
Abstract
Objective:
To discuss the TULUA (transverse Plication, no undermining, unrestricted liposuction, Umbilical Amputation with neo-umbilicoplasty, Abdominoplasty) impact, widespread adoption, and surgeon’s acceptance in improving safety and aesthetic outcomes, while contrasting it with established methods.
Background:
Traditional abdominoplasty, practiced for over a century, often involves extensive flap dissection, vertical plication, umbilical transposition and restricted liposuction, leading to complications such as necrosis, poor scarring and aesthetic dissatisfaction. TULUA introduces an innovative, vascular-preserving approach that reduces complications and enhances results.
Methods:
This study examines the surgical technique of TULUA, encompassing patient selection, preoperative markings, operative steps and postoperative care. The rationale behind the surgical modifications is explored, highlighting the technique’s application in aesthetic and reconstructive procedures, including TULUA-DIEP for donor site closure in breast reconstruction.
Results:
Clinical evidence reveals TULUA’s significant advantages: reduced necrosis, minimised wound closure tension and superior aesthetic outcomes. These include improved contouring, optimal umbilical shape and positioning and lower scar placement. Its proven safety has driven widespread adoption in aesthetic and reconstructive surgery.
Discussion:
TULUA shifts from vertical plication to a transverse technique, prioritising blood supply preservation and enabling safe, unrestricted liposuction. This method achieves enhanced outcomes, aligns with modern surgical reasoning and establishes TULUA as a reference for safety and efficacy in abdominoplasty.
Conclusion:
TULUA reduces complications and improves results, with future developments in laparoscopic techniques and new technologies promising to expand its applications further.
Introduction
For over 125 years, abdominoplasty has been a central procedure in plastic surgery, evolving incrementally to meet patient demands and improve outcomes. However, many of its traditional practices; including wide flap dissection, vertical plication and combined liposuction; were associated with significant complications such as necrosis, wound dehiscence and unsatisfactory scar positioning. 1 The TULUA abdominoplasty (an acronym for transverse plication, no undermining, unrestricted liposuction, umbilical amputation with neo-umbilicoplasty, abdominoplasty) introduced in 2011, 2 revolutionised this field, offering a safer alternative by modifying established paradigms. 3
TULUA was initially developed to address complex cases. Its key innovations included preserving flap vascularity by avoiding dissection above the umbilicus (no undermining), performing transverse rather than vertical plication, and allowing unrestricted liposuction for improved contouring. Over time, these techniques proved not only safer but also aesthetically superior, gaining widespread adoption globally (Table 1).4,5
TULUA Acronym Based on Abdominoplasty Paradigm Shifting.
This article delves into the origins, principles and evolution of TULUA, answering pivotal questions that catalysed this paradigm shift. It also provides a comprehensive overview of the surgical technique and discusses its impact on aesthetic and reconstructive applications.
Methods
TULUA Technique Surgical Description 6
Patient Selection
TULUA abdominoplasty is most suitable for patients aged 18-60 who have indications for abdominoplasty, such as wall laxity, excess skin and fat and without significant diastasis recti or epigastric hernias. Contraindications include obesity, active smoking and uncontrolled comorbidities. Proper preoperative evaluation, including thromboembolism risk assessment and detailed patient counselling, is essential.
Preoperative Markings
Preoperative markings are performed with the patient standing, emphasising a low transverse scar placement 6 cm above the vulvar commissure or penile base. Upward traction is applied while determining the mark on the mons. The planned incision length is tailored to patient-specific anatomy to prevent dog-ear deformities. The upper resection limit typically encompasses or exceeds the umbilical level.
