
Abstract
Introduction:
Breast reduction surgery, or reduction mammoplasty, is a procedure aimed at correcting both functional and aesthetic concerns associated with macromastia. The surgery not only alleviates these symptoms but also corrects breast to body proportion and boosts self-esteem. One of the essential aspects of surgical planning is the selection of an appropriate vascular pedicle, which determines the perfusion of the nipple–areolar complex (NAC) and overall surgical outcomes.
Methods:
Multiple pedicle techniques are described, each with their advantages, limitations and varied clinical indications. According to our study, the superior and superomedial pedicle-based techniques are preferred for maintaining upper pole fullness, whereas the inferior pedicle is widely used for its reliable blood supply, especially in large breast reductions. Selecting the ideal pedicle is influenced by patient anatomy, breast size, degree of ptosis and surgeon expertise. Optimal aesthetic outcome is the goal unless the patient has significant comorbidity or a high body mass index (BMI) where ensuring vascularity of the pedicle and NAC viability takes priority.
Conclusion:
In conclusion, this article provides a guideline for choosing the right pedicle, focusing on their anatomical considerations, surgical implications and postoperative outcomes. Additionally, we have discussed the risk mitigation strategies to reduce complications of surgery. A systematic approach to pedicle selection improves surgical precision, reduces surgical complications, enhances patient satisfaction and ensures better long-term aesthetic and functional outcomes. However, there is no just the one pedicle which is ideal for all patients. The best is the one which a surgeon can perform comfortably and safely.
Keywords
Introduction
Reduction mammoplasty is a true interface between reconstructive and aesthetic surgery, designed to decrease breast volume while maintaining shape, function and vascularity. Large breast size, or macromastia, often causes significant physical and psychological distress, including musculoskeletal pain, skin irritation or rashes, infection in intertriginous areas and restrictions in physical activities. Breast reduction surgery aims to tackle these problems while achieving more mature and pendulous breast shape that is in proportion to the body size of the patient and is also aesthetically pleasing. 1 Optimal aesthetic outcome is the goal unless the patient has significant comorbidity or a high body mass index (BMI) where ensuring vascularity of the pedicle and nipple–areolar complex (NAC) takes priority. 2
The surgical success of breast reduction largely depends on the choice of vascular pedicle, which ensures adequate blood supply to the NAC and parenchyma. The ideal pedicle should provide adequate perfusion, preserve nipple areola sensation while allowing necessary tissue resection and reshaping. Various pedicle techniques have been described over time, each with their own merits and demerits. Each is deployed depending on patient anatomy and surgical goals.
The commonly described pedicles include the superior, the medial, the superomedial and the inferior pedicles.3–8 The superior and superomedial pedicles are advantageous in maintaining upper pole fullness, but are often limited in their ability to support extensive tissue resection.9,10 The inferior pedicle is widely used for large reductions due to its reliable vascularity. 8 Medial and lateral pedicles offer targeted shaping benefits, whereas the central pedicle provides a robust and versatile option but with practical limitations.
Numerous factors influence selection of the pedicle including breast size, degree of ptosis, NAC position, expected volume of resection, age, patient comorbidities and the surgeon’s experience. Proper planning and meticulous surgical technique are essential to eliminate complications such as NAC necrosis, loss of sensation and aesthetic deformities. This article aims to provide a detailed analysis of pedicle options in breast reduction surgery, guiding surgeons towards proper decision-making for optimal patient outcomes.
Materials and Methods
In the Indian scenario, most patients seeking breast reduction present with larger breast sizes. For the novice surgeon, the need for a robust pedicle with reliable vascularity is crucial to prevent complications. This typically led to an increased preference for the inferior pedicle. Many of these patients have a high BMI, which further increases the risk of surgery. Additionally, darker skin tones often lead to visible and poor scarring.
Numerous pedicle techniques have been described in the literature, including bi-pedicle, random-pattern, medial and lateral pedicles. However, these techniques hold more of a historical perspective than practical utility in breast reduction surgery. The popularity of superior, superomedial and inferior pedicles has largely outdated other methods due to their superior vascular reliability and aesthetic success.
