
Abstract
Intralesional triamcinolone acetonide has been used as a common treatment modality for nodulocystic acne and can induce a significant reduction in the acne nodules owing to its anti-inflammatory effect. Intralesional steroids have been associated with potential adverse events like erythema, telangiectasias, secondary infections, hypersensitivity reactions, panniculitis, hypopigmentation, atrophy, and rarely Cushing syndrome. However, improper administration may lead to rare but significant complications like sterile abscess formation and risk of facial deformity. Inadvertent injection of high concentration or amount, wrong site, and multiple doses can lead to these localised or systemic side effects. As acne is a common skin condition affecting the adolescent age group, the possibility of such localised complications, especially a sterile abscess, cannot be ignored. This report documents an unusual presentation of a subcutaneous cystic collection following intralesional steroid injection for acne.
A 22-year-old female presented with a one-month history of swelling over the left cheek. The swelling developed two days after she received a triamcinolone acetonide injection for her acne breakout at a local hospital nearby. She was started on oral antibiotics immediately after the onset of swelling. Despite starting on antibiotics, the swelling progressively enlarged, covering the left side of the face from the infraorbital region to the mandibular line. There was pain associated with the swelling. There was no redness, itching, or systemic symptoms. The patient had no significant medical or surgical history and was not on any medications or supplements. She denied any history of smoking or regular alcohol intake.
Physical examination showed vital parameters within normal limits. Clinical examination revealed a fluctuant swelling extending from the infra-orbital region to just above the mandibular border on the left side of the face. The swelling was not hyperaemic or warm to touch. The skin over the swelling was stretched. There were no signs of facial nerve weakness.
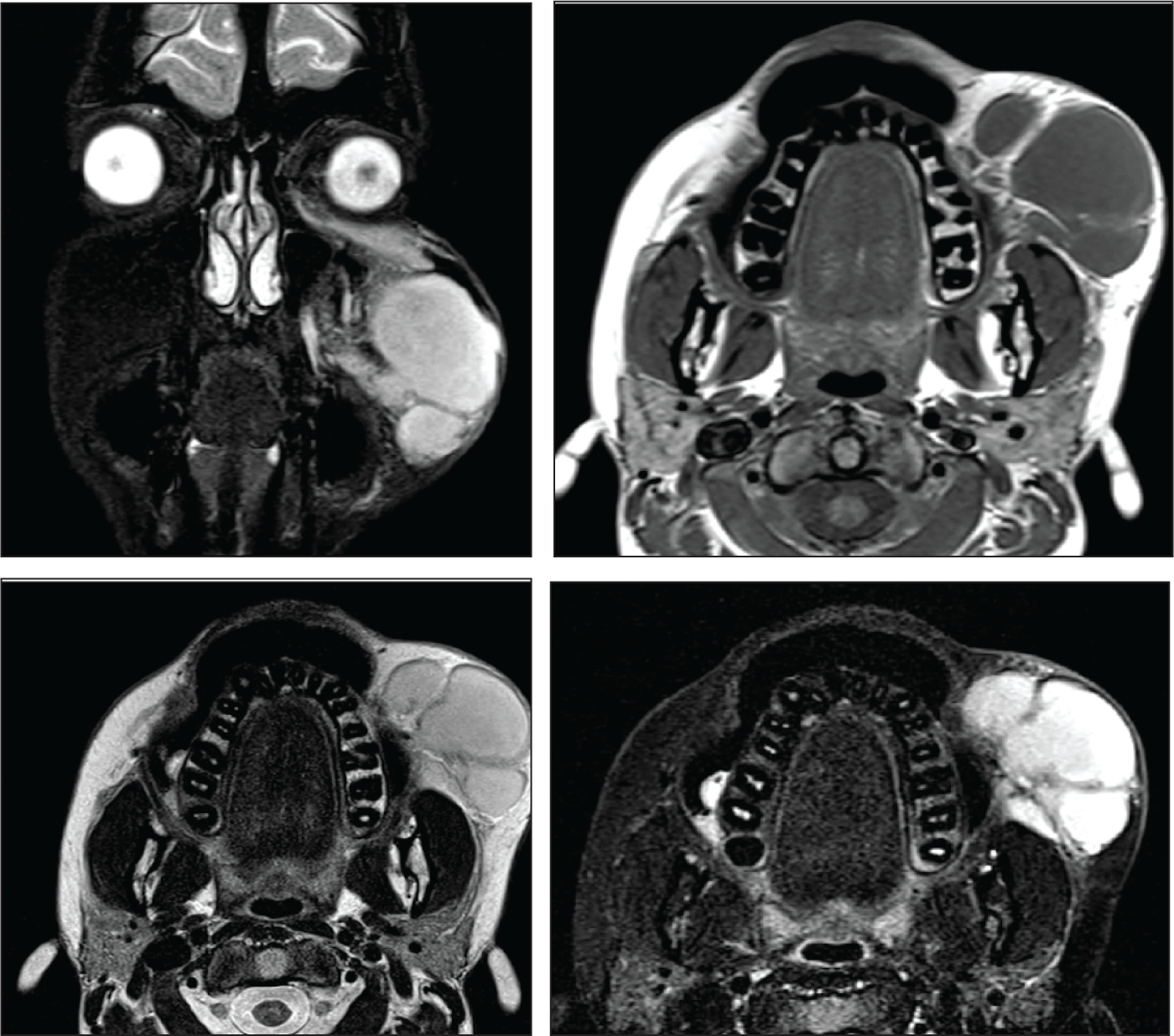
