
Abstract
Secondary breast implant surgery is a significant and important part of aesthetic breast surgery practice. It is more complex and variable surgery than primary augmentation surgery. Secondary implant surgery may be related to problems with the implant, overlying breast tissue or both. Systematic anatomical breast analysis as well as patient education regarding their anatomy and how it influences their surgical options and outcomes is a vital part of the preoperative consultation and surgery planning.
We propose a traffic light tool for secondary breast implant surgery patients that classifies their anatomical complexity and difficulty into three levels; Level 1 (green) with little anatomical distortion and good quality tissues, Level 2 (amber) with some anatomical complexities or compromised breast tissues and Level 3 (red) with significantly complex breast anatomy or poor-quality breast tissues.
Use of this traffic light system guides the surgeon to systematically analyse the breast and produces a clear visual aid for patient education.
Introduction
Breast augmentation continues to be one of the most popular aesthetic surgery procedures worldwide. Numbers of breast augmentation procedures also continue to rise annually.1,2 Breast implants are long term rather than lifelong devices with expected secondary surgery in the future3-6; so with the growth in primary breast augmentation surgery, growth in secondary breast implant surgery will also take place in due course.
Secondary breast augmentation differs significantly from primary breast augmentation in terms of breast analysis, surgical planning and complexity. Patients already have an implant in place. They may or may not know the type, size or style of implant previously used and they have a range of reasons for undertaking secondary surgery. Revision reasons may be related to the implant, for example, rupture, malposition or capsular contracture, the impact of the implant on the overlying breast, for example, inframammary crease displacement or double bubble and/or changes to the overlying breast, for example, ptosis, atrophy leading to rippling or visibility of the implants or hypertrophy. As well as having an implant in situ, frequently breast ageing has occurred as well as life events such as pregnancy, breast feeding, menopause and weight changes since the primary surgery.7,8
The extent and complexity of these issues vary considerably from patient to patient. Therefore, thorough breast analysis recognising the variations in anatomy and nuances that increase complexity of surgical planning or affect the clinical outcome is essential. Communication of these differences from primary breast augmentation surgery and education of patients regarding their anatomy and potential outcomes is also essential.
Previous publications have looked at tissue-based planning for primary breast augmentation9-11 or at some or all aspects of breast secondary implant analysis.7,8,12,13 They are primarily analytical tools for the surgeon. We propose a traffic light secondary breast analysis tool that allows for a thorough breast analysis to aid the surgeon in understanding the breast issues at play and to plan secondary surgery as well as acting as an easily understood education tool for patients.
Traffic Light Secondary Breast Implant Classification
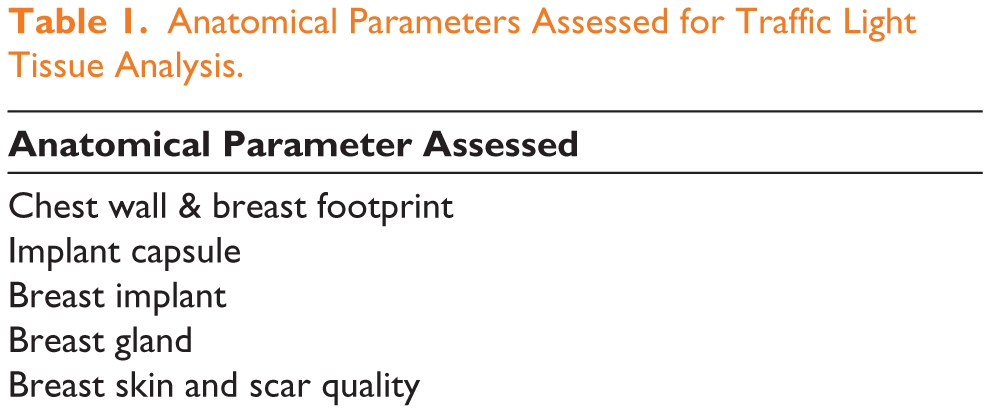
The traffic light classification is anatomically based on analysing the chest wall and breast footprint, the implant capsule, the breast implant, glandular tissue, scar and breast skin quality (Table 1). Each of the above components is assessed, and as well as noting the problem or absence of a problem, the anatomical area is categorised into a level of difficulty. This is where the traffic light system is implemented. Level 1 is categorised as green, Level 2 amber and Level 3 red in increasing order of perceived difficulty in management (Table 2). As well as a reminder particularly for the plastic surgeon early in practice, it is also a visual aid to show patients that easily conveys to them how their anatomy affects surgical planning and clinical outcomes.