Selection of Vascular Pedicle Criteria
Based on amount of resection and size (Figure 1 and Table 1).
Upper breast border.
We prefer to use the upper breast border (UBB) as a measurement guideline to determine the new nipple position. The new nipple position is typically 8–10 cm below the UBB. Thus, the variability of patient height in nipple placement is eliminated and aesthetic breast reduction can be planned based on the breast footprint. We prefer the superior pedicle when the nipple position is moved up to the new position by 5 cm or less. This usually lends to a circum–areolar scar or a circum–areolar with a short vertical (lollipop) scar. Breast footprint decides the postoperative position of NAC as repositioning of complete breast on the chest wall is not possible.
Aesthetic considerations: Better medial fullness—superomedial pedicle.
Choice of Vascular Pedicle Depending on Expected Amount of Resection and Breast Size.
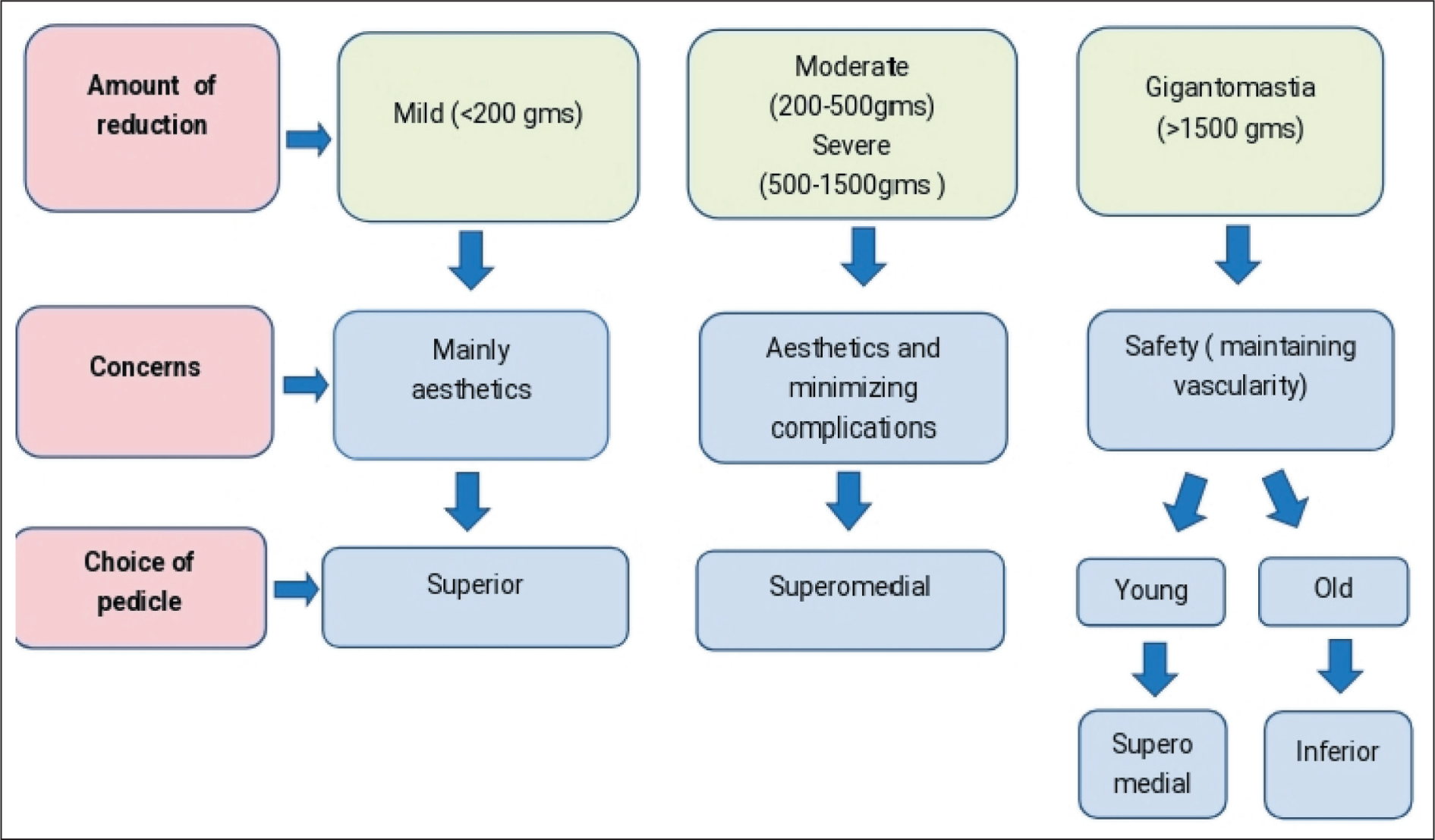
Classification of Breast Hypertrophy According to Amount of Reduction.
