
Abstract
Background:
The combination of liposuction and avulsion is a novel technique that preserves the lymphatic and neurovascular structures of skin flaps enabling better wound healing. We have expanded its use to include abdominoplasty, legplasty, keloid scar excision, belt lipectomy, thighplasty and brachioplasty. The postoperative outcomes have been positive, with significant improvement in wound healing and a remarkably low complication rate.
Methods:
A retrospective analysis was conducted on 25 patients who underwent avulsionplasty between 2010 and 2023, covering 13 years. In total, 47 liposuction-avulsions were performed using a similar surgical technique of liposuction followed by avulsion. The patients were followed up to assess postoperative recovery and detect any complications.
Result:
We observed a very low postoperative complication rate. Only one patient of thighplasty had partial wound dehiscence which healed with conservative management and dressings. None of the other patients had any complications and had satisfactory wound healing. Out of a total of 47 avulsions performed, only one patient experienced wound dehiscence, resulting in a complication rate of 2.13%. However, when considering thighplasty alone, the complication rate was higher at 6.25%.
Conclusion:
Liposuction, followed by the avulsion technique of excision, is a novel combination that can be applied in a wide variety of plastic surgery procedures that involve the removal of tissues. The preserved lymphatics and neurovascular structures may be responsible for improved and predictable wound healing with a decreased incidence of complications in these cases. However, other biomechanical factors may also contribute, and further studies are required to identify them.
Introduction
The superiority of the avulsion technique of resection of tissues in thighplasty and brachioplasty over conventional dissection and resection was well illustrated by Hunstad et al. in their study. 1 He attributed this mainly to the well-preserved lymphatic network in the bed of resection when liposuction and avulsionplasty were used concomitantly. We extended the use of this novel technique to include abdominoplasty, legplasty and keloid scar excision as well along with thighplasty and brachioplasty and saw good postoperative outcomes in terms of improved wound healing and strikingly low complication rate.
Body contouring procedures are amongst the most commonly performed procedures in aesthetic surgery practice. Efforts are always underway to reduce the complications in these elective procedures. Inadvertent damage to the lymphatics and neurovascular structures while dissection is the main factor responsible for most postoperative complications such as neuromas in brachioplasty 2 and lymphoceles in thighplasty 1 and wound dehiscence in abdominoplasty amongst others.
An understanding of the anatomy of lymphatics of the body makes it evident how liposuction and avulsion cause minimum disruption. In the lower limbs, the lymphatics are grouped as a ventromedial and a dorsolateral bundle, both running superficial to the superficial fascia, hence the incisions beyond the superficial fascia are bound to disrupt them. Also, the ventromedial lymphatics are thick-walled and can withstand the traction caused by liposuction cannulas.
In the upper limbs, the lymphatics run superficial to the superficial fascia as well as drain in the axillary nodes. Even in the abdomen, most lymphatics draining the abdominal wall are located superficial to the Scarpa’s fascia. Hence in both these areas any deep incisions and dissection are bound to disrupt them.
The safety of liposuction in removing fat from the thigh without disrupting the lymphatics has been shown in studies by Hoffman. 3
Liposuction followed by avulsion also preserves the neurovascular structures apart from lymphatics. This also translates into improved wound healing. With the preservation of neurovascular structures, there is less chance of hematomas, neuromas and other traumatic disruptions that may prolong the inflammatory phase and delay wound healing. The preserved capillary network also increases local oxygen tension, washes away pro-inflammatory mediators and aids wound healing.
Materials and Methods
Between 2010 and 2023, 25 patients who underwent avulsionplasty were analysed retrospectively (Table 1). Among these eight patients had avulsion thighplasty (16 thighs) (Figure 1), eight patients underwent brachioplasties (16 arms) (Figure 2), two patients underwent avulsion legplasty (four legs) (Figure 3), two patients underwent avulsion abdominoplasties, one chest wall keloid scar excision with avulsion technique was done (Figure 4). Two patients had belt lipectomies by avulsion techniques (Figure 5) and four patients underwent avulsionplasty of trochanteric regions.
