
Abstract
Introduction:
Theory and practice are complementary and have mutually reflective relationships supported by a robust feedback mechanism. Therefore, medical educators should ideally be familiar with various learning theories to use the most effective method for providing tailored instruction to learners. Unfortunately, pedagogical theories are not routinely used in designing and delivering medical education curricula. Therefore, the present study will discuss relevant pedagogical theories and construct a consensus-based conceptual framework for an authentic, evidence-based curriculum.
Methods:
A modified Delphi methodology was used to develop an agreement amongst experts on the relevant educational theories and overarching themes. The expert panel members (n = 36) were internationally recognised subject matter experts and programme directors with more than 20 years of experience in clinical teaching, curriculum design and delivery across the continents. The questionnaire included a short write-up explaining the main concepts of selected educational theories and was emailed using www.surveymonkey.net. A consensus was defined as an agreement score of ≥80% (mean = 4) and Cronbach’s a = 0.90, as recommended in the literature.
Results:
Members of the expert panel (Mean ≥4) agreed to include proposed educational theories and overarching themes in the conceptual framework (Cronbach’s a = 0.89 and 0.93), indicating a high internal consistency and reliability.
Conclusion:
This study proposes an evidence-based conceptual framework anchored on educational theories. This framework will serve as a road map for developing learning objectives, curriculum design, delivery strategies and assessment strategies for postgraduate non-surgical aesthetic education.
Keywords
Introduction
Evidence-based medicine (EBM) is the conscionable, precise and prudent application of sound science in decision-making for a patient’s benefit. The practice of EBM implies combining one’s clinical knowledge with concrete scientific evidence from controlled clinical trials and systematic research. Physicians are sensitive to the high standards of medical evidence, which are fundamental to guiding them in developing their speciality. On the contrary, physicians do not uphold the same evidence-based medical teaching and learning standards. Good science, such as peer review, rigour in quality control and continuous professional development, all of which are evident in clinical practice, are scarcely practised in medical education. The typically employed training methods are dominated by intuition and tradition, reflecting how physicians have been taught for decades.
With the advent of non-surgical aesthetic (NSA) procedures for enhancing one’s physical features, pharmaceutical and device companies have proactively entered NSA education. These programmes are mostly ‘show and tell’ and driven by the trainers’ perspectives, ‘this is how I do’, without employing any teaching and learning principles. 1 Such training programmes are based on the conviction that trainees will learn NSA procedures by observing experts. Moreover, most programme directors assume that the physicians they enlist as faculty for their programmes, who are recognised experts in their field, are equally qualified as teachers because of medical degrees, specialist certifications and demonstrated scientific ability. The assumption is that the better they are as clinicians, the better they are as teachers.
The issue is not whether the current practice in NSA education is substandard but whether it can be improved; teaching and learning in NSA education are too important to be left to chance. A recent integrative systematic literature review followed by a cross-sectional global needs analysis has established the need for an authentic evidence-based curriculum in NSA education. 2 Literature suggests that the foundation of an evidence-based curriculum should be on sound educational principles, encompassing how to inspire learners to reflect and actively participate in the learning process.3,4 It should be ensured that the curriculum is robust and flexible to meet individual learners’ varied needs. 5 Non-surgical aesthetic education can be designed based on educational theories with an ultimate objective to optimise skill development, knowledge mastery and behavioural changes.
The present study will discuss relevant educational theories for NSA education and construct a conceptual framework for delivering an authentic evidence-based curriculum.
Methodology
Literature Review on the Educational Theories
Every aspect of education design is deeply rooted in educational theories and philosophy, from curricular content to assessment, evaluation and practice to performance and action. 6 Implementing educational theories provides a robust foundation for promoting evidence and is critical to driving efficiency in clinical education. It is essential to apply theory to the real world of practice and ensure that trainee physicians are prepared for it.7,8 Educational philosophers and psychologists have hypothesised several theories to elucidate how learners attain, structure and employ knowledge and skills. Moreover, individuals may utilise various ways to acquire knowledge and skills; therefore, understanding one specific educational theory may not be adequate for educators. It is essential to develop an in-depth understanding of all the relevant educational theories to create an environment that can proliferate learning in NSA education. 4
Community Constructive Theory
Constructivism is a social theory of education derived from psychology; it describes the way individuals might develop skills and understanding. It has been established that thinking and learning are social activities and are very much affected by the environment. The principle of constructivism is anchored on the power of observation and suggests that individuals master their understanding and skills by assimilating information and reflecting on their experiences.9,10 Educational psychologists believe that learners develop new knowledge and insight based on their existing knowledge.11–13 It is thought that the theory of constructivism promotes critical thinking, conceptual growth, teamwork and enquiry, 14 which is the desired skill set to be successful as an NSA practitioner.
