
Abstract
Background
Trauma to anterior teeth is a common occurrence in dental practice, often resulting in crown fractures that require prompt esthetic and functional rehabilitation. Reattachment of the fractured tooth fragment is considered a conservative and effective treatment option as it preserves natural tooth structure and restores original morphology.
Aim
To present the clinical management of complicated crown fractures of maxillary anterior teeth using the tooth fragment reattachment technique following endodontic treatment.
Case Description
This manuscript describes two cases of complicated crown fractures involving maxillary anterior teeth. In both cases, endodontic therapy was performed, followed by reattachment of the fractured tooth fragment using adhesive restorative techniques. Proper case selection and patient cooperation were essential for successful treatment outcomes.
Results
Both cases demonstrated satisfactory esthetic and functional outcomes. The reattached fragments restored the natural contour, color, and function of the teeth, with good clinical stability.
Conclusion
Tooth fragment reattachment is a predictable, conservative, and cost-effective treatment option for the management of fractured anterior teeth. When performed with proper case selection and technique, it can provide excellent esthetic and functional rehabilitation.
Introduction
Crown fractures are the most common anterior tooth injuries, occurring mainly in the maxillary incisors due to their prominent position.1, 2 Mandibular central incisors are less often affected. These fractures make up 18%–22% of dental injuries, with about 96% involving the maxillary central incisors. 3
Around 25% of individuals sustain at least one anterior tooth fracture before the age of 18, most often due to falls, contact sports, or motor vehicle accidents. 4
Management of coronal tooth fractures depends on factors such as the fracture extent and pattern, pulpal status, soft-tissue and alveolar bone condition, and the viability of the fractured fragment. Additional considerations—occlusion, esthetics, cost, and prognosis—help determine whether conservative restoration, fragment reattachment, endodontic therapy, or extraction is the best option. 3
When an intact fragment is available, reattachment is the preferred conservative approach, particularly for patients with high esthetic expectations. It preserves natural tooth structure, restores the original contour and shade, and maintains incisal translucency.5–7 Among different reattachment methods, the use of a glass-fiber post provides superior retention and stability of the fragment. 5
This article reports two coronal tooth fracture cases that were successfully treated using tooth fragment reattachment.
Case Report
Case 1
Case Report
A 29-year-old male patient reported to the Department of Conservative Dentistry and Endodontics with a chief complaint of trauma-induced fracture and associated pain in the maxillary anterior region. The injury resulted from a road traffic accident, and the patient presented approximately 2 h post-trauma, having preserved the fractured tooth fragment in skimmed milk (Figure 1C), an appropriate medium for maintaining fragment hydration and vitality.
(A) Pre-operative Clinical Photograph (Labial View). (B) Pre-operative Clinical Photograph (Lingual View). (C) Fractured Tooth Fragment. (D) Pre-operative Radiograph. (E) Working Length Determination. (F) Obturation. (G) Post Space Preparation. (H) Clinical Photograph After Electrocautery. (I) Incision. (J) Flap Reflection. (K) Radiograph After Post Cementation.
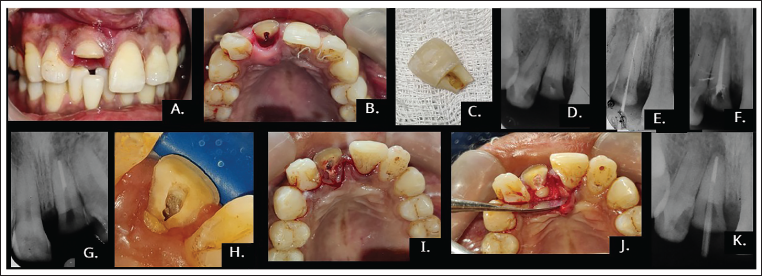
Clinical examination revealed a crown fracture of the right maxillary central incisor, with the labial fracture margin supragingival (Figure 1A) and the lingual margin extending approximately 1–1.5 mm subgingivally (Figure 1B). Cold vitality testing elicited no response, indicating a non-vital pulp. Radiographic assessment showed involvement of enamel, dentin, and pulp (Figure 1D), with only 2–3 mm of coronal tooth structure remaining on the buccal aspect. Soft tissue examination revealed no lip lacerations or other associated injuries, apart from localized gingival inflammation around the affected tooth. Based on clinical and radiographic findings, a diagnosis of a complicated crown fracture with pulpal involvement and a non-vital upper right central incisor (Ellis Class IV fracture irt. 11) was made. Examination of the fractured fragment (Figure 1C) demonstrated an excellent fit with the remaining tooth structure, without any discernible discrepancies in contour or shape.