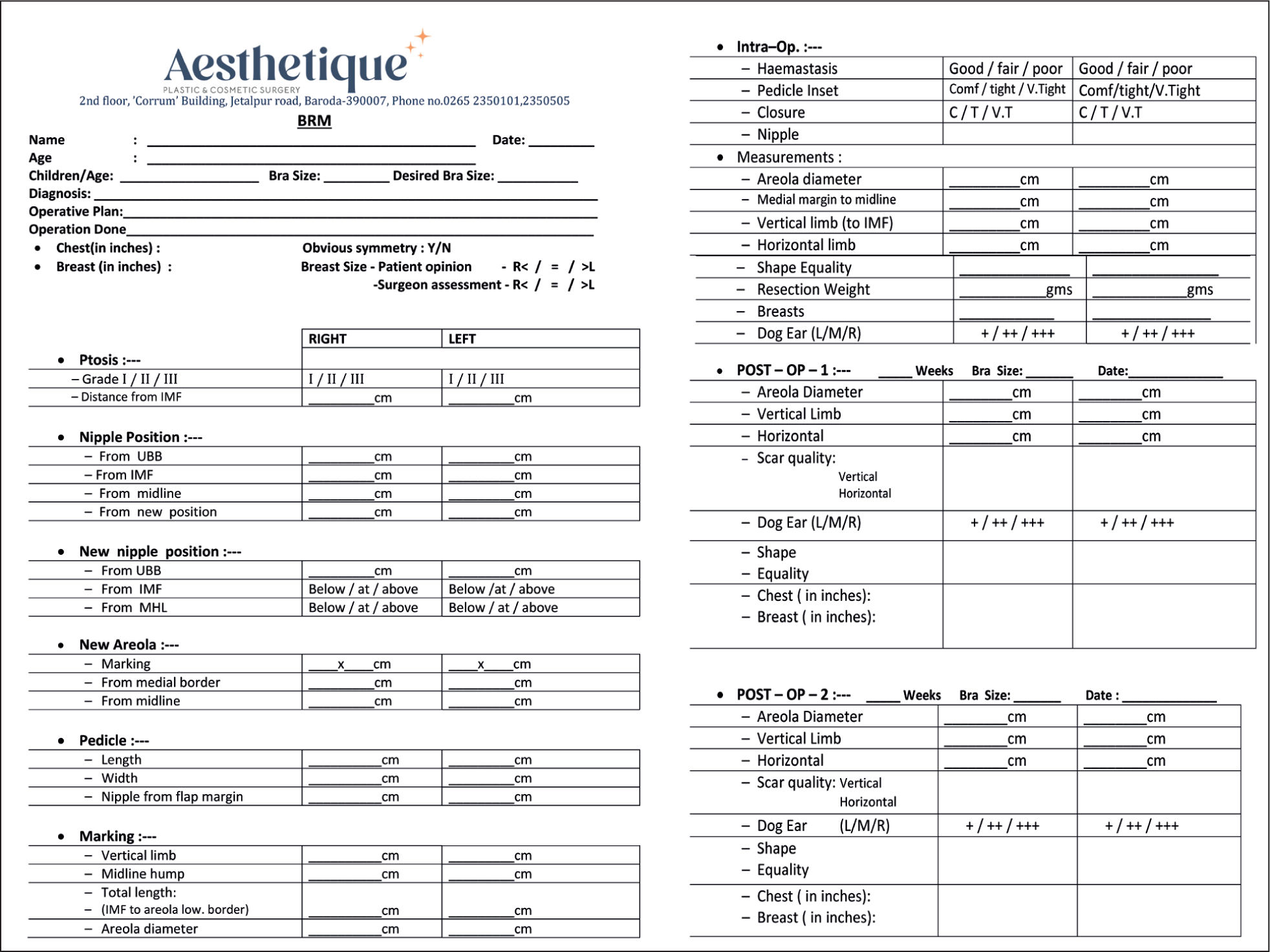
Preoperative assessment of breast shape, breast footprint, asymmetry and markings is crucial for accurate tissue resection and pedicle preservation, which are done in a standard stepwise manner and recorded. The procedure begins with skin incisions according to the chosen pattern (e.g., wise, vertical or circum-areolar). Skin excision technique whether vertical scar or inverted-T shaped technique is chosen according to amount of resection and skin excess. The pedicle is carefully dissected, ensuring adequate vascular supply for maintaining NAC viability. The pedicle is always extended beyond the areola by at least 2–3 cm by taking a cuff of breast tissue (Swartzman manoeuvre). Excess glandular and fatty tissue is excised, and the breast is reshaped. The NAC is positioned according to preoperative planning, ensuring symmetry. The incisions are closed in layers. The closure should be relatively tension free. Particular attention is paid to strict haemostasis which has helped eliminate the routine use of postoperative drains in our practice. All the preoperative, intraoperative and postoperative data are recorded in the format shown below (Figure 2). Breast reduction for gigantomastia with free nipple graft was never required.
Case Record Proforma for Preoperative, Intraoperative and Postoperative Evaluation.
Results
Results of different pedicle techniques based on above-mentioned criteria are shown in Figures 3–6. Results were qualitatively assessed for patient satisfaction and aesthetic outcomes. The inferior pedicle technique was most commonly chosen for gigantomastia cases, providing stable long-term results with minimal risk of NAC compromise. 