Anatomical Parameters Assessed for Traffic Light Tissue Analysis.
Levels of Difficulty Based on Traffic Light Tissaue Analysis.
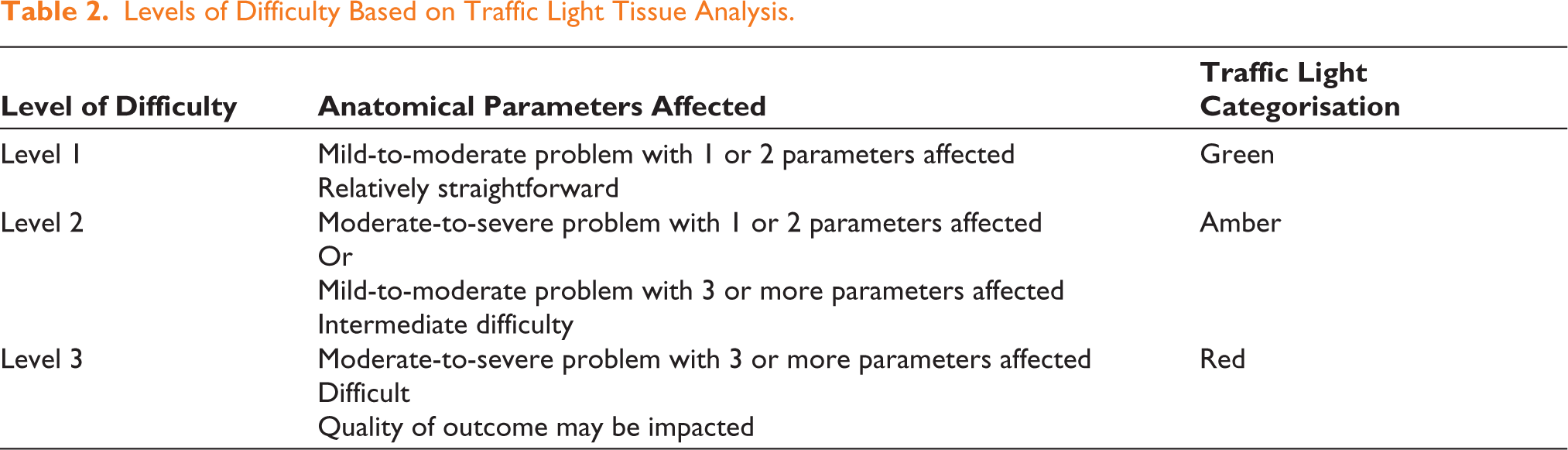
Levels of difficulty one to three are based on the following five parameters:
Breast footprint & chest wall Capsule Implant Gland Scar & skin quality
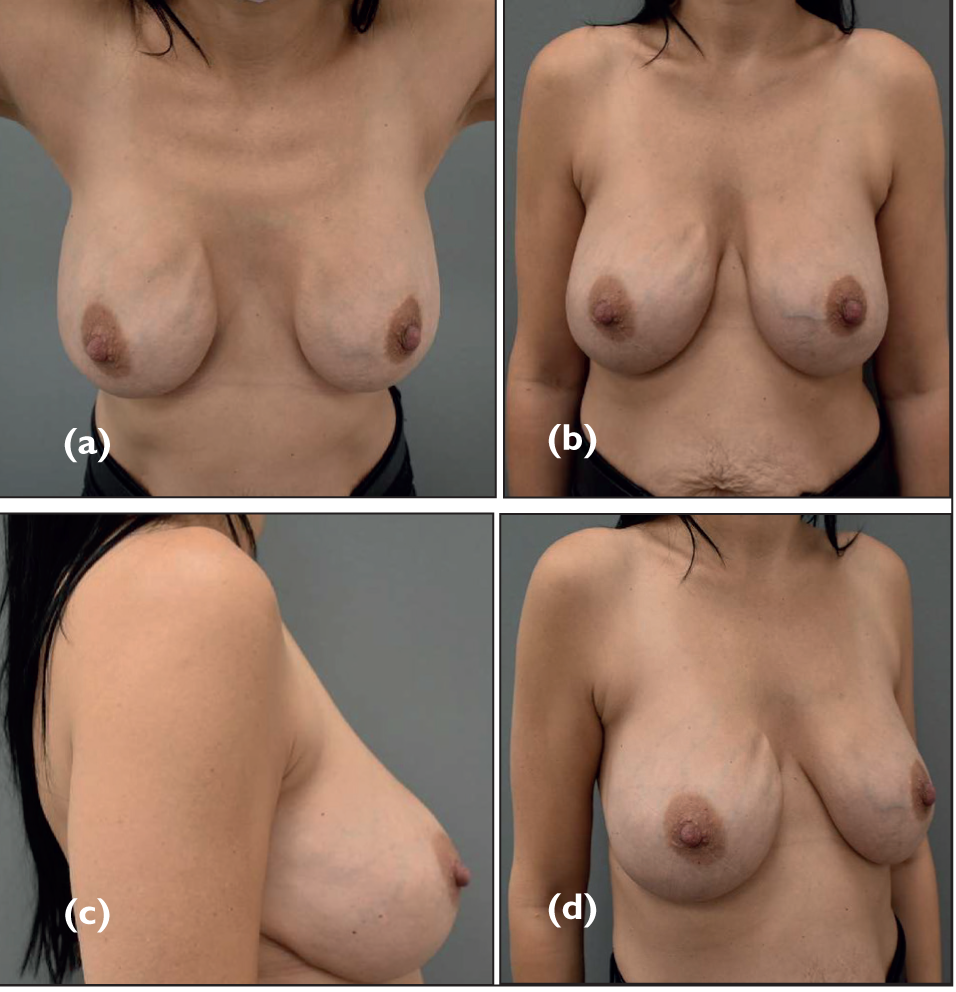
Level 1 (green) is where the surgeon has found a mild-to-moderate problem with one or two parameters affected and normal parameters in the other areas. Most or all of their anatomical analysis do not show impaired tissues. The surgical planning and execution are likely to be straightforward (Figure 1).