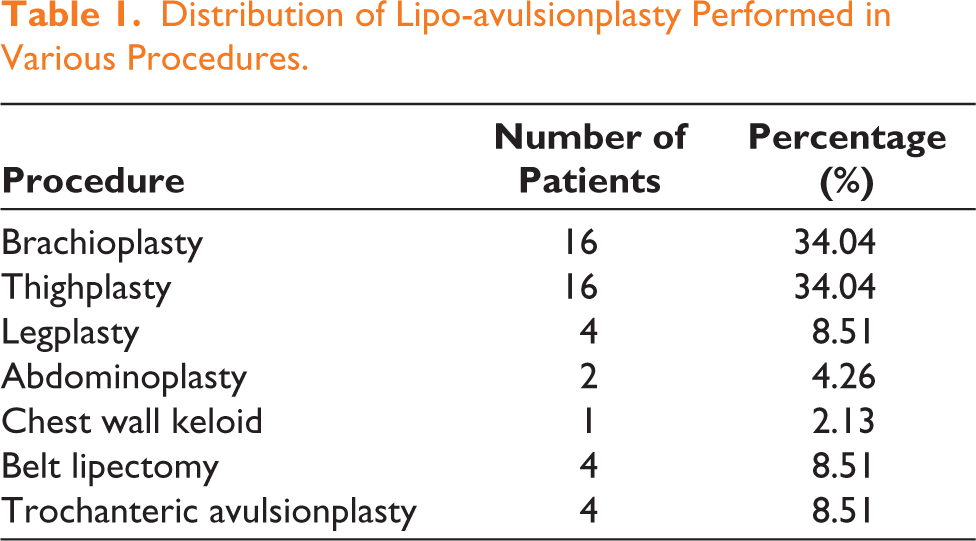
Distribution of Lipo-avulsionplasty Performed in Various Procedures.
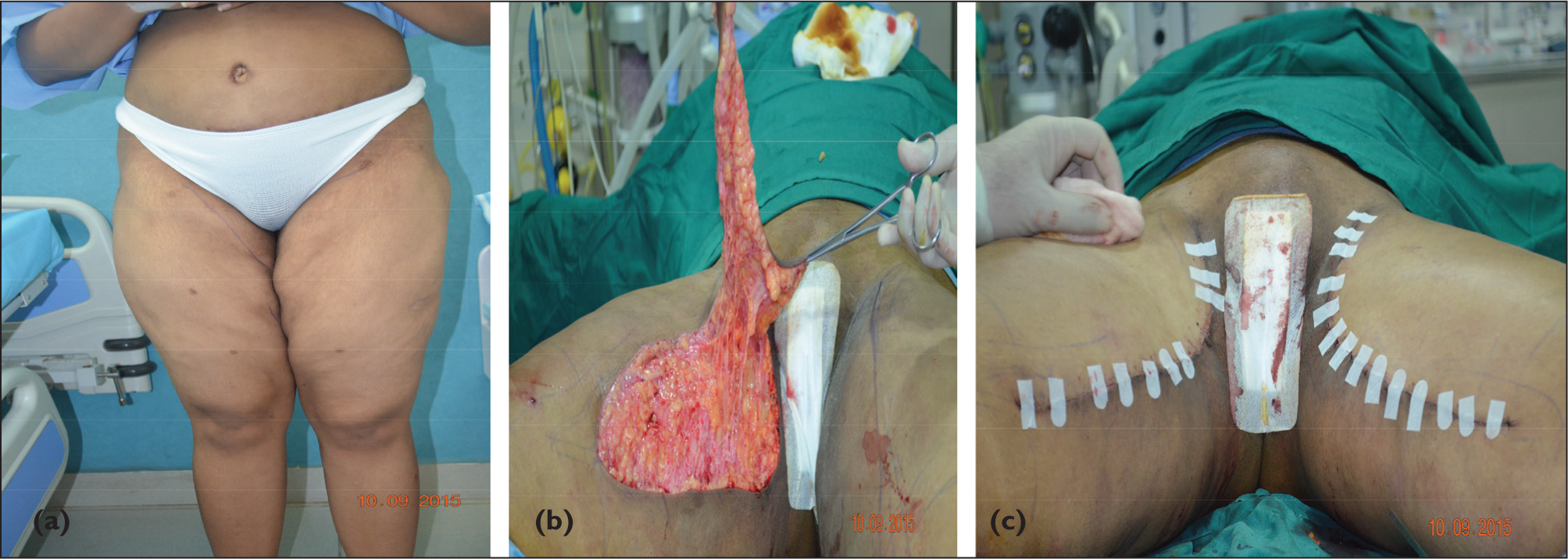
(a) Preoperative Picture of a 37-year-old Woman for Lipo-avulsion-thighplasty. (b) Intraoperative Picture of Avulsionplasty Being Performed. (c) Immediate Postoperative Picture, Post-lipo-avulsion-thighplasty.
