
Abstract
Introduction
Our scoping review intends to investigate the impact of dental material waste (DMW) on environmental pollution throughout its lifecycle (production, use, and disposal).
Methods
A systematic literature search was conducted across four databases from inception till April 15, 2025. The primary outcomes of this review were to examine the contribution of DMW to environmental pollution by generating a quantitative summary of the amount of material waste produced by dental facilities and its associated pollution indicator.
Results
A total of 2808 records were retrieved, of which only 41 studies were included. 60.98% of the included studies were cross-sectional, 19.52% experimental, and the remaining 19.5% were life cycle assessments, comparative study designs, and one case study. Quantitative summary demonstrated dental amalgams to be a major polluter, and mercury was the primary pollutant. The environmental impact was most significant in the case of water contamination, followed by soil contamination. All the material wastes were found to breach safer concentration limits with mercury being most potent in air, water and soil [mercury = 2.3 mg/L to 261 mg/L (water), 0.094 mg/m3 to 102.7 g/m3 (air), 0.3 g/d to 82.3 g/d (soil)].
Conclusion
The significant contributor to environmental pollution was dental amalgams, from their production to their disposal.
Introduction
Dental waste (DW) produced is are byproduct of the treatments and procedures performed by dental professionals. 1 This includes wastes categorized as hazardous (chemical and toxic), non-hazardous, infectious, sharps, and pharmaceutical waste, which includes dental amalgams, impression materials, cotton swabs, syringes, cardboards, papers, etc. This waste from dentistry accounts for only 3%–4% of the total waste generated by the health sector.2–4 Although this percentage is relatively small, it has demonstrated a significant contribution toward the environmental pollution in terms of carbon emissions, waste production and disposal issues. 5
Dental treatments have prioritized the efficient delivery of quality healthcare, and this has led to the widespread adoption of advanced restorative materials, including nano-engineered materials. 6 As modern dentistry has become more focused toward improving clinical outcomes, it has exacerbated the environmental burden due to different types of waste generated by dental practices in recent times.7–10 Despite such changes, mercury amalgams were identified as one of the common components in the majority of the waste produced, which has been evidenced as a highly toxic metal when exposed to the atmosphere. A report by the United Nations Environmental Program: Global Mercury Assessment Report (2013) revealed that an estimated amount of 270–340 metric tons of mercury entered the environment came from dental amalgams, accounting for approximately 20% of global mercury consumption. 11 Interestingly, Mulligan et al. (2018) reported that every 90,000 kg of mercury used in amalgams results in the entry of 100 kg of mercury delivered to the environment. 12 This creates a concerning image regarding the disposal of these wastes and their aftermath in the environment. Other material wastes like lead (dental radiography), heavy metals, resin composites, ceramics, gypsums, etc., have also demonstrated similar figures. For instance, according to the US Environmental Protection Agency (EPA), dental offices generate about 4.8 million lead foils in a year, which commonly enter the environment through regular domestic waste, indicating that a significant amount of lead waste in the environment has entered till now.4 Similarly, the development of modern resin composite filling material dates back to the late 1950s, when it was assumed earlier to be inert, but is now believed to cause microplastic pollution. 13
Existing literature has evidenced the potential risks of material waste from dentistry in aggravating environmental pollution. Environmental concern is critical, as the entire ecosystem faces significant risks due to the consequences of uncontrolled waste generation and inadequate management practices. 14 The risk of contamination of water or soil can make the whole community living nearby a potential victim of this “ripple” effect. 15 This threatens the sustainability of the environment. 16 Eco-friendly dentistry has gained popularity, but putting it into practice has been a practical challenge. The lack of standard practice protocols for effective DW management has contributed to environmental pollution. 17 While literature appreciates notable efforts like the 3Rs (reduce, reuse, recycle) and the use of filters or trappers to minimize the impact of dental material waste (DMW) before releasing it into the environment, it needs to be implemented uniformly in practice. 18 The available evidence demonstrates a fragmented picture of DMWs and associated environmental complications quantitatively. This evidence narratively demonstrates a relation between material waste from dentistry and the environment. However, it was identified that there exists a paucity of literature that quantitatively evaluates the pattern, nature, and level of association between the two. Thus, this scoping review aims to investigate the impact of DMW on environmental pollution throughout its lifecycle—beginning with industrial manufacturing of dental materials, followed by their use in clinical practice and subsequent disposal. The objective of this review was to quantify the effects of DMW on environmental pollution and analyze the trends in waste production over the years. This study aims to address the existing knowledge gap by offering a perspective on the environmental impact of dental materials. It seeks to quantify existing evidence and analyze global trends in material waste production. Additionally, it aims to support the development of practical solutions to enhance the environmental sustainability of dental care, aligning with the goals of sustainable development.