Her total leucocyte count was 11,770 cells/mm 3 with an absolute neutrophil count of 8120 cells/mm 3 and erythrocyte sedimentation rate (ESR) of 21 mm/hour. Blood cultures were negative, and all other haematological and biochemistry values were within normal limits. Ultrasound imaging showed a hyperechoic lesion measuring 4 × 2 cm, while Magnetic Resonance Imaging (MRI) identified a 2.7 × 4 × 7 cm peripherally enhancing lobulated cystic collection in the subcutaneous plane of the left premaxillary region (Figure 1). No extension into the orbit or communication with deeper facial structures was noted. The MRI also showed peripheral wall enhancement with a thickness of 2 mm, suggestive of an encapsulated collection.
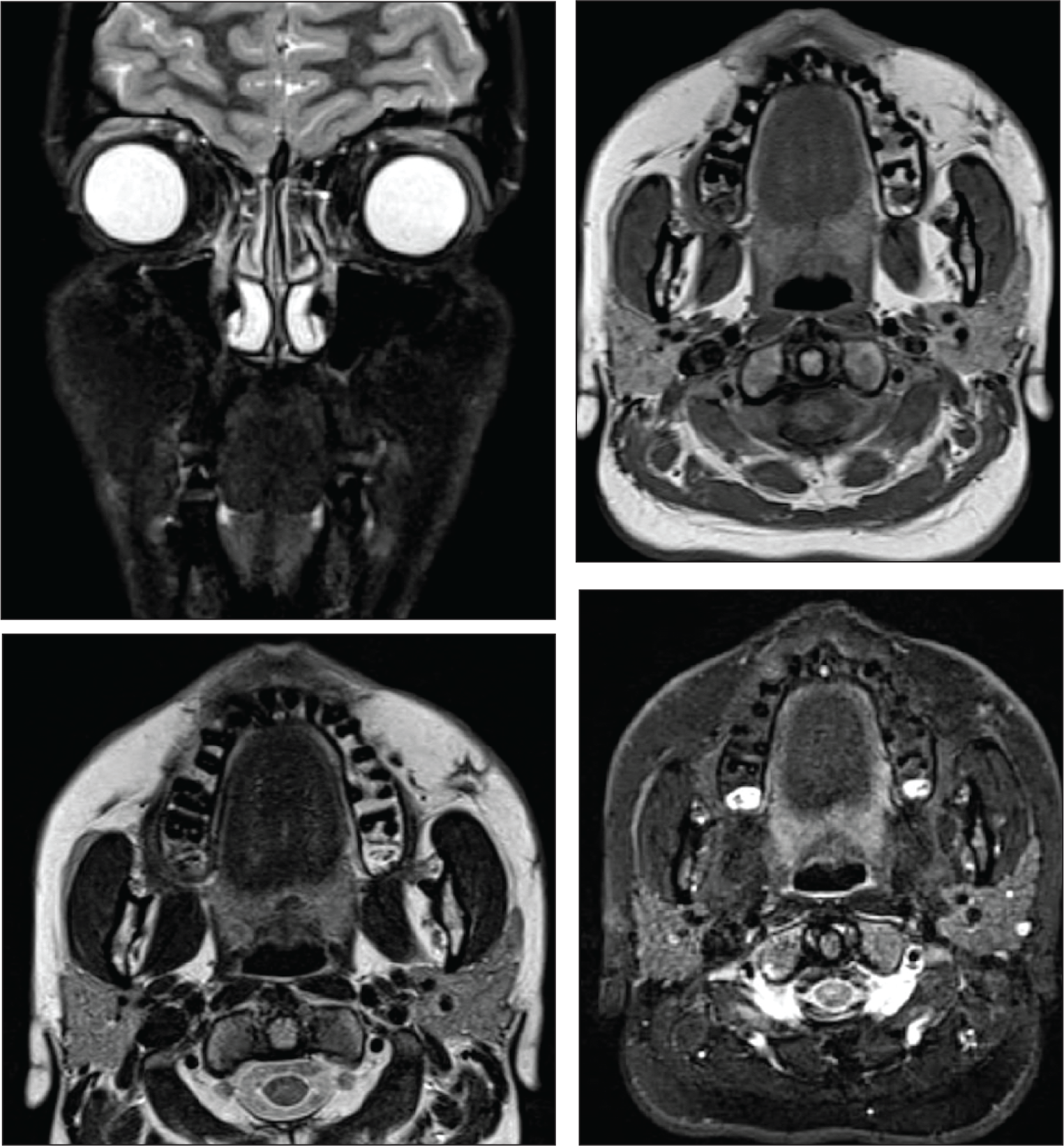
After reviewing the findings, surgical exploration was planned under general anaesthesia. A pre-auricular incision was made, and a sharp-tip cannula was used to create a subcutaneous plane to access the swelling. Upon perforation of the capsule, 50 ml of thick yellowish non-offensive fluid was noted. All the septations were broken with the cannula. The fluid was sent for aerobic and non-aerobic cultures. The cavity was irrigated with an antibiotic solution, small suction drain placed and the incision site closed. A 1-week course of oral 3rd-generation cephalosporin was given post-operatively. The culture reports came as negative and the patient recovered without complications (Figures 2A and 2B). Follow-up MRI revealed a 1.2 ml loss of volume on the left cheek as compared to the right, indicating the probable loss of subcutaneous fat at the site (Figure 3).
Preoperative MRI Showing the Extent of the Sterile Abscess.
(A) Preoperative Clinical Image with Swelling of the Left Cheek. (B) Complete Resolution of the Swelling After the Treatment. The Photograph Was Taken 6 Months After the Treatment.

Postoperative MRI Showing the Resolution of Sterile Abscess and Replacement with a Foci of Scar Tissue.
Discussion
Intralesional steroids are indicated in skin conditions where topical treatment is ineffective and systemic administration can lead to adverse effects. The solubility of an injectable steroid is inversely related to the duration of effect. Betamethasone and dexamethasone are more soluble steroids with a faster onset of action, but their systemic absorption can lead to adverse effects. On the other hand, triamcinolone acetonide is a less soluble steroid with a long-lasting effect and less risk of systemic adverse effects. 1 Among injectable options, triamcinolone acetonide is the most commonly administered intralesional steroid, especially in India. 2