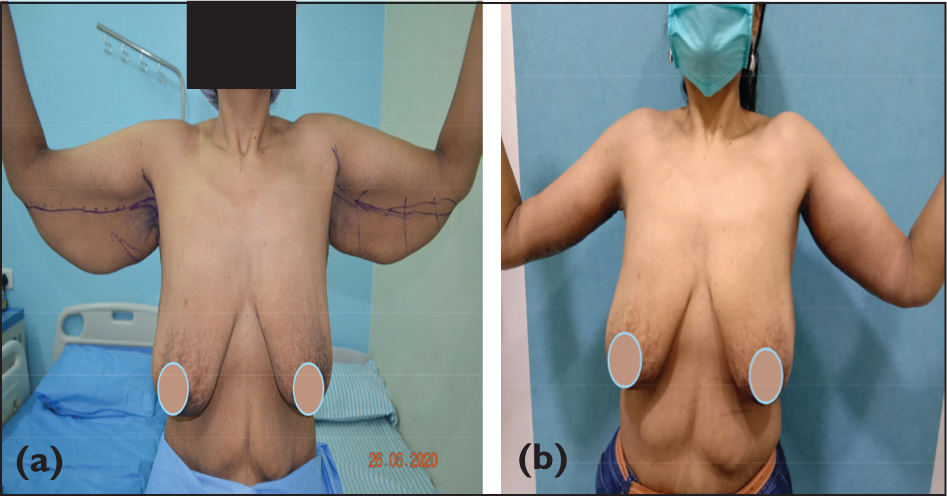
(a) Preoperative Picture of a 50-year-old Woman for Lipo-avulsion-brachioplasty. (b) Immediate Postoperative Picture, Post-lipo-avulsionbrachioplasty.
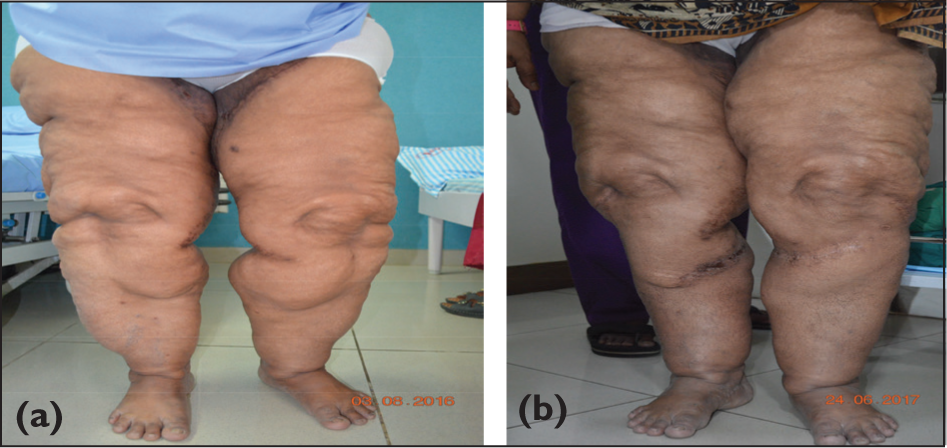
(a) Preoperative Picture of a 42-year-old Woman for Lipo-avulsion-legplasty. (b) One-month Follow-up of Lipo-avulsion-legplasty.
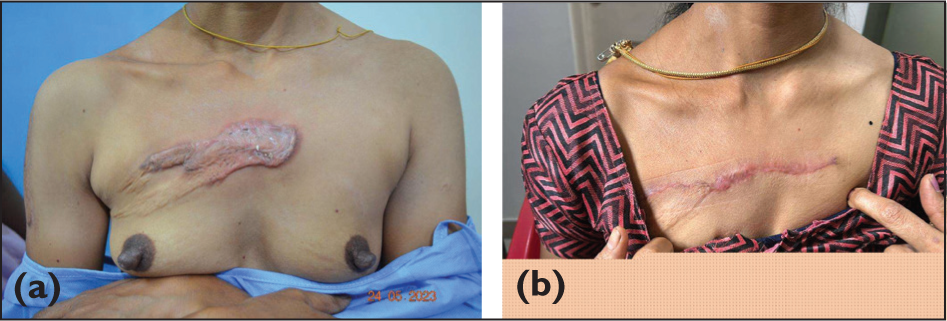
(a) Preoperative Picture of a 40-year-old Woman with a Keloid Scar on Her Chest. (b) Postoperative One Month After Lipo-avulsion Scar Excision Over the Chest for Keloid Scar.
