
Abstract
Background
SCJ asymmetry is poorly understood due to its rarity and limited imaging in asymptomatic populations, with few studies linking it to patient-reported symptoms, prompting our investigation of its clinical relevance in a healthy cohort. This study aims to identify the prevalence of subjective anatomical size and mobility differences in the sternoclavicular joint (SCJ) within a non-pathologic cohort, and the rate of functional interference and/or pain in this cohort.
Methods
Patients presenting to clinic with lower extremity orthopedic complaints were surveyed via a modified Nottingham Clavicle Score, tailored specifically to the SCJ. Patients included in the study additionally underwent retrospective chart review to identify demographics, comorbidities, and past medical history relevant to the SCJ.
Results
The final cohort consisted of 83 subjects and was majority female (n = 49; 59.04%), with a mean age of 55.3 years (range: 19–90) and BMI 30.69 kg/m2 (range: 17.58–57.54). Among the cohort surveyed, 27 patients reported an asymmetry of the sternoclavicular joint, majority of which indicated a larger right SCJ (n = 21; 77.8%) as compared to the left. SCJ asymmetry was associated with significantly increased differences in subjective mobility between sides (P = .020), and increased rates of perceived weakness on overhead activities (P = .005). However, perceived SCJ asymmetry was not statistically significantly associated with increased rates of pain (P = .225) or movement/clicking of the joint (P = .826).
Conclusion
Approximately 33% of patients in a non-pathologic cohort reported asymmetry across the sternoclavicular joints. Subjective asymmetry was significantly associated with significantly increased differences in mobility between sides as well as perceived weakness on overhead activities.
There are conflicting studies about the frequency of SCJ asymmetry in imaging studies, and none of these studies assess patient symptoms associated with any asymmetry. There is limited data that acromioclavicular joint asymmetry may affect shoulder kinematics. This study assesses patient’s subjective awareness of SCJ asymmetry and the association of asymmetry with perceived mobility and strength differences.What is Known About This Subject
What This Study Adds to Existing Knowledge
Introduction
The sternoclavicular joint (SCJ) is relatively infrequently associated with clinically significant pathological presentations due to the immense force required to injure this joint secondary to its ligamentous support. 1 As such, there is limited imaging of this joint, particularly in atraumatic and asymptomatic patients making it difficult to quantify normal variations in sternoclavicular joint size and the associated range of motion. Additionally, there are further limitations to the available data about subjective patient-reported outcomes pertaining to size, pain, function, and mobility of this joint.
Two studies have aimed to quantify SCJ asymmetry rates in healthy, non-traumatic populations.2,3 However, these studies did not utilize patient-reported outcomes and instead based there evaluation on computerized tomography (CT) imaging. In one study, less than 15% of patients had imaging evidence of asymmetry, while the other found no difference. These studies present opposing findings, both with limited sample size, offering much to be desired in the study of SCJ asymmetry. They also did not provide clinically useful information about the effect of SCJ asymmetry on patient’s subjective symptoms.
Similarly, there is a lack of literature regarding asymmetry rates in the acromioclavicular joint (ACJ) and their association with pain and dysfunction. However, one study found 60% of patients exhibited asymmetry in clavicular length, though SCJ-specific data were not examined. 4 The study emphasized the observable effects of activity and loading behavior on asymmetry patterns. A separate study found 35% of patients had more than 5 mm of clavicular asymmetry. 5 Both studies found left clavicular length to be greater. Similarly, Cunningham et al (2013) reported that 28% of clavicles exhibited asymmetry, with 7% of patients showing clinically significant asymmetry (>10 mm) that could impact treatment decisions. 6
Lastly, the glenohumeral joint has been studied for asymmetry in kinematics and strength, particularly in overhead athletes. Internal rotation deficits and small asymmetries in shoulder kinematics were noted.7,8
Despite the paucity of literature investigating asymmetry of the sternoclavicular joint, there remains evidence of asymmetry in various shoulder joints and clavicular dimensions, with implications for joint function and potential clinical significance. The present study aims to identify the prevalence of anatomical size and mobility differences in the sternoclavicular joint within a non-pathologic cohort, and the rate of functional interference and/or pain in this cohort. We hypothesize that there will be asymmetries present in size and mobility of the sternoclavicular joint within a non-pathologic cohort, and that these asymmetries will not commonly interfere with function or pain.
