
Abstract
Background:
Progressive tension sutures (PTS) have emerged as a key technique in abdominoplasty, initially to reduce complications such as seroma formation, and more recently to enhance aesthetic outcomes. This study evaluates the clinical and aesthetic impact of PTS in lipoabdominoplasty.
Methods:
A retrospective analysis was conducted on 291 patients who underwent lipoabdominoplasty with standardised PTS placement between October 2021 and October 2024. The surgical protocol included 360 circumferential liposuction, limited central undermining and PTS application for anatomical contouring. Patient satisfaction was measured using a validated five-point Likert scale. Descriptive statistics summarised outcomes.
Results:
The mean patient age was 38.1 ± 9 years; 90.6% were female. The overall complication rate was low: seroma occurred in 7.8% (back) and 3.1% (abdomen), with minimal rates of widened scar (3.1%), hypertrophic scar (3.1%), wound dehiscence (1.6%) and necrosis (0.8%). No secondary procedures or scar revisions were required. Patient satisfaction was high: for abdominal shape and contour, 95.9% were satisfied or highly satisfied; for umbilicus shape, 94.9%; for scar quality, 93.5%; and for skin laxity, 97.9%.
Conclusion:
The addition of PTS to lipoabdominoplasty increases operative time by only 15–20 min but significantly reduces seroma formation and improves both aesthetic outcomes and patient satisfaction. PTS should be considered a standard component of abdominoplasty. Further multicentre studies are recommended to standardise technique and optimise outcomes.
Introduction
Abdominoplasty, commonly referred to as a ‘tummy tuck’, is a surgical procedure involving the removal of excess fat and skin from the abdominal wall and the reinforcement of the weakened musculofascial system. 1 One of the earliest descriptions of abdominoplasty as a surgical technique dates back to the 1800s. Up until the early 1900s, it was primarily utilised for the treatment of open abdominal wounds and large, bulging ventral hernias. It was not until the 1970s that surgeons recognised its potential as a technique for achieving a firmer and flatter trunk. Since then, abdominoplasty has undergone significant evolution, driven by advances in surgical techniques and instrumentation. 2
The modern approach to abdominoplasty often incorporates liposuction, a combination known as lipoabdominoplasty, which is also the technique employed by the author. 3 Despite these advancements, post-operative complications persist, with seroma formation being the most common. In their original article, Pollock and Pollock concluded that the use of progressive tension sutures (PTS) led to a reduction in seroma formation. PTS is a technique in which the abdominal flap is secured in its new, advanced position using barbed sutures strategically placed at multiple points. A 2017 meta-analysis by Seretis et al. further confirmed that progressive tension suturing independently decreases the incidence of seroma formation. 4
While initial research on progressive tension suturing focused primarily on complication reduction, more recent literature and clinical experience suggest that PTS also contributes to improved aesthetic outcomes. These benefits include greater flap advancement, enhanced contour definition around the waist and umbilicus, and finer scars due to reduced tension along the suture line. Anatomy-defining PTS techniques have also been utilised to subtly enhance the definition of the linea alba and linea semilunaris. 5 Additionally, the lateral aspect of the abdominal flap can be advanced and sutured more inferomedially, resulting in improved waist definition and reduced lateral skin redundancy. 6
This study focuses on our experience with progressive tension suturing, thereby minimising variability in surgical technique and outcome evaluation. The nuances of the procedure are detailed to ensure reproducibility, and the benefits of incorporating this step as part of the standard of care in abdominoplasty are highlighted.
Materials and Methods
This retrospective study included patients who underwent lipoabdominoplasty with PTS between October 2021 and October 2024.
Surgical technique: Lipoabdominoplasty with PTS (Video:
Pre-operative Marking
Pre-operative markings were performed with the patient in the standing position. The midline (xiphoid to pubic symphysis), rectus abdominis borders, planned incision line, areas of redundant skin and zones for liposuction were delineated.
