
Abstract
Introduction:
Injection of the human lips with soft tissue filler is a common instance in daily aesthetic medicine practice. This article aims to clarify particular structural characteristics that define the human lip. Salient clarifications at the anatomical, histological and embryological details are covered, followed by further clarification on anatomical jargon.
Injection technique:
The anterograde needle injection technique and its merits are briefly described through three very different interesting cases that were treated strategically with this technique: case 1: a patient with an ‘inverted cupid bow’ in the lower lip vermilion border; case 2: a patient with maxillofacial asymmetries at the coronal and sagittal planes and sideward ‘tilting’ of the head; case 3: a senile patient with advanced senile lip changes.
Conclusions:
Important conclusions are drawn upon the characteristics that define the human lip; an accurate lip injection technique is achieved through detailed knowledge of lip anatomy jargon. In this article, the white lip roll is defined in terms of a particular living anatomy observation. The term ‘Anterograde Needle Injection Technique’ is coined, with citations from previous authors also being covered. Haemodynamic and technical observations are made regarding the merit of using the 27G needle versus the 30G needle. The anterograde needle injection technique can serve a strategic role in making complex or unusual lips easier to treat. The concept of the ‘Rheological Sum’ is coined to highlight the salient decision-making steps that injectors cover in daily practice for any given treatment. This is an especially important and delicate consideration for lip treatment with soft tissue filler.
Introduction
When we refer to the lip in common parlance, we almost always have in mind the red part of the lips, but when we speak about lips in the world of plastic surgery or aesthetic medicine, we do keep in mind that there is one ‘lip’, which we subdivide into a ‘white part’ and a ‘red part’. The dry part of the red lip is the proper owner of the term ‘vermilion’. 1
We can still slip into inaccuracy if we say that the lip is a unique feature of the human body: it really is not so. At a histological level, our lips are merely a transitional mucosa, something that we see in many other species, be it fish, mammals or others. 2
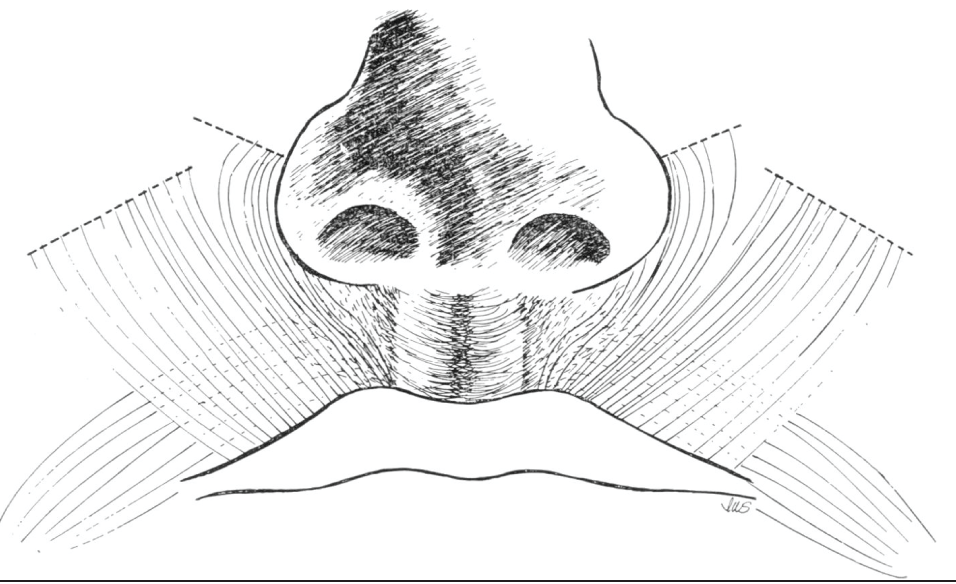
What is truly a unique feature of the human lip is the shape of its contour: the ‘vermilion border’. 3 We owe this to the muscular origins, insertions and decussations of the intrinsic and extrinsic peri-oral apparatus. These contribute to the outline of our lips in the early stages of foetal development. 4 Also thanks to this muscular arrangement, the human lips can achieve another important feature that is quite unique to us: the articulation of speech.
