improved Symmetry and Repositioned NAC. Note: There is a Postural Tilt Towards the Right Side, Which is Present in Both Pre- and Postoperative Images.

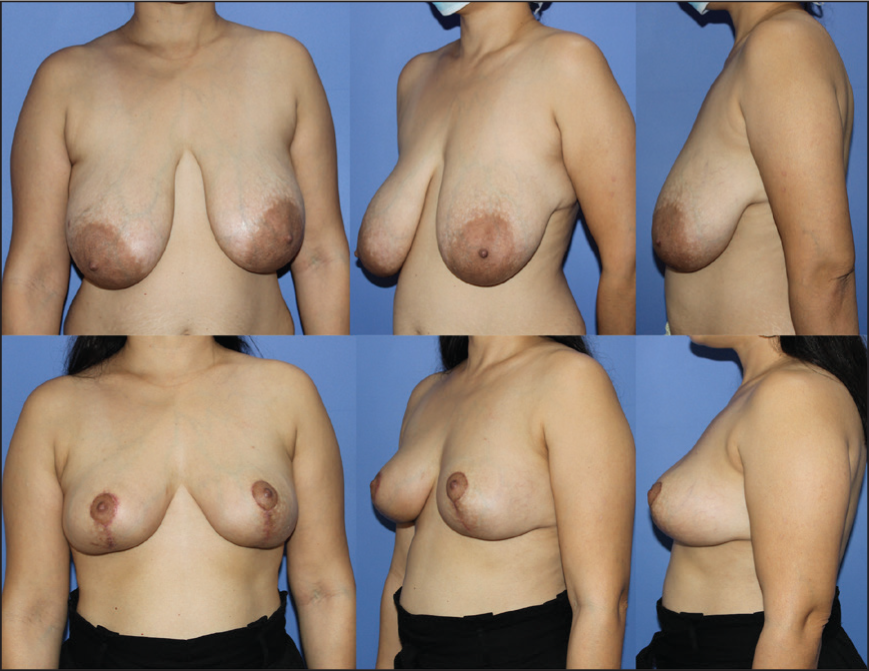
Preoperative Images A-C Show Asymmetry with Significantly Larger Right Breast and Difference in the Direction and Level of NAC; Postoperative Images D-F Show Postoperative Result After 3 Weeks with Improved Symmetry and Repositioned NAC.
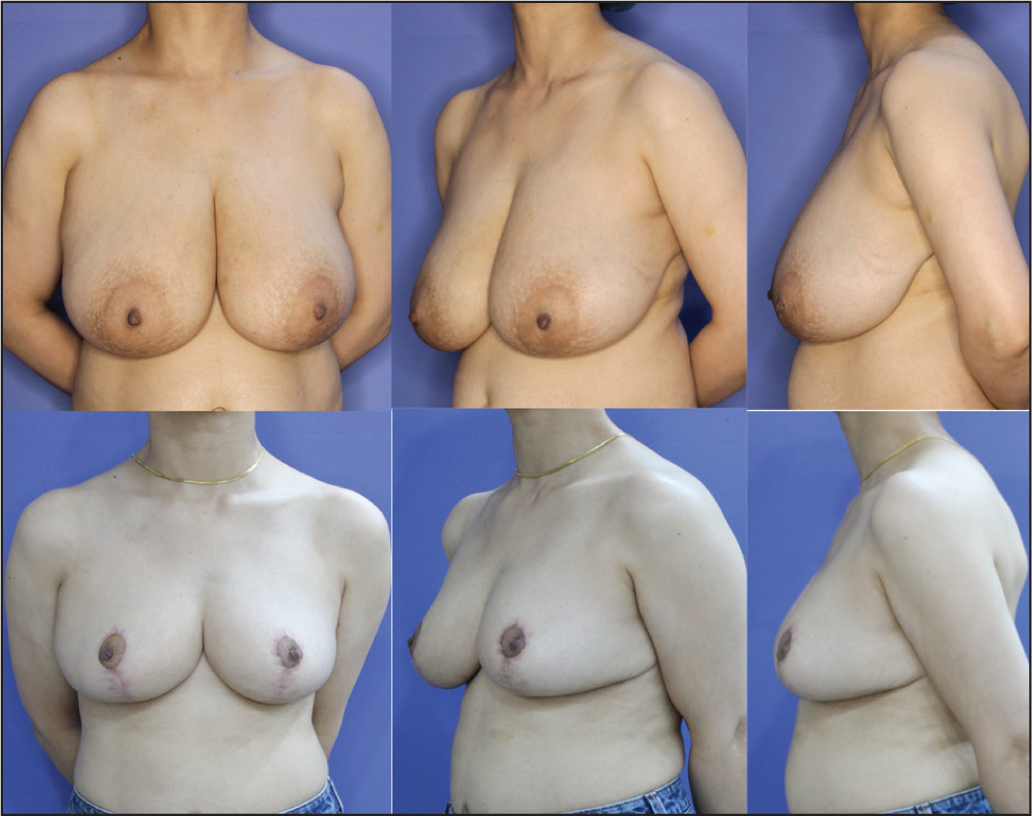
Preoperative Images A-C Show Asymmetry with Larger Left Breast and Severe Ptosis; Postoperative Images D-F Show Postoperative Result After 8 Weeks with Improved Symmetry and Repositioned NAC.

