
Abstract
Parry–Romberg syndrome (PRS), also known as progressive hemifacial atrophy, is a rare disorder characterised by slow and progressive hemifacial atrophy. The treatment offered for the syndrome generally aims at improving aesthetics. Microsurgical reconstruction is the standard method of treatment. Free flaps using rectus abdominis and Gracilis muscles are used to restore facial contour. Bone graft, orthognathic surgery and bone distraction are also sometimes required. Currently, autologous fat grafting is increasingly used for the correction of facial atrophy. In this study, we report a series of 15 PRS cases treated by lipotransfer. Most of them required a second and some required a third injection. A total of 36 procedures were done. Fat was harvested from the abdomen. Significant improvement in facial symmetry was achieved in all patients. Lipotransfer is a simple and effective treatment for PRS; it obviates the need for more extensive and expensive microsurgical procedures.
Introduction
Parry–Romberg syndrome (PRS), or progressive hemifacial atrophy, is a rare disorder characterised by slow, progressive deterioration (atrophy) of the skin and soft tissues of half of the face (hemifacial atrophy). Progressive hemifacial atrophy was described by Parry in 1825 and better studied by Romberg, in 1846.1,2 Also known as PRS, this rare disorder is characterised by unilateral facial atrophy, which affects the skin, subcutaneous, muscle and rarely, osteo-cartilaginous adjacent structures. The left hemiface is the most affected, and it can spread to the ipsilateral hemibody. 3
PRS involves dermatomes or multiple branches of the fifth cranial nerve. 4 Its aetiology is unknown, suggesting a pathogenic factor such as autoimmunity, an abnormality of the trigeminal nerve, cervical-facial trauma or infections.3,5 It begins in adolescence, in general in the first or second decade of life. It is more common in females than in males, 6 and usually begins between the ages of 5 and 15 years, and then it becomes stationary. Cases of disease onset in adulthood have been reported as well. PRS may also be accompanied by neurological abnormalities, optic nerve damage, alopecia and pigmentations. The cause of PRS is unknown, and currently, there is no cure for the disease.
The atrophy progressively spreads involving the skin and its adnexa, as well as underlying subcutaneous structures such as connective tissue (fat, fascia, cartilage, bones) and/or muscles of one side of the face. 6
The syndrome is sometimes associated with a depressed linear scar extending down the forehead on the affected side. This scar is referred to as a ‘coup de sabre’.3,6 Enophthalmos (recession of the eyeball within the orbit) is also seen commonly. 7 The tissues of the mouth, including the tongue, gingiva, teeth and soft palate, are sometimes involved in PRS. 8
Treatment of PRS entails flap reconstructions which demand special expertise and are quite expensive.
There are several alternative treatments for correction of facial defects, such as fat, cartilage or bone graft, or alloplastic material tantalum, acrylic and silicone implants. 4
Autologous fat grafting has the advantage of a better cost-benefit, improved skin texture and more natural contours and facial expressions. However, unpredictable loss of volume due to reabsorption of the fat in the recipient area is still a limiting factor for this procedure.
Materials & Methods
The study was conducted at Cosmetic Surgery Centre Ltd, from October 2005 to January 2020. Fifteen patients with PRS were treated. All the patients were females. The age range was 14-39 years. The diagnosis was made based on the history and clinical examination. A total of 36 procedures were done.
Preoperative photographs were taken at different angles for postoperative evaluation of the result of treatment. The patient was explained about the lipoinjection procedure, especially about the fact that she will require further sessions of lipotransfer (usually two to three), depending on the amount of fat absorption that takes place postoperatively. Retrospective data from a private plastic surgery centre in Dhaka was collected from patient records to review the number and outcome of lipotransfers.
Procedure
After careful preoperative markings, general anaesthesia was employed. Fat harvesting was then done from the lower abdomen using a thin liposuction cannula. Low negative suction pressure was used to avoid fat cell injury during the liposuction procedure. The lipoaspirate was then kept upright in the syringes to allow separation of the liquid fat and also the red blood cells. Repeated transfer of the fat between two syringes under airtight conditions was then done. Small aliquots of fat are deposited in the affected areas by cannula. Multiple passes are made in different directions to maximise the volume of fat injection, while at the same time avoiding injection of too much fat in one point. Ports were closed by a single 6/0 Vicryl stitch.