Liposuction
After tumescent infiltration, unrestricted deep and superficial liposuction is performed on the abdomen, flanks, back and complementary areas. Care is taken to maintain uniform flap thickness to ensure optimal contouring. The epigastrium is thoroughly thinned, addressing both deep and superficial planes without concern. After flap advancement and wound closure, additional superficial liposuction is performed through the neo-umbilical opening along the linea alba above the umbilicus, as well as from the lower incision to the costal margins, to enhance the definition of the semilunar lines. The total liposuction volume typically averages 4,000 cc (ranging from 100 to 7,200 cc). The author uses conventional liposuction techniques and does not prefer powered handpieces or additional energy-based devices for fat emulsification or tissue contraction. 7
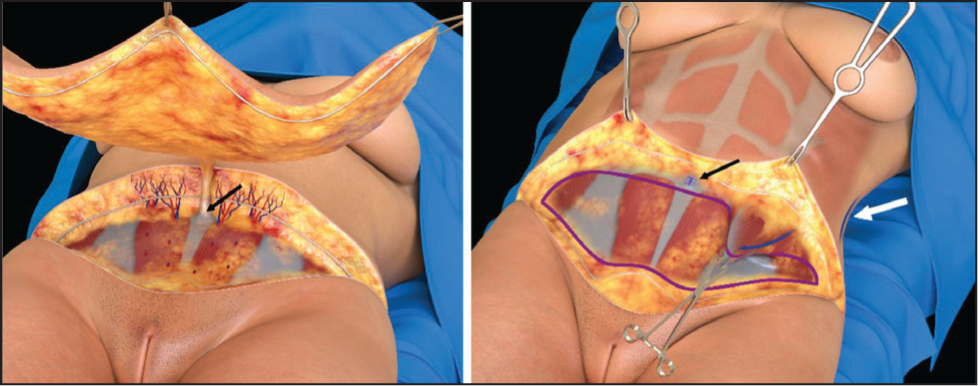
Pannus Resection
An en bloc resection is recommended, with dissection stopping at the umbilical level. 8 A bevelled incision in the suprapubic area preserves fat and prevents step deformity during closure. The resection is performed in the supra-muscular plane, carefully fulgurating or ligating individual perforators to control bleeding. The umbilical stalk is circumferentially dissected, milked and sectioned, followed by secure closure of the umbilical ring. In secondary cases or based on surgeon preference, pannus resection can be deferred to closure, though this may extend the surgical time (Figure 1).
Transverse Plication
The operating table is flexed at 30°, and the patient is fully relaxed with appropriate medication. A transverse plication is performed from the umbilicus to the pubis, extending between the anterior iliac spines (10-14 by 25-32 cm), with dimensions tailored to each patient. Vertical plication is avoided but may be considered in cases of significant diastasis, where a vertical tunnel is dissected above the umbilicus to complement the transverse plication. Polypropylene 0 is used for transverse plication, and polyglactin for vertical plication if needed.
Wound Closure
Layered closure minimises tension and ensures an aesthetically pleasing scar. Scarpa’s fascia is sutured with 2-0 polyglactin, and progressive tension sutures may be used to reduce seroma risk in the presence of dead space. A subdermal layer is closed with individualised stitches, followed by running sutures in the dermal plane. Suction drains are recommended, typically inserted through the incision, though some groups achieve acceptable results with a drainless technique. 9
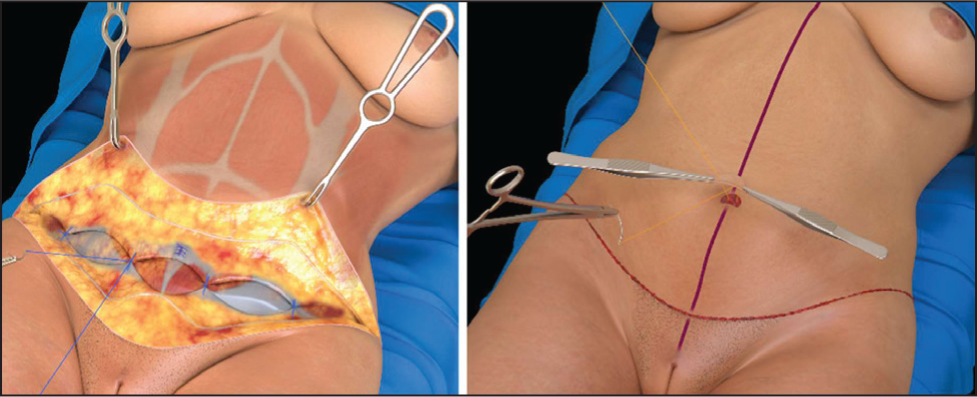
Neo-umbilicoplasty
After the native umbilicus is amputated, a new one is created using a small graft. Proper positioning, typically 9-9.7 cm above the incision along the midline, is recommended. An inverted U incision is made, followed by periorificial defatting to shape the area. The neo-umbilicoplasty is completed by placing a skin graft at the base of the new umbilicus, which is securely fixed to the linea alba using catgut sutures (Figure 2).
Postoperative Care
Patients are given compression garments, encouraged to ambulate early and receive thromboprophylaxis as needed to prevent venous thromboembolism. Drains are removed between 5- and 12-days post-surgery, based on individual progress. Follow-up visits monitor healing and address concerns. Notably, no postoperative massages or additional therapies are used, simplifying recovery.
