
Abstract
Background
Despite advances in surgical techniques, complication rates for patients undergoing total wrist arthrodesis (TWA) remain high. In this study we retrospectively review a case series of 24 consecutive patients who underwent TWA with 100% union rate and minimal postoperative complications.
Methods
A retrospective chart review was conducted between 2019-2023 of patients who underwent TWAs by a single hand surgeon. Demographic data, outcome measurements, radiographic images, and operative reports were extracted from the patients’ medical records at the time of data collection. Radiographs were reviewed for bony union.
Results
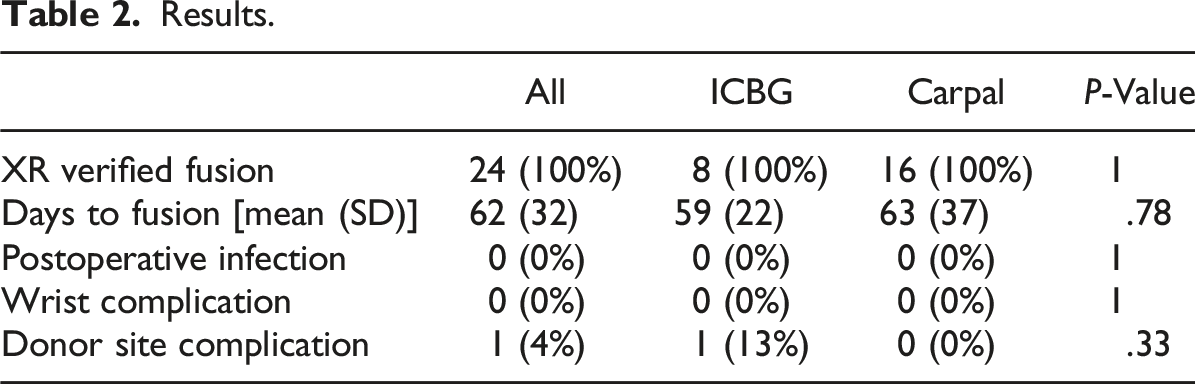
24 total patients were identified for analysis, 16 male and 8 female with an overall mean age of 46 years at the time of TWA. Overall postoperative follow-up time had a mean of 179 days. All patients had radiographically confirmed fusion by X-ray. Mean time to fusion was 62 days (SD 32). No patients developed surgical site infections, malunion, or failure of fusion, and no patients required return to the operating room for revision.
Conclusion
By following meticulous techniques, we have successfully performed wrist arthrodesis with favorable outcomes and with minimal complications in a large consecutive series.
Keywords
Introduction
While firmly cemented as the “gold standard” for correcting end-stage wrist arthritis refractory to conservative treatment, total wrist arthrodesis (TWA) is also recognized as the definitive salvage operation for failed wrist reconstructive procedures. Initially indicated to alleviate pain in patients with end-stage degenerative osteoarthritis, inflammatory (rheumatoid) arthritis, and posttraumatic osteoarthritis, the scope of this procedure has broadened to encompass a wide array of conditions over the years to include cerebral palsy, brachial plexus injuries, and other spastic and contracture-based illnesses. 1 TWA in its simplest form is the fusion of the carpus to the radius, allowing for forearm rotation while restricting wrist flexion–extension and radial–ulnar deviation.
Literature reports TWA having a high degree of patient satisfaction with mean Disabilities of the Arm, Shoulder and Hand (DASH) scores ranging from 25 to 38 (scores range from 0 for no disability to 100 for most severe disability).2,3 For reference, DASH scores after carpal tunnel release and internal fixation of distal radius fracture average around 15 with ranges from 0 to 67.4-6 Although TWA has been shown to provide pain relief and improve function and grip strength,7,8 there have been reported high re-operation and complication rates. 9 Reported complications following TWA include non-union, tendon ruptures, plate breakage, deep wound infection, fracture of healed fusion, neuroma, hematoma, carpal tunnel syndrome, and refractory pain at the third carpometacarpal joint (often due to nonunion).10,11 The rate of adverse events for TWA ranges widely, with some authors publishing that it can be as high as 61%.1,9 Of all of the complications, nonunion remains a common problem with studies demonstrating rates ranging from 2.8 to 8.3%.8,9,12-14 The reoperation rate following TWA is also high with reported rates up to 19%, 28%, and even 63%.1,12,14
Despite the many varying techniques and implants at the surgeon’s disposal, complications and reoperation rates are astonishingly high. 7 In this study we retrospectively review a case series of 24 consecutive patients who underwent total wrist arthrodesis without any significant complications or need for reoperation. We present a collection of technical insights that contribute to our high success rate to assist the surgeon in reproducing our outcomes and changing the perception of this powerful surgical procedure.
Methods
The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2000 and 2008, and the protocol was approved by the hospital institutional review board.