Methods
After obtaining Institutional Review Board (IRB) approval, patients undergoing orthopedic treatment for lower extremity complaints by a fellowship trained primary care sports medicine physician were prospectively recruited to the study from April 2025 to May 2025. Patients were excluded if they had a history of significant injury and treatment involving the sternoclavicular joint, acromioclavicular joint, or clavicle (defined as needing any treatment beyond physical therapy); a mental health disorder that, in the opinion of the principal investigator, could interfere with active study participation; or a history of pain syndromes such as fibromyalgia, systemic lupus erythematosus (SLE), complex regional pain syndrome (CRPS), or rheumatoid arthritis. Additional exclusions included a history of shoulder, cervical spine, or cardiothoracic surgery, as well as the presence of shoulder pain at the time of recruitment.
Patients presenting to clinic with lower extremity orthopedic complaints were surveyed via a modified version of the validated Nottingham Clavicle Score (NCS) (Appendix 1), tailored specifically to the sternoclavicular joint. 9 No Minimally Important Clinical Difference (MCID) has been established for the NCS, however, it has been found to have an effect size (ES) and standardized response mean (SRM) of 1.8 and 2.6, respectively. 10 Using background data from previous studies, we estimated that 20% of patients have a larger SCJ size in their dominant arm.2,3 We determined that our study would be powered at 80% and the standard error was set to 0.5. To ensure adequate precision, we computed the required number of patients such that the half width of a Wilson 95% CI is not more that .22 on the arcsin transformed scale. For example, if the true proportion equal were .75, we have a 95% chance of not getting an observed percentage of less than .65 or greater than .84. This led a study size of 80 and 3 additional patients were recruited to account for possible ambidextrous patients.
This study sought patients with lower extremity complaints to avoid selecting patients with a pathology that may impact their SCJ, or their perception of pain and mobility of the joint. Patients included in the study additionally underwent chart review to identify demographics, comorbidities, and past medical history. Demographic information collected included race, ethnicity, sex, age, and BMI. Comorbidity information collected included a past diagnosis of conditions that affect bone mineral density, joint mobility, and connective tissue. Past medical history included history of shoulder, neck, or rib/anterior chest wall pain from injury or trauma.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Equity, Diversity, and Inclusion