Methods
This scoping review was conducted according to the Joanne Briggs’ Institute, 2020
19
and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA-SCR) guidelines.
20
A scoping review was chosen to comprehensively cover the subject area and incorporate a diverse range of relevant study designs. Furthermore, it was necessary to conduct a wider search for studies that investigated the environmental impact of DMW. The protocol was developed and prospectively registered with Open Science Framework (Registration DOI:
Research Question (PCC Framework)
Population: Dental clinical facilities and dental professionals.
Concept: Environmental impacts of DMW, including waste generation, pollutant release, and sustainability indicators.
Context: Any geographical setting and any stage of the material lifecycle (manufacture, clinical use, disposal).
Research question: “How do commonly used dental materials contribute to environmental pollution across their lifecycle within dental care settings?”
Search Strategy and Information Sources
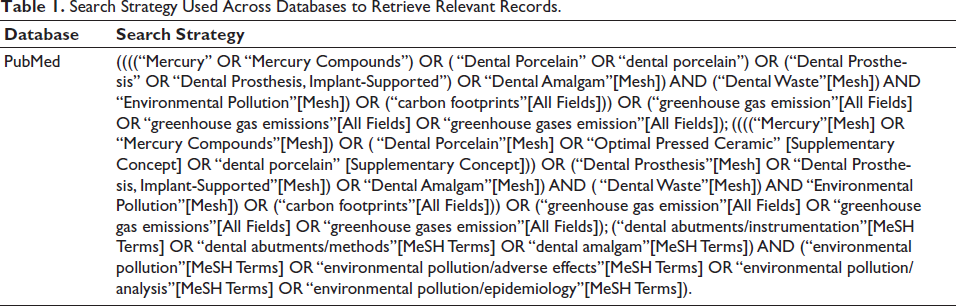
Based on the focused research question, a robust search strategy was designed using the Medical Subject Headings (MeSH) terms and the Boolean operators like “AND” and “OR” (Table 1). An exhaustive literature search was conducted by two authors (AM and MB) independently across four electronic databases: PubMed-Medline, EMBASE, Scopus, and Science Direct from inception till April 15th, 2025. A manual search was also conducted using Google Scholar to retrieve gray literature. Additionally, sources like the WHO Healthcare Waste Management Repository Resources, 3 EPA’s Waste and Recycling Section, 4 European Environment Agency (EEA) Environment and Health Section 21 and Fédération Dentaire Internationale (FDI’s) “Sustainability in Dentistry” report, 22 were explored to retrieve additional relevant literature. The full search strings for all databases, including keywords, MeSH terms, and Boolean operators, are provided in Supplementary File 2 along with the date of the last search (April 15, 2025).
Search Strategy Used Across Databases to Retrieve Relevant Records.
Eligibility Criteria
In order to be included in this review, research records are required to meet the systematically set eligibility criteria. Studies were only included if they examined the association between DMW and its impact on environmental pollution. Only studies utilizing primary study designs, including cross-sectional, longitudinal, cohort, ecological, or life cycle analysis, were deemed eligible for inclusion. Retrieved records not originally in English were translated into English following the methodology outlined by Balk et al. (2013). 23 However, records identified as reviews (narrative, systematic, mini, etc.), opinion or perspective articles, commentaries, short communications, letters to editors, etc., were excluded from the scope of this review.