A retrospective review was performed on patients undergoing total wrist arthrodesis by the senior surgeon between 2019 and 2023. Patients were identified using current procedural terminology (CPT) codes including “arthrodesis, wrist joint (including radiocarpal and/or ulnocarpal fusion); without bone graft,” “arthrodesis, wrist joint (including radiocarpal and/or ulnocarpal fusion); with sliding graft,” “arthrodesis, wrist joint (including radiocarpal and/or ulnocarpal fusion); with iliac or other autograph (includes obtaining graft).” All patients, both pediatric and adult, who underwent TWA with complete electronic medical records were included in the study.
Demographic characteristics, outcome measurements, radiographic images, and operative reports were extracted from the patients’ medical records at the time of data collection. Radiographs were reviewed at each follow-up for bony union, and chart review was conducted to assess for any known reported complications. Patients were split into 2 groups for a more detailed sub-analysis based on whether iliac crest bone graft (ICBG) or bone graft from excised carpal bones was used for arthrodesis.
SPSS 29.0 (IBM Corp., Armonk, NY) was used for statistical analysis. For comparative analysis of the study groups (ICBG vs carpal bone grafts), Fisher’s exact test was performed for categorical variables, and student’s t-test for continuous variables. The level of significance was set at P < .05 for all analyses.
To achieve the high rate of fusion without the need for revision and low rate of complications seen in our patient cohort, the senior author employs a surgical technique that includes many refinements that we believe are critical to this success. 1. Proximal row carpectomy (PRC) serves to minimize the number of fusion surfaces while supplying bone autograft. This is particularly helpful in younger patients with good quality carpal bones for use as autograft, as they are spared an additional surgical site to obtain ICBG (Figure 1C and D). 2. Fusion surfaces are carefully prepared with manual sharp debridement of all articular cartilage using a variety of rongeurs, curettes, and occasionally osteotomes to create the optimal fusion surface while eschewing burrs and power devices that could cause heat necrosis. The carpal bones are very small and exquisitely sensitive to thermal necrosis. 3. Bone graft is used in every case to assist in bony fusion. Only bone autograft is used, never allograft or synthetic bone graft materials. Carpal bone graft from the PRC is ideal (Figure 1D and E); however, ICBG serves as an excellent alternative if carpal bone quality is suboptimal, as can be seen with older, osteoporotic patients. 4. An Eaton-style dorsal capsular flap
15
is elevated and subsequently carefully repaired to ensure secure containment of bone graft during healing (Figure 1A, B and F). 5. Rigid fixation is achieved using a dorsal wrist spanning plate, and a specialized compression-distraction tool is employed to apply significant compression across the fusion sites to promote bone fusion (Figure 1G and H). In the senior author’s practice, the TriMed Compression-Distraction Tool is used with their Total Wrist Fusion Plate (TriMed Inc, USA) to generate this compression, although several alternatives exist on the market. The compression-distraction tool is a specialized device that can be used in conjunction with an oblong sliding hole in the fixation plate to move the plate either proximally or distally to generate compression or distraction, respectively. The use of the device is described in detail in this technique paper,
16
and in TWA, the plate is only moved proximally to increase compression across the wrist fusion site. 6. Insertion of a surgical drain in the dorsal wrist to prevent hematoma and facilitate optimal wound healing is crucial in minimizing complications. The senior surgeon uses a 10-French Blake channel drain which is removed at the 2-week postoperative visit. 7. Rigorous cast immobilization for a minimum of 8 weeks. If fusion is not seen on X-ray at 8 weeks, then cast immobilization is continued. If at 12 weeks there is still no clear evidence of successful arthrodesis on X-ray, then a computed tomography scan of the wrist is obtained to evaluate for fusion. 8. A short course of corticosteroids in the form of a Medrol dose pack is prescribed at discharge to mitigate postoperative inflammation and edema.
17
Surgical technique: (A) design of the Eaton-style dorsal capsular flap which is used to access the wrist joint; (B) elevated dorsal capsular flap; (C) PRC; (D) status post PRC and removal of joint cartilage with excised carpal bones processed into bone autograft; (E) bone autograft packed into wrist fusion site; (F) dorsal capsular flap repaired; (G) fixation with dorsal total wrist fusion plate; (H) use of the compression-distraction tool to move the plate proximally on the radial shaft and generate compression across the wrist fusion site.

Results
Patient Demographics.

Bold indicates significant p-value < 0.05
Results.
Discussion
Historically, TWA was performed with cortical bone graft alone which required prolonged immobilization and was associated with graft displacement and donor site complications. 18 The evolution of subsequent techniques included intramedullary pins to achieve wrist fusion and enhanced stability by Clayton, 19 Rush pin and staples to prevent rotation by Mannerfelt and Malsten, 20 and eventually the use of a compression plate across the wrist. 21 Initial techniques introduced by the AO (Arbeitsgemeinschaft für Osteosynthesefragen) group used a conventional dynamic compression plate, but now there are many options for dedicated wrist fusion plates.13,14 The TWA technique utilized by the senior author includes the use of a dorsal total wrist fusion plate to apply compression across the wrist fusion surfaces as well as other technical refinements as described above which has helped produce reliable wrist fusion with minimal complications. Our patient cohort represents 24 patients spanning a broad age range across 4 years of surgical practice. All patients achieved bony fusion with none requiring any revisions. This technique is reliable across all age ranges as our youngest patient was 15 and oldest 88 and for all wrist pathologies indicated for arthrodesis.