Participants were not excluded on the basis of race, ethnicity, nationality, socioeconomic status, or membership in marginalized groups. The author team consisted of 3 male junior researchers and 1 male senior researcher. Our study population included both male and female adults from different socioeconomic backgrounds from a single state in the United States; thus, findings may not be generalizable to all regions. Analysis included consideration for gender, race, and ethnicity.
Data Analysis
Statistical analysis was conducted using IBM SPSS Statistics software for Macintosh, version 29.0 [IBM, Armonk, NY]. Statistical tests for continuous variables included Pearson correlation, two-tailed Student t-test, and one-way ANOVA, and tests for categorical variables utilized Chi-square test. If more than 20% of cells had an expected count of less than 5, Fisher’s Exact test was used instead of Chi-square test. Alpha value of .05 defined significance for all tests.
Results
Demographics and Medical History of Patients Surveyed Stratified by Arm Dominance
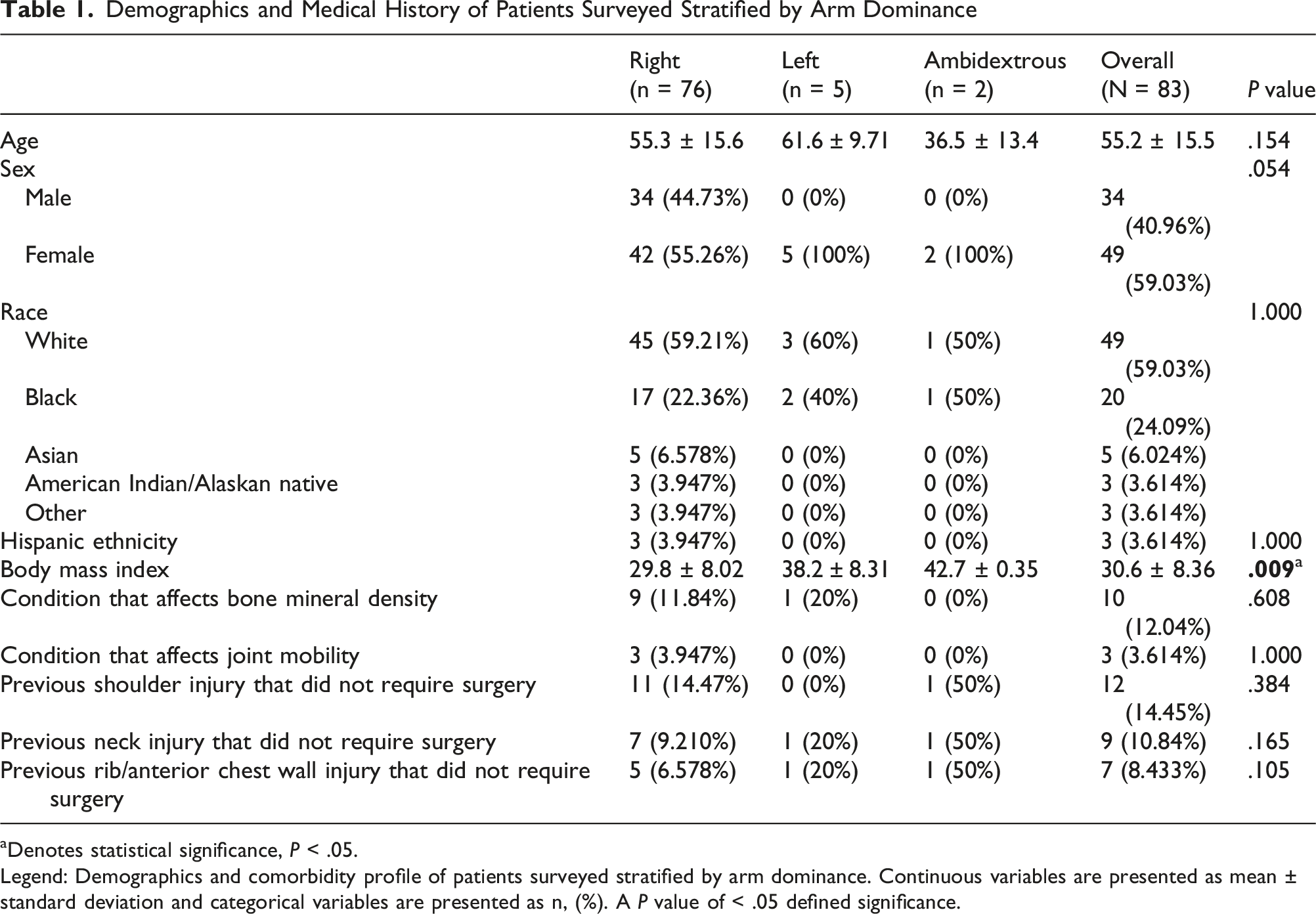
aDenotes statistical significance, P < .05.