Discussion
The TULUA technique has redefined abdominoplasty by challenging long-standing paradigms. By prioritising vascular preservation, reducing complications and enhancing aesthetic outcomes, it has set a new standard in abdominal surgery. Clinical studies have validated its safety and effectiveness, reporting reduced necrosis rates and improved aesthetic scores. Its acceptance is growing, with the potential for global reach and widespread adoption. 10
Questions that Shaped TULUA
Can liposuction and abdominoplasty coexist safely?
Historically, combining liposuction with abdominoplasty was considered risky due to concerns about vascular compromise.11–15
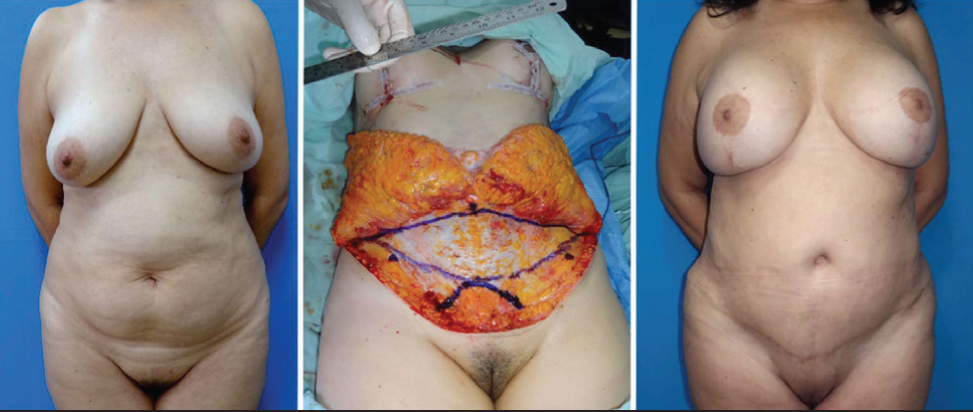
By preserving flap vascularity and incorporating liposuction into the overall contouring strategy, TULUA enhances aesthetic outcomes without increasing complication rates. The technique extends the concept of ‘no undermining’,16,17 ensuring the preservation of direct perforators from the superior epigastric artery that supplies the fat and skin above the umbilicus within its angiosome. TULUA’s approach incorporating ‘no undermining’ allows unrestricted liposuction even in traditionally ‘danger zones’18,19 proving that these procedures could coexist safely (Figure 3).
Is diastasis recti correction the same as abdominal wall laxity correction, or are they distinct conditions requiring different approaches?
Vertical plication has been the standard method for correcting diastasis recti for over a century.20,21 However, this approach often neglects the complex and multivectorial nature of abdominal wall laxity, which can result from pregnancy, weight fluctuations, ageing, trauma or prior surgeries. While vertical plication can effectively reduce the interrectus distance, it requires extensive dissection that may compromise the blood supply to the overlying skin and fat. Furthermore, vertical plication pulls tissues toward the midline, often leading to complications such as midline bulging (the ‘dome effect’) and vertical skin sagging.
Experimental studies highlight the advantages of transverse plication, which aligns with the natural tension lines and dynamics of the abdominal wall muscles. This approach provides broader correction of abdominal wall laxity and enhances wall tensioning beyond the plication site. 22 Transverse plication facilitates downward and medial repositioning of the rectus muscles, reducing the interrectus distance while preventing rebound or compensatory epigastric bulging. 23 Additionally, it advances the external oblique muscles downward and inward, improving waistline definition and overall abdominal contour. 24
The long-standing paradigm of relying solely on vertical plication in abdominoplasty warrants reconsideration. Transitioning to transverse plication or combining transverse with vertical techniques25–27 offers superior outcomes by addressing the distinct characteristics of abdominal wall laxity. Ultimately, diastasis recti correction and abdominal wall laxity correction are separate challenges that require tailored approaches. In the absence of very wide and pathological diastasis, using isolated transverse plication, indicated in most cases, provides a balanced and highly effective solution, optimising both functional and aesthetic results (Figure 4). 28

Is wide flap dissection necessary to advance down the epigastric skin, or could it be avoided?