Anaesthesia and Liposuction
All procedures were performed under general anaesthesia. Tumescent solution was infiltrated into the upper and lateral abdomen and mons pubis. Liposuction was performed using VASER→ (Vibration Amplification of Sound Energy at Resonance) for fat emulsification, followed by power-assisted liposuction (PAL) for fat extraction.
Abdominal Flap Elevation
A lower transverse abdominal incision was made, and the abdominal flap was elevated in the subfascial plane. The umbilicus was circumferentially incised and dissected free. Central undermining was limited to approximately 2 cm bilaterally from the midline, extending superiorly to the xiphoid. Rectus muscle plication was performed as indicated.
Progressive Tension Suturing (PTS)
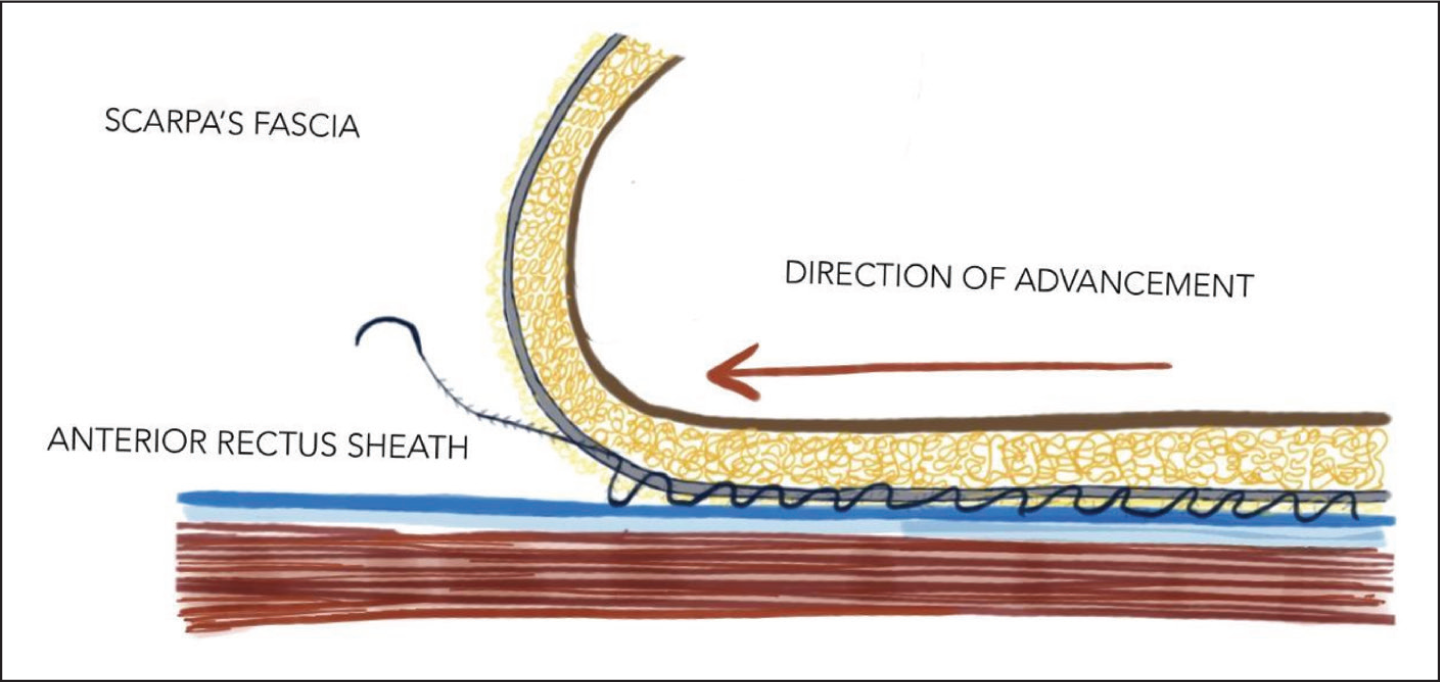
PTS placement was performed using barbed No. 1 polydioxanone (PDS) sutures, combining running and interrupted techniques. All sutures were placed strictly in the midline between Scarpa’s fascia and the rectus sheath, an anatomical plane devoid of significant neurovascular structures, thereby minimising the risk of vessel or nerve entrapment.