The treatment options considered included: (a) extraction followed by prosthetic rehabilitation, (b) intra-alveolar repositioning or surgical extrusion, (c) orthodontic extrusion, and (d) reattachment of the fractured fragment following root canal treatment and fiber post placement. After a thorough discussion of the advantages, disadvantages, prognosis, and costs associated with each approach—and taking into account the patient’s strong preference to preserve his natural tooth—reattachment of the fractured fragment was chosen as the treatment of choice.
Local anesthesia was achieved using 2% lignocaine with adrenaline (1:80,000) (Lignox, Mumbai, India) via infiltration around the affected tooth to ensure adequate pain control. All procedures were performed under rubber dam isolation using the split-dam technique. Following access cavity preparation, the working length (Figure 1E) was determined and established at 16 mm. Biomechanical preparation was carried out up to a #60 K-file (Mani, Japan) using the step-back technique. Root canal irrigation was performed using a 2.5% sodium hypochlorite solution. Approximately 10 mL of irrigant was used per canal, delivered with a 30-gauge side-vented needle placed 1 mm short of the working length. Final irrigation was performed with 17% ethylenediaminetetraacetic acid (EDTA) for 1 min, followed by a saline flush. Calcium hydroxide (RC Cal, India) was placed as an intracanal medicament, and the access cavity was temporarily sealed. The patient was scheduled for a follow-up visit after 1 week. The subgingival fragment was stable, and there is no need for splinting of the subgingival fragment.
At the second visit, due to the subgingival extension of the lingual fracture margin, electrocautery was performed to expose the margin while preserving the biological width and allowing proper isolation (Figure 1H). Root canal obturation was subsequently completed using gutta-percha and AH Plus sealer (Dentsply, Germany) employing the lateral condensation technique (Figure 1F).
During the third visit, post space preparation was carried out using a No. 3 Peeso reamer, leaving 5 mm of apical gutta-percha intact (Figure 1G). The fit of the fractured fragment was then verified. A sulcular incision was made, extending one tooth anteriorly and posteriorly to the affected tooth, using a No. 15C blade inserted at a slight angle to the tooth surface and directed into the depth of the gingival sulcus until bone contact was achieved (Figure 1I). The incision was performed in a continuous posterior-to-anterior motion, with care taken to preserve the interdental papilla to ensure optimal esthetic and periodontal outcomes.
The post space was sequentially prepared and cleaned using liquid EDTA (Prime, India). After flap reflection (Figure 1J), a No. 2 fiber post (Angelus, Brazil) was selected. The fiber post was conditioned using 10% hydrofluoric acid (Bisco, Canada), followed by rinsing and drying. Following this, a silane coupling agent (Ivoclar, Switzerland) was applied and left to dry for 30 s. Calibra resin cement (Dentsply, Switzerland) was applied to both the fiber post and the prepared post space. The post was carefully seated and light-cured for 20 s to ensure complete polymerization (Figures 1K and 2A, 2B).
(A) Clinical Photograph After Post Cementation (Labial View). (B) Clinical Photograph After Post Cementation (Lingual View). (C) Immediate Postoperative Clinical Photograph (Labial View). (D) Immediate Postoperative Clinical Photograph (Lingual View). (E) Clinical Photograph After Suturing. (F) Immediate Postoperative Radiograph. (G) Postoperative Clinical Photograph After Finishing and Polishing. (H) Five-year Follow-up Radiograph. (I) Five-year Follow-up Clinical Photograph.