8 The superomedial pedicle was associated with better upper pole fullness and a more youthful breast contour, while the superior pedicle was preferred in cases requiring minimal tissue excision without significant breast ptosis.3,4 Postoperative assessment was done by noting the breast measurements and by the incidence of major and minor complications. Major complications, including those reported in literature, were NAC necrosis (partial or total), haematoma, wound dehiscence, breast asymmetry, excessive bottoming-out, severe infections and deep vein thrombosis (DVT). Minor complications included delayed wound healing, hypertrophic scars or keloids, temporary or permanent loss of nipple–areola sensations, bruising or swelling, mild asymmetry, fat necrosis, itching or sensory changes. These findings underscore the importance of pedicle selection based on patient-specific needs.
A 45-year-old E Cup Breasts, Operated by Superomedial Pedicle Technique, Respected 1,000 g Per Side. Pictures Showing Preoperative and One Year Postoperative Photos. The Breast Footprint Is High as Seen in Preoperative, So the Lift and Upper Pole Fullness Appear More Postoperative.

A 37-year-old E Cup Breast, Operated by Superomedial Pedicle Technique, Respected 1,900 gm from Left Side and 2,000 gm from Right Side. Pictures Showing Preoperative and One Year Postoperative Photos.

A 32-year-old G Cup Breast, Inferior Pedicle Technique, Resected 1,800 gm from Left and 2,000 gm from Right. Pictures Showing Preoperative Marking, Intraoperative Pedicle Length >20 cm and One Year Postoperative. It Could Achieve a Significant Reduction as Per Patients Desire by Thinning the Pedicle. Good Postoperative Symmetry Is Achieved.