It is vital to highlight the importance of context and community for social constructivism 15 and essential to have a ‘Community of Practice’ (CoP) for continuously motivating and mentoring the learner.16,17 The theory of constructivism is very relevant for postgraduate NSA education and continuing professional development, where learners enrol with prior knowledge and skill sets. Notably, these learners will have their challenges, likings and experiences. One needs to remember that learning is built on the principle that cognition is the outcome of ‘mental construction’ and is greatly influenced by both the context in which a concept is introduced and the attitude and values of learners.
Situated Learning Theory
The classical paradigm of clinical and procedural skills mastery wherein trainees learn by shadowing the teachers is now replaced by a more modern internship approach based on the CoP. 17 Situated learning theory motivates learners to immerse in a contextual learning condition mirroring the actual clinical scenario where newly acquired knowledge and skills will be applied. When considered as situated learning, the principal defining element of learning is the process of ‘legitimate peripheral participation’. 16 Learners’ participation in the CoP is vital as the mastery of the skills does not sit with the master but instead with the community of which the master is a part. Situated learning theory and CoP sit with the idea of social constructivism and help during the skill development of NSA practitioners.
Adult Learning Theory (Andragogy and Heutagogy)
Adult learners want to co-create their learning journey and focus on the immediate gain in their personal and professional life from educational activities.18–20 The content theory focuses on what motivates an adult learner, and the process theory examines how an individual gets motivated. 21
Heutagogy, or the theory of autonomous learning, is a self-determined learning concept that originated from andragogy and is entirely concentrated on developing the learners’ competence. Thus, the learner acts as ‘the main agent in their learning, which occurs due to personal experience’. 22 The idea of self-determination incorporates several specific concepts or practices considered to resolve current educational challenges and constraints and offer improvement, mainly in an evolving work climate.
Moreover, applying adult learning theory (andragogy and heutagogy) in NSA education demands a change in learners’ and educators’ attitudes to improve efficiency. Both must actively participate in the learning process where educators need to consider themselves as both learner and teacher, whereas learners need to become active in knowledge construction by changing their beliefs and views. It is vital to have mutual respect between the teacher-learner and the learner-learner to reap the full benefit and behavioural change from an active learning environment.
Learning Styles
In postgraduate education, the most significant challenge is developing evidence-based clinical expertise and decision-making skills in trainee physicians relatively quickly. Moreover, reduced work hours and increasing responsibility for ‘documentation and noneducational work’ further drift residents from gaining enriched clinical experience. 23 Thus, clinical educators must formulate a strategy to gain insight into trainees’ learning styles and adapt their teaching to enhance the learning experience effectiveness. Evidence from medical education literature suggests the wide use of Kolb’s experiential learning theory across several specialities such as anaesthesiology, surgery, paediatrics, plastic surgery and internal medicine24,25 and may be advantageous to NSA educators.
Experiential Learning
Experiential learning can be described in very basic terms as ‘learning through experience’. Aristotle elaborated his view on learning in The Nicomachean Ethics; ‘for the things we have to learn before we can do them, we learn by doing them’. 26 The concept of experiential learning within clinical education for developing clinical skills in trainee physicians is well recognised. In his book Experience and Education, John Dewey argued for a ‘progressive approach’ to teaching and emphasised the relevance of experience for effective learning. 27
Clinical clerkship is an essential and challenging aspect of postgraduate clinical education for learners and clinical educators. Evidence suggests that understanding and learning styles matching Kolb’s experiential learning model during the clinical rotations can enhance learning effectiveness in trainee physicians. Further, Kolb has emphasised the power of reflection as a way for learners to create, abstract and transfer their new knowledge to a newer context. 28 Non-surgical aesthetic education can immensely benefit from employing experiential learning while facilitating learning during simulations and hands-on sessions.