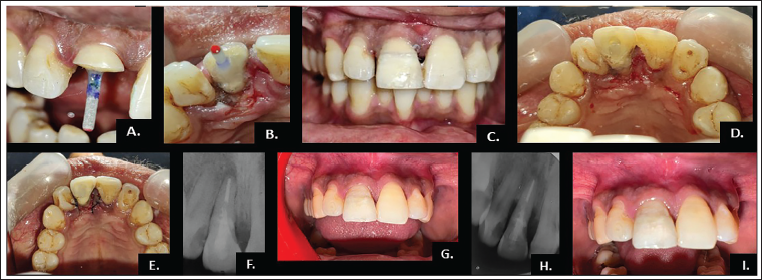
A retentive hole was then prepared in the fractured fragment and in the tooth as well. Both the fragment and the exposed tooth surface were etched with 37% phosphoric acid, rinsed, blot-dried, and treated with a bonding agent (Prime & Bond NT, Dentsply, Switzerland). Self-adhesive resin cement was applied to both the fiber post and the prepared fragment, which was carefully repositioned onto the tooth under firm finger pressure to ensure precise adaptation and alignment, followed by light curing for 20 s (Figure 2C and 2D). At the end, a postoperative radiograph was taken (Figure 2F), followed by the flap was repositioned and sutured using 4-0 non-resorbable sutures (Figure 2E), and occlusion was checked, and postoperative instructions were given to the patient.
After polymerization, excess resin cement was carefully removed using a fine diamond finishing bur. Final finishing and polishing were performed with a Super-Snap Mini Kit (Shofu, Japan) and TC 11EF (Mani, Japan), achieving an optimal esthetic outcome and a smooth surface (Figure 2G).
Follow-up evaluations were conducted periodically over a 5-year period. The restored tooth remained functionally stable and esthetically satisfactory, with no signs of discoloration, fragment detachment, or secondary complications. Radiographic assessment at the 5-year follow-up revealed only localized bone loss around the tooth, while the fragment remained intact and the restoration continued to be clinically serviceable (Figure 2H and 2I).
Case 2
A 28-year-old male patient presented to the Department of Conservative Dentistry and Endodontics with a chief complaint of a fractured tooth and pain in the maxillary anterior region for the past 2 days, following a road traffic accident. Clinical examination revealed a crown fracture of the right maxillary lateral incisor, with the labial fracture margin supragingival and the lingual margin extending approximately 1 mm subgingivally. The patient had preserved the fractured fragment in normal saline to maintain hydration (Figure 3A–3G). The diagnosis was made as an Ellis Class IV fracture irt. 12 .
(A, C) Pre-operative Clinical Photograph (Labial View). (B) Pre-operative Clinical Photograph (Lingual View). (D) Pre-operative Radiograph. (E and F) Clinical Photograph After Fragment Removal (Labial View). (G) Radiograph After Fragment Removal. (H) Obturation. (I) Post-space Preparation. (J) Radiograph After Post Cementation. (K) Clinical Photograph After Post Cementation (Lingual View). (L) Retentive Hole Preparation in Fractured Fragment. (M) Immediate Postoperative Clinical Photograph (Labial View). (N) Immediate Postoperative Radiograph. (O) One Month Follow-up Clinical Photograph.
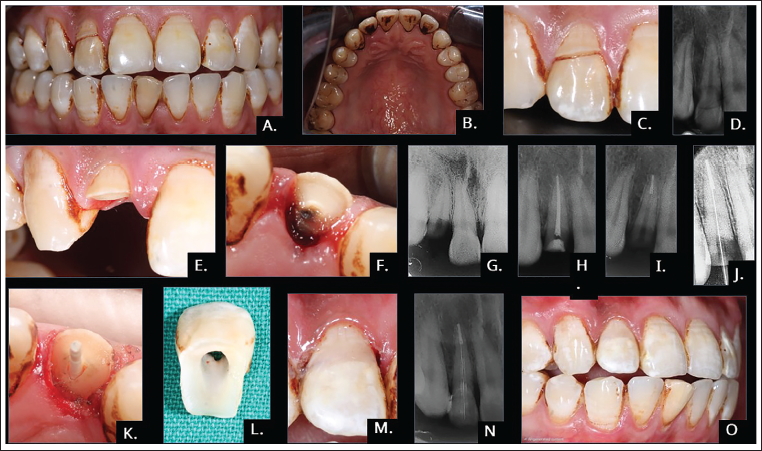
All clinical procedures were performed following the same protocol as in Case 1, including root canal treatment with a master apical file of #50 K-file using a similar step-back method, fiber post placement (No. #2), and reattachment of the fragment using adhesive resin cement (Figure 3H–3N). At the 1-month follow-up, the tooth demonstrated excellent esthetics and functional stability, with no signs of discoloration, fragment detachment, or secondary complications (Figure 3O).
