
Abstract
Background:
Rhinoplasty in short, depressed and thick-skinned Indian noses presents unique challenges. The thicker nasal skin acts as a veil, shrouding the distinct features of the underlying skeletal framework and diminishing their visibility. Traditional approaches often focus on thinning the dermis, which can compromise blood supply, lead to skin necrosis, surface irregularities and postoperative fibrosis. Augmenting only the dorsum in these noses often results in an artificial, unnatural and ‘done nose’ appearance.
Materials and Methods:
Our technique involves an open approach, preserving Pitanguy’s ligament in primary noses. We occasionally remove excess fat from the supratip region and between the domes. A firm cartilaginous framework is created through reinforcing the weak cartilaginous vault and using a differentially carved dorsal strut. In primary noses, Pitanguy’s ligament is restored. In secondary noses or cases where Pitanguy’s ligament was not preserved, supratip subdermal suture is used. This suture obliterates the dead space, adjusts supratip skin thickness internally and prevents supratip bulging. This approach allows for desired tip shape without actual thinning of supratip skin.
We emphasise the importance of nasal lengthening, which maintains nasal proportions with the face. Lengthening also helps stretch thick skin, creating a more refined appearance.
Results:
Patients expressed high satisfaction with the aesthetically pleasing and durable outcomes, which were maintained over a minimum follow-up period of one year. Notably, no supratip deformity was observed postoperatively, and the tip and midvault regions exhibited adequate projection, contributing to a favourable and long-lasting result.
Conclusion:
Rhinoplasty in short, depressed and thick-skinned Indian noses can be performed safely and effectively without thinning the supratip skin. By tailoring the dorsal strut to skin thickness, obliterating the dead space at supratip and ensuring a firm cartilaginous framework, surgeons can achieve natural-looking results with minimal risk and ensuring adequate tip projection.
Keywords
Introduction
The performance of rhinoplasty on short, depressed and thick-skinned Indian noses is a complex and nuanced procedure that requires a thorough grasp of nasal anatomy and skin properties. Conventional methods, which typically involve reducing the thickness of the supratip skin and augmenting the dorsum, can be fraught with complications such as skin necrosis and fibrosis, and may produce a nose that appears unnatural and surgically altered, rather than achieving a natural and aesthetically pleasing result.
A patient with typical Indian nasal characteristics who seeks augmentation of the dorsum usually presents with a nose which is a low dorsum, broad bridge, short length, flared alae, thick sebaceous skin and paradoxically weak lower lateral cartilages (LLC).
Simply augmenting the dorsum of the nose in these patients is insufficient, as it fails to address the underlying issues and can result in an unnatural appearance. Instead, a more comprehensive approach is needed, involving augmentation and structural reinforcement in multiple dimensions. A 3D augmentation concept found to be effective in achieving this, provided the soft tissue envelope is accommodating and allows for lengthening of the nose, adequate tip projection, and dorsal augmentation simultaneously. However, in cases where the soft tissue envelope is restrictive, compromises may be necessary, and it is preferable to compromise on the height of the dorsum rather than sacrificing nasal length.
Key challenges include:
Relatively short or tight soft tissue envelope. The scarcity of septal cartilage due to the short nasal length, which limits the availability of local donor cartilage for grafting purposes. Paradoxically weak LLCs requiring reinforcement. The need for a significant amount of cartilage grafts to address the depressed dorsum and short nasal length, while also providing reinforcement for the weak LLCs.
Grafting options:
Septal cartilage: While it has good strength, it is often in short supply in these noses. Conchal cartilage: Unfortunately, it lacks both strength and quantity, making it a less desirable option. Costal cartilage: Costal cartilage possesses both strength and abundance, making it the go-to choice for augmenting, reinforcing and lengthening these noses. Costal cartilage is the preferred graft material for these noses, offering a reliable and effective solution for achieving the desired aesthetic and functional outcomes. However, its tendency to warp poses a challenge. To address this issue, the authors employ their innovative Counterbalancing (Namaste) technique, which effectively mitigates warping and ensures a stable, long-lasting result.
1
Materials and Methods
This is a retrospective review of a total of 63 patients who underwent surgery using this concept, comprising 48 females and 15 males over six years. Patients with preoperative sebaceous hyperactivity requiring medical management were not included in this study. The age range of the patients was between 17 and 62 years. All patients received systemic antibiotics for five days postoperatively.