Preoperative Images A-C Show Asymmetry with Larger Right Breast with Large Areola and Difference in the Direction and Level of NAC; Postoperative Images D-F Show Postoperative Result After 8 Weeks with Improved Symmetry and Repositioned NAC.
Preoperative Images A-C Show Asymmetry with Larger Left Breast with Bilateral Axillary Fullness and Large Areola with Difference in the Level of NAC; Postoperative Images D-F Show Postoperative Result After 8 Weeks with Improved Symmetry, Reduced Axillary Fullness with Repositioned NAC and Reduced Areola.

Preoperative Images A-C Show Asymmetry with Larger Left Breast with Ptosis and Large NAC; Postoperative Images D-F Show Postoperative Result After 3 Weeks with Unilateral Reduction for Symmetry and Improving NAC Size and Position.

Discussion
One crucial factor in predicting long-term preservation of aesthetic outcomes is the degree of similarity in treatment of both breasts. Breasts that are treated more symmetrically (with similar procedures on both sides) are more likely to maintain a desirable aesthetic outcome over time compared with breasts treated asymmetrically (different procedures on both sides). This is because breasts treated more symmetrically are more likely to undergo similar changes and react to aging, pregnancy or changes in weight in a similar manner over time. 6 Therefore, asymmetrically treated breasts may experience dissimilar changes, and thus, a desirable aesthetic outcome may not be sustained.6,7
Few studies have described ways to improve breast symmetry in reduction mammoplasty cases by operative modifications. Planas J and Mosely LH, 8 in their study on improving breast shape and symmetry in reduction mammaplasty, concluded that bilateral reduction mammoplasty alone may result in disappointing asymmetry and shape despite accurate preoperative measurements and precise operative procedure. Underscoring the importance of Gillies maxim ‘In plastic surgery, never throw anything away,’ the modified Strombeck technique reduces mammoplasty by pressing on the need to elevate an inferior dermofat flap, which could be used to address asymmetry on table after skin and parenchymal resection. 9 However, we strongly believe that while the patient is in the supine position the exact assessment of breast size cannot be made. The ideal time for maximising the probability of achieving symmetry postoperatively is while making the preoperative markings in the standing position with the effects of gravity maximised.
Reduction mammoplasty is one of the most gratifying yet technically demanding procedures in terms of aesthetics. It is essential that we understand that breast borders are available for alteration by either addition or subtraction of volume and thus determining the position of the mound and nipple areola complex. Understanding what is left after the reduction is more important, as it provides an accurate idea of what actually needs to be excised.
We strongly advocate superomedial pedicle for achieving extensive reduction and maintaining symmetry and a desirable form. Depending on the skin quality, degree of ptosis and volume, the choice of skin excision pattern can be made. The removal of an inferior wedge of breast tissue allows the surgeon to narrow and cone the breast, thus improving its shape. It also removes the heavy inferior breast tissue and leaves behind the superior breast tissue, thereby resisting the effect of gravity. We prefer the superomedial pedicle because it has dual axial blood supply, it rotates easily into position without kinking or compression if adequate volume is reduced, and it has a better sensation than other pedicles. A (true) superomedial pedicle can provide consistent, predictable and long-lasting results with a good breast shape 5 which is not dependent on the skin envelope for its suspension.
In this study, we have seen that the single landmark that changes the entire planning strategy and simplifies it is the upper breast border. It is the slightly curvilinear superior limit which lies at the level of indentation where the pre-axillary fullness meets the breast. Previously, SSN-N distance was taken as the guide, however this distance is measured along the skin surface and this measurement is clearly different from a true vertical measurement. We chose the UBB as our key point since the visual impression of NAC is more relevant in relation to the UBB, being high or low positioned rather than any other landmark or breast. It also negates the bias generated with the level of breast footprint in relation to the clavicle.
The need for marking the medial and lateral pillars by medial and lateral rotation of the breast can be challenging to perform in heavy and asymmetric breasts and can be subjective based on the comfort of the patient and the surgeon, and is thus mitigated with this technique.