Anatomical Jargon
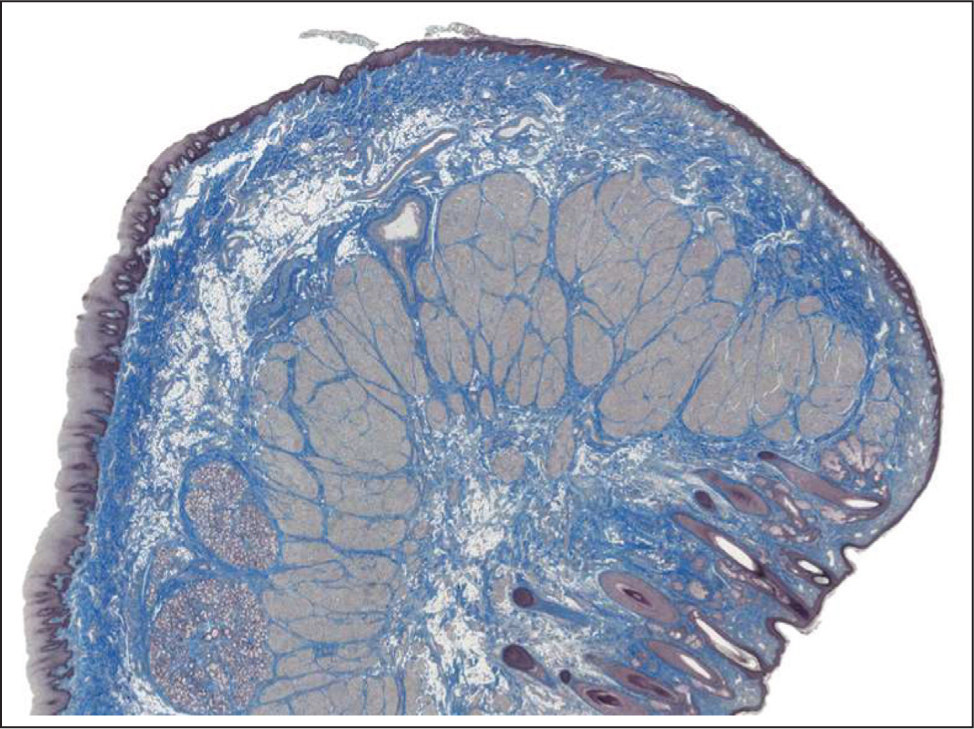
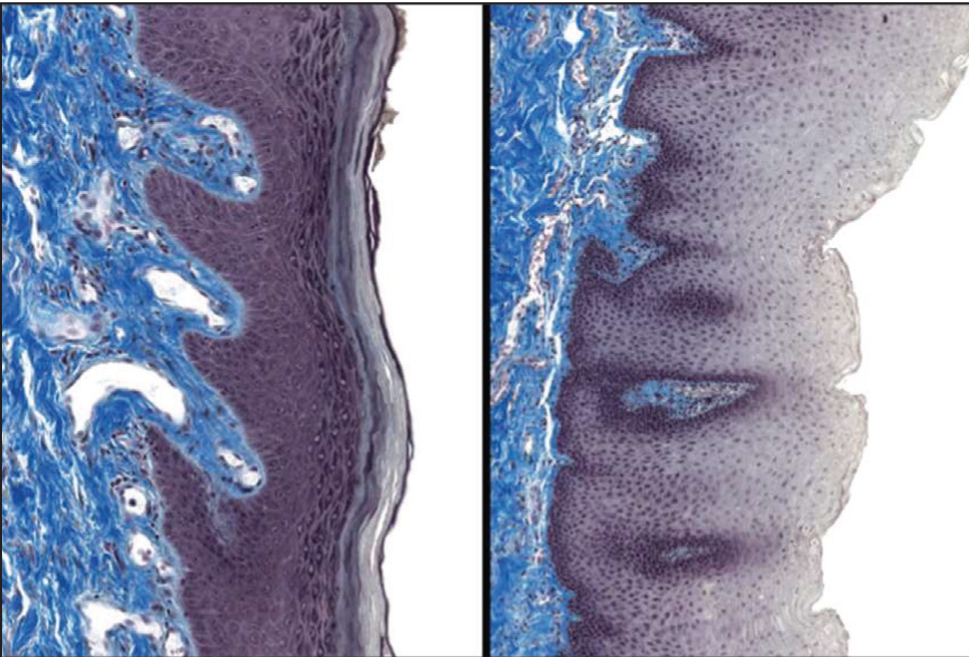
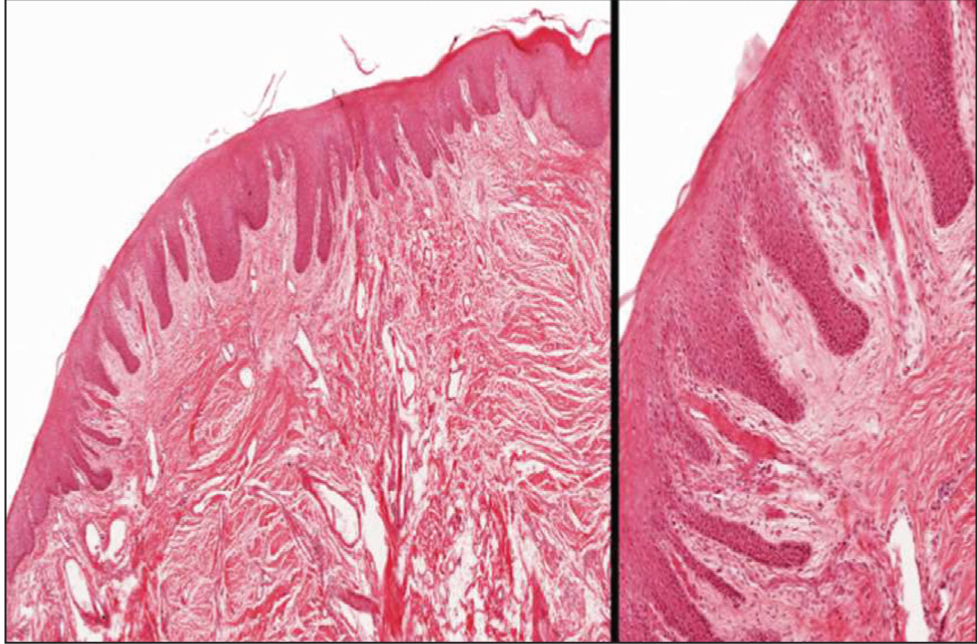
Further from what has already been said, some more clarification on the jargon of lip anatomy and histology is still due. The white lip is covered in skin, and the red lip is covered in hairless mucosa. The dry part of the red lip (vermilion) is covered in transitional mucosa, and it looks red because the keratinocytes of this region are relatively thinly keratinised and, therefore, proportionately richer in transparent eleidin. 5 The epithelium and underlying lamina propria also have more numerous papillae, and the superficial blood vasculature is richer. 6 The wet lip, on the other hand, is a buccal-type mucosa, and it is much richer in minor salivary glands and therefore no longer a vermilion-type mucosa (Figures 1–3).

The limit of the vermilion is of course the vermilion border. One last important feature that is often omitted from anatomical diagrams is the white lip roll: in living anatomy, this is seen as a fine rim of white lip that is just outside of the vermilion border, upon which falls a thin white rim of ambient light. 3
Distinguishing the white lip roll from the vermilion border is of crucial importance if one wants to perform an accurate vermilion border injection technique, such as will follow in this article (Figure 1).