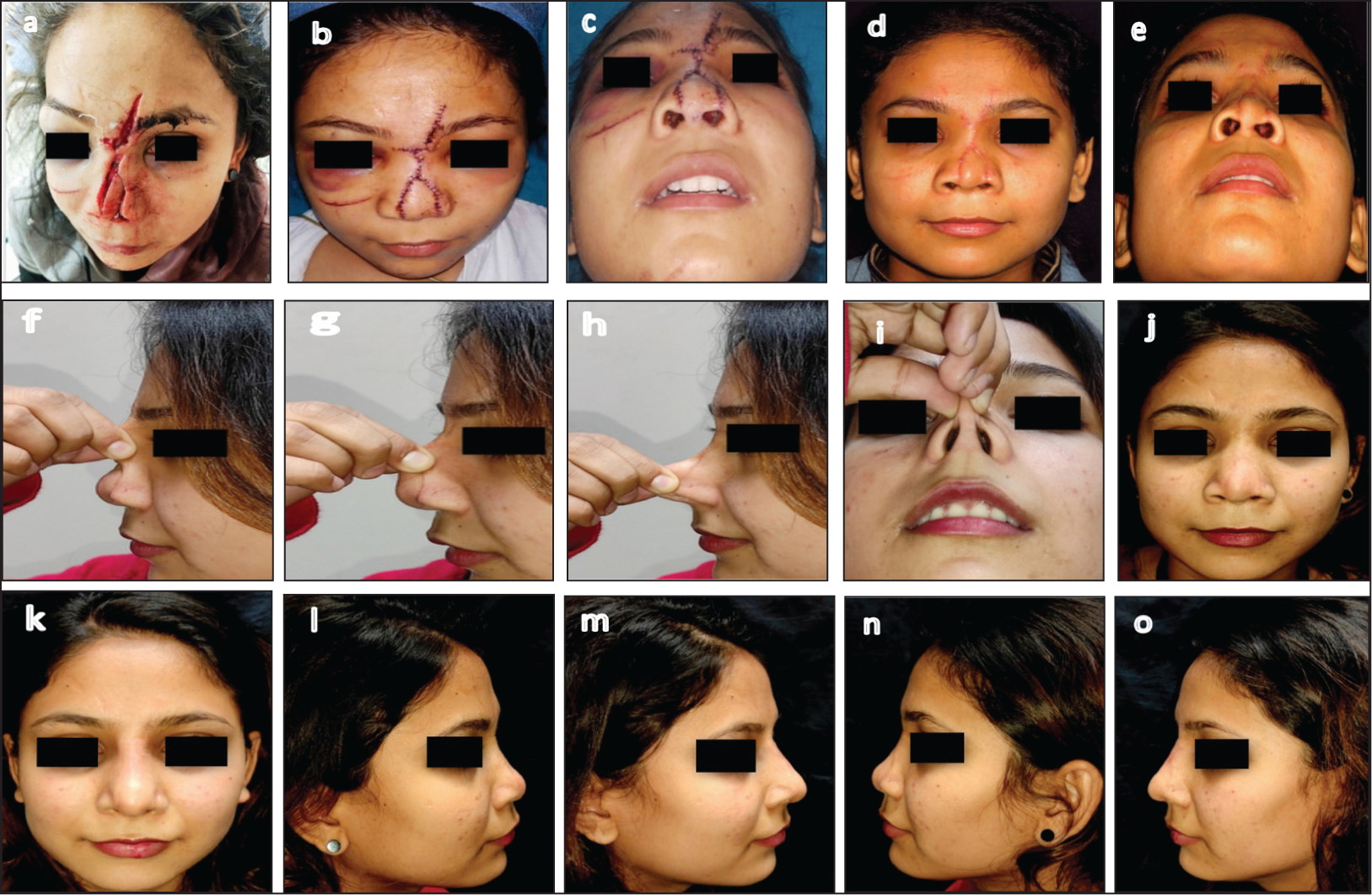
Nasal skin with varying textures poses distinct challenges. While thick, pliable skin can be accommodated with minor surgical adjustments, thick, sebaceous skin necessitates preoperative treatment to render it operable. In cases of severely depressed primary, post-traumatic and secondary noses, the nasal skin is often thick, contracted, tough and unyielding. To restore softness and pliability, vigorous massage and skin stretching are essential before surgery can be considered. Although the duration of this preparatory phase varies, it has proven effective in the majority of patients (Figure 1).
Thickness of the skin complicates the surgery and usually leads to significant post-operative contraction, altering shape notably without robust structural reinforcement.
Understanding the Unique Skeletal Anatomy of the Nose
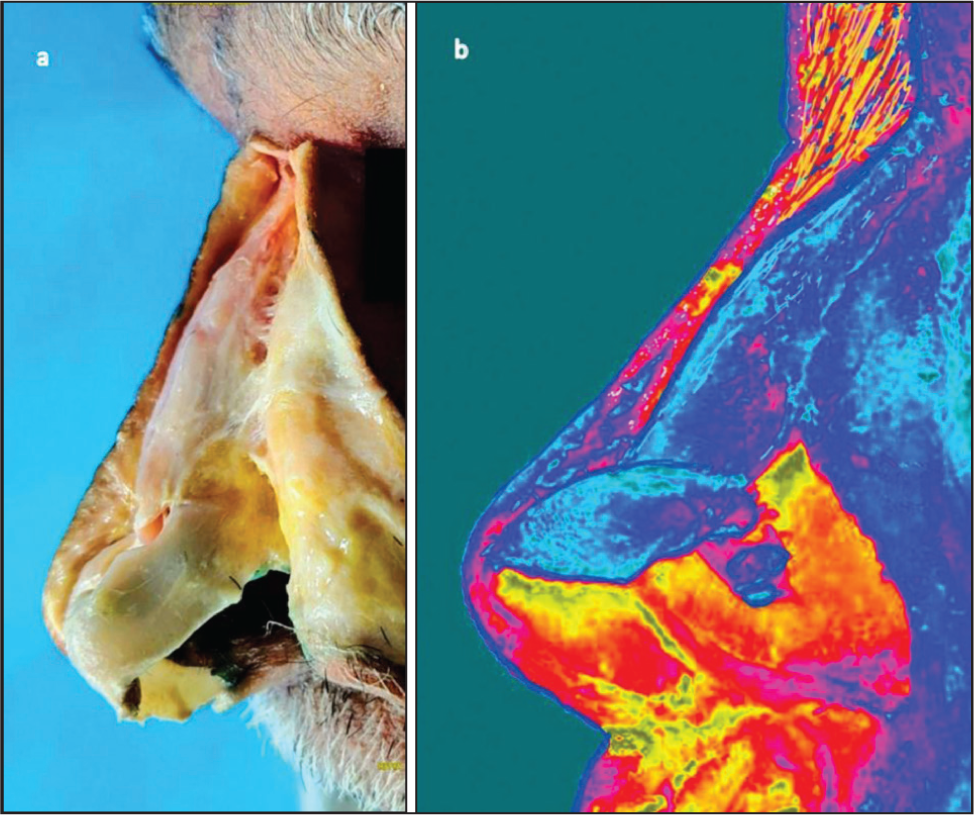
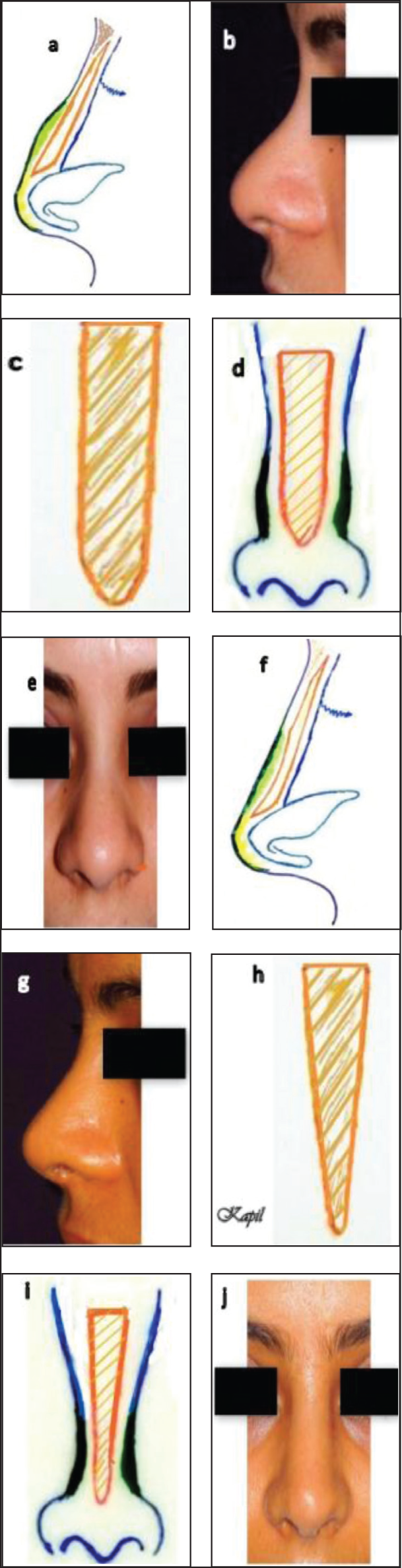
The nasal skeleton is a marvel of natural design. Externally, the dorsum appears straight, with the nasal tip projecting a few millimetres beyond it. However, internally, the dorsum slopes on both sides—cephalically toward the radix and caudally toward the supratip (Figures 2a and 2b). This anatomical arrangement likely serves to accommodate the thickness of the skin within the nose, particularly in the radix and supratip regions. As a result, despite the substantial skin thickness at both ends, the external dorsum maintains a straight appearance. This ingenious design is a testament to the wonders of natural creation and seamlessly integrates structural harmony and aesthetic balance.
Illustrates the Transformation of a Post-traumatic Nose with Torn and Hardened Skin to a More Pliable and Receptive State for Augmentation. (a) Post-road Accident Broken Nose with Torn Skin. (b and c) One Week Post-suturing of Torn Skin. (d and e) One Month Post-suturing, Showing Rocky Hard Skin and Soft Tissue. (f-i) Ten Months Post-vigorous Massage, Demonstrating Improved Skin Pliability and Faded Scars. (j-o) Desired Augmentation Achieved in all Directions Due to Improved Skin Pliability.
Cadaveric Dissection Demonstrating Variable Skin Thickness. (a) The Nasal Skin Appears Thickest in the Radix Due to Thickness of Dermis as Well as the Presence of the Procerus Muscle, Thinnest in the Middle Third and Thick Again in the Supratip Area. (b) Heat-map Photograph Highlighting Skin Thickness Variations.
Surgical Technique
Our technique is based on key principles:
Preserving the dermis: Preserve the dermis to avoid damaging the subdermal vascular plexus. Thinning the dermis risks damaging the subdermal vascular plexus, leading to complications such as necrosis or surface irregularities. Selective fat removal: This procedure is performed judiciously, only when deemed absolutely necessary, to avoid compromising the delicate blood supply in the supratip area. In cases where a distinct fat pad is present, careful excision can be carried out to remove excess fat without disrupting the subdermal blood supply. To minimise the risk of injury to the subdermal plexus, a ‘balloon technique’ can be employed.
2