Inclusion criteria:
Primary empirical studies (cross-sectional, cohort, longitudinal, experimental, life cycle assessments, ecological studies). Studies reporting quantitative or qualitative data on waste generation, pollutant concentrations, or environmental indicators (e.g., COD, BOD, CO₂-eq). Studies examining air, water, or soil contamination attributable to dental materials. Gray literature from reputable bodies (WHO, EPA, EEA, FDI) if containing primary environmental data.
Exclusion criteria:
Review articles, commentaries, letters, opinions, and short communications. Studies lacking environmental outcome measures. Records without an accessible full text.
Gray Literature Handling
Gray literature was screened using the same PCC-aligned criteria. Only documents reporting primary environmental measurements or quantitative waste estimates were included.
Screening and Selection
The retrieved records were imported into Zotero 5.0 for an initial screening based on titles and abstracts. They were further imported into MS Excel (version 2019) to manage the pooled data. Another screening process was conducted independently by two reviewers (AM and MB) to exclude irrelevant records based on the type of document. Records that were without an abstract but indicated an alignment with current review objectives were considered potentially eligible for full-text screening. Any disagreements between the two reviewers were resolved through mutual discussion, and in cases where a common consensus could not be reached, the decision of a third reviewer (VM) was considered final. At this stage, extensive full-text records retrieval was conducted. Additionally, two reviewers (AM and MB) manually searched the reference lists of all selected studies to enhance the maximum coverage of the potentially eligible records. The level of agreement between the two reviewers, calculated by Cohen’s kappa (k), was 0.92 for titles and abstracts and 0.90 for full texts.
Outcomes to Be Measured
The primary outcomes of this review were to examine the contribution of DMW to environmental pollution by generating a quantitative summary of the amount of material waste produced by dental facilities and its associated pollution indicator, as reported by the included research records. The secondary outcome measure of this review was to illustrate trends in material waste generated from dental facilities over the years.
Data Items
There were multiple outcome variables considered for analysis under this scoping review:
Environmental pollution: This was conceptualized in terms of material concentration, either in wastewater, in the form of vapors, or in municipal waste. Pollution indicators: This is measured in terms of CO2 emitted, pH of water or soil, biochemical oxygen demand/chemical oxygen demand [COD]), eutrophication, and mercury vapor released. Material waste (or DMW): It refers to material waste such as amalgams, resin-based composites, lead, heavy metals, etc., produced during dental treatments. Material production: This review has reported waste generated per dental chair, procedure, or clinic in terms of “g day-1” or “g patient-1.” DW: It consists of dental wastewater (DWW) and dental solid waste (DSW). Here, DWW is a heterogenous fluid containing saliva, treatment water, etc., released from the dental clinic/chair/procedure as a discharge. DSW is a mixture of all the waste released from dental practice categorized as infectious, non-infectious, hazardous, biodegradable, non-biodegradable or biomedical waste.
Data Extraction and Data Analysis
Data extraction followed a predefined charting framework consistent with JBI and PRISMA-ScR guidance. 19 Two reviewers independently extracted study characteristics, waste quantities, pollutant concentrations, and environmental indicators.
Thematic charting was performed by grouping extracted data into predefined analytical domains:
Waste generation patterns, Water contamination, Air emissions, Soil contamination, Greenhouse gas emissions, and Public-health hazards.
Disagreements were resolved by consensus, with adjudication by a third reviewer when necessary.
Methodological Quality Appraisal
Consistent with scoping review guidelines, a formal assessment of the methodological quality of the included articles was not conducted.