Finally, the Glogau-Klein points, cupid’s bow, philtral columns and philtral fossa are all intimately related to the vermilion border, the white lip roll and the extrinsic and intrinsic peri-oral muscular decussations (Figure 2). 4
Injection Technique
For the majority of cases, the vermilion borde should be exploited during lip injection with soft tissue filler, provided that a well-defined and natural result is achieved. Often either a cannula or a needle is used, with retrograde injection. In this technique, the needle pricks two or three times along the border of each half lip. A third technique exists, which is the least traumatic and the least painful for the patient, where the needle is used to prick the vermilion border once for every half lip. It is often avoided or overlooked because the filler needs to be ‘trusted’ to flow in the correct direction by itself, with an anterograde technique.7,8 Since inaccurate injection can make the filler flow overboard into the white part of the lip, this technique is avoided by many. However, mastering it with care and accuracy can give superior results in terms of no need for anaesthesia, very small chances of ecchymoses or haematomas, avoiding filler accumulation into the white lip over time and easily obtaining very natural results—especially when a particular lip feature needs to be preserved. 3 Respecting all the components of the lip anatomy is always of crucial importance, but this is especially important for the anterograde needle injection technique.
The author would like to add one further technical consideration for this technique: although a 30G needle has often been suggested for this use, 7 in truth, it is easier and safer to make use of a 27G needle. 3
The vermilion border is a connective tissue with an elastic limit, and it could lose continence for filler if it is overtreated or mishandled. In truth, under equal extrusion force, a wider 27G needle would produce a gentler flow rate of the same soft tissue filler, precisely because it is wider. This is an age-old law of fluid dynamics that was first described by Castelli when he studied the flow of rivers. 9 In modern medicine, Castelli’s law is more known to vascular surgeons who perform haemodynamic assessments of the lower limb venous system. 10 In the author’s experience, the wider diameter of the 27G needle also allows for better positioning of the needle along the correct direction for injection. 3
At a molecular level, the filler’s physical properties are better safeguarded if the needle gauge used by the injector is that which is supplied by the manufacturers who designed the product. The needles supplied for lip fillers usually are 27G.
Three interesting cases will follow, where the anterograde needle injection technique is used not only for its own purpose of defining the vermilion border but also to serve other significant purposes within the same treatment plan.
Case 1: Preserving an unusual lip feature.
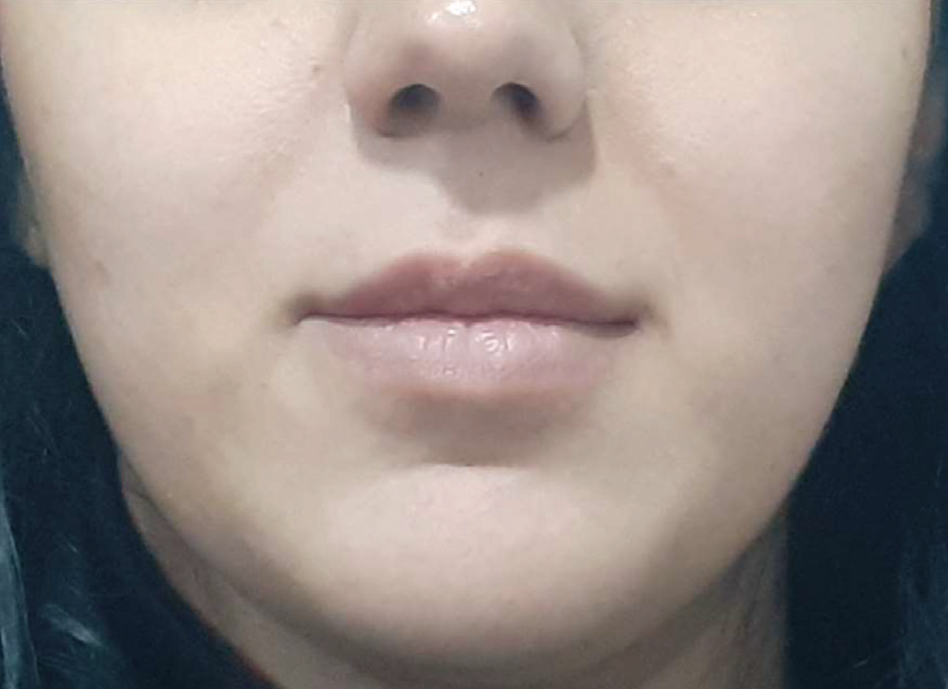
A 25-year-old lady presents for lip augmentation for beautification purposes. She has an interesting innate anatomical feature: A ‘cupid bow’ and a ‘fossa of Venus’ in the lower lip. This is an uncommon feature, which usually occurs in male subjects. However, it did not give a masculinising appearance to this young patient, and it was agreed to preserve this interesting shape. The vermilion border technique was therefore used to make the filler follow along the natural shape of the patient, and the feature was successfully preserved (Figure 6).