By infiltrating the area with normal saline using a 26-gauge needle, the fat tissue becomes distended and can be easily removed in a single sheet, using a gentle scissor stroke, thereby preserving the integrity of the subdermal plexus (Figures 3c and 3d). Creating a rigid underlying skeletal framework: A strong structural framework is essential to support the weight of a thick skin-soft tissue envelope. To establish a solid foundation, the native cartilaginous framework must be reinforced with rigid grafts, such as spreader grafts, to enhance the dorsum. Tip support is achieved by placing lateral crura inlay (Figures 4a-4d), onlay or strut grafts to strengthen the LLCs and utilising a septal extension graft (SEG) (Figures 5c and 6c), which not only elongates the nose but also provides additional tip reinforcement. Over time, the sturdy skeletal framework applies gentle, consistent pressure, refining the thick dermis, making it thinner, smoother and softer, ultimately enhancing the underlying definition with greater precision. Costal cartilage is often harvested to provide the necessary structural support, both in primary procedures and in secondary or revision cases. Stretching of the Nasal skin with a strong and stable skeleton, also counters post-op contraction forces. The authors have a liberal approach to utilising tip grafts, including shield grafts (Figure 6e), cap grafts, lateral crural strengthening and lateral crural strut grafts, to achieve optimal tip refinement. To ensure a natural appearance, it is essential to cover these grafts with a layer of fascia or perichondrium (Figure 6f), thereby minimising the risk of graft visibility and promoting a seamless integration with the surrounding tissue, while enhancing tip definition and projection. Differential carving of the dorsal strut (designing and clinical application of a dorsal strut): Carve the dorsal strut to mimic natural nasal anatomy, ensuring it aligns with the existing dorsum and accounts for variable skin thickness. A differentially carved design is essential: thin and slanted in the radix to accommodate the procerus muscle and maintain the frontonasal angle, while tapering to a pencil-thin shape in the supratip for proper skin adaptation. The authors create customised dorsal struts, taking into account native nasal anatomy and variable skin thickness, by employing their ‘diced cartilage under perichondrial carpet with reinforcement’ (DCUP) technique
3
(Figures 3g and 6d). A uniformly thick and wide strut risks obliterating the nasofrontal angle and causing supratip bulging both superiorly and laterally (Figure 7). Elimination of the dead space, prevention of polybeak and creation of supratip break by restoration of Pitanguy’s ligament or using supratip subdermal sutures: These techniques help obliterate dead space, maintain dermal integrity and ensure the supratip skin remains well-adjusted within the nasal framework. In patients with a thick skin-soft tissue envelope, the flap often exhibits significant inelasticity, making it difficult to re-drape over the nasal skeletal framework, even with a differentially carved dorsal strut. After completing all surgical modifications, the skin-soft tissue envelope is repositioned over the skeletal framework, and any dead space in the supratip area is eliminated either by placing a subdermal suture (Figures 5d and 5e) or restoring Pitanguy’s ligament (Figures 8a and 8b). This single manoeuvre serves multiple purposes: it secures the supratip skin to prevent bulging (Polybeak), eliminates dead space to avoid fluid accumulation and subsequent fibrosis (which could lead to Polybeak), and helps create a desirable supratip break. Nasal lengthening: Authors use nasal lengthening as a primary strategy to stretch thick skin. Lengthening a short and depressed nose is often more important than dorsal augmentation.