A 58-year-old, Needing a Pedicle Lift of 5 cm Coupled with a Minor Reduction, Achieved with a Superior Pedicle Technique. Significant Residual Skin Laxity, Age and Skin Quality Dictate the Decision for Inverted T Incision.

Long-term Results
NAC sensation: Sensation was retained in most patients, with the majority regaining normal sensation. Some had a reduced sensitivity, while others did have hypersensitivity. There was no pedicle bias in the outcome.
Breastfeeding: In our centre, coincidentally all women in the childbearing age group had undergone reduction with the superomedial pedicle technique. A survey of those who went through a subsequent pregnancy showed that 25% could not lactate, 25% lactated inadequately, while the others had adequate lactation.
Discussion
The vascular supply of the breast primarily consists of branches from the internal mammary artery (internal thoracic artery) and lateral thoracic artery, with intercostal perforators. 11 The inferior and central pedicle techniques rely on deep vascular and dermal vascular networks, while the superior and medial pedicles preserve branches from the internal mammary system. Proper selection of the pedicle is essential to ensure adequate perfusion, preventing ischaemic complications. In terms of innervation, the breast derives sensory input from the fourth to sixth intercostal nerves. The preservation of these neural pathways is critical in maintaining NAC sensation postoperatively. Proper pedicle selection and avoiding excessive dissection can minimise chances of sensory loss, improving patient satisfaction and long-term outcomes.
The surgical goals include achieving pleasing appearance, adequate size and form, minimal scarring and a low complication rate. Good surgical results mainly depend on meticulous planning, detailed marking and execution of the plan. 12 Challenges, while performing breast reduction surgery, for novice surgeons include choosing a proper technique from the bouquet of options available; for established surgeons the challenge is avoiding the complications and those for domain expert is achieving superior breast aesthetics. Reasons for poor aesthetic outcomes in breast reduction surgery are 1. faulty surgical designs and 2. following complications, both of which are ultimately related to vascularity. Thus, choosing the right pedicle is the key in achieving better aesthetics.
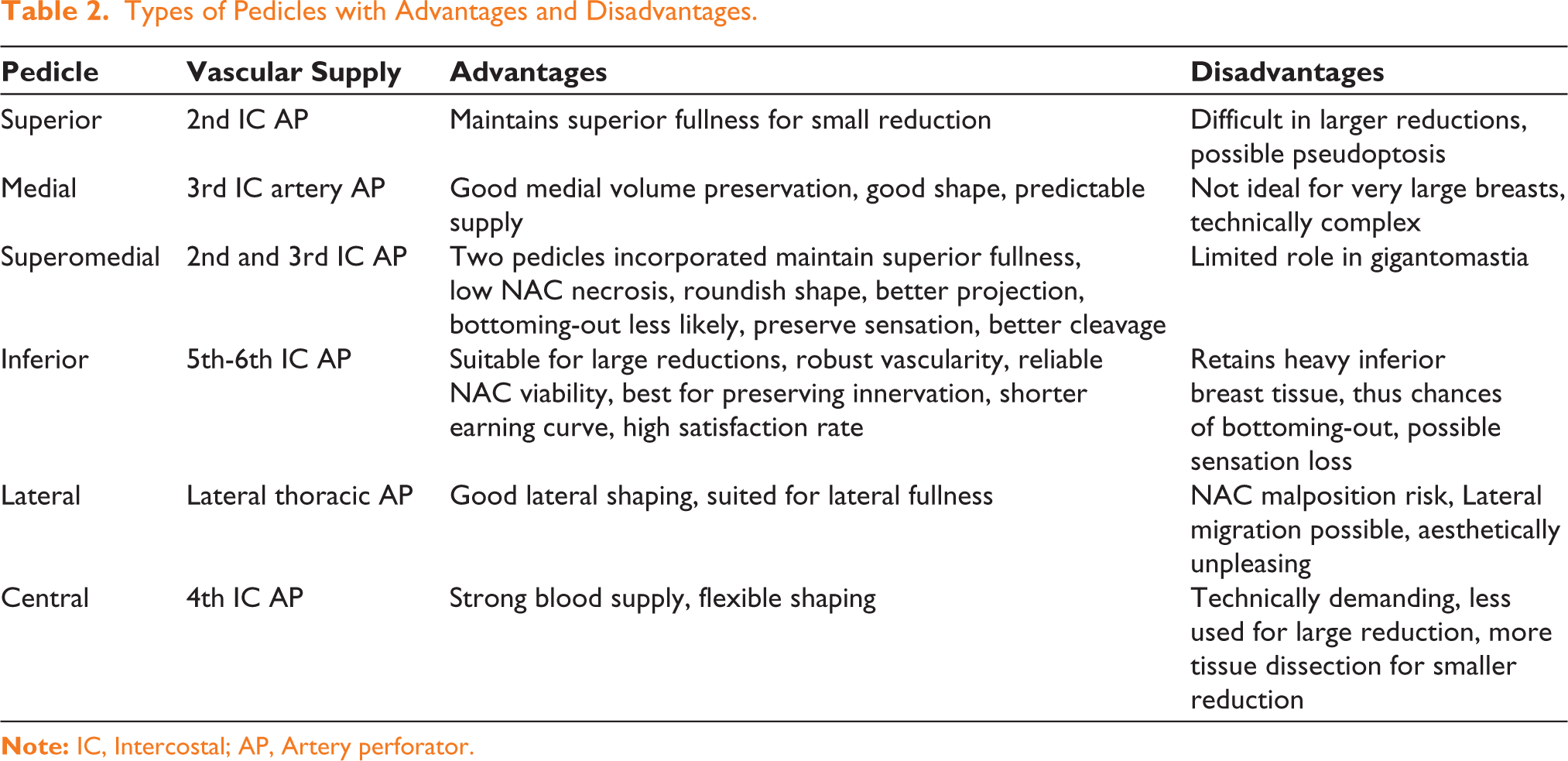