Results
Search Results and Study Selection
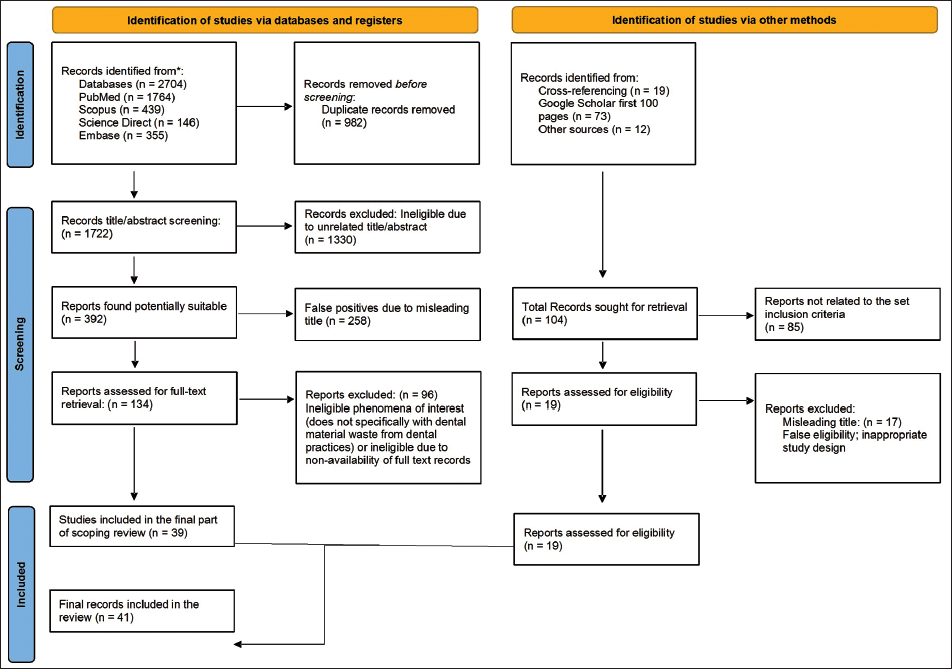
A total of 2,808 records were identified, including 2,704 records retrieved from database searches and 104 records from additional sources. After removing 982 duplicates, 1,826 unique records underwent title and abstract screening. Of these, 1,692 records were excluded for not meeting the PCC-aligned eligibility criteria. Full texts were retrieved for 134 potentially eligible articles, and 93 were excluded for the following reasons: No primary environmental data reported (n = 41), non-eligible study design (review, commentary, opinion, short communication) (n = 27), No environmental outcome measures (n = 15), Full text unavailable or insufficient data for extraction (n = 10). A total of 41 studies satisfied all inclusion criteria and were incorporated into the final synthesis. The complete selection process, with numeric details at each stage and categorization of all full-text exclusions, is shown in the updated PRISMA-ScR flow diagram (Figure 1).
PRISMA Flowchart to Depict the Selection Process.
Study Characteristics
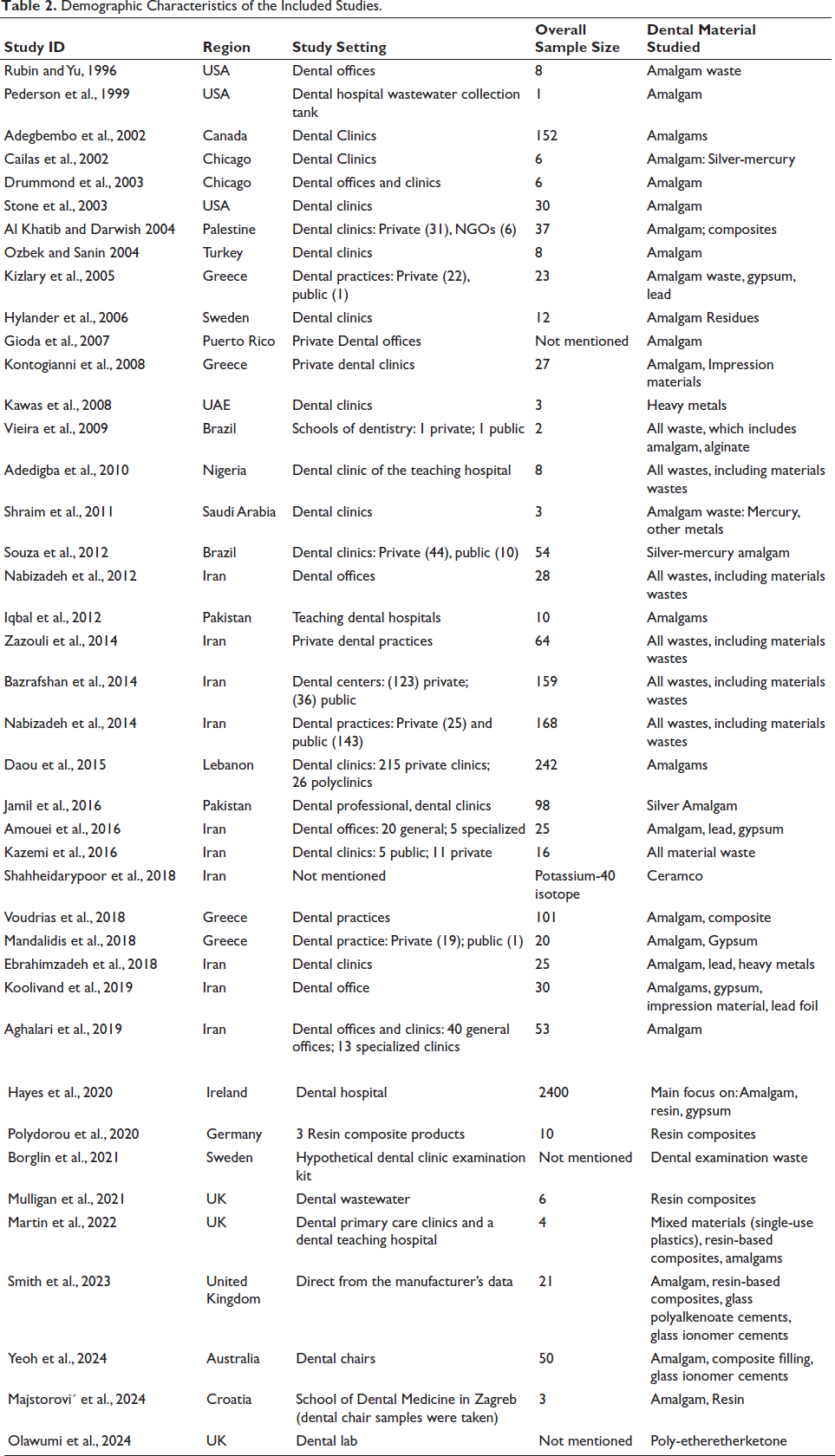
A total of 41 studies were included in this scoping review.1, 2, 7, 8, 24–59 Table 2 represents the demographic characteristics of the included studies. Of the 41 studies included, 60.98% (n = 25) utilized cross-sectional study designs, 19.52% (n = 8) were experimental studies, while the remaining studies comprised life cycle assessments (n = 4), comparative studies (n = 2), and one observational study and one case study (n = 1 each). The majority of the included studies were from Iran (n = 10), followed by the UK (n = 4) and the USA (n = 3). The overall sample size covered under this review was 3913. The distribution of overall study settings was heterogeneous, ranging from dental clinics (private and public), dental offices, dental hospitals (mostly teaching institutes), and dental professionals to miscellaneous settings like NGOs and dental experimental labs. As shown in Table 2, 34.15% of the included studies focused exclusively on amalgam waste. The remaining studies examined other material wastes, with amalgams frequently included as a common component.
Demographic Characteristics of the Included Studies.