An Unusual Feature of the Lower Vermilion Border (a Cupid’s bow) Is Successfully Preserved, Using the Anterograde Vermilion Border Technique.

Unfortunately, since augmented lips also suffer an augmentation of any dynamic asymmetries (usually seen during consonant pronunciation), on a second treatment the cupid bow of the inferior lip was removed using a different vermilion border technique in the centre of the lower lip, to correct this feature. The result was a graceful heart-shaped lip (Figure 7).
In a Subsequent Session, the Central Portion of the Vermilion Border Was Treated with Conventional Retrograde Needle Injection, Due To Dynamic Asymmetries Noted by the Author. The Result is a Graceful Heart-shaped Lip.

Case 2: A patient with maxillofacial asymmetries along the coronal and sagittal planes.
This young patient’s lip asymmetry was due to significant underlying skeletal asymmetries along both the coronal and sagittal bony axes (Figures 8 and 9). Maxillofacial surgery was not being considered at all by this patient, but she had received soft tissue filler in the past to achieve some compensation at the soft tissue level.
Apparent Soft Tissue Asymmetry Is Seen To Be Due To Underlying Skeletal Misalignment Along Both the Sagittal and Coronal Planes.

Apparent Soft Tissue Asymmetry Is Seen To Be Due To Underlying Skeletal Misalignment Along Both the Sagittal and Coronal Planes.

Injecting the vermilion border with this technique allowed the author to obtain a judgement of what she considers as the ‘innate rheology’ of the patient’s lip tissue. 3 Thereby, an estimate of the volume of filler that was then to be injected into the wet-dry border could be calculated, based on the clinical impression of the tissues’ interaction with the filler that had been used at the vermilion border. These considerations put together could be called the 'Rheological Sum'. For this case, the rheological considerations helped with two different aspects of symmetry: morphological symmetry (having an equal looking upper lip) and textural symmetry (having an equal-feeling upper lip, as much as possible). Since the filler contained a small percentage of lidocaine, the relatively painful vertical lip injections were saved for last to achieve further symmetry under pain-free conditions. This helped to avoid asymmetries caused by formal local anaesthesia methods or by the additional related swellings or haematomas that could occur.
After treatment, the patient’s neck position is seen to have improved—the nostrils stand on the same plane when the standing patient faces the camera. In maxillofacial surgery terms, there is evidently less ‘tilting’. This seems to be due to optimised lip proprioception feedback mechanisms after lip filler treatment (Figure 10).
Soft Tissue Compensation Is Achieved Through Lip Filler Treatment in the Right Half of the Upper Lip. The Patient’s Neck Position When Standing Is Seen to Have Improved, the Nostrils and Chin Follow the Horizontal Plane Better and There Is Less ‘Tilting’. Possibly This Is Due To Optimised Lip Proprioception Feedback Mechanisms.
It appears that a simple lip filler treatment has achieved some important postural improvement in this patient’s case, despite the underlying bony asymmetries.
Case 3: A senile patient with advanced senile lip changes.
A 77-year-old patient with a long history of sun exposure and smoking and with a body mass index that was below the ideal healthy range.