Historically, various pedicle designs have been described, including bipedicle techniques, lateral-based pedicles and centrally positioned techniques. 13 However, these approaches have been largely superseded in current day practise due to more consistent and better long-term outcomes and lesser complications of the popular ones. The evolution of reduction mammoplasty has streamlined the choice of pedicle techniques, prioritising those with proven efficacy and safety (Table 2).
Types of Pedicles with Advantages and Disadvantages.
Factors Influencing Pedicle Selection
The decision to use a specific pedicle technique depends on multiple factors like patient anatomy, breast size, degree of ptosis and desired aesthetic outcomes. 14 Larger breast reductions often necessitate techniques with more robust vascular supply, such as the inferior pedicle. In contrast, smaller reductions with a focus on upper pole fullness may benefit from a superior or medial pedicle approach. Additional considerations include skin quality, age of patient and previous surgical history, which can influence vascular integrity and healing capacity. High NAC repositioning favours superior or medial pedicles to maintain perfusion. Older patients or those with diabetes, smoking history or obesity may benefit from an inferior or central pedicle due to their more robust blood supply. Most pertinently, familiarity with a specific pedicle technique significantly influences surgical success.
Good outcomes depend on the maintenance of breast shape, NAC position and overall patient satisfaction. Our experience mirrors that patients undergoing superior pedicle techniques report better upper pole fullness, whereas those treated with inferior pedicle experience greater longevity of shape. Long-term scar quality can be influenced by patient genetics, tension at closure sites and adherence to postoperative scar management protocols.
The lateral pedicle has an inconsistent vascular supply, leading to a higher risk of NAC necrosis. 15 Additionally, lateral displacement of the NAC can result in poor aesthetic outcomes. Due to these drawbacks, the lateral pedicle is not commonly used in standard breast reduction surgeries. The central mound offers good vascular support but, we feel it often results in excessive residual tissue bulk, making contouring suboptimal. Venous congestion is another concern, leading to prolonged oedema and suboptimal healing. These limitations make the central pedicle less favourable compared to superior, superomedial, and inferior pedicles.