There have been several techniques described to lengthen the nose, for example, (a) Dorsal strut, (b) SEG and (c) Tent-pole graft.
The simplest method of achieving mild lengthening in the short nose is dorsal onlay or radix grafts.
The techniques that we have found most useful and effective are described here. Technique 1: SEG is a powerful and straightforward way of lengthening the nose and controlling tip projection simultaneously. It can be used: (a) In the patient with no lining restriction, (b) good over-lying skin quality and (c) abundant septal cartilage of adequate strength (Figures 5c and 6c).
Shows the Pitfalls of Inadequate Rhinoplasty. (a and b) A Secondary Nose Case Illustrates the Consequences of Incomplete Dorsal Augmentation in a Typical Indian Nose. The Initial Attempt Focused Solely on Dorsal Enhancement, Neglecting the Tip, Nasal Length and Overall Proportions. This Resulted in an Unnatural, ‘Done Nose’ Appearance. (c) Showing Authors’ ‘Balloon Technique’ of Excess Fat Removal by Injecting Normal Saline in the Supratip Area. (d) Showing Resected Fat. (g) Showing the Shape of the Dorsal Strut. (f and i) Post-operative Photographs Demonstrate a Dramatically Improved Outcome, Achieved by Addressing all Aspects of Nasal Aesthetics: A Well-defined Dorsum, a Sleek, Refined Tip, Optimal Dorsal Height and Harmonious Proportions, Enhanced by Chin Augmentation. This Case Highlights the Importance of Comprehensive Rhinoplasty Planning, Considering all Facets of Nasal Anatomy to Achieve a Natural, Balanced Result.

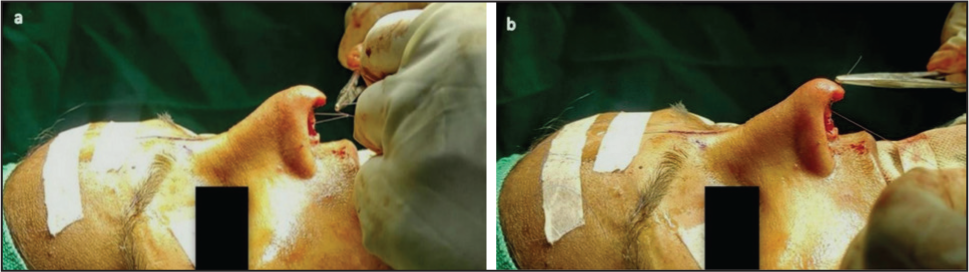
This Series of Photographs Demonstrates the Transformative Effect of Reinforcing Weak Lower Lateral Cartilages Using Lateral Crural Inlay Grafts. (a) Preoperative View: Note the Loose and Flattened Appearance of the Tip and Base of the Nose. (b) Intraoperative View: Lateral Crural Inlay Grafts Being Secured to Reinforce the Weak Cartilages. (c) Postoperative View: The Lower Lateral Cartilages Now Appear Tensed and Taut, Providing Improved Structural Support. (d) Postoperative Result: A Pleasing Change in the Shape of the Tip and Base is Evident, Highlighting the Effectiveness of Cartilaginous Reinforcement in Achieving a More Refined Nasal Appearance.

