
Abstract
The rehabilitation of teeth with severe structural compromise remains a major clinical challenge, especially in the anterior region, where esthetics and periodontal integrity are crucial. Achieving an adequate ferrule effect is essential for long-term restoration success. Orthodontic extrusion represents a conservative alternative to surgical crown lengthening, which may otherwise jeopardize gingival architecture. This case report presents the management of a 65-year-old male with a fractured maxillary canine (tooth 23) that had previously served as a bridge abutment. Radiographic evaluation revealed a fractured endodontic post and minimal remaining coronal structure. Given the favorable root length and bone support, slow orthodontic extrusion was selected over surgical crown lengthening to preserve esthetic harmony. Before extrusion, an adhesive fiber-reinforced biobase was built using polyethylene fiber (Ribbond®) and short fiber-reinforced composite resin (EverX®, GC), following a biomimetic protocol. Orthodontic traction was applied with a closed elastic chain anchored to a passive wire supported by the adjacent provisional implant restoration. Orthodontic extrusion successfully re-established the ferrule effect while maintaining gingival symmetry. The adhesive fiber-reinforced restoration provided internal support without the need for an intra-radicular post, thereby preserving the weakened root. This case highlights how the combination of controlled orthodontic extrusion and biomimetic adhesive reinforcement offers a minimally invasive, functional, and esthetically predictable approach for the rehabilitation of structurally compromised teeth.
Keywords
Introduction
The rehabilitation of severely compromised teeth remains a persistent clinical challenge, particularly when substantial coronal structure has been lost. Preserving the natural tooth is often prioritized over extraction or implant placement, as properly treated and maintained teeth have demonstrated superior long-term survival compared with prosthetic replacements. 1
The ferrule effect—a 1.5- to 2-mm circumferential band of sound tooth structure above the crown margin—is a key biomechanical requirement that significantly reduces fracture risk.2–6 When the ferrule cannot be obtained by conventional means, alternative techniques such as surgical crown lengthening, surgical extrusion, and orthodontic extrusion are available. Among these, orthodontic extrusion stands out as a conservative and biologically respectful option that allows controlled tooth elevation while maintaining periodontal attachment.7–9
Orthodontic extrusion, or forced eruption, uses light continuous forces to elevate the tooth, exposing sound coronal structure while stimulating remodeling of the supporting tissues. This approach is particularly advantageous in the anterior esthetic zone because it preserves interdental papillae and supracrestal tissue integrity.7, 8, 10, 11 Concurrently, advances in biomimetic restorative dentistry have emphasized the preservation and functional imitation of dental tissues. Reinforcing fibers—both continuous and short—mimic the biomechanical properties of dentin and reinforce weakened structures without rigid posts or invasive preparation. Continuous polyethylene fibers (Ribbond®) show an elastic modulus close to dentin (10–30 GPa), enabling stress homogenization and reducing catastrophic fracture risk.12, 13 Short fiber-reinforced composites (SFRCs) such as EverX Posterior and EverX Flow enhance fracture toughness, fatigue resistance, and crack-stopping ability.14–16 This case report demonstrates a conservative, functional, and esthetic approach for the rehabilitation of a severely compromised anterior tooth using slow orthodontic extrusion and biomimetic adhesive reinforcement, highlighting the clinical advantages of preserving both natural tooth structure and periodontal tissues.
Case Presentation
A 65-year-old male with no significant medical history presented to the dental clinic with a fractured prosthetic abutment (tooth 23) of a fixed bridge extending from teeth 21–23. The patient reported: “The tooth holding my bridge broke.” Radiographic examination revealed a fractured endodontic post lodged within the root canal. Tooth 21 showed no abnormalities, and site 22 was edentulous, with implant placement already planned. The patient expressed a strong preference to preserve the remaining natural teeth. Clinical evaluation indicated that tooth 23 had insufficient supragingival structure (less than 2 mm) to achieve a ferrule effect. However, the root presented favorable length and bone support, making preservation feasible. Given the esthetic implications, surgical crown lengthening was ruled out, and slow orthodontic extrusion was indicated to expose sound tooth structure and re-establish a ferrule effect.