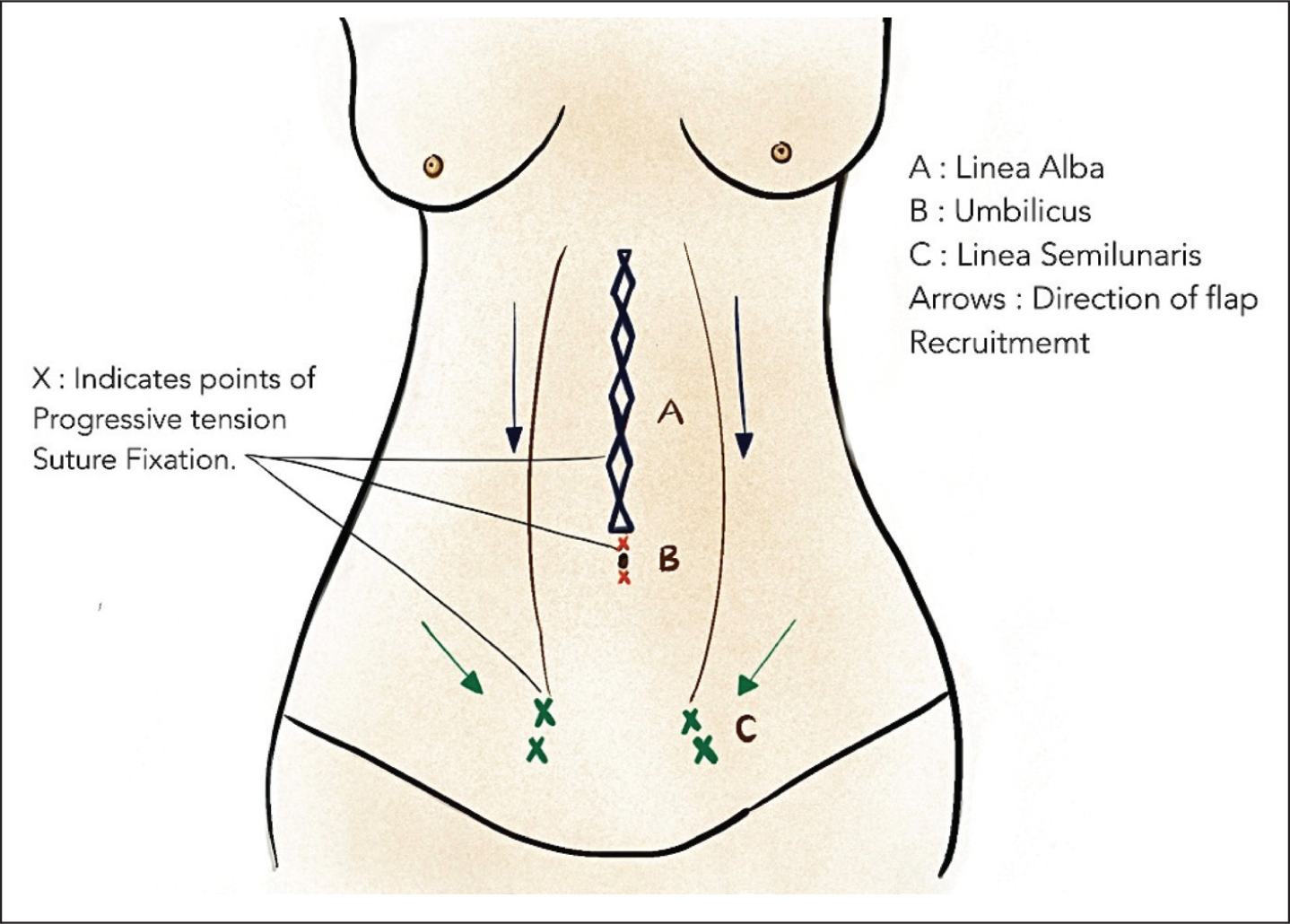
Linea alba definition: A continuous running suture anchored Scarpa’s fascia of the abdominal flap to the rectus sheath from the xiphoid to the umbilicus, accentuating the linea alba. The linea alba suturing was performed using a double-barbed suture.