Legend: Demographics and comorbidity profile of patients surveyed stratified by arm dominance. Continuous variables are presented as mean ± standard deviation and categorical variables are presented as n, (%). A P value of < .05 defined significance.
Demographics and Medical History of Patients Surveyed Stratified by SCJ Asymmetry
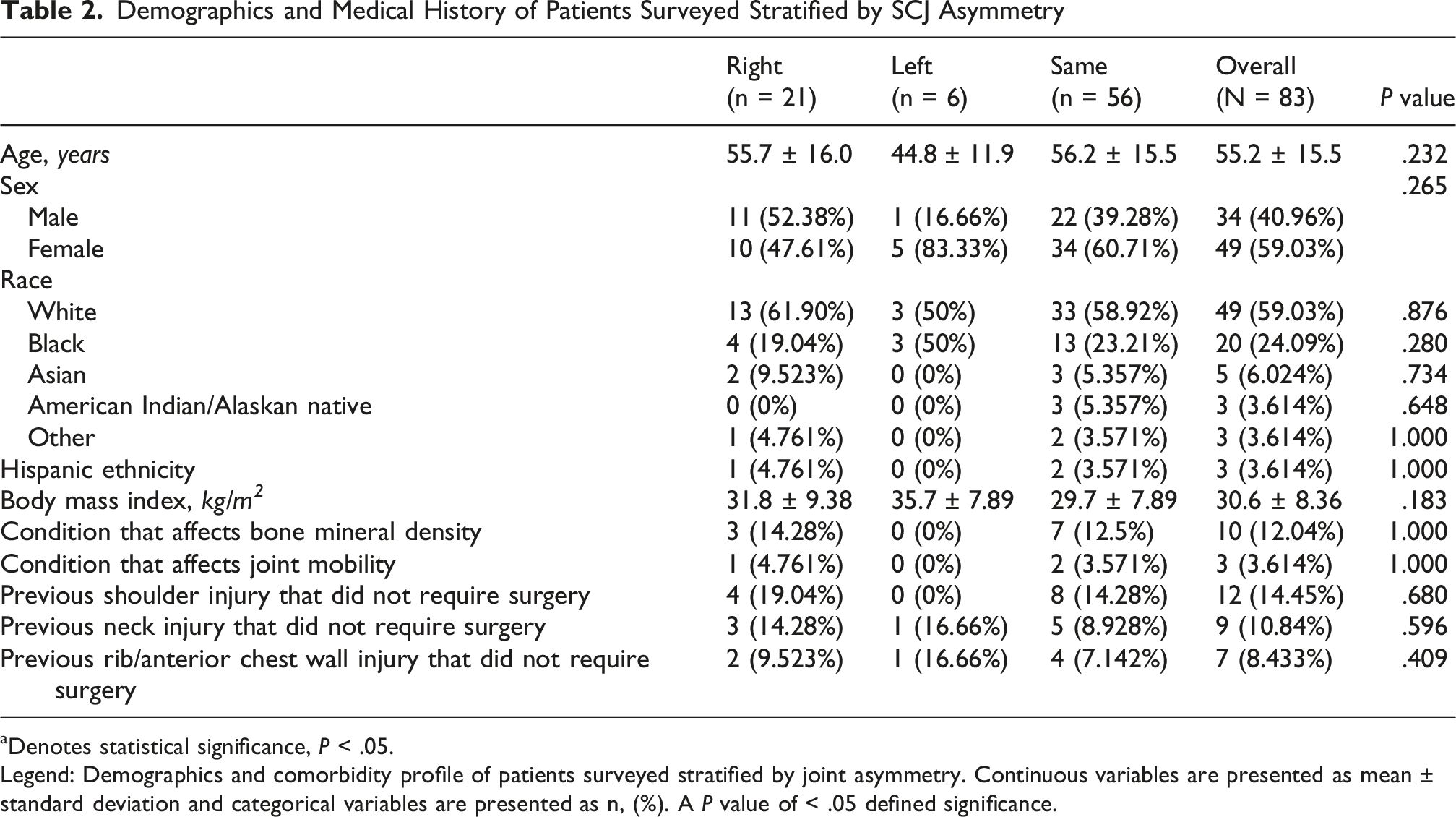
aDenotes statistical significance, P < .05.
Legend: Demographics and comorbidity profile of patients surveyed stratified by joint asymmetry. Continuous variables are presented as mean ± standard deviation and categorical variables are presented as n, (%). A P value of < .05 defined significance.
Pain, Mobility, and Function of the Sternoclavicular Joint Stratified by Any Joint Asymmetry
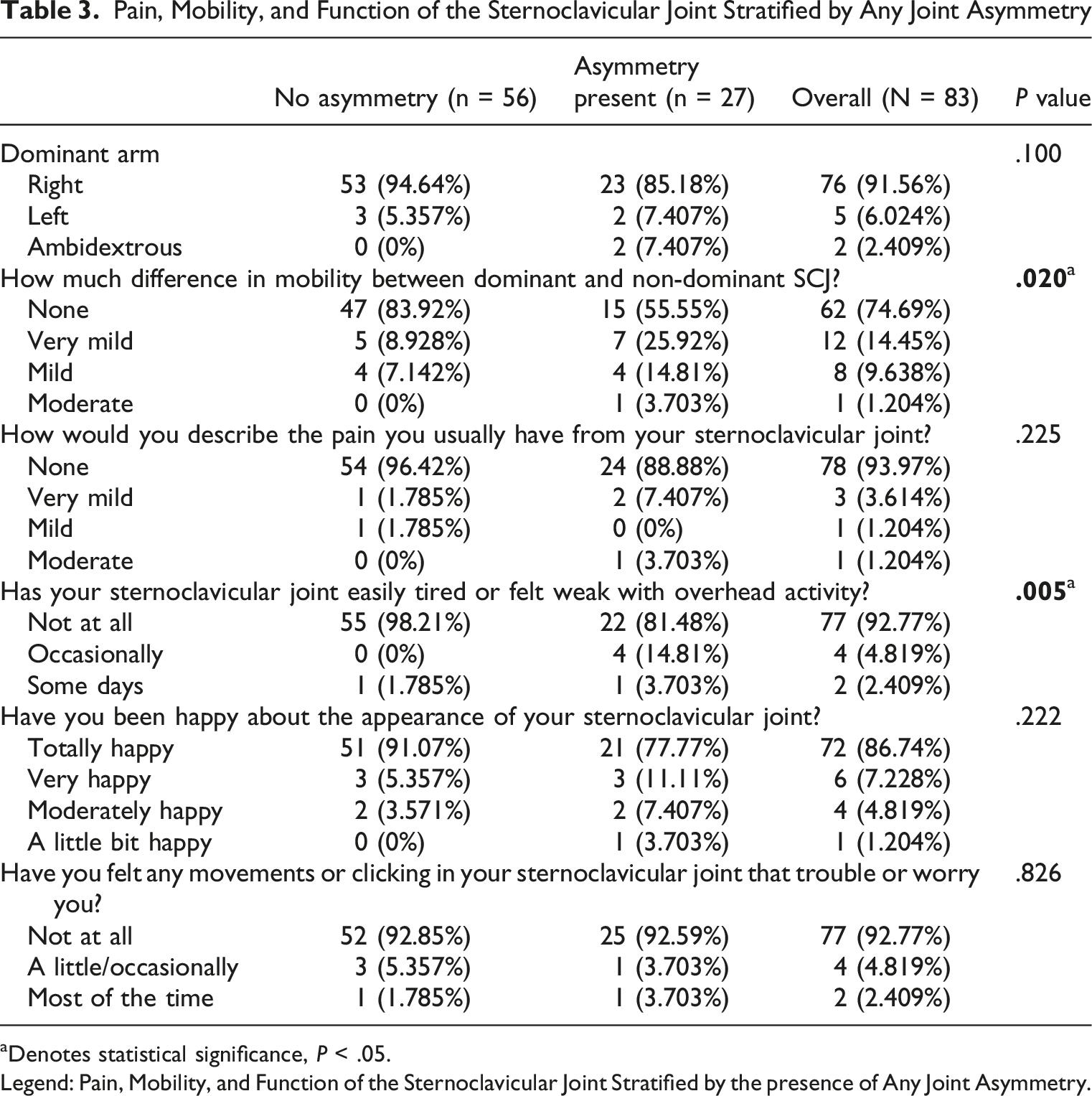
aDenotes statistical significance, P < .05.
Legend: Pain, Mobility, and Function of the Sternoclavicular Joint Stratified by the presence of Any Joint Asymmetry.
Pain, Mobility, and Function of the Sternoclavicular Joint Stratified by Larger Joint in Asymmetry
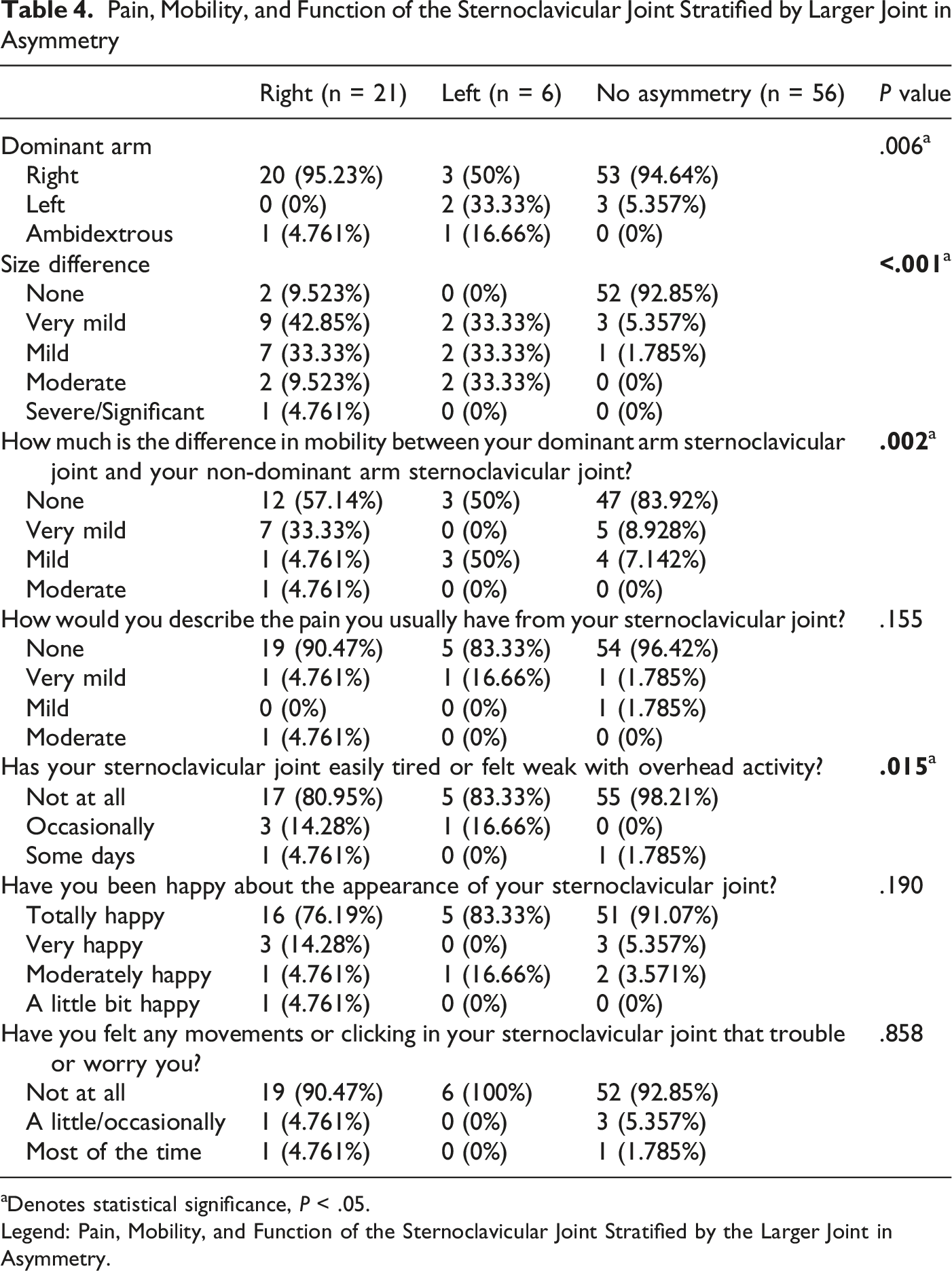
aDenotes statistical significance, P < .05.
Legend: Pain, Mobility, and Function of the Sternoclavicular Joint Stratified by the Larger Joint in Asymmetry.
Discussion