Activity Theory
The work of Yrjö Engeström is particularly relevant to activity theory (AT)’s Scandinavian school of thinking, which is the one that has been referenced most in the literature. Engeström took Vygotsky’s older notion of mediation and reinterpreted it to embrace learning with others through using and interacting with artefacts (Scandinavian Activity Theory). Engeström’s approach focused on explaining human thought processes by considering how they relate to human behaviours in different contexts and considering the extent to which human activity impacts the environments in which these activities occur. 29
Individuals utilise exterior (e.g., surgical knife, hammer, computer and vehicle) and internal (e.g., planning and cognitive mapping) instruments to accomplish their objectives when performing an AT task. In the social realm, many objects have cultural and social importance. Activities should be relevant and iterative to keep students engaged and motivated so that the community of learners may collaborate and collectively increase their knowledge. Equally, educators should know that technology has the ability to both restrict and support social connections; thus, it should be employed judiciously and specifically to help students achieve their maximum potential. 30
Critical Thinking
Critical thinking is the most sought-after skill across an individual’s learning journey and is rated as an essential skill for workplace survival in the twenty-first century. The importance of critical thinking can be seen across the disciplines as we see an increased emphasis on enquiry- and problem-based learning. Francis Bacon defines, ‘Critical thinking is a desire to seek, patience to doubt, fondness to meditate, slowness to assert, readiness to consider, carefulness to dispose and set in order; and hatred for every kind of imposture.’ 31 Black defines it as a cognitive dialogue to build arguments based on analysis and evaluation. 32 Facione elaborated critical thinking as a determined, self-regulatory injunction that includes construction, diagnosis and assessment of the decision’s context. Further, theorists have argued for strong coordination between pedagogy, curriculum and assessment strategies to promote critical thinking. 33
Clinical Reasoning
Clinical reasoning is an essential competency required for clinicians to make logical decisions while dealing with patients. It requires a strong understanding of evidence-based medical and scientific knowledge. It involves both rational and metacognitive reasoning (or analysis) and relies on analytical thinking. The approach of clinical reasoning delivers an immersive paradigm designed to accurately explain and solve clinical issues, along with a set of well-conceived, focused examples that explore clinical reasoning, help trigger rational thought and provide innovative treatment. 34 It is noteworthy that clinical reasoning occurs within social settings, often about the patient, caregivers and healthcare workers. Physicians find themselves operating in the circle of relatives who have concerns regarding the patient and his/her health outcome.35,36 Clinical reasoning skills help trainees formulate a proper treatment plan for patients seeking NSA procedures. Therefore, it is essential to have profound clinical reasoning for running a safe clinical practice.
Clinical Judgement
The Royal College of Physicians elaborated on the medical profession as ‘a vocation in which a doctor’s knowledge, clinical skills, and judgment are put in the service of protecting and restoring human well-being’. 37 Therefore, clinical judgement becomes the core of a clinician’s profession and is crucial for performing his/her role. Insights, deliberate practice, training, understanding and consistent logical reflection enrich clinical judgement skills. It applies to all the areas of medical sciences, such as investigation, treatment planning, patient–physician communication and decision-making. 38 A central and strategic philosophy to be remembered is the theory of judgement. This includes clinical logic, judgement and its interaction, and interdependence with other educational philosophies in NSA education practices.
Reflective Learning
‘Reflection is a metacognitive process that occurs before, during, and after situations to develop a greater understanding of both the self and the situation so that future encounters with the situation are informed from previous encounters.’ 39 Reflective learning theory considers that one’s critical reflection leads to action and subsequently results in behavioural change. Reflective learning40,41 has a significant role in clinical education. 42 Reflective learning enables learners to fill the gap between ideas and obligation, authority and knowledge, thought and action, as well as theory and practice. 43 Reflection as a way of exploration is critical to experiential learning and professional development. It is often challenging to connect classroom learning and actual clinical practice without adequately reflecting on one’s actions. Reflection helps the learners in more in-depth learning and problem-solving and encourages them to take meaningful actions. 44
A reflection is an influential tool for critically appraising hypotheses and perceptions of self, fellow clinicians and patients, helping solve a clinical problem and decision-making. There is a growing consensus amongst medical educationalists to include critical reflection across the graduate and postgraduate curricula.45–47 In the clinical education literature, it has been very aptly argued that critical reflection is an essential skill for trainee physicians.48,49
Critical reflective theory perfectly fits into the conceptual framework for NSA education as it allows the learners to think critically about an event and develop a newer perspective.