Postoperative evaluation was made to see the amount of fat resorption at the end of one, three and six months. Out of the 15 patients treated, 13 received a second lipoinjection after six months and eight received a third injection after one year of the first procedure. Two patients were lost to follow-up after the first injection.
Results
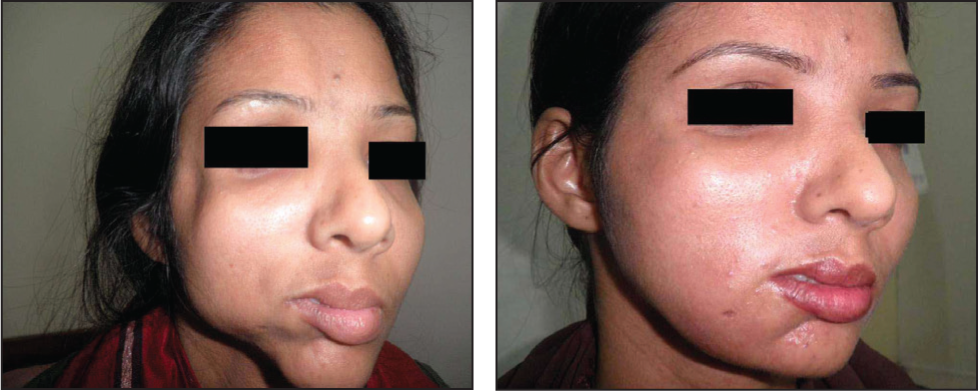
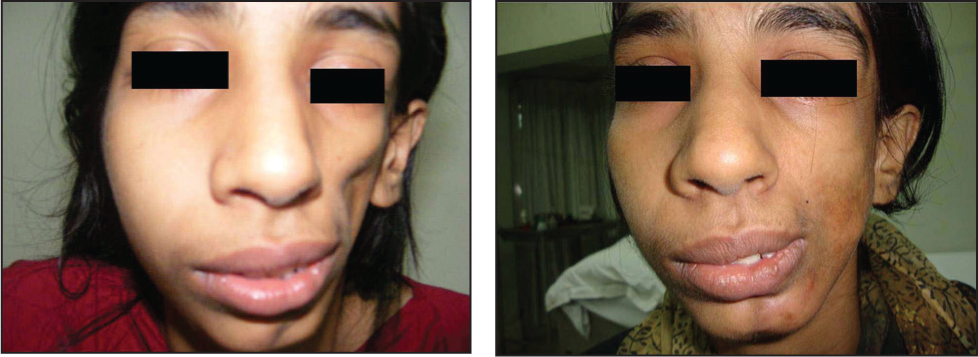
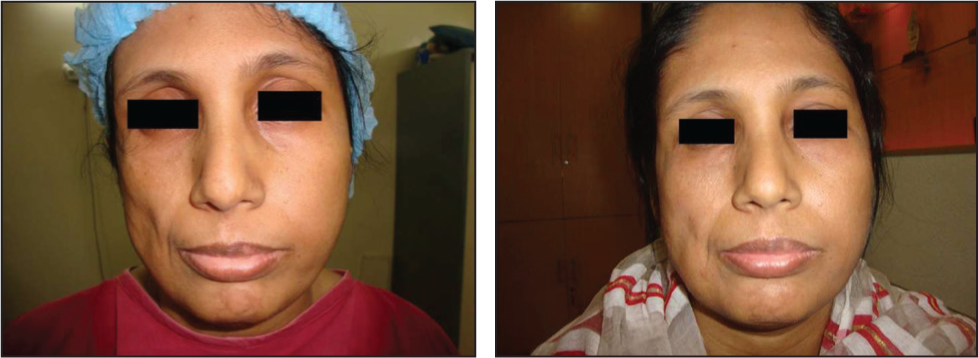
Significant soft tissue augmentation was achieved in all the cases (Figures 1, 2, 3 and 4). Photographs taken after three months revealed some amount of volume loss (Figure 5) in all the patients, but enough remained to show significant improvement as compared to preoperative pictures (Figure 6). After the second and third injections, further improvement in facial contour was achieved. Out of the 15 cases, two were lost to follow-up because they got married and decided not to continue further treatment.
Right Hemifacial Atrophy in a Young Lady—Before and After Three Months of Lipotransfer.