(a) Preoperative Picture of a 37-year-old Woman for Lipo-avulsion-thighplasty. (b) Intraoperative Picture of Avulsionplasty Being Performed. (c) Immediate Postoperative Picture, Post-lipo-avulsion-thighplasty.

Patients were followed for up to one month postoperatively and were assessed for any surgical site complications in terms of wound dehiscence, delayed healing, seromas, neuromas, lymphomas, hematomas, etc.
Technique
The term excision site liposuction is self-explanatory and explains the procedure details. The original Hunstad technique cautions not to suction beyond the planned excision limits. In our technique, liposuction was done beyond the planned limit but no dissection was done beyond the excision. Dissection is the limiting factor for all wound-healing disasters.
The planning of the ellipse is crucial. After the tentative area is marked by pinching, another ellipse inside the double ellipse is marked to avoid any kind of wound tension at the time of closure.
The very important technical step is to free the dermis all around. The dermis is the strongest structure of the skin. If any bit of dermis is incompletely incised the avulsion process is halted at that point. Further incision is needed to avulse the skin paddle.
To start the avulsion from proximal to distal or the other way does not seem to influence the procedure. The avulsion process is started from the point of technical ease.
Avulsion in stages is critically important in extremities mainly arms and thighs. After avulsing through a marked length, the wound margins are temporarily stapled or sutured to prevent the flap oedema which may prevent approximation at the end of avulsion.
Wound closure without a drain completes the procedure.
Crucial factors are:
An ellipse of appropriate tension Complete incision of the dermis and release of the skin No dissection
Results
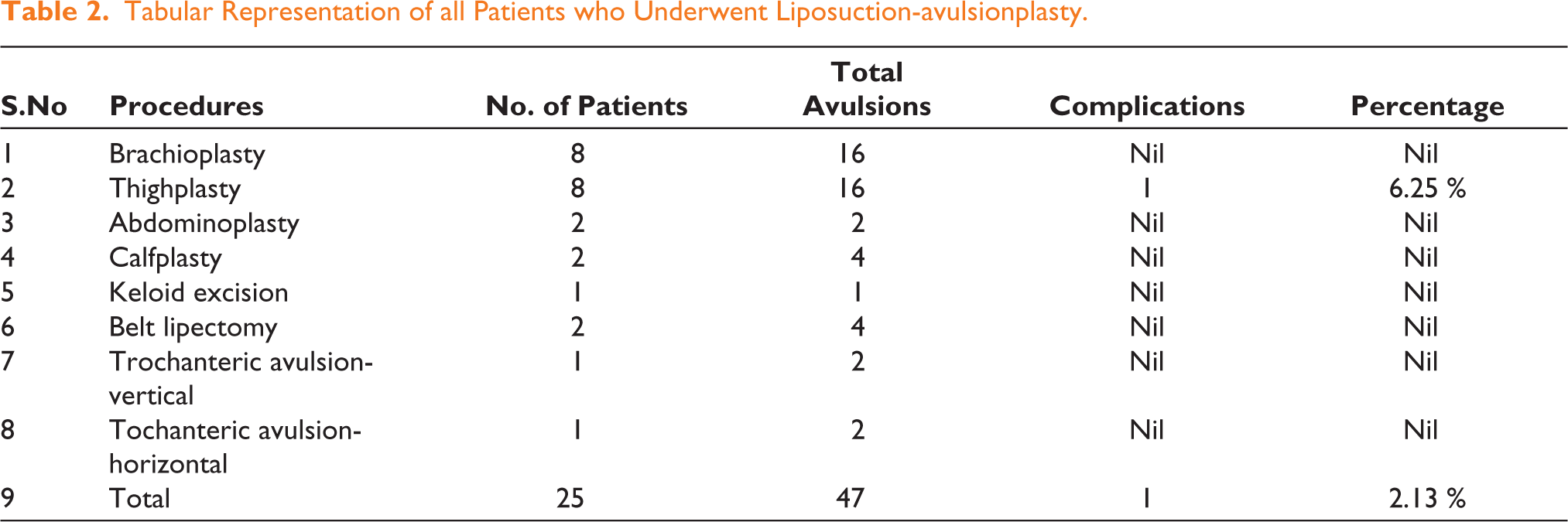
We observed a very low complication rate in the postoperative period (Table 2). Only one patient of thighplasty had partial wound dehiscence which healed with conservative management and dressings. None of the patients who underwent brachioplasty, abdominoplasty, legplasty, or thighplasty experienced any complications and all had a smooth recovery with satisfactory wound healing. Out of 47 avulsions, only one patient (2.13%) experienced wound dehiscence. When considering only thighplasty, the complication rate was 6.25%.