Shared Decision-making
Compared to physicians making decisions on behalf of patients, shared decision-making (SDM) is gaining more importance in healthcare policy.50,51 Shared decision-making has been described as a method in which the best available data are shared between the physician and patient while making mutually agreeable decisions and empowering the patient to explore alternative options. 52 The SDM strategy includes a massive effort to encourage patient-centred treatment. It cares about the patient’s interest in the clinical aspects and respects patients’ ability to make choices regarding their well-being. Further, SDM supports patients in forming an educated and individualised opinion about their care. 53 Shared decision-making concepts are well known, but implementing them into regular clinical practice is challenging and requires conscious effort from the institutions. It is the physician’s responsibility to establish trust during the consultation process so that patients can feel comfortable expressing their desire and concern. A three-step framework is suggested to achieve the SDM objective, anchored on preference, options and decision-making methods.
Professional Identity Formation
Professional identity is defined as the ‘stable and enduring constellation of attributes, beliefs, values, motives and experiences in which people define themselves in a professional role’. 54 The ultimate aim of medical education is to transform a trainee into a qualified medical professional. Based on the idea of ‘CoP’, Lave and Wenger’s theory defines learning as an enhanced engagement in social and cultural activities in an atmosphere where participants share a common mission. Learners build their identity through socialisation with a new social language that involves learning to walk and talk. In this regard, the driving force behind confirmation of identity is based on the need for social recognition that allows individuals to engage in societies to which they belong.55,56 Since NSA practitioners come from varied training backgrounds, professional identity formation (PIF) can be handy in developing a sense of belongingness and ‘CoP’.
These educational theories have generated several important sub-theories which inform more than one theory. Therefore, after careful examination, educational theories and sub-theories were grouped into four overarching themes: enquiry-based learning, skills acquisition, professional identity and shared decision-making. Furthermore, overarching themes were analysed and elaborated into overlapping themes, such as critical thinking, values and attitude, information mastery, work-based learning, regulations and ethics.
Modified Delphi
A modified Delphi methodology was employed for developing the agreement on the relevant educational theories and overarching themes between NSA education experts.
Expert Panel
An expert panel was recruited following the steps discussed in the literature. 57 The expert panel members were globally recognised subject matter experts and programme directors (n = 36) with over 20 years of experience in clinical teaching, curriculum design and delivery across the continents.
Questionnaire Development
A questionnaire was developed based on the educational theories discussed in the earlier section. The questionnaire consisted of a short write-up on selected educational theories explaining the main concepts, followed by the corresponding survey question. Survey questions were sent to experts via email using www.surveymonkey.net by momentive.ai. San Mateo, CA, United States. The experts were asked to respond on a 5-point Likert scale (1, strongly disagree; 2, disagree; 3, neither disagree nor agree; 4, agree; 5, strongly agree). Moreover, experts were requested to provide suggestions, if any, to include them in the subsequent rounds.
Determination of Consensus
As recommended in the literature, an agreement score of ≥80% (mean = 4) and Cronbach’s a = 0.90 were set to represent a consensus.
Data Collection
Delphi Round 1
The first email invitation to the expert panel triggered the consensus-building process. The panel members were requested to rate the most relevant educational theories and regulations.
Delphi Round 2
During the second round, experts received the items and the first-round ratings. They were asked to revise their judgement or elaborate on the reason for disagreement from the group opinion. This round provides an opportunity for experts to rethink and adjust their feedback.
Delphi Round 3
Since trainee physicians are critical stakeholders, the outcome of the second round was presented to them (n = 16), and they were asked to express their views on each item.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Mac, Version 27.0 (IBM Corp. Armonk, NY, USA). The relevance of each educational theory was determined by calculating the mean score, while internal reliability was determined by Cronbach’s a.