Reported complication and revision rates in TWA have historically been high in the literature with nonunion remaining a significant problem despite the advancement of dedicated wrist fusion plates. Although some have speculated that this is due to the use of corticosteroids and other anti-inflammatory agents in patients with rheumatoid arthritis of the wrist, studies have shown that in non-inflammatory cases of end-stage arthritis, the complication and reoperation rates are just as high. In our case, all of our patients received postoperative corticosteroids with no adverse effects. Recently, Wei and Feldon reported an overall complication rate of 29% among 1782 wrist arthrodeses and a reoperation rate of 19%. 8 A more recent retrospective review of patients undergoing TWA similarly found that roughly one-third of its cohort experienced a postoperative complication with a reoperation rate of 19%. 12 Reigstad et al examined 76 patients who underwent TWA for noninflammatory arthritis and reported that 46 (61%) patients developed complications, resulting in 65 reoperations. 9 In these 3 studies, the reported nonunion rates were 4.4%, 2.8%, and 4%, respectively.8,9,12 Sauerbier et al and Houshian et al reported nonunion rates of 8.3% and 7% in their cohort studies following TWA using wrist fusion plates.13,14 Although the union and satisfaction rates are higher in patients with cerebral palsy who had TWA, the complication and hardware removal rate is just as high as in other wrist pathologies. 22 In our cohort, all patients achieved full wrist fusion. No patient developed a postoperative infection and no patients needed operative revision. We believe the surgical techniques outlined above are critical to the excellent outcomes we have seen in our patient cohort.
Nonunion continues to be a significant problem after TWA often requiring reoperation as it is essentially failure of the intended treatment. We believe performing PRC with every TWA is crucial to the 100% union rate we saw in our patient cohort. There are multiple advantages provided by PRC with minimal downside. The only disadvantage might be increased operative time to perform the PRC. However, this time might already be offset by making it far easier to prepare the carpal joint surfaces for fusion after the proximal row is excised. PRC decreases the number of joint surfaces requiring arthrodesis, which would expectedly also increase the rate of successful union. In addition, with the proximal row removed, there is less motion and therefore increased stability across the wrist during postoperative healing which would again be expected to lead to improved union. Lastly, PRC also has the advantage of providing an immediate source for autologous bone graft without the morbidity of a second surgical. One concern that could arise from the routine incorporation of PRC in TWA is decreased tendon excursion with shortening of the carpus leading to problems in hand function. However, our experience has not found this to be an issue amongst our patients. Since both extensors and flexors are shortened equally, muscle accommodation across the wrist remains balanced. A recent meta-analysis showed that shortening the carpus does not affect grip strength as there was no difference in post-operative grip strength when comparing four-corner arthrodesis vs PRC. 23
There are many options for bone graft material in TWA with no clear consensus on which one is the best. Although allografts can be used, bone autograft harvested from the iliac crest, ulna, radius, or olecranon are the most common. 7 In our patient cohort, only autograft was used. Patients who were operated on earlier in the study period were more likely to have had ICBG, particularly the older patients. However, over time carpal bones became the predominant source for bone autograft. Our data shows that the use of carpal bone autograft is very effective in achieving fusion and spares the patient from having a separate donor site. The senior author does evaluate the carpal bone quality in each patient and will use ICBG in patients with osteoporotic bone or with significant degenerative disease. Our results show that there is no difference in outcome between the 2 autograft types, and complications are minimal in both groups. One patient did experience persistent pain at the iliac crest donor site, so preferential use of carpal bones would decrease that occurrence.
We recognize our study has several limitations. The most significant is our small sample size which precludes any major statistical analyses. However, this is not a commonly performed procedure, and we feel our results still contribute valuable new information. The retrospective nature of the study also only permits pattern identification in the data rather than any direct causal relationships. Even though some patients had follow-up periods of greater than 1 year, overall, the follow-up period in our patient cohort is quite short. Although the length of follow-up was enough to demonstrate the primary goal of wrist fusion in all of our patients, it is not long enough to capture all of the potential complications that could arise from TWA. Hardware failure or tenderness leading to hardware removal; tendon adhesion, irritation, or rupture; and nerve irritation are all complications associated with TWA that could manifest in the long term. Future studies with a prospective design, larger patient cohort, and long-term outcomes would be beneficial.
Although revision and complication rates in TWA have historically been reported in literature to be quite high, we present a patient cohort with 100% fusion rate, no revisions or reoperations, and minimal complications. A refined surgical technique that ensures strong compression across fusion sites, good quality bone autograft, and careful closure and protection of the surgical site has been critical to achieving this success.
Footnotes
Ethical Consideration
This study was approved by the Montefiore Einstein Institution Review Board with IRB #2022-14122 initially approved on June 8th, 2022.
Informed Consent
There is no information in the submitted manuscript that can be used to identify patients. Informed consent was waived per the institutional review board.
Author Contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study is available to be shared upon request to the corresponding author.