Skin quality influences long-term aesthetic outcomes. Older patients skin lends to earlier ptosis in the late postoperative period. Similar is the case with postbariatric patients of all age groups. Choice of pedicle or pedicle design does not have a bearing on this.
Following are reasons patients presented for us for redo/revision breast reduction:
Inadequate resection during first surgery Secondary enlargement of residual breast tissue To correct poor aesthetic outcomes of initial surgery
Most of these patients did not have the relevant operative details of previous surgery. However, while planning the redo surgeries, the surgery was undertaken de novo as in the above-mentioned formats. We disregarded the pedicle design of the previous surgery.
Complications
As is well documented in literature, reduction mammoplasty is one of the procedures with the highest complication rate amongst aesthetic procedures. This is taking into account both minor and major complications. 16 We assess and divide the complications into two types: surgical or aesthetic.
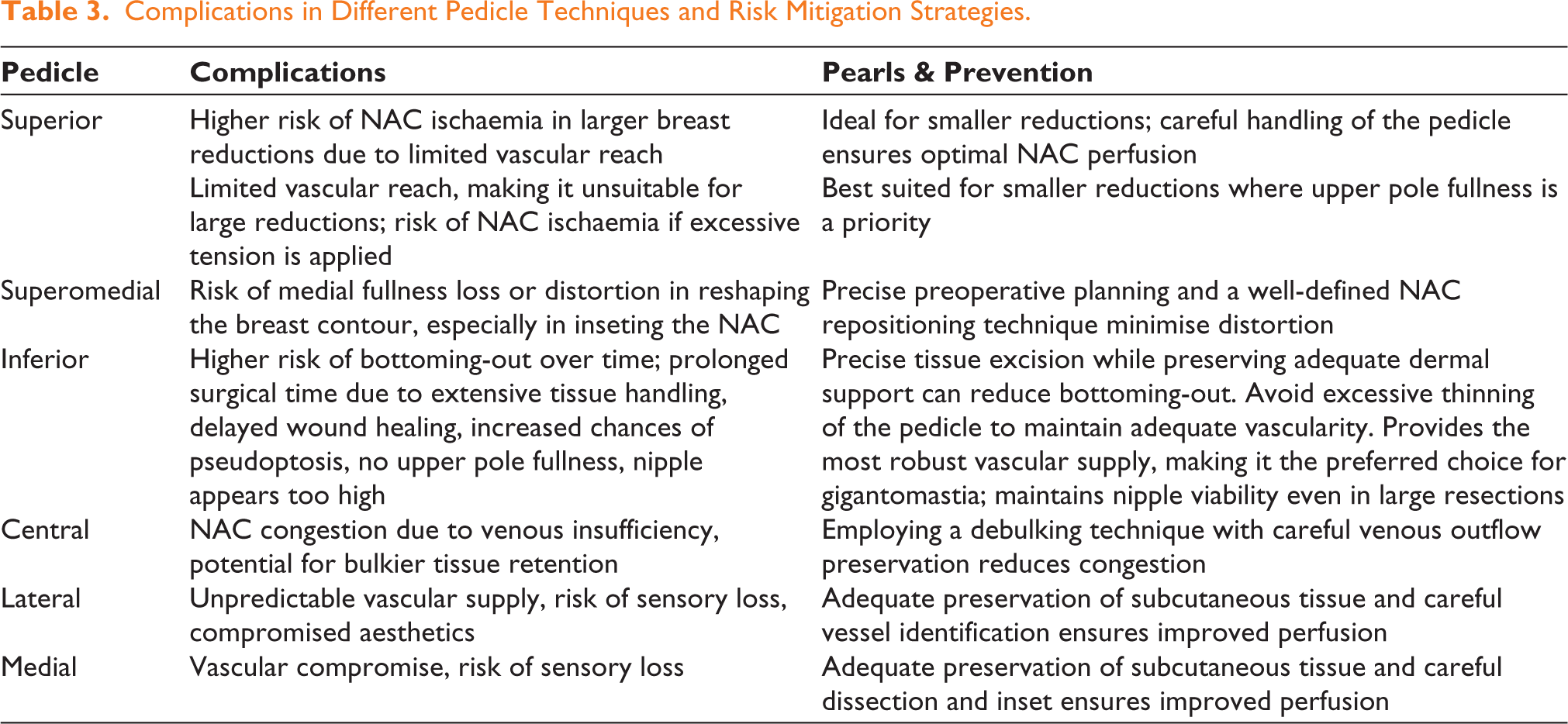
All surgical complications in breast reduction mastopexy are fundamentally related to vascularity; thus, pedicle selection plays a vital role. 14 Complications may be related to the execution of a procedure, tissue handling or suturing technique. A well-perfused NAC ensures a successful outcome, while inadequate perfusion increases the risk of necrosis, sensory loss and asymmetry. Table 3 shows common complications associated with different pedicle techniques and strategies to mitigate them. Common complications include NAC necrosis, sensory loss, asymmetry, poor scar healing, dog ears, puckering and bottoming-out. Sensory loss is minimised by preserving neural pathways in the chosen pedicle technique. Asymmetry, one of the most common concerns, can be reduced through meticulous preoperative planning and intraoperative adjustments.
Complications in Different Pedicle Techniques and Risk Mitigation Strategies.
Complications in aesthetic outcomes include:
Less than ideal outcome Aesthetic deformity
Assessment of the Breast After Reduction Mammoplasty
It is important to remember that breast shape and position change in the postoperative period. Thus, aesthetic outcomes are ideally assessed at the one year mark. A successful breast reduction should result in aesthetically pleasing, proportionate breasts with long-term stability.
17
We recommend assessment of the following specific features of an ideal breast after reduction surgery:
Breast symmetry