Discussion
The management of fractured anterior teeth has progressed significantly with advances in adhesive dentistry, allowing clinicians to restore both function and esthetics through reattachment of the patient’s own tooth fragment. When biological considerations, material selection, and clinical techniques are carefully evaluated, reattachment can closely replicate the natural characteristics of the original tooth, including its shape, contour, and surface texture. This approach preserves the tooth’s natural color, translucency, and optical properties, ensuring seamless integration with adjacent dentition, while also maintaining natural wear patterns and providing psychological comfort to the patient. 8
Advances in adhesive dentistry have made fragment reattachment a reliable option for managing fractured anterior teeth. With proper case selection, materials, and technique, clinicians can restore the tooth’s natural form, color, translucency, and surface characteristics. This biologically conservative approach preserves tooth structure, blends seamlessly with adjacent teeth, maintains natural wear patterns, and offers significant psychological benefits to patients. 8
When these factors are carefully addressed, reattachment offers predictable and durable outcomes. Studies, including those by Cavalleri and Zerman, have demonstrated that reattached fragments exhibit a favorable long-term prognosis compared with other restorative options, making this technique a dependable and highly esthetic solution for anterior tooth fractures. 8
Fragment discoloration may occur if rehydration is inadequate, and debonding can result from improper adhesive protocol or excessive occlusal forces. Thus, proper case selection, precise bonding, and patient compliance are essential for long-term success. 9
Surgical crown lengthening and orthodontic extrusion were avoided because they would worsen the crown–root ratio, disrupt the gingival zenith, and make biological width preservation difficult, reducing esthetic predictability. 10
Numerous factors influence the longevity of a reattached tooth fragment, including the storage medium used after fracture, the adhesive system and restorative material selected, and the protection of the dentin–pulp complex. The flow properties of the composite resin or luting cement also affect the quality of the bond. Additionally, the specific reattachment technique plays a critical role in the long-term success. 11
In our cases, the fractured fragment was stored in milk (Case 1) and normal saline (Case 2). The choice of storage medium immediately after fracture is crucial, as it maintains hydration and preserves the tooth’s color, translucency, and structural integrity. Hydrated storage also enhances bond strength by preventing the collapse of dentinal collagen fibers, which can impair adhesion.12, 13 Studies show that appropriate storage significantly increases fracture resistance, with skimmed milk providing the highest resistance, followed by normal saline, both outperforming dry storage. 14
Fiber posts are widely accepted in restorative dentistry due to their advantages over metallic posts. Their modulus of elasticity closely matches dentin, allowing better stress distribution and reducing root fracture risk. They can be luted with adhesive systems and resin cements, creating a homogeneous bond within the root. This uniform stress distribution enhances biomechanical performance and results in fewer catastrophic failures compared to traditional metallic posts. 15
Fiber posts offer superior esthetics in the anterior region due to their translucency, avoiding the gray discoloration seen with metal posts. When over 50% of the coronal structure is lost, a post-and-core foundation is indicated. 15 They also require minimal canal preparation, using natural undercuts to enhance bonding while preserving radicular dentin and reducing fracture risk during function or trauma. 16
Surface treatment and cementation of fiber posts are essential for achieving strong, durable adhesion in fragment reattachment. Hydrofluoric acid etching provides the highest bond strength, but bonding is limited because fiber posts contain an epoxy resin matrix that resists penetration by methacrylate-based resins. 15 Therefore, silanization is recommended, as silane enhances the chemical bonding between the post surface and the resin cement. 16
Self-adhesive resin cements, such as Calibra Universal, are widely used due to their dual-cure capability and ability to simultaneously etch and bond through a pH shift during polymerization. They offer good handling and predictable adhesion. 16
Possible long-term complications include bone loss, fragment detachment, and periapical pathology, which may later require an implant or prosthetic rehabilitation. In the present case, bone loss was noted at the 5-year follow-up, though reattachment remained a viable treatment during this period. 8
Conclusion
Reattachment procedures are a valuable option for restoring tooth stability and function while addressing the psychological needs of patients, particularly younger individuals who are keen to retain their natural teeth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval from relevant committee was obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.