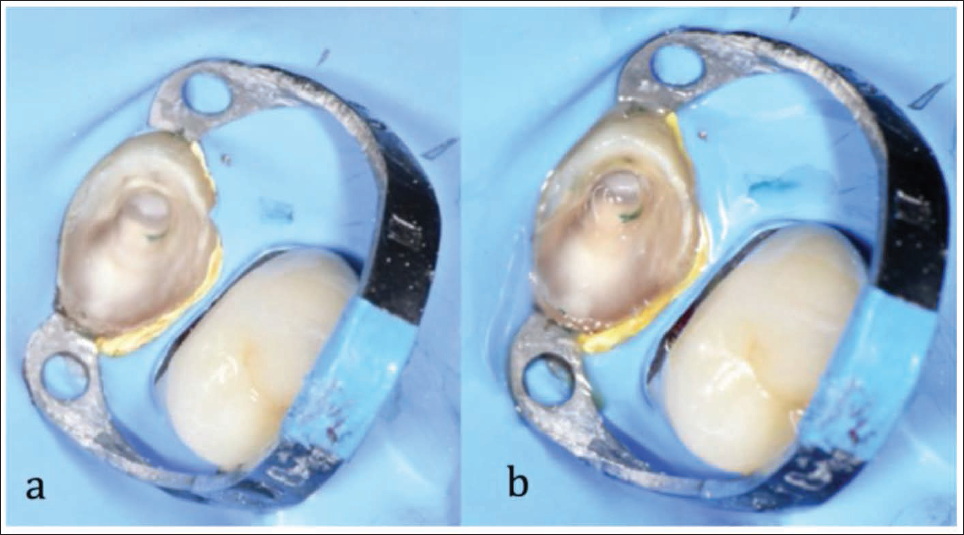
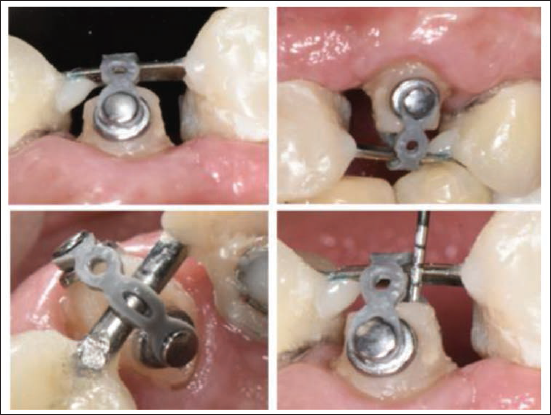
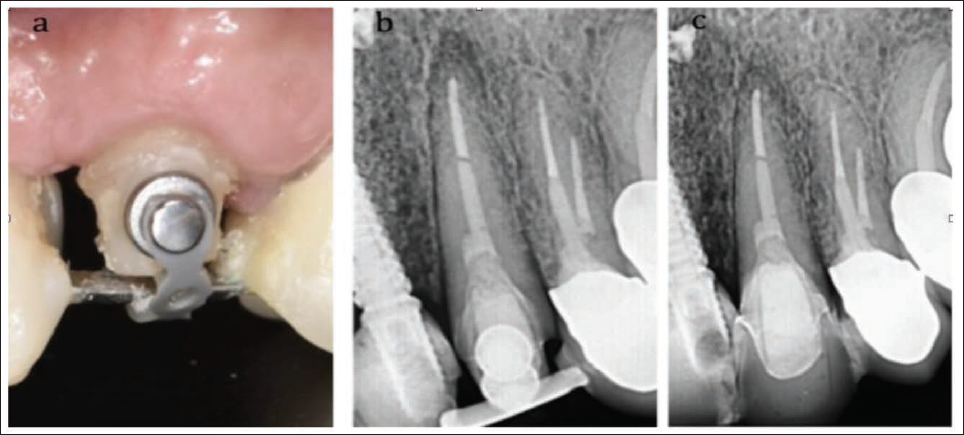
Prior to extrusion, an internal adhesive biobase was built following a biomimetic protocol. Absolute isolation was achieved with a B4 clamp and Teflon inversion of the rubber dam. After caries removal and air-abrasion with 53 µm aluminum oxide, the tooth was treated using a fourth-generation adhesive (Optibond FL®, Kerr). Two Ribbond® strips were placed: a 4-mm buccopalatal and a 2-mm mesiodistal, creating a three-dimensional reinforcement matrix. The cavity was then filled with SFRC resin (EverX®, GC, Tokyo, Japan) to replicate dentin-like resilience (Figures 1–3). Two orthodontic buttons were bonded to the buccal and palatal surfaces near the cervical margin using a universal adhesive (AllBond Universal®, Bisco) and resin (Transbond XT®, 3M Unitek). A closed elastic chain (American Orthodontics®) of four links connected the buttons, applying traction toward a passive wire spanning from tooth 24 to the provisional implant crown at site 22 (Figure 4). After 15 days, sufficient extrusion was achieved to allow crown preparation and ferrule formation. A provisional crown was placed and maintained for 6 weeks to permit soft-tissue stabilization (Figure 5). The definitive zirconia crown was subsequently fabricated and cemented, achieving full esthetic and functional integration (Figure 6).