Traditional abdominoplasty often relied on extensive flap dissection to facilitate vertical plication, umbilical transposition and the downward displacement of the upper flap to cover the resection defect. However, this approach created significant dead space and often required excessive undermining, increasing the complexity of the procedure. 29
No undermining techniques have demonstrated that wide flap dissection is unnecessary. Discontinuous dissection combined with unrestricted liposuction effectively loosens the flap, enabling it to slide downward easily.30,31 Transverse plication further assists in flap displacement, creating a natural pulling effect that simplifies flap repositioning while minimising dead space at the suture line, enhancing ease of closure, with minimal effort, placing the final incision in a concealable location, typically 6 cm above the genitalia. 32
Wide flap dissection is not required for effective flap mobilisation in abdominoplasty and is completely avoided using TULUA (Figure 5). 33
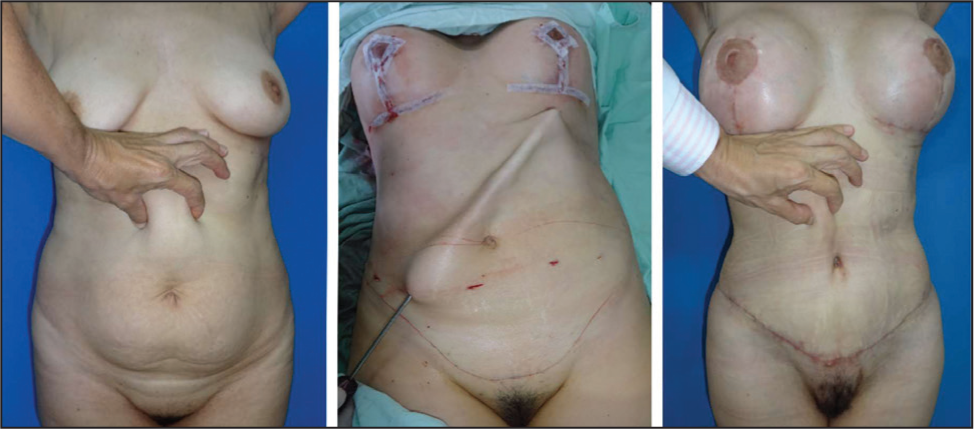
Can the abdominoplasty scar be placed in a very low position to make it more concealable?
Various techniques have been developed to avoid unexpected tension or the inability to close the abdominoplasty defect after resection. Planas (1978) 34 introduced the ‘vest over pants’ technique, which involved advancing the upper flap over the lower abdomen to determine the amount of resection. Later, Uebel (2009)35,36 described the ‘pull-down’ technique, relying on upper abdominal dissection up to the rib cage and simulating flap advancement to calculate the final resection and scar position. Similarly, Tiryaki (2017) devoted an entire book on ‘inverse abdominoplasty’, describing flap advancement to decide the amount of resection: While this approach provided tension-free closure with vascular and healing advantages, they often resulted in high scars that were difficult to conceal.
Traditional methods tailored resection in abdominoplasty to the last steps of surgery after estimating flap advancement, limiting the surgeon’s control over the final scar placement. These approaches often required additional resources, such as an inverted T closure 37 or a mid-abdominoplasty 38 with an intermediate vertical closure of the advanced umbilical hole. In contrast, TULUA offers en bloc wide resection and eliminates these limitations by facilitating flap sliding and allowing precise, tension-free scar positioning. 8 The final scar can typically be placed in a concealable location, such as 6 cm above the genitalia (Figure 6). 39
Is native umbilicus transposition necessary, or is neo-umbilicoplasty a better alternative?
Early abdominoplasty often involved amputation of the umbilicus without reconstruction. Torek later introduced the first umbilical graft, and transposition from its native stalk became the standard technique. While widely adopted, transposition requires significant flap elevation and limits modifications to the umbilicus’s position, leading to potential complications like necrosis, poor scarring and variable aesthetics. 40
Although neo-umbilicoplasty has traditionally been used in reconstructive cases, it allows greater freedom by amputation and reconstruction of the umbilicus, enabling better control over its position, shape and size.41–43 TULUA incorporates neo-umbilicoplasty as the standard, improving aesthetic outcomes without the risks associated with transposition.