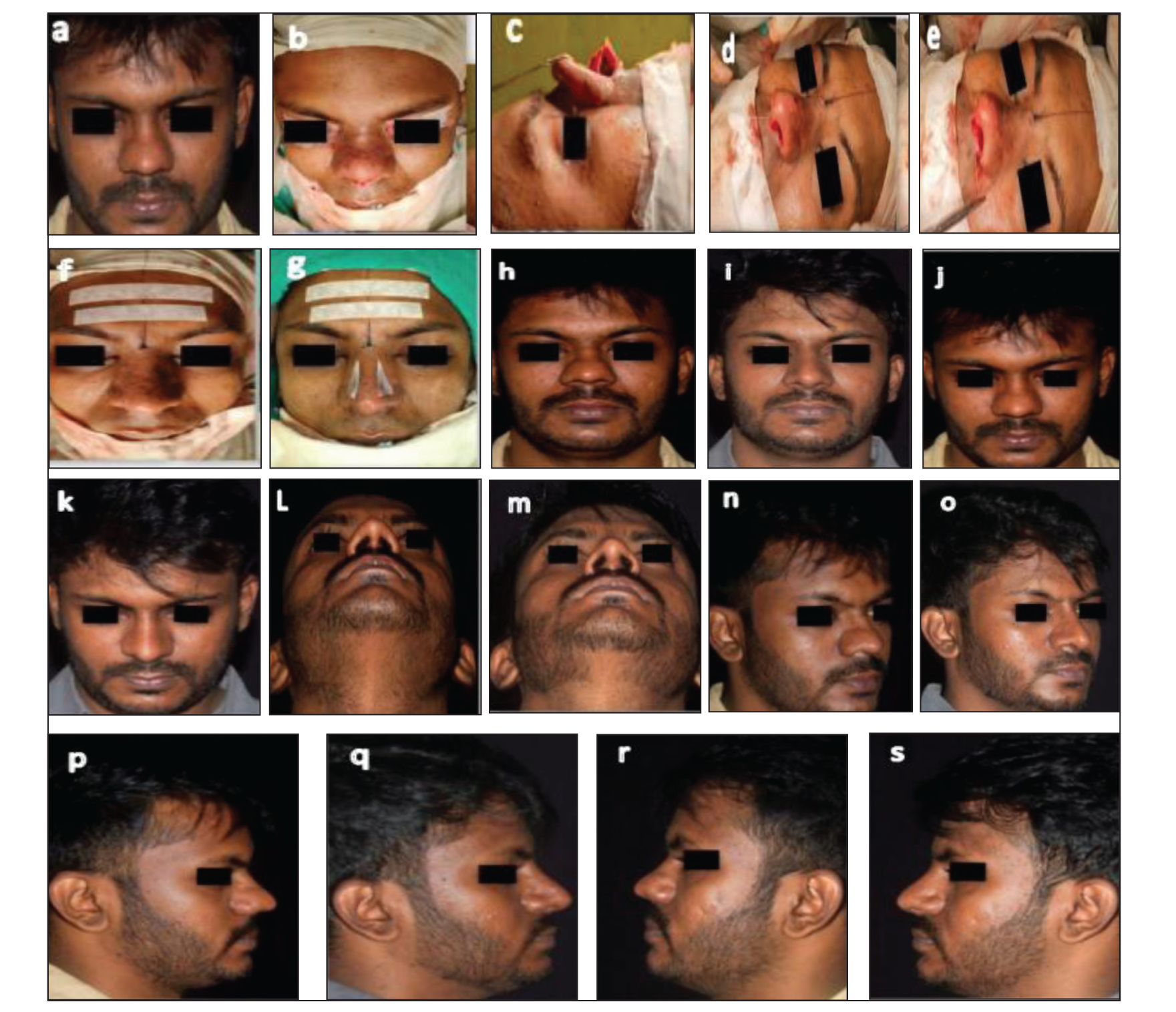
This Series of Photographs Showcases the Surgical Transformation of a Typical Indian Nose, Characterised by a Short Length, Depressed Dorsum and Bulbous Tip. (a) Preoperative Photograph: The Nose Exhibits a Short Length, Depressed Dorsum and Bulbous Tip. (b) Intraoperative Photograph: Showing the Opened Nose Without Structural Strengthening. (c) Intraoperative Photograph: A Septal Extension Graft and Tip Graft are Secured to Enhance Nasal Proportions. (d) Intraoperative Photograph: The Supratip Area Appears Bulbous Before Tightening the Subdermal Suture. (e) Intraoperative Photograph: The Supratip Area is Refined After Tightening the Subdermal Suture, Adjusting the Supratip Thickness Internally. (f) Intraoperative Photograph: After Closure, the Nose Exhibits a Pleasant, Refined Appearance. (g) Intraoperative Photograph: Lateral Compression Sutures are Placed to Control Lateral Bulgings. These Sutures are Removed After 48 Hours to Prevent Permanent Marks. (h-s) Twenty-six-month Postoperative Photographs: The Result Demonstrates Stable, Long-term Improvement with no Recurrence of Supratip Bulging.
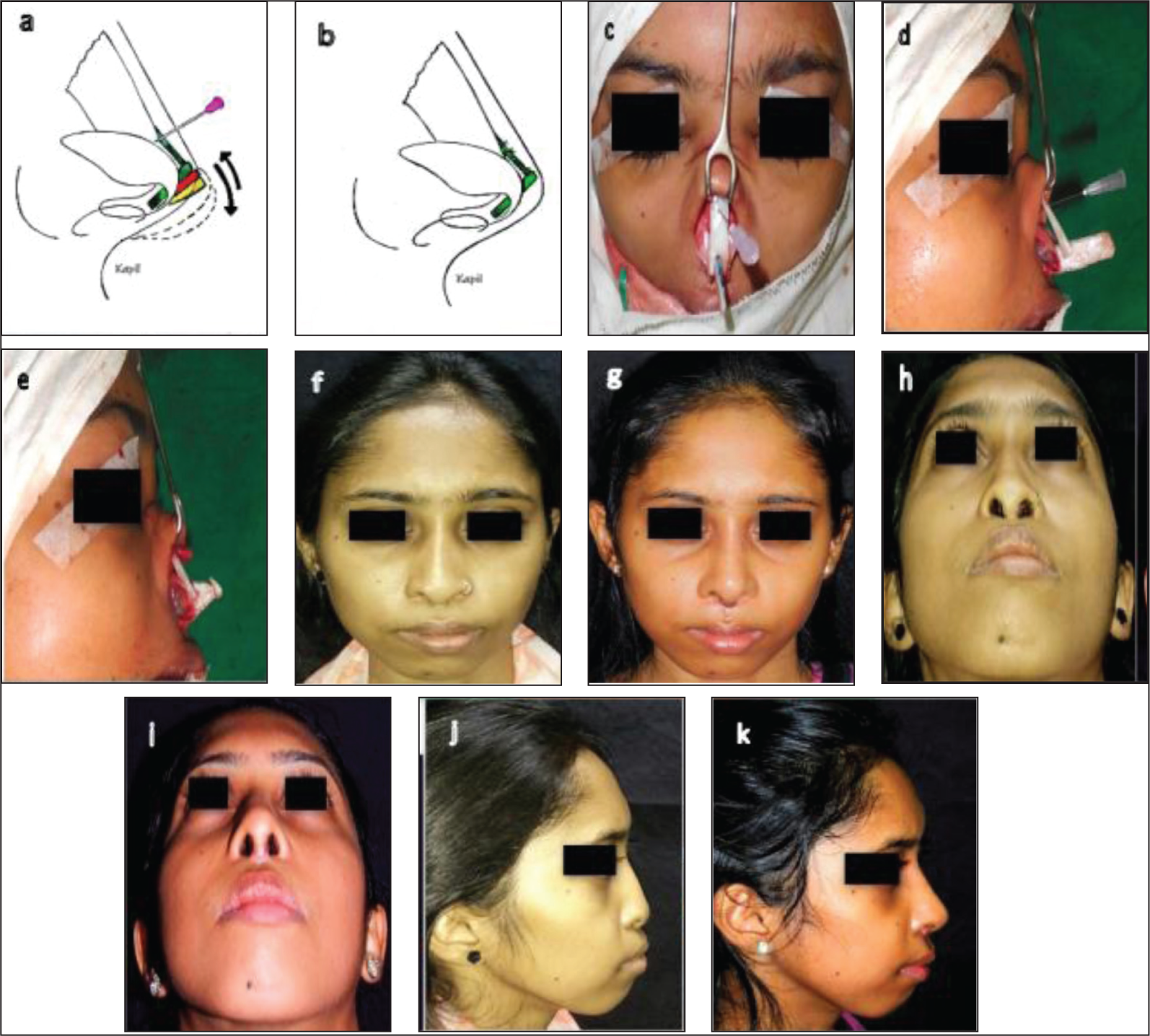