Tooth Isolation and Adhesive Protocol. (a) Initial Isolation Without Adhesive. (b) Adhesive System Applied and Light-cured.
Fiber-reinforced Biobase with Internal Adhesive Ferrule to Enhance Retention and Stability.
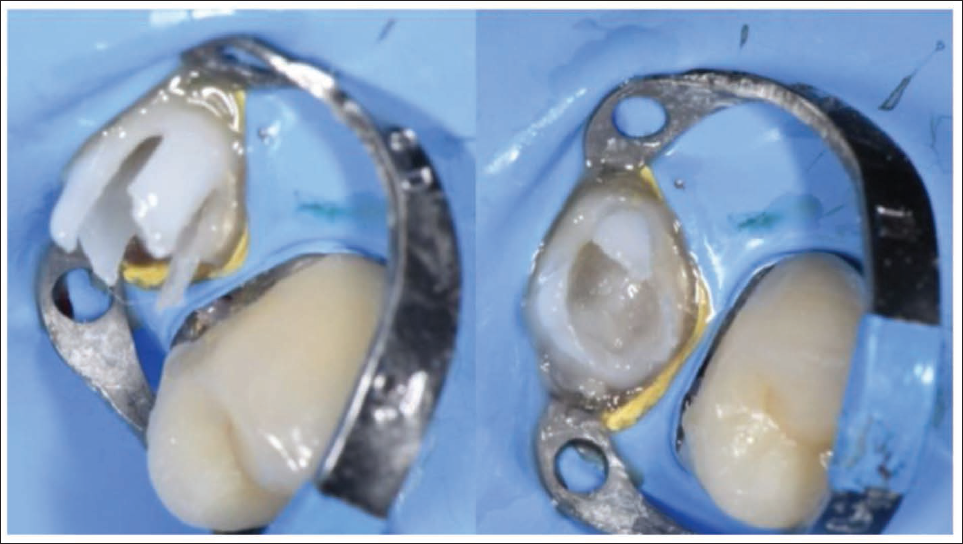
Reconstructed and Prepared Tooth Core After Biomimetic Restoration.

Restorative Abutment With Orthodontic Buttons and Elastic Chain Positioned for Controlled Extrusion.
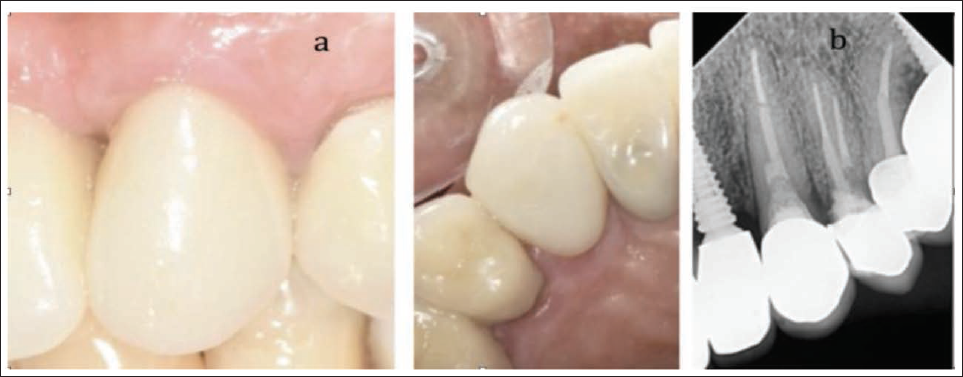
(a) Extruded Abutment Showing Re-established Ferrule Effect. (b) Radiograph After Extrusion Demonstrating Bone Remodeling Consistent With Orthodontic Movement. (c) Radiograph Showing Provisional Restoration in Function.