Level 1 (green) breast analysis: Chest wall/breast footprint green, capsule green, implant amber (unstable, malpositioning inferiorly), gland green, scar and skin quality amber (thin skin, needed a mastopexy previously). Overall Level 1 (green).
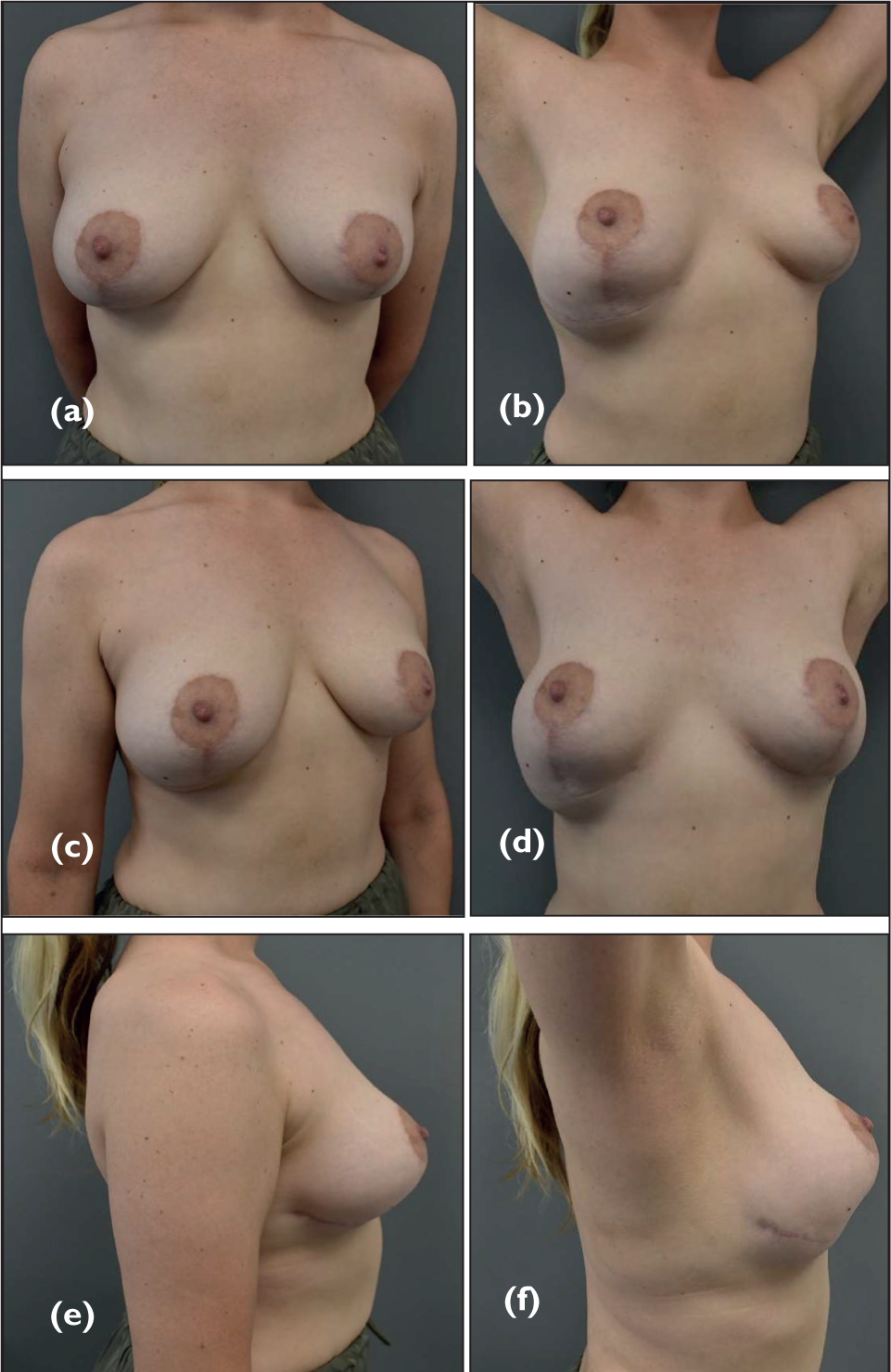
Level 2 (amber) is used when the surgeon has found moderate-to-severe problems with one or two parameters affected or mild-to-moderate problems with three or more parameters affected. The surgical planning and execution are now of intermediate difficulty (Figure 2).