Technique 2: Tent-pole graft is used to lengthen the nose and to set a nasolabial angle of choice in patients: (a) where the caudal septum is lying too low to get proper purchase to fix SEG, (b) multiple times operated nose where you do not want to risk dissecting the caudal septum, (c) patient is having septal perforation and (d) shortage of cartilage grafts 4 (Figure 9 and Supplementary Video).
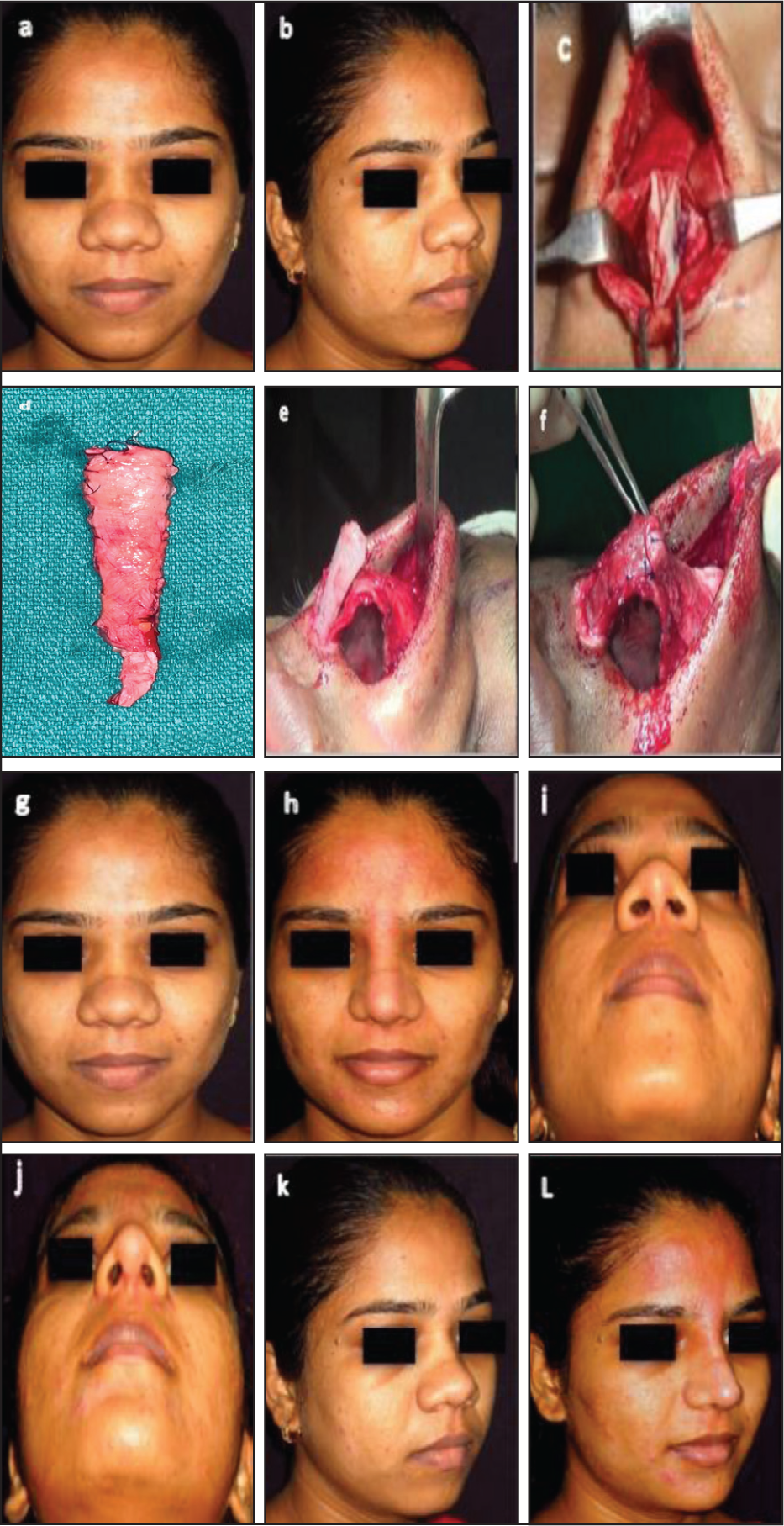
Female Version of the Typical Indian Nose. This Series of Photographs Showcases the Transformation of a Female Typical Indian Nose, Characterised by a Short Length, Depressed Dorsum and Bulbous Tip. (a and b) Preoperative Photographs: The Nose Exhibits a Short Length, Depressed Dorsum and Bulbous Tip. (c) Intraoperative Photograph: A Septal Extension Graft is Created Using Two Thin Sheets of Costal Cartilage, Employing a Counterbalancing Technique to Prevent Warping. (d) Intraoperative Photograph: The Dorsal Strut is Shaped Using DCUP (Diced Cartilage Under Perichondrial Carpet with Reinforcement). (e) Intraoperative Photograph: A Shield Graft is Placed to Refine the Tip. (f) Intraoperative Photograph: The Shield Graft is Covered with a Sheet of Perichondrium to Conceal Its Visibility. (g-l) One-year Postoperative Photographs: The Result Demonstrates a Pleasing Dorsal Appearance and a Considerably Refined Tip, Showcasing a Successful Transformation of the Typical Indian Nose.