Waist contouring: Interrupted sutures advanced the lateral flap inferomedially, reducing lateral skin redundancy and enhancing waist definition.
Umbilical aesthetics: Interrupted PTS were placed superior and inferior to the umbilicus to create a natural periumbilical contour.
Linea semilunaris enhancement: Bilateral sutures along the lower flap margin define the linea semilunaris.
PTS differs from traditional quilting sutures by prioritising tension redistribution, dead-space reduction and anatomical contouring rather than simple flap fixation (Figures 1 and 2).
Anatomy Defining Progressive Tension Sutures.
Lateral View of Suture Placement Between Scapa’s Fascia and Anterior Rectus Sheath.
Closure
Umbilicoplasty was performed, followed by excision of excess flap tissue. Layered closure was completed over a single closed-suction drain (e.g., Romovac→).
Aesthetic outcomes were evaluated by the operating surgeon using standardised pre-operative and post-operative photographs at 3- and 6-month follow-up (Figures 3–8).
47-year-old Female (Pre-op and 24 Weeks Post-op).

38-year-old Female Postpartum (Pre-op and 24 Weeks Post-op).

Patient satisfaction was assessed using a validated five-point Likert scale focusing on abdominal appearance and scar quality (Figure 9). Descriptive statistics were used to summarise patient demographics and outcomes.
Final Fine Surgical Scar—8 Months Post-operative.

Results
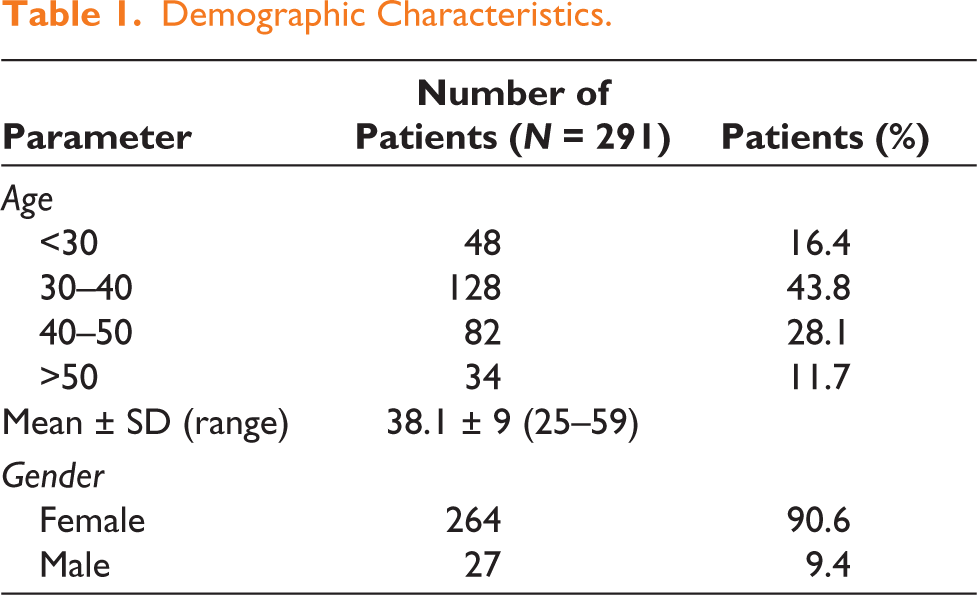
A total of 291 patients underwent lipoabdominoplasty with PTS during the study period. The mean age was 38.1 ± 9 years (range: 25–59). The majority of patients were female (n = 264, 90.6%) (Table 1).