Level 2 (amber) breast analysis: Chest wall/breast footprint green, capsule green, implant amber (too large, base too wide, has dropped below breast footprint), gland amber (thin tissues, ptosis), scar and skin quality amber (thin skin, ptosis, rippling/visibility of implant). Overall Level 2 (amber).
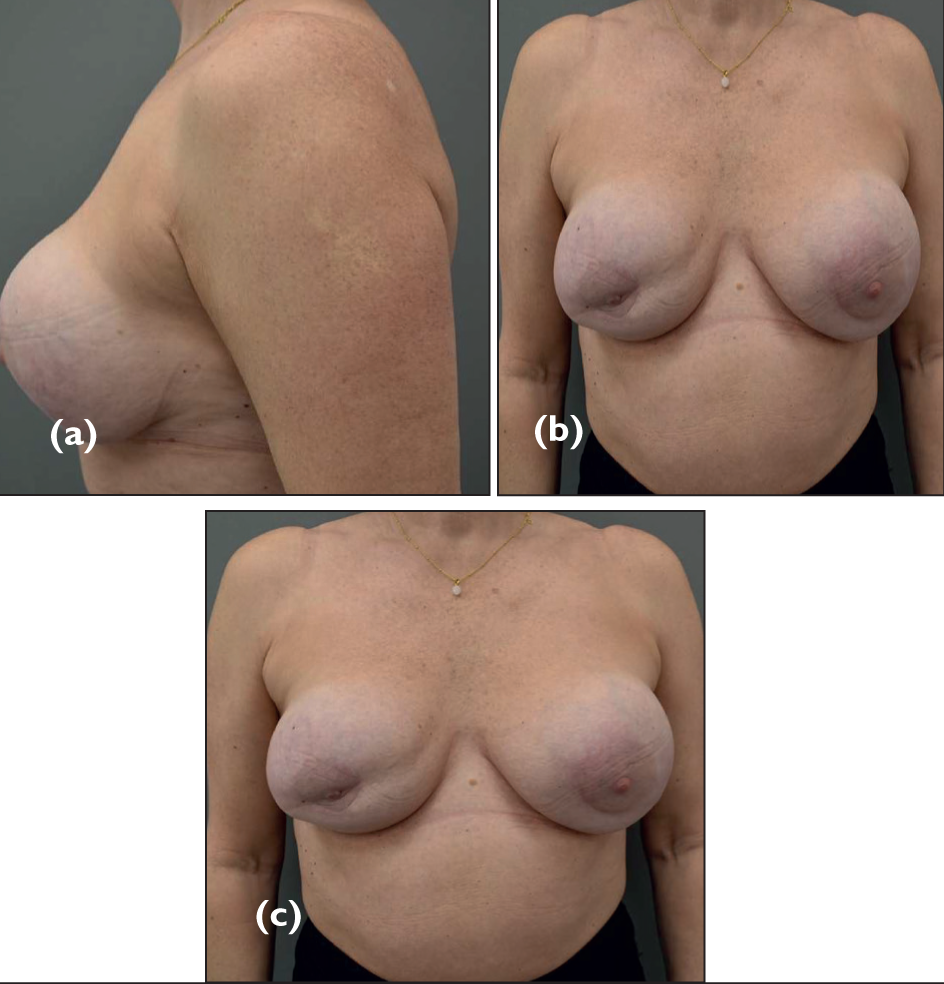
Level 3 (red) is used when the surgical analysis shows moderate-to-severe problems with three or more parameters affected. The surgical planning and execution are difficult, and the clinical outcome and quality of the result may be impacted (Figure 3).