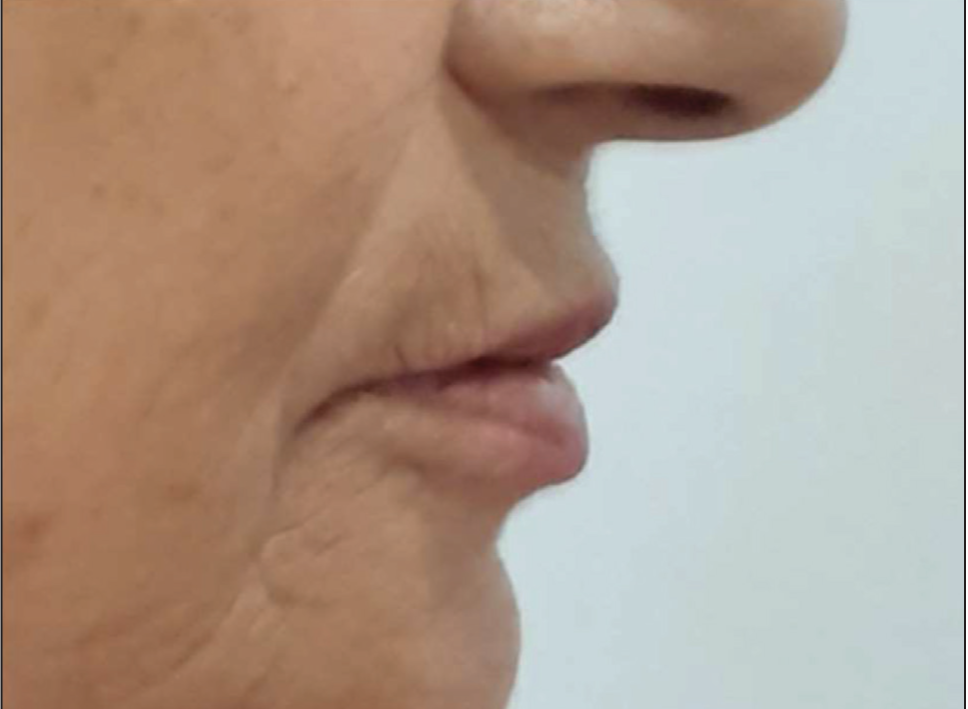
This elderly patient desired an increment of the vermilion area. Although it is theoretically postulated that a lip filler treatment would improve peri-oral rhytids and white lip projection, it is often wiser not to promise heavily on these items at the pre-treatment stage. In this case, there was a very reasonable improvement. Most importantly, since this technique offers a very natural result, the treated lips do not look out of context with respect to the senile facial features in the background (Figures 11 and 14).
Advanced Senile Changes of the Lips in a Senile Patient with a Long History of Smoking and Sun Exposure and a Sub-optimal Body Mass Index. Peri-oral Rhytids Are Seen to Encroach on the Vermilion Border and Reach Into the Red Lip.

After Treatment, the Peri-oral Rhytids Are Significantly Improved and the Red Lip Is Reasonably Incremented. The Natural Result Is Not Out of Context with the Background Senile Features.

A natural result is of great importance, especially for mature patients, patients with a reserved character or patients where societal values do not openly embrace medical procedures for aesthetic purposes.
Senile lips offer a soft innate rheology and therefore a sturdier filler rheology, but a reasonably agreeable viscosity is required. Once again the considerations of the 'Rheological Sum’ are applied to the patient’s tissue characteristics and the soft tissue filler properties. 3 Every injector makes these considerations actively or automatically, but perhaps it would be better to formalise this concept, especially where such a delicate soft tissue structure as the lip is concerned.
The improvement of peri-oral rhytids is more appreciable in the anterior view (Figures 11 and 12), whereas the improvement of the B line and S line are appreciated in the lateral view (Figures 13 and 14).

Conclusions
The lip is a transitional mucosa, and as such lips are not unique to humans. The human lip is unique for its shape and for the contour of the vermilion border. Accurate knowledge of lip anatomy jargon is highly important and translates into accurate injection techniques. The living anatomy of the white lip roll is given further formal description. The anterograde needle injection technique, though seemingly ‘difficult’, can make complex lips easier and more interesting to handle. Apart from serving to define the vermilion border of the lip, this technique can be used as a strategic step to complement or serve other purposes within the same lip treatment plan. Under equal extrusion force, a 27G needle gives a gentler flow rate than a 30G needle for a given filler, based on Castelli’s law of fluid dynamics.. The performance of a soft tissue filler’s rheology also depends on the patients’ ‘Innate Rheology’ of the tissues. These observations could be considered as the’ Rheological Sum’ of the patient’s tissue characteristics and the soft tissue filler rheological properties. This is an especially important and delicate consideration for lip treatment with soft tissue filler.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.