Differential Carving of Dorsal Strut: A Key to Preventing Supratip Bulging in Thick-skin Noses. A Series of Diagrams and Photographs Illustrate the Impact of a Uniformly Wide and Thick Dorsal Strut in Thick-skin Noses, Demonstrating How It Can Cause Supratip Bulging in Both Superior and Lateral Directions. However, Differential Carving of the Dorsal Strut Proves to Be an Effective Solution in Mitigating Supratip Bulging.
Restoration of Pitanguy’s Ligament: A Key to Refining the Supratip Area. This Figure Illustrates the Impact of Restoring Pitanguy’s Ligament on the Supratip Area. (a) Pre-knot Tightening: The Supratip Area Appears Bulbous Before the Restoration of Pitanguy’s Ligament. (b) Post-knot Tightening: After Tightening the Knot, the Supratip Area Exhibits a Refined Break or Adjustment, Effectively Addressing Supratip Bulging and Creating a More Defined Nasal Profile.
Sequential Diagrams and Photographs Showing the Placement and Effectiveness of Tent-pole (Dorso-columellar) Graft. (a and b) Schematic Diagrams Demonstrating the Precise Placement of the Tent-pole Graft. (c-e) Intraoperative Photographs Showcasing the Use of the Tent-pole Graft to Increase Nasal Length and Establish a Refined Nasolabial Angle. (f-k) Postoperative Photographs Highlighting the Efficacy of the Tent-pole Graft in Achieving the Desired Nasal Length and Nasolabial Angle, Resulting in a Harmonious and Refined Nasal Profile.
Surgical Steps
The surgical steps involve skin-soft tissue envelope dissection using an open rhinoplasty approach, with the flap elevated under the superficial musculoaponeurotic system (SMAS) preserving the Pitanguy’s ligament wherever possible. In select cases, where a blob of fat is seen in supratip area, fat can be easily excised using ballooning technique, respecting the subdermal plexus 2 (Figure 3c and d). SMAS debulking is not done in any of the cases. Additionally, the fatty tissue between the domes can be removed, creating more definition of the underlying structures of the nose.
Postoperative Care
In a few patients, swelling in supratip area may persist mainly on the lateral aspect. Postoperative taping is crucial in these cases but it should not be overly tight. Taping helps compress the skin envelope to the framework and should be advised for four to six weeks at night and on weekends.
Results
Our technique has been consistently successful in achieving a defined nasal dorsum and supra tip without the need for dermal thinning. Complications such as skin necrosis, surface irregularities and postoperative fibrosis are significantly reduced. Patients report high satisfaction rates, with aesthetically pleasing and long-lasting outcomes.
One patient with secondary cleft lip nasal deformity, in whom fat excision with dermal thinning was attempted, had necrosis of a few mm of skin which healed with scarring (Figure 10). Skin thinning, in any form, must be avoided in all cases to avoid these complications. The nasal splint, micropore tape and sutures were removed after one week, and a new splint was applied for an additional week. The follow-up period ranged from one to five years, during which no supratip deformity was observed. The tip and midvault regions demonstrated adequate projection, indicating a successful outcome.
Complication of Inadvertent Skin Thinning: This Photograph Illustrates an Unfavourable Outcome Resulting from Excessive Thinning of the Nasal Tip and Supratip Skin, Highlighting the Importance of Dermal Preservation and Use of Differentially Carved Dorsal Strut and Adjustment of Skin Thickness Inside the Nose.