Level 3 (red) breast analysis: Chest wall/breast footprint green, capsule amber (Baker grade IV capsules bilaterally), implant amber (ruptured on ultrasound scan), gland red (thin tissues, deficiency mid breast of tissue both sides, worse on right (implants are subglandular, the visible line is not the pectoralis muscle)), scar and skin quality red (thin skin, previous periareolar scars tethering, ptosis present). Overall Level 3 (red).
Implementation of Traffic Light Classification in Clinical Practice
Intuitively plastic surgeons understand the importance of patient education and patient understanding of their surgery and expected outcome. We develop ways to communicate with patients that become more effective and honed over time as we build experience and understand both our abilities, human tissue anatomical and quality variation and our patients more. 14
The traffic light classification of secondary breast implant anatomy allows the surgeon to perform a systematic analysis of breast anatomy including the main anatomic components that need to be assessed and planned for in the secondary surgery. It also creates a clear visual aid to show the patient so that they can understand their own anatomy. The traffic light colours of green, amber and red are universally known and understood. By educating the patient about their own anatomy, the patient can also understand why a more complex surgery may be needed to correct the concern or achieve their goals and why their secondary surgery may be different or more challenging than their primary breast augmentation. This then leads seamlessly into a discussion about expectations from surgery and aids managing expectations if patients are unrealistic.
Exceptions or Additional Considerations
Of course, there are some exceptions whereby additional considerations or discussions need to take place. If breast implant associated—anaplastic large cell lymphoma (BIA-ALCL) is suspected, this takes precedence until a diagnosis or exclusion has taken place. 15 Patients worried that their silicone breasts implants are or could cause systemic symptoms related to silicone breast implants should have the latest evidence in this area discussed which is moving away from a direct association between silicone breast implants and systemic symptoms16-20 but still need to understand their breast anatomy in the context of secondary procedures such as explantation or capsulectomy.
Discussion
Secondary breast implant surgery is an increasing workload for aesthetic plastic surgeons who perform aesthetic or reconstructive breast surgery. The variation in clinical presentation is huge compared to primary breast implant surgery. Patients may present many years after the original surgery with significant changes in their breast tissue quality over that time.7-10 It is not uncommon that pregnancies, breast feeding, menopause and weight changes have taken place affecting breast tissue since the first implant placement. There are also often implant or implant capsule changes such as malposition, 10 rupture and capsular contracture 9 to treat. All of this leads to a more complex assessment, discussion and surgery for the patient.
A thorough anatomical analysis for secondary breast implant surgery is just as important as tissue-based planning for primary breast augmentation. 7 After this, the secondary surgery (tertiary or quaternary or more in some cases) can be planned more accurately and the level of difficulty or ease predicted. Our tool is not just as a patient education resource. It also ensures the plastic surgeon undertakes a systematic breast analysis and brings each parameter assessed into the surgical planning.
From a patient perspective, understanding their own breast anatomy and how it determines the type of surgery needed as well as the type of outcome possible and realistic is key to success in secondary implant surgery. The use of green, amber and red colours for each anatomical parameter assessed as well as the overall dominant colour in their individual analysis is an easy and clear visual aid to assess with this understanding.
We have kept the traffic light classification relatively simple as this increases its usability in clinic for the surgeon and understanding for the patient. It does not take up much time in clinic as it can be readily incorporated into the routine physical examination and subsequent discussion. We put this forward as a simply implemented logical examination tool that doubles as an educational and communication aid for our patients.
Limitations
The anatomical analysis and classification into a normal, mild, moderate or severe rating is done by the plastic surgeon and is a subjective rating. More experienced surgeons may classify differently than less experienced surgeons However, this is also the level of difficulty they perceive when planning or executing the surgery and so retains a degree of personal accuracy when discussing with the patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclosures
Nora Nugent and Marc Pacifico undertake remunerated educational work for Mentor (Johnson & Johnson). They do not hold any shares or financial interests in Mentor.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.