Demographic Characteristics.
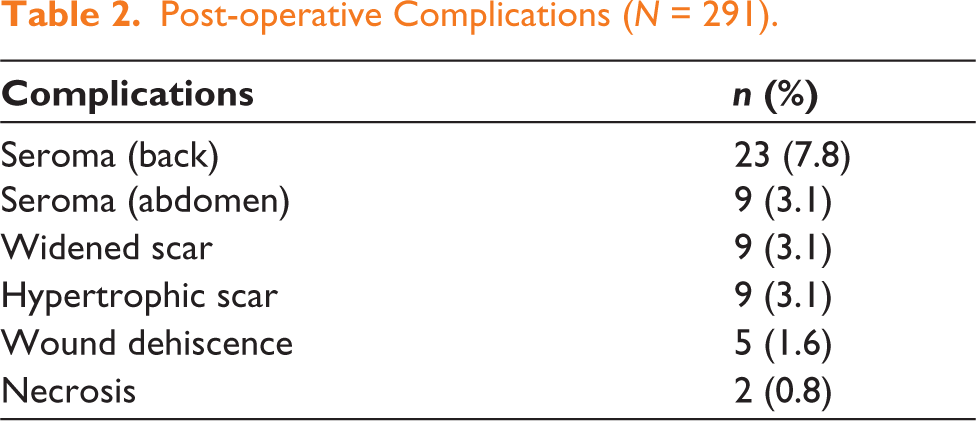
The overall complication rate was low. Seroma formation occurred in 23 patients (7.8%) in the back and 9 patients (3.1%) in the abdomen. Widened scar and hypertrophic scar were each observed in nine patients (3.1%). Wound dehiscence of less than 5 mm only, occurred in five patients (1.6%), and small area flap necrosis (at midline of less than 5 mm) was noted in two patients (0.8%) (Table 2). No secondary procedures or scar revisions were needed in these cases, as they healed secondarily.
Post-operative Complications (N = 291).
Patient-reported outcomes demonstrated high satisfaction. A validated five-point Likert scale was used to assess satisfaction levels (Table 3).
Patient Satisfaction Outcomes (N = 291).

Discussion
The roles of PTS in abdominoplasty can be broadly divided into two categories: complication reduction, which was the original focus of surgeons incorporating its use, and aesthetic enhancement, which is a current topic of interest.
Seroma formation remains one of the most common and challenging complications in abdominoplasty. This complication is multifactorial, often attributed to damage of lymphatic channels, the presence of dead space between the abdominal flap and the underlying sheath and the inflammatory response following tissue manipulation. For decades, surgeons have sought effective strategies to minimise seroma formation. The technique of quilting sutures in abdominoplasty was first described by Ricardo Baroudi in 1998 as a method to reduce seroma risk. 7 This approach was further advanced in a landmark publication by Pollock in 2000, where the use of PTS—distinct from traditional quilting—was introduced as a technique to decrease local complications in abdominoplasty. In his review of 65 abdominoplasties, Pollock concluded that there was a significant reduction in complications with the use of PTS. 8
Subsequent studies have reinforced the efficacy of PTS. Bromley et al. reported a reduction in seroma risk to as low as 0.1% with the use of PTS. 9 In a comprehensive review of 597 cases, Pollock and Pollock demonstrated a statistically significant decrease in seroma formation associated with progressive tension suturing. 10 Since then, numerous studies have evaluated the role of PTS. Notably, a randomised study by Nahas et al. in 2007 compared four patient groups: those treated with drains, with PTS, with both, or with neither. While seroma rates were similar in the drain and PTS groups, the severity and volume of fluid collections were notably lower in the PTS group, suggesting a more effective collapse of the dead space when PTS was used. 11
Recent evidence further supports the safety and efficacy of PTS. Ledezma Rodríguez et al. compared conventional abdominoplasty with abdominoplasty utilising PTS and found that PTS not only decreased complications but also led to reduced rates of seroma formation and wound dehiscence. 12 Theoretically, PTS provides a more even distribution of tension, preventing excessive pressure on blood vessels and reducing the risk of flap necrosis or dehiscence. Moreover, anchoring the flap with PTS offers greater stability and minimises shearing forces that could disrupt primary healing.