Result
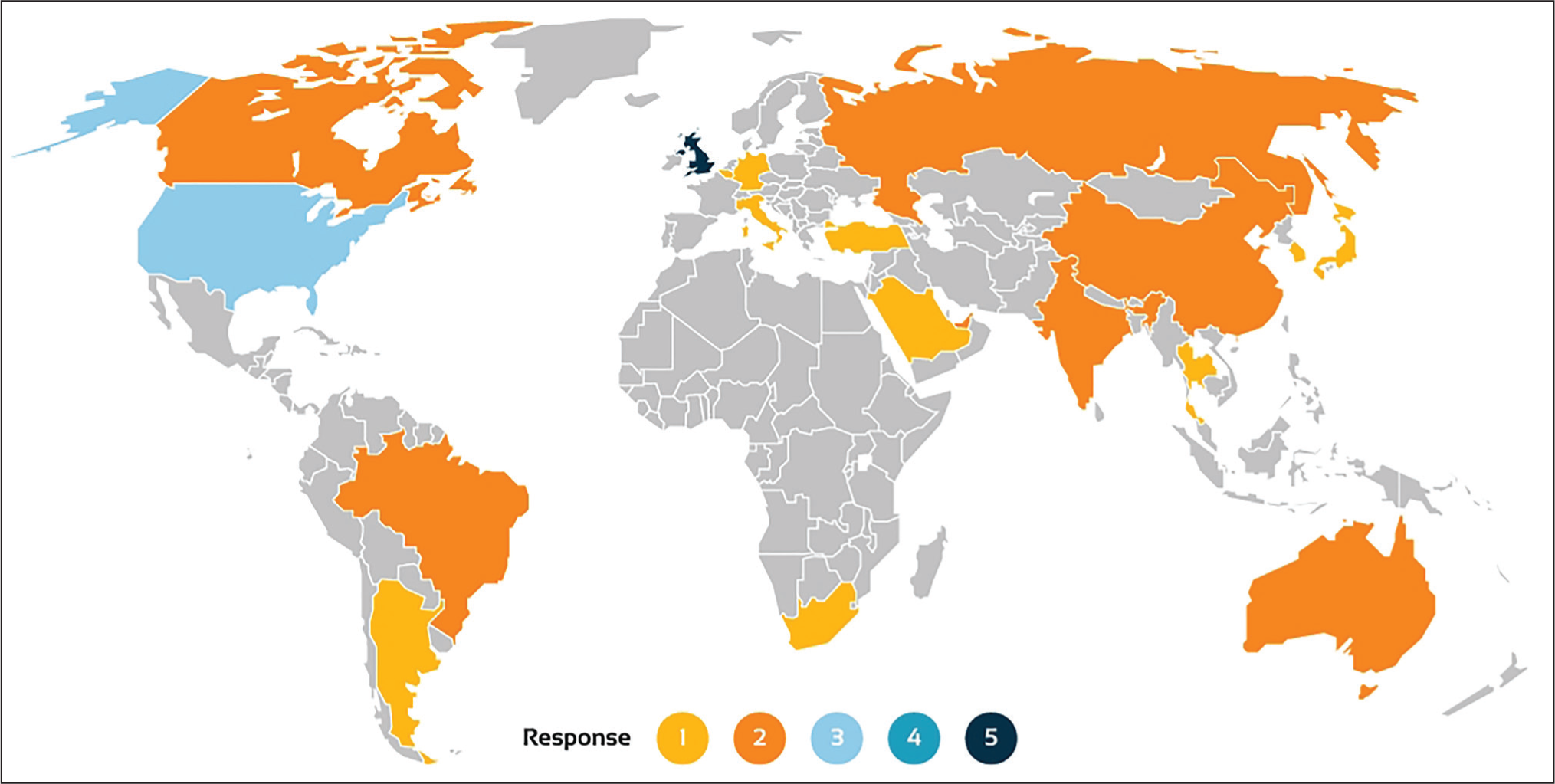
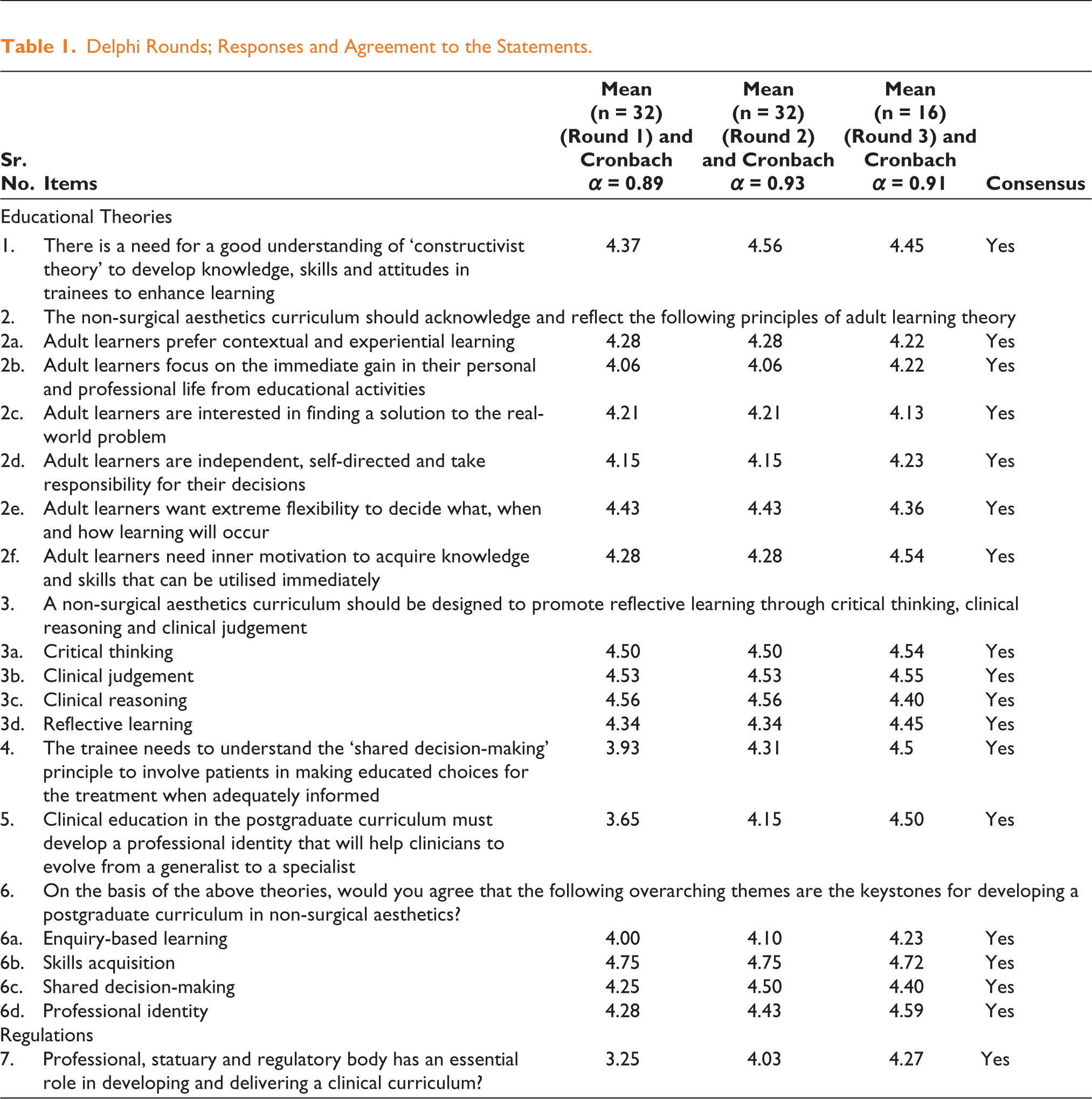
The overall response rate in the expert group was 89% (n = 32). The geographical distribution of the respondents is presented in Figure 1. The expert panel agreed (Mean ≥ 4) to incorporate proposed educational theories and the overarching themes for the conceptual framework. Cronbach’s a for the first Delphi round was a = 0.89 and for the second round, it was a = 0.93, which showed a high internal consistency and reliability level Table 1.
Geographical Distribution of Responders (n = 32).
Delphi Rounds; Responses and Agreement to the Statements.
Conceptual Framework
For curricular growth, the fundamentals on which the content, curriculum design, evaluation and assessment, and expected educational results are based must be explained. 58 However, the fundamental resumes (plastic surgery, dermatology and dentistry) lack sufficient technical clarity to support the proposed NSA curriculums, contributing to current practice. To establish such a vision, it was essential to participate in a broad and critical dialogue with the professional community.