Discussion
In the realm of rhinoplasty, the Indian nose exhibits distinct characteristics that differentiate it from the Caucasian nose. According to Nagarkar et al., these differences include thicker skin, darker pigmentation and weaker upper lateral cartilage (ULC) and LLCs. The presence of thick skin can lead to prolonged postoperative oedema, masking the underlying cartilaginous framework changes. Consequently, significant modifications in the nasal framework, such as augmentation or reduction, are often necessary to achieve optimal results. Moreover, extended postoperative splinting and taping may be required to mitigate oedema. 5
Various surgical techniques have been proposed to refine thick-skinned noses. Oleh et al. advocates for an open rhinoplasty approach incorporating septal strut and shield grafting, intradomal/subcutaneous fat excision and LLC manipulation. This includes dome division, cephalic strip, domal and intradomal suturing to enhance nasal definition. 6
Histologic studies of excessively thick nasal tip skin conducted by Garramone et al. revealed abundant subcutaneous fibromuscular tissue as the primary cause of S-STE thickening. Although some dermal thickening was also observed, fibromuscular tissue provided most of the additional skin thickness, whereas adipose tissue was only a minor component of nasal skin. 7
Although the histology of excessively thick nasal skin is well characterised, cutaneous defatting is still regarded by many as a potentially hazardous means of improving nasal tip definition. Many of these concerns probably stem from the large number of conspicuous skin injuries observed in patients undergoing tertiary rhinoplasty. Although any invasive rhinoplasty technique has the potential to produce iatrogenic skin injury, defatting techniques that involve direct dermal manipulations are far riskier and probably account for most defatting complications.8,9
The thickness of the skin in rhinoplasty patients is often attributed to a hypertrophied SMAS layer, as noted by Baser et al. Surgical debulking of the SMAS can aid in thinning the skin and improving tip definition; however, caution must be exercised to prevent damage to the subdermal vascular plexuses to ensure adequate skin perfusion. This approach must be individualised to avoid excessive thinning and potential skin discoloration. 10
A key challenge in rhinoplasty is addressing supratip deformity, previously referred to as ‘pollybeak’ or ‘parrot beak’ deformity. Kim et al. described this as a convexity or fullness just above the nasal tip, which may be congenital or post-rhinoplasty in origin. This deformity requires meticulous surgical intervention to ensure a refined nasal contour. They suggested the importance of intra-SMAS dissection in the tip and supratip regions to separate the superficial and deep SMAS. A partial SMASectomy of the deep SMAS is then performed while ensuring the elevated skin flap retains a consistent thickness to preserve the subdermal plexus circulation of the tip envelope. 11
Davis et al. caution that ‘defatting’ a thick-skinned nasal flap may yield only marginal improvements in tip definition, necessitating realistic cosmetic expectations for such patients. Thick, unyielding skin can easily mask surgical changes to the nasal framework, cosmetic improvements are frequently most challenging in the thick-skinned patient. Surgically induced contracture of otherwise normal skin may distort a weakened nasal skeleton, resulting in bossae, asymmetry or other contour deformities (the so-called ‘shrink-wrap’ phenomenon). Improved nasal contour is often best achieved through augmentation of the underlying nasal skeleton. 12
Rohrich et al. identified the lateral nasal artery as the predominant blood supply of the nasal tip skin. The lateral nasal artery originates from the angular artery adjacent to the alar crease, and is located superficial to the nasal SMAS within the subdermal fat. Hence, debulking to the dermal level, particularly near the alar crease, is strongly discouraged, because it risks disruption of nutrient blood flow. 13
Further insights from Guyron et al. highlight that nasal skin is thickest at the radix and nasal tip while being thinner at the rhinion and columella. The sebaceous gland density in the supratip region significantly influences skin quality. Managing sebaceous hyperplasia involves a structured skincare regimen, retinoid therapy and, in some cases, oral isotretinoin. A critical aspect of thick-skinned rhinoplasty patients is the removal of excess fat between the nasal domes. Eliminating dead space is essential to prevent blood accumulation, reduce swelling and avoid fibrofatty tissue formation, which may compromise tip definition. The use of a supratip stitch helps approximate the skin envelope to the underlying framework. 14
The dermocartilaginous ligament of the nose, as first described by Pitanguy, has been shown to influence the equilibrium of the dorsum-tip relationship. In some noses, this is manifested by a residual convexity after routine rhinoplastic management of the osteocartilaginous structures. This structure is believed to unite the dermis of the upper third of the nose to the junction of the medial crura and to reach down to the subseptum. Therefore, it is considered to influence the equilibrium of the dorsum-tip relationship, especially in bulbous or Negroid noses. Moreover, division of this structure was found to result in an important upward liberation of the lower third of the nose in these patients.15-17
Lengthening the short nose is a difficult operation in aesthetic rhinoplasty, requiring adequate release or supplementation of soft tissue and cartilage to address this deficiency. Moreover, the lengthened nose can lose much of its intraoperative length in the postoperative period as the soft tissues pull the nose back toward its original length. Sufficient release of the LLC from the ULC and septal lengthening procedures are, therefore, indispensable elements in correcting the short nose deformity. Our approach for the correction of the short nose includes sufficient release of the LLC from the ULC and septal lengthening with a SEG using rib cartilage. The rib provides the most abundant source of cartilage for graft fabrication and is the material of choice when reliable structural support and lengthening of the septum are needed. In this article, we describe our experience using this technique to correct short nose deformity in Asian patients. 18
Lengthening a short nose is a challenging rhinoplasty problem. To address this, two key steps are recommended: First, significant soft tissue release is necessary to facilitate lengthening. Second, a three-part technique is employed, involving: (a) bilateral release of the septal mucoperichondrium, (b) release of the upper laterals from the LLC and (c) placement of a baton graft attached to the septum to support the tip cartilages in a more caudal position. This approach has yielded satisfactory results in 13 surgical cases, with minimal complications. 19
Several techniques have been proposed for nasal lengthening. Among them, Byrd et al. have described the SEG as the most effective approach. This technique is particularly beneficial for patients with no lining restrictions, good overlying skin quality and sufficient septal cartilage of adequate strength. SEG not only lengthens the nose but also provides precise control over tip projection.20-22
Conclusion
Rhinoplasty in short, depressed and thick-skinned Indian noses can be performed safely and effectively without actually thinning the supratip skin. Creation of differentially carved dorsal strut guided by variable thickness of the nasal skin and natural anatomy of dorsum, creation of a firm cartilaginous framework, restoration of Pitanguy’s ligament in primary noses and the use of supratip subdermal sutures in other noses to obliterate dead space and to adjust the thickness of supratip skin internally, nasal lengthening and adequate tip projection, surgeons can achieve natural-looking results while minimising risks.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Consent of photography and use of photographs for teaching and publication purposes was obtained from all patients.