The results of our study similarly demonstrate a significant reduction in seroma formation and drain output compared to historical controls. The combination of PTS and a drain allows for effective collapse of potential spaces for fluid collection. The use of tension sutures was associated with lower drain output and a shorter duration of drain use, leading to enhanced recovery post-surgery. With fewer or no drains required, patient recovery is more comfortable, and early mobilisation is facilitated, which may also reduce the risk of serious complications such as deep vein thrombosis. Additionally, a shorter reliance on drains simplifies post-operative care and may reduce overall costs.
Beyond its role in complication prevention, recent literature—though still limited—has explored the aesthetic benefits of incorporating PTS in abdominoplasty. Conventional abdominoplasty often results in a flat and unrefined abdominal appearance, lacking the natural contours that are considered aesthetically pleasing. A defined midline groove between the rectus muscles, as well as the delineation of key anatomical landmarks such as the linea alba and linea semilunaris, contribute to a more desirable and toned abdominal contour. The author utilises PTS to define these features, creating the highlights and shadows characteristic of a chiselled abdomen. Strategic placement of PTS also enhances umbilical positioning and contour, while advancing and suturing the lateral aspect of the abdominal flap more inferomedially improves waist definition and reduces lateral skin redundancy.
Patronella has emphasised the importance of modified ‘anatomy-defining’ PTS for restoring form in abdominoplasty. 12 In his 2021 article, Patronella further expanded the concept of PTS to abdominal contouring, describing the use of sutures to define the linea alba and linea semilunaris. 13
It is well established that excessive tension at the surgical site can lead to scar widening and hypertrophy during healing. PTS allows for redistribution of tension across multiple points, rather than concentrating it at the incision line, thereby promoting narrower and flatter scars. However, final scar quality remains subject to individual patient healing characteristics.
The authors’ review of cases over the past 3 years has yielded high patient satisfaction scores, attributable to these refinements of the conventional technique.
Nevertheless, the technique is not entirely without drawbacks. Placement of multiple sutures may increase operative time and requires a thorough understanding of anatomy to avoid issues such as skin puckering or nerve irritation. Fortunately, these complications are uncommon and generally transient when proper technique is used. As Ledezma Rodríguez et al. concluded, abdominoplasty with PTS does not increase complication rates. 12 Furthermore, the application of PTS has now been extended to other procedures in plastic surgery, such as brachioplasty and body lifts.
PTS serve a dual role in abdominoplasty: they are a proven strategy for reducing complications, particularly seroma formation, and a valuable tool for achieving superior aesthetic outcomes. Ongoing research and long-term follow-up will further clarify the full spectrum of benefits offered by this technique.
Future Recommendations
Further high-quality, multicentre studies and meta-analyses are warranted to comprehensively evaluate its long-term outcomes. Establishing universal guidelines for PTS placement and technique will facilitate broader adoption and may ultimately position PTS as a standard of care in abdominoplasty, rather than an optional adjunct.
Conclusion
PTS help not only in reducing the chances of seroma formation and reducing tension on the suture line, but also, if used in the described manner, can help achieve high-definition results to enhance the contouring achieved in this surgery. The incorporation of PTS in abdominoplasty adds only 15–20 min to the overall surgical time, a modest increase that is outweighed by the substantial benefits in reducing complications and enhancing aesthetic outcomes.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Adarsh Keshari from APAR Health, Gurugram, for medical writing assistance (SPARK PROGRAM).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.