Assessed by the measurements as per the chart shown in Figure 2 and by photographic analysis The medial breast contour-balanced cleavage
Check for a balanced cleavage Ideal breast shape and projection
Natural, youthful contour No boxy or flattened appearance A gentle teardrop shape The projection: balanced with the patient’s body frame NAC Positioning
The nipple at the level of the inframammary fold (IMF) NAC in a forward-facing direction, no lateral or downward displacement Areola: shape circular, diameter: 4 cm-4.5 cm Proportional upper and lower pole ratio (45:55)
Upper pole: fullness to be maintained, no excessively concave or deflated look The lower pole: natural convex projection without excessive sagging or bottoming-out IMF position
Well-defined and positioned height relative to the thorax. Not be placed too high, which creates a constricted or unnatural breast appearance. Well-placed and minimal scarring
Concealed and well-healed scars in natural contours The areolar scar to blend with the surrounding tissue Skin and soft tissue quality
Smooth skin, without irregularities or puckering at incision sites Good elasticity and skin tone help maintain breast shape and prevent premature ptosis Long-term stability
The breast should retain its shape and position over time with minimal distortion Proper pedicle selection and tissue support help maintain long-term breast aesthetics
Conclusion
The choice of a vascular pedicle in breast reduction surgery is decided by anatomical, physiological and aesthetic considerations. The superomedial pedicle has become the workhorse for breast reduction surgery, accounting for the vast majority of cases performed. The superomedial pedicle is ideal for moderate-to-large breast reductions, offering a balance between vascular reliability and upper pole fullness. The superior pedicle technique is most suitable for mild cases without significant breast ptosis, providing excellent projection and NAC viability. The inferior pedicle remains the preferred option for gigantomastia due to its robust blood supply and ability to support extensive tissue resection. Breast reduction surgery with free nipple graft for gigantomastia was never required/considered.
Thus, mastering this particular technique may be okay for the surgeon performing this surgery occasionally. However, we feel that, for those aspiring/performing, more reductions should be proficient in more than one pedicle technique as per their patient demographics. Individual patient factors and surgeon expertise ultimately determine the optimal technique for achieving the best surgical outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.