To ensure coherence and clarity, the findings of this scoping review are presented according to key thematic domains identified during data extraction. These themes include: (a) patterns of DMW generation across clinical settings; (b) contamination of water systems with mercury, heavy metals, and monomeric residues as reported in the included studies; (c) air contamination related to mercury vapor release from amalgam handling; (d) soil contamination resulting from improper disposal of solid DW; (e) greenhouse gas emissions associated with the lifecycle of dental materials; and (f) public-health hazards emerging from identified pollutants. The subsequent subsections present the quantitative findings and associated risks within these thematic categories while maintaining the original structure and reported values from the included studies.
Amount of DMW Generated and Associated Pollution Indicator: A Quantitative Summary of Evidence
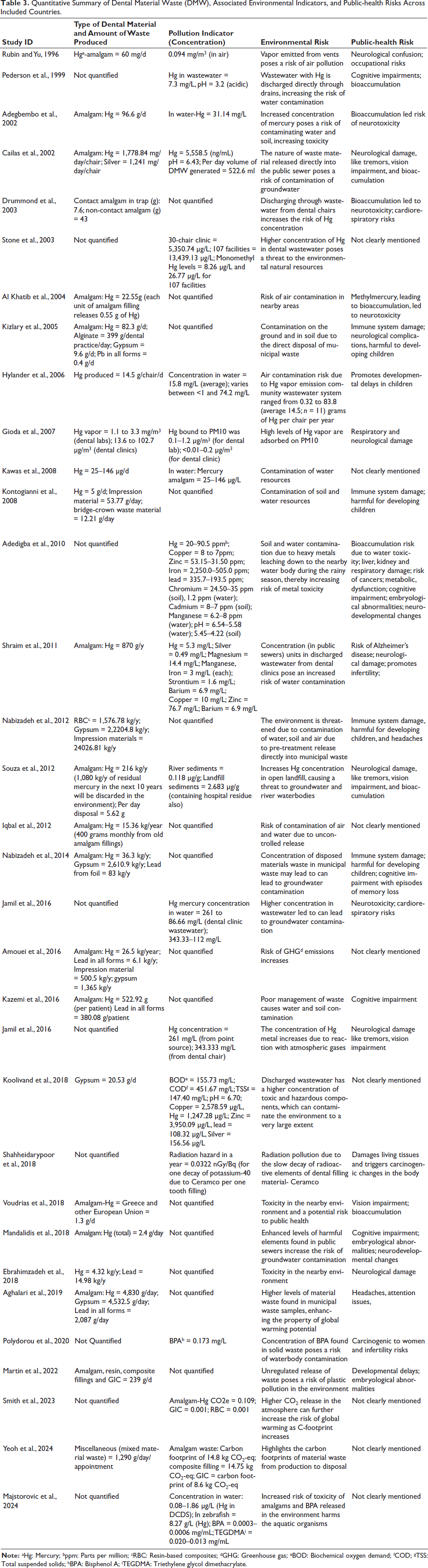
This section quantitatively summarizes the amount of DMW produced by different dental facilities and its associated impact on the environment. Overall, out of 41 included studies, only 33 of them have reported quantitative evidence. Tables 2–4 collectively include all quantitative variables required for environmental assessment. Table 2 provides the country of origin, sample size, study setting, and specific dental materials assessed. Table 3 illustrates that mercury is the primary pollutant, and dental amalgams are the most commonly studied DMW (n = 31) compared to others. Studies have measured pollution parameters mostly in terms of concentration of air, water and soil; level of pH; or biological oxygen demand (BOD), COD, and carbon footprint (CO₂-eq). Table 3 illustrates that prior to 2010, studies primarily focused on mercury pollution in water and air. However, after 2015, research expanded to include carbon footprints, life cycle analysis, and plastic pollution alongside the previously studied topics. The overall assessment indicates that mercury, gypsum, and lead were major contributors to pollution in the form of air, water, and soil contamination, thereby exacerbating the global issue of climate change.
Quantitative Summary of Dental Material Waste (DMW), Associated Environmental Indicators, and Public-health Risks Across Included Countries.
Comparison Between Standard Threshold Limits and Reported Levels of Concentration of DMW in the Environment