Neo-umbilicoplasty, as demonstrated in TULUA, offers superior flexibility and more consistent results, making it a preferable alternative to transposition (Figure 7). 44

Conclusion
TULUA’s global acceptance highlights its alignment with sound medical principles, improved patient safety, and superior outcomes. The technique has broadened its applications to include secondary cases, 45 umbilical and infraumbilical hernias, 46 and post-bariatric reconstructions,47,48 often combined with belt lipectomy or oblique flank resections.49,50 Its adaptability to repeated resections provides a reliable solution for managing complications such as necrosis in the umbilical or subumbilical regions. Additionally, TULUA offers a safe alternative for patients with unilateral or bilateral subcostal scars, expanding its reach to more complex cases, 51 and has been implemented in ‘Mini and Mid’ abdominoplasty concepts.52,53
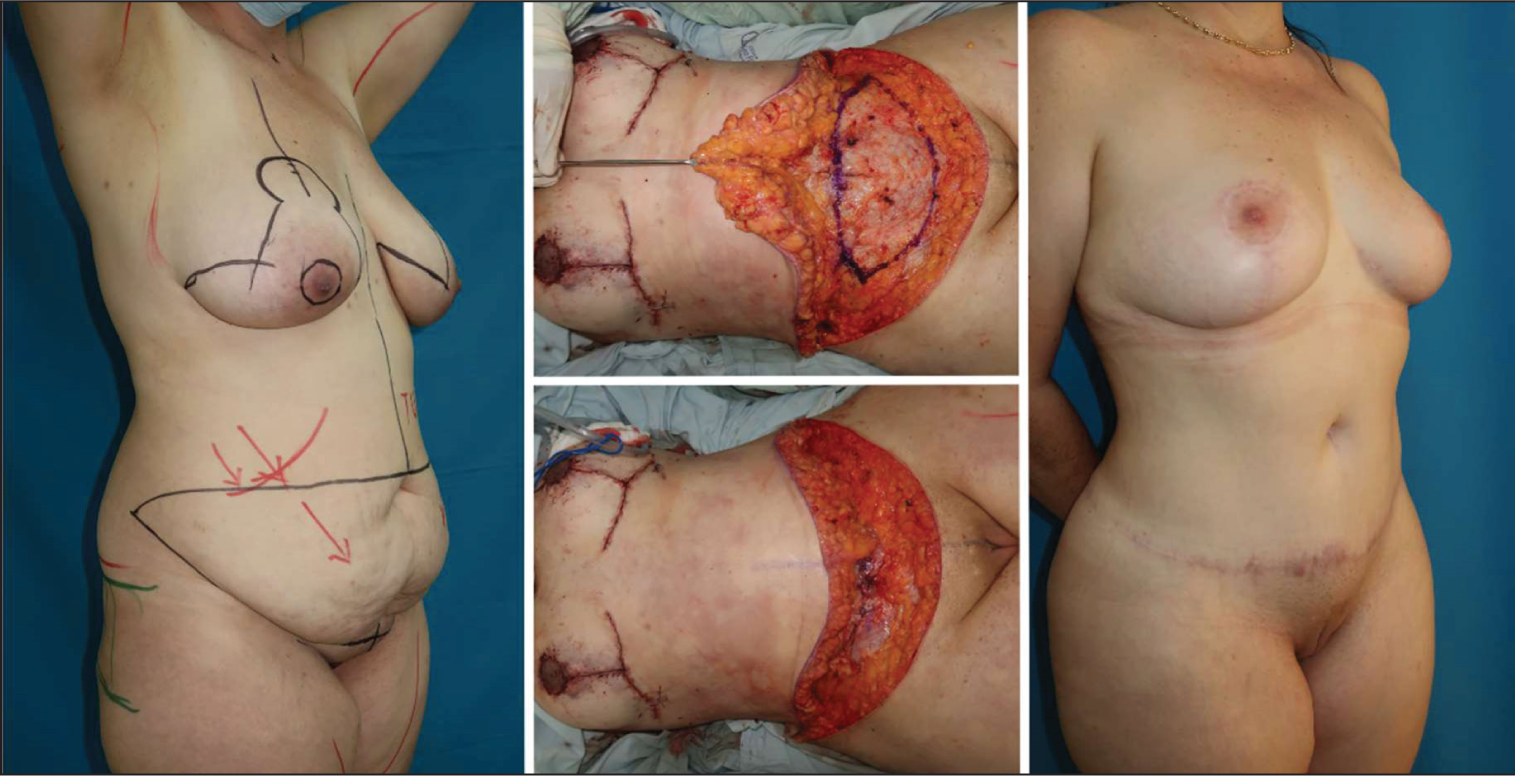
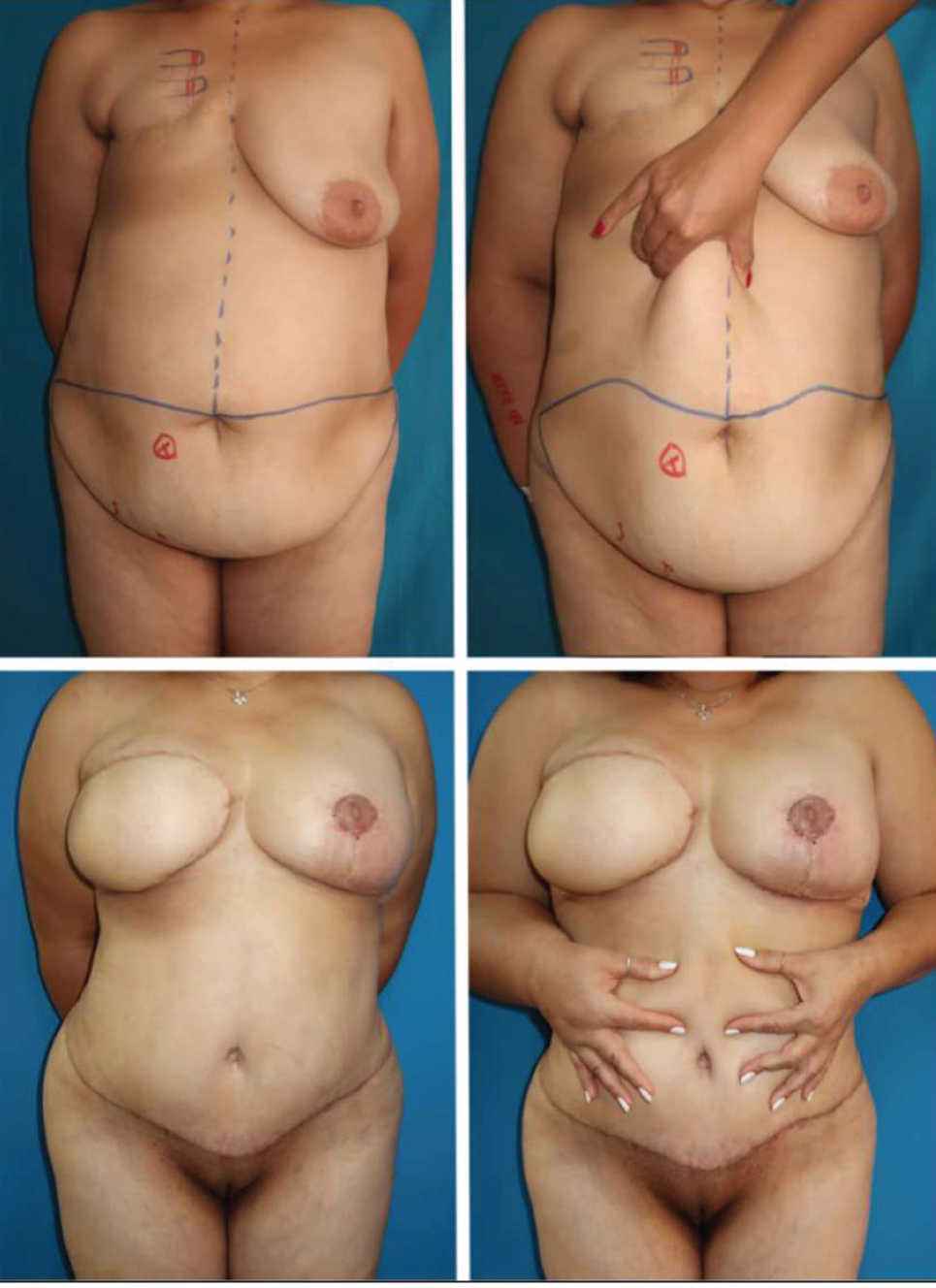
TULUA’s application has extended to high-definition abdominoplasty for both women and men, 54 seamlessly integrating fat grafting techniques to enhance abdominal musculature. 55 Its versatility is also evident in reconstructive procedures such as TULUA-DIEP and TULUA-HemiDIEP,56,57,58 demonstrating its ability to address both aesthetic and functional challenges. These innovations are well-documented in multiple publications and a comprehensive textbook, further cementing TULUA’s status as a groundbreaking surgical technique (Figures 8 and 9).2,59

Looking forward, the integration of TULUA with laparoscopic and robotic techniques presents new opportunities for treating epigastric laxity and hernias without flap undermining, broadening its utility even further. 60
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.