In this present study, we have realised that UBB helps in defining a few important aspects of planning in a case of reduction mammoplasty.
One of the most essential aesthetics of the breast is the upper pole fullness. Stitching the parenchyma to the pre-pectoral fascia in the upper pole around the 2nd rib may lead to an on-table fullness and be an early positive result, but disappoints over time as it slides down with the effect of gravity in due time. What needs to be understood is that in a well-executed reduction procedure with adequate excision of both skin and parenchyma, the upper pole is automatically made full without raising the upper breast border.
It also provides a confirmation for the new NAC position where it should actually lie, thus further confirming the position and avoiding a high or a low placed nipple.
The frontal curve of the breast is what changes in the most impressive way, 10 and yet there are no markings until now to give us a full control over this critical variable.
The length to pillars from its medial and lateral edges can help in truly predicting the actual skin excision pattern, thus giving more symmetrical and predictable results every time. This measurement range of 12 cm-13 cm has been deduced by the primary author (SB) after making measurements of breast perimeter along its curvature in patients with normal breast cup sizes B and C in a chest size of 32–34 inches with nil to Grade 1 Ptosis after due consent. A total of 25 measurements were taken and an average range was calculated which was then halved to give two lengths that come together to give the breast perimeter post parenchymal excision. This particular measurement also helps in removing the ambiguity of turning the breast parenchyma to mark the pillars thereby avoiding any asymmetry.
The vertical scar is in the centre and more aesthetic.
By using this approach, we have effectively addressed both parenchyma and skin to achieve a symmetrical, predictable result (Figures 2–13). However, akin to planning in reverse, we are fixing the envelope first and matching the parenchymal excision, which helps us determine the range essentially. Since the technique focuses on the aesthetics of the tissue that remains and guides what should be optimally excised, it also holds good for all regular breast reductions as well.
Preoperative Images A-C. Postoperative Images D-F After 24 Weeks.

Preoperative Images A-C. Postoperative Images D-F After 24 Weeks.

Preoperative Images A-C. Postoperative Images D-F After 24 Weeks.

Preoperative Images A-C. Postoperative Images D-F After 18 Weeks.

Preoperative Images A-C. Postoperative Images D-F After 18 Weeks.
Some authors have also attempted to achieve a reduction in bilateral asymmetric hypertrophy of the breast11–13 using liposuction rather than resection. Although reduction by liposuction is associated with a faster return to work and daily activities, and the shortest possible scars, this technique has had difficulty gaining widespread acceptance, predominantly because it does not offer improvements in breast shape, as aesthetic results largely rely on skin retraction, which is not achieved with liposuction alone.
Conclusion
Using reduction mammoplasty with a vertical scar and superomedial pedicle for addressing breast asymmetry is a versatile technique that provides a great range of execution if planned correctly. The aim of this study was to make the planning more approachable and mathematically repeatable so as to achieve more consistent results. With a different perspective of what needs to be saved, and changing the perspective of landmarks, it appears that UBB and the perimeter length have given more simplicity to the technique, hoping to give more confidence to a novice as well as an experienced surgeon to take up cases with medium to larger size breasts and provide dependable results. In due time, the long-term stable results will require a comparative analysis to establish the efficacy of this approach.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Clearance
This study did not require formal ethical committee approval as all participants were patients treated within the standard scope of care at our institution. No experimental interventions or deviations from established clinical protocols were undertaken. The study complies with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent for Publicatione
Written informed consent was obtained from all patients for the surgical procedures performed and for publication of their anonymised clinical details and images in this article. All personal identifiers have been removed to ensure complete patient confidentiality.