This study highlights the prevalence and perceived functional implications of SCJ asymmetry. Historically, the literature has focused on SCJ assessment through objective measures such as radiographic imaging, with a lack of consensus regarding the prevalence of SCJ asymmetry.4,11 Our findings expand on these studies through patient reported outcomes. Patients who reported SCJ asymmetry most frequently perceived the right side as more prominent. Further, professed overhead weakness and asymmetric mobility showed correlation with perceived SCJ asymmetry.
Tuscano, Banerjee, and Terk (2009) examined 104 chest CT scans in the transverse plane, finding that 11% of patients had asymmetrical clavicular head diameters, and 14% showed asymmetry in the measurement from the anterior border of the manubrium to the anterior-most margin of the clavicle (MCA). 3 The differences in clavicular head diameters ranged from 0 to 1 cm, SCJ space from 0 to 0.57 cm, and MCA from 0-0.8 cm. De Maeseneer et al (2016) followed up on this study, addressing limitations such as scan region (neck vs chest) and examined planes (transverse only vs coronal and transverse). 2 Their study of 66 CT scans in both coronal and transverse planes reported no significant differences in right and left joint space widths. These studies present opposing findings, and both had limited sample sizes. They also were limited as there was no investigation about the effect of SCJ asymmetry on patient’s subjective symptoms.