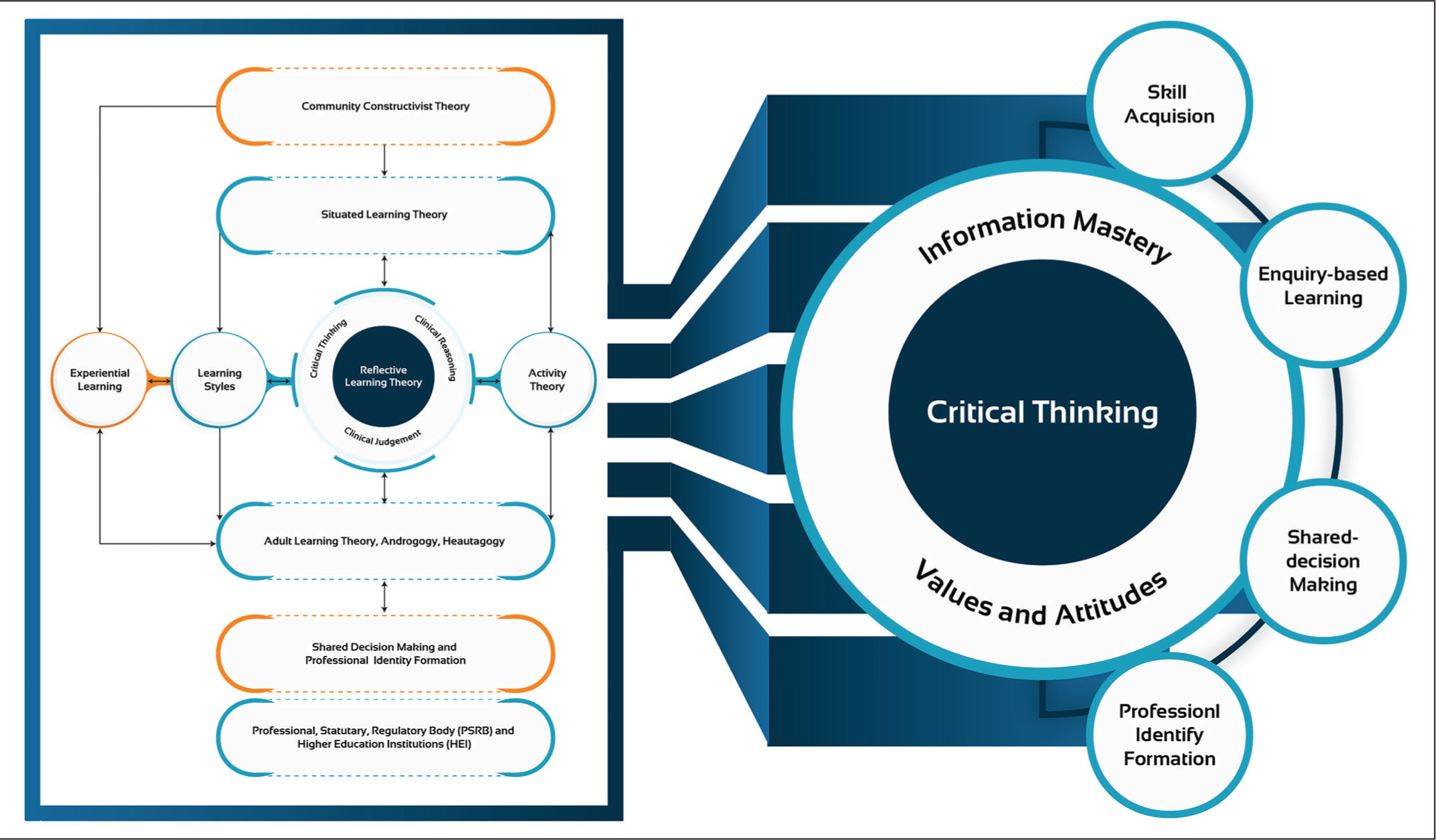
The proposed conceptual framework is driven by a specific philosophy of constructivism while linking all the educational theories and overarching themes (Figure 2). This futuristic conceptual framework covers dynamic societal change, the evolving educational environment and patients’ interests. Further, it offers a general overview of each educational theory and template to design, develop, implement and evaluate the NSA curriculum. Finally, it will enable programme directors and policymakers to participate in an analytical, regulated and application-oriented process that promotes education fidelity through the theoretical approach.
Conceptual Framework.
Discussion
‘There is nothing so practical as a good theory.’ 59 Theory and practice have complementary and mutually reflective relationships supported by a robust feedback mechanism—new insights generated from the practice help refine the theory. Medical educators should ideally be conversant with various learning theories to adopt the most effective method for delivering bespoke teaching to learners. 6 Moreover, it is unfortunate to see that educational theories are not routinely employed in curriculum design and delivery in medical education. 60 This is the first study to build a consensus to develop an authentic and evidence-based conceptual framework for NSA education anchored on critical educational theories.