Triamcinolone acetonide has been used as a common treatment modality for nodulocystic acne and can induce a significant reduction in the acne nodules owing to its anti-inflammatory effect. 2 While effective, intralesional steroids have been associated with potential adverse events like erythema, telangiectasias, secondary infections, hypersensitivity reactions, panniculitis, hypopigmentation, atrophy, and rarely Cushing syndrome. 1 Inadvertent injection of high concentration or amount, wrong site, and multiple doses can lead to these localised or systemic side effects. 3
There are limited reports of steroid-induced sterile abscess in literature, but none following the use of intralesional triamcinolone for the treatment of acne.4,5 As acne is a common skin condition affecting the adolescent age group, the possibility of this complication cannot be ignored. The possible reasons for the formation of sterile abscess could be due to the direct vasoconstrictor effect of steroid to reduce oxygen and nutrient flow to the site, reduction of endothelial growth factor, and lesser water solubility of triamcinolone. The culture proved to be sterile, probably due to the initiation of antibiotics as seen in other studies. 5 This case highlights a rare but significant complication of intralesional steroids for acne. Imaging findings were crucial in characterising the extent of the lesion, ruling out deep tissue involvement, and planning treatment.
Lessons Learnt
Triamcinolone acetonide is the most commonly injected intralesional steroid for varied skin conditions, especially nodulocystic acne.
Triamcinolone acetonide is a suspension, so it is essential to shake the solution before every use to prevent crystal formation in the tissues.
A small gauge needle (26-30G) should be used to inject triamcinolone into the target tissue in the right plane with minimum effective concentration and volume.
Although subcutaneous atrophy and hypopigmentation are common adverse effects of injectable steroids, sterile abscess/tissue necrosis is an inadvertent complication following injection of a high volume or dose of triamcinolone acetonide.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study participant provided informed consent prior to study enrolment. The research was conducted in accordance with the principles embodied in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent form has been attached as a supplementary file.