Tabular Representation of all Patients who Underwent Liposuction-avulsionplasty.
Discussion
Liposuction is considered to be one of the most beneficial developments of the 1990s. Properly done liposuction using a smaller diameter cannula results in fat depleted flap supported by loose neurovascular and lymphatic mesentery. This sliding flap can be advanced by stretching to close the post-excisional defects without tension. Suction followed by dissection is injurious to the flap’s survival.
The avulsionplasty was initially shown to be useful in excisional thighplasty by lowering the incidence of lymphatic complications like lymphatic cysts. Hunstad believed this technique of avulsion was more physiological by leaving lymphatics in the bed thereby reducing this complication.
Expanding indications for this technique in other sites like flank, lower abdomen, and scar sites lead us to postulate that this technique of avulsion excision though looks crude has more than the lymphatic preservation. The cobweb of loose tissues comprises neurovascular tissues. The much better healing observed in these areas vouches for definite supremacy over the dissection excision.
Complications relating to wound healing are fairly common in patients undergoing body contouring procedures. These patients are usually obese with pre-existing metabolic predicaments like diabetes, and thyroid issues, all of which contribute to hindering wound healing. Hence this subset of patients warrants increased focus on prevention of complications.
By replacing sharp dissection with liposuction, the lymphatics as well as neuro-vascular structures remain well preserved in the wound bed.
Dissection and undermining of the flaps lead to the destruction of neurovascular structures increasing the risk and chances of skin necrosis and sensory deficits. This was elucidated by Brauman in his study. 4
While the role of preserved lymphatics in improved wound outcome has been discussed in previous papers, we believe that the preserved neurovascular structures and other unknown factors also contribute to this effect. We observed a marked decrease in postoperative bruising at and around operative sites along with the absence of any hematoma which strongly suggests that capillary and vascular networks are better preserved.
Aggressive liposuction while reducing fat preserves the vascular network and hence improves the blood supply to the remaining flap.
The concept of sliding flaps has been described earlier.4-6 Brauman described how the liposuction technique creates sliding flaps by multiple factors. Thinning the flaps by fat removal and by transecting cutaneous ligaments and neurovascular mesenteries creates sliding flaps. These flaps retain their rich blood and nerve supply and can be mobilised for closure with decreased chances of necrosis.
It has been established in previous studies on wound healing that closure under tension directly can lead to necrosis and scar-related complications.7,8
Nguyen and Rohrich in their study suggested liposuction before avulsionplasty be confined to the area of skin excision, otherwise, it can lead to wound healing complications from trauma and oedema in surrounding areas, 9 but in our experience, liposuction in surrounding areas creates sliding flaps which help in tension free closure and decrease the complication rate.
Several improvisations have come to reduce the complications related to avulsionplasty. In thighplasty Webster suggested a helicoidal incision approach to avoid scar intersections and thus fewer cicatricial stress points and wound complications. 10
Thighplasty has been associated with high complication rates relating to wound healing in past studies. 11 Hunstad also noted an overall complication rate of 59% in his thighplasty study series. 1 Employing liposuction and avulsion resulted in low complication rates: 6.25% in thighplasty and 2.13% overall in lipo-avulsionplasties.
The role of lymphatics in wound healing has been well established. Lymphatics play an important role in wounds by draining the exudative extracellular fluid modulating the local immune response and maintaining the tissue pressures.12,13
Reduced lymphatics in the wound bed can thus lead to persistent oedema and delayed removal of debris and inflammatory cells thus impairing the wound healing process. 14
Liposuction and avulsion hence are a novel combination. While liposuction creates sliding flaps and enables closure without tension, preserves lymphatics and neurovascular structures by avoiding dissection. Avulsion also enables tissue excision along natural planes preserving the neurovascular and lymphatics and avoiding dissection. These two when performed together can be applied in a variety of surgical scenarios wherever excision of a skin segment is indicated.
Conclusion
Liposuction followed by the avulsion technique of excision is a novel combination, which can be used in a wide variety of plastic surgery procedures that involve the excision of tissues such as abdominoplasty, thighplasty, brachioplasty and large scar excision. Preserved lymphatics and neurovascular structures may be responsible for improved and predictable wound healing with decreased incidence of complications in these cases, but other biomechanical factors may also contribute, which requires further studies to explore this novel technique.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.