Another Girl with Left-sided Hemifacial Atrophy—Before and After Three Months of Lipoinjection.
Another Lady with Parry–Romberg Syndrome Presented with Right Hemifacial Atrophy—Before and After Lipoinjection.
Young Girl 10 Days After Lipoinjection.
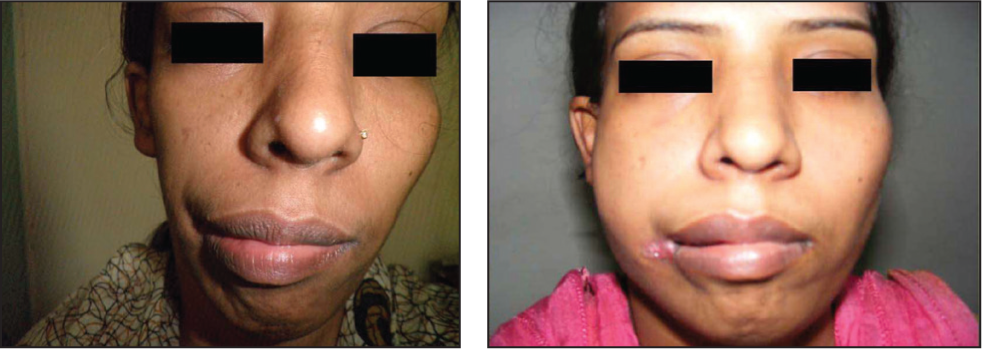
The Same Patient as in Figure 4, Showing Absorption of Fat from the Treated Areas at Three Months—Compared with a Picture on 10th POD.

Result After 10 Days and Three Months of Lipoinjection.

All the cases gave a history of progressive loss of volume on one side of their face, but none had any neurological abnormality. Twelve out of 15 patients were unmarried when treatment was started.
Discussion
Unilateral atrophy of the face, as described in the case above, is a clinical symptom that occurs in different diseases. Diagnosis can be difficult, especially at the beginning of the condition. Progressive hemifacial atrophy, also known as PRS, is characterised by progressive unilateral atrophy of the facial tissues. 6 Aetiology of PRS is not established yet, and probable causes are neuritis of the trigeminal nerve or changes in the sympathetic nervous system. 4 Other causes of unilateral facial atrophy include the Goldenhar syndrome and facial trauma.
In general, the treatment offered for PRS patients aims at improving their physical appearance. In this specific case, reconstructive surgical treatments should be assessed after clinical inactivity of the disease. Treatment by immunosuppressive drugs, chloroquine and calcipotriol has been discussed by some authors, 9 but there is still no scientific evidence for their use to treat PRS.
The treatment often offered for the syndrome is based on the replacement of tissue that was lost due to atrophy. 10 The standard method of treating PRS is by microsurgical reconstructive surgery. Free flaps using rectus abdominis, latissimus dorsi or Gracilis muscles are utilised to restore a more normal contour to the face. 11 Additional procedures, such as bone grafts, orthognathic surgery and bone distraction, are also sometimes required. The timing of surgical intervention is controversial; some surgeons prefer to wait until the disease has run its course, 2 while others recommend early intervention. 12
Autologous fat graft is preferred because it is readily available, and easy to harvest, and there is no risk of rejection. The main disadvantage is reabsorption, which is somewhat unpredictable. 10 Rarely, swelling, hematoma or seroma can appear in the donor or recipient site. Loss of vision due to fat embolism after fat grafting can be an extremely rare complication. 13
Alternative methods used for treating PRS are injections of hyaluronic acid, bone autograft, acrylic prosthesis, hydroxyapatite and alloplastic implant can be used. However, these materials can lead to infection and extrusion. 14
An average lipoinjection procedure takes less than an hour, whereas a free flap can take several hours. Microsurgical reconstruction also requires a bigger surgical team and extensive instrumentation. It is, therefore, much more expensive than a lipoinjection procedure. 11
Conclusion
With the introduction of lipotransfer as an effective means of soft tissue augmentation, lipoinjection has become a simple and effective alternative to the more extensive microsurgical operations.
Footnotes
Acknowledgements
The authors acknowledge that this study has been accepted for presentation at the ASiT Surgical Conference, March 2025 (Association of Surgeons in Training), United Kingdom.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.