Adult learning theories (andragogy and heutagogy) are very relevant in NSA education and help create the most hospitable environment for the proliferation of learning. Adult learners are ostensibly independent and self-directed and have inner motivation to acquire knowledge and skills that can be utilised immediately in their clinical practice. With its student-centric approach, heutagogy shifts the epicentre from the educator to the learner and the learning process. Therefore, this theory supports the twenty-first-century learner who takes control of his/her learning by addressing the gap in knowledge and skills by following an enquiry-based learning approach. To succeed, these learners must be accommodative, flexible and have good communication skills to collaborate with their learning networks. Evidently, heutagogy is anchored in constructivist and humanistic principles and connects with several other educational theories into an integrated collage of learning fit for NSA education.
Constructivist theory provides people with new perspectives, judgements, thoughts, knowledge or behaviour within their position as learners. It begins with the presumption that thoughts can only be constructed according to past experience and what they know. 61 The analysis and reflection that enable individuals to draw new conclusions and add new meanings to their comprehension are included within these activities. During education, both collective learning and independent learning take place. This connects to the methods and approaches of education and practice. Building on and interacting with other educational ideas offer a robust learning base. Since constructivist learning resonates strongly with skills-based clinical education, it offers opportunities to deconstruct and recreate previous perspectives and practices and construct new ones. Therefore, the constructivist learning approach can be of interest for teaching complex skills such as problem-solving or critical-thinking skills, 62 which are extremely important in NSA education.
The established system of procedural skill attainment by observing the teacher has been replaced by a more modern approach to clinical clerkship, and mostly learning occurs at the workplace. Work-based learning is valuable for NSA education, is based on heutagogy and grants enough autonomy to learners to explore their passion for building new knowledge and skills. Similarly, action learning and action research permit the learners to experiment with real-world experiences, and subsequently, learning can be evaluated in the following learning cycle. Moreover, a case log or case portfolio commonly used in postgraduate clinical education can be used in NSA education as an effective reflective and experiential learning tool.
It is evident from the Delphi consensus that the NSA curriculum should actively help in building the SDM approach in trainee physicians. Shared decision-making is one of the crucial pillars of EBM and fits very well within the NSA curriculum due to the availability of several treatment options. Moreover, these elective procedures are driven by individuals’ motivation and desire to improve their corporeal features and affect the final decision-making. However, since NSA procedures are self-pay driven by market economics, it is prone to get compromised. Therefore, the patient’s values and perspectives are highly significant in the decision to undertake aesthetic procedures and should be considered in the decision-making process for treatment planning. Therefore, developing the right attitude and culture to promote SDM in present and future physicians is essential to effectively communicate the pros and cons of a procedure. Such practice will encourage patients to get involved in SDM, and patients can make education choices once fully informed. 63 Shared decision-making can be actively developed and promoted in trainee physicians through CoP and PIF.
The Delphi panel agreed to include PIF in the non-surgical curriculum. Professional identity formation is a relatively new concept in medical education and focuses on developing professionalism in new physicians. The idea is to develop the right values, attitudes and characters in trainee physicians through socialisation. 64 Professionalism is an interpersonal mechanism that considers, establishes and implements a hierarchical relationship with others. Individual characteristics remain crucial; however, they are not set between individuals but mutable and co-created. 65 Medical education requires professional discourses for unveiling the hidden curriculum, allowing students to recognise and combat the curriculum’s adverse impact.66,67 In the context of NSA education, trainees should participate in ‘the community’ and adopt an enquiry-based approach to problem-solving to build new knowledge and skills. Moreover, through its participatory sociocultural practices, ‘CoP’ actively promotes the PIF in new learners.
Further, the expert panel recognise the critical role of professional, statuary and regulatory bodies in developing and delivering the NSA curriculum. Since NSA is a new and evolving field in medical sciences, trainee physicians must be appropriately trained on ethics and existing regulations.
Conclusion
The study gives the collective evidence produced around education theories to guide NSA educators to standardise the training and education for the next generation of a esthetic physicians. Further, it proposes the conceptual framework, which will act as a guiding map for developing the learning objectives, curriculum design, delivery and assessment strategies in NSA education.
Footnotes
Acknowledgements
The research for this article was done as part of a PhD thesis at the University College London, United Kingdom. The authors sincerely thank all the experts for participating in the Delphi panel.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this articles research, authorship and publication.
Funding
The authors received no financial support for this article’s research, authorship and publication.