(a) Definitive Zirconia Crown Integrated Harmoniously Within the Anterior Arch. (b) Postoperative Radiograph Confirming Restoration Stability.
Discussion
Orthodontic extrusion was chosen as the primary treatment approach because it offered the safest and most biologically conservative method for recovering sound coronal tooth structure while preserving periodontal and esthetic harmony. Surgical crown lengthening would have displaced the gingival margin apically and disrupted anterior soft-tissue symmetry, compromising the patient’s smile line, whereas surgical extrusion involved higher biological costs and increased risk of periodontal breakdown. The favorable root length and bone support of tooth 23 further justified preservation over extraction. Consistent with the observations of Cordaro et al. 1 and Roxanna et al., 9 controlled slow extrusion promotes soft-tissue maturation and maintains the interdental papilla and supracrestal attachment apparatus, both essential for achieving long-term esthetic stability in the anterior region.
Although age-related changes in the periodontal ligament and alveolar bone may slow orthodontic tooth movement and increase the risk of root resorption or delayed tissue remodeling, available evidence indicates that adult patients can still undergo controlled orthodontic extrusion successfully when periodontal health and bone support are adequate. Wang et al. 17 reported that, although adults demonstrate reduced cellular activity and slower movement rates, the underlying biological response remains functional and treatment effectiveness is preserved. In the present case, the patient’s favorable periodontal condition and root morphology allowed a predictable extrusion. Although treatment progressed more slowly than in younger individuals, no signs of periodontal deterioration or root resorption were observed during the 12-month follow-up. Regarding relapse, current evidence indicates that orthodontic extrusion demonstrates minimal rebound when an adequate retention period is provided, as periodontal fibers require several weeks to reorganize. A stabilization period of 4–6 weeks is commonly recommended to prevent coronal relapse, and this protocol was followed in the present case. Therefore, controlled orthodontic extrusion remains a viable and safe option even in mature adults, provided that periodontal and osseous conditions are adequate.
The restorative strategy, based on an adhesive biobase combining continuous and short fibers, reinforced the weakened root and restored biomechanical integrity. Continuous polyethylene fibers distribute stresses evenly and prevent crack propagation, whereas short fibers enhance internal toughness and perform as artificial dentin.12, 15 This approach aligns with modern adhesive dentistry principles that prioritize the conservation of residual coronal structure and the avoidance of intra-radicular posts.3, 18 This case confirms that integrating orthodontic extrusion with biomimetic adhesive reinforcement provides a predictable and minimally invasive method for managing structurally compromised teeth. The outcome demonstrates how biologically oriented mechanics and restorative reinforcement can jointly restore function, esthetics, and periodontal harmony.
Conclusion
Controlled orthodontic extrusion proved to be a conservative and esthetically sound method for rehabilitating a structurally compromised anterior tooth. The procedure re-established the ferrule effect without altering gingival architecture and avoided the morbidity associated with surgical crown lengthening. When combined with biomimetic adhesive reinforcement, this approach enables a biologically respectful, functionally durable, and visually harmonious restoration—reinforcing its value as a tooth-preserving strategy in contemporary restorative dentistry.
Footnotes
Acknowledgment
The authors thank the staff of the Clinic/Department for their assistance.
Authors’ Contributions
All authors contributed equally to the conception, clinical management, data acquisition, and manuscript preparation, and approved the final version for publication.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
This clinical case did not require institutional review board approval according to local regulations, as it describes a single-patient treatment carried out in accordance with accepted clinical standards and ethical principles (Declaration of Helsinki).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given written consent for his clinical information and images to be reported in the journal. The patient understands that his name and initials will not be published, and that every effort will be made to conceal his identity. However, complete anonymity cannot be guaranteed.