In the acromioclavicular joint (ACJ), there is literature regarding asymmetry rates in and their association with pain and dysfunction. However, studies have been conducted on clavicular bone asymmetry and its functional consequences. Auerbach and Raxter (2008) analyzed clavicular length and found that more than 60% of patients exhibited asymmetry, though SCJ-specific data were not examined. 4 Ergisi et al (2023) evaluated 100 patients with non-traumatic CT scans, finding 29% of patients had more than 5 mm of clavicular asymmetry, and 6% had more than 10 mm of difference. 5 As previously stated, both studies found left clavicular length to be greater. Similarly, Cunningham et al (2013) reported that 28% of clavicles exhibited asymmetry, with 7% of patients showing clinically significant asymmetry (>10 mm). 6
Lastly, in the glenohumeral joint, Srivastav et al (2018) found that 29.1% of collegiate athletes exhibited internal rotation deficits, though these deficits were not associated with scapular dyskinesia or external/internal rotation strength ratios. 7 Additionally, Schwartz et al (2013) studied 22 subjects and found small asymmetries in shoulder kinematics, particularly for abduction in the frontal plane and flexion in the sagittal plane. 8
Our findings provide further subjective information about patient perceptions about their shoulder joint, specifically focused on the SCJ. It shows that not only are patients aware of their SCJ asymmetry, but they also perceive it as functionally meaningful. Reports of overhead weakness and asymmetric mobility may reflect subtle biomechanical changes seen with differing SCJ sizes. However, the lack of pain associated with SCJ asymmetry leads us to believe that these patients are able to functionally compensate well and this compensation allows SCJ asymmetry to remain clinically insignificant for many. Finally, the predominance of a larger right-sided SCJ might reflect arm dominance. This finding agrees with that of previous studies of general populations as well as athletes which indicate an association between limb dominance and increased size and asymmetry.11-13
The studied cohort has a mean age of 55.3 years, making it most applicable to middle-aged adults. Even in the absence of pain, decreased mobility and strength are important physical performance factors that may affect a patient’s ability to work and complete activities of daily living. This study demonstrates the relative frequency of perceived SCJ differences in this working age population. It thus provides important background information for the clinician seeing a patient of this age who is presenting with concerns regarding asymmetry in the SCJ. While SCJ asymmetry can be a marker of certain disease states, the individual patient sitting in front of the physician may in fact be part of the roughly one-third of the general population who has an asymptomatic SCJ size and mobility difference. In context of other history, exam, lab, and imaging data, it may be appropriate to reassure patients about the commonality of SCJ asymmetry.
Limitations
We must acknowledge several limitations of this study. First, patient reported outcomes are subjective and can be prone to bias. Although difficult to circumvent given the nature of survey administration, prompt bias could have reasonably impacted the answers provided by patients who participated in the study. We also did not confirm reported asymmetry of patient SCJs through imaging. We did not collective objective data such range of motion on physical exam, motion capture, or goniometry. Future studies could incorporate patient subjective measures with imaging and range of motion analysis to confirm SCJ asymmetry. In a similar sense, biomechanical studies to assess overhead weakness and asymmetric mobility should also be considered.
Clinical Implications
This study is the first to assess sternoclavicular joint (SCJ) asymmetry in a healthy population using patient-reported outcomes. It identifies a significant association between SCJ asymmetry and upper extremity functional differences, such as mobility limitation and overhead weakness, despite the absence of increased pain or cosmetic dissatisfaction. These findings suggest that SCJ asymmetry, while often clinically silent, may have functional implications not previously captured in radiographic studies alone.
Conclusion
Approximately 33% of patients in a non-pathologic cohort reported asymmetry of their sternoclavicular joints. Subjective asymmetry was significantly associated with subjective increased differences in mobility between sides as well as perceived weakness on overhead activities. However, there was no significant association with pain of the joint. Future longitudinal studies should investigate the relationship between SCJ asymmetry and objective physical limitations. As mentioned, a combination of imaging modalities, range of motion analysis, and strength testing could be used to quantify the existence and impact of SCJ asymmetry on a patient. The current study has revealed the prevalence of perceived variations in size, pain, function, and mobility, in the general population.
Supplemental Material
Supplemental Material—Prevalence, Function, and Pain of Asymmetry in Size and Mobility of the Sternoclavicular Joint
Supplemental Material for Prevalence, Function, and Pain of Asymmetry in Size and Mobility of the Sternoclavicular Joint by Joshua L. Morningstar, BS, Daniel Faraj, BS, Tyler Hutchens, BS, Michael Seifert, MD in Montefiore Einstein Journal of Musculoskeletal Medicine and Surgery
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from UNC Hospitals Institutional Review Board 25-0077.
Consent to Participate
Written informed consents were obtained and stored for each patient who participated.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Data Availability Statement
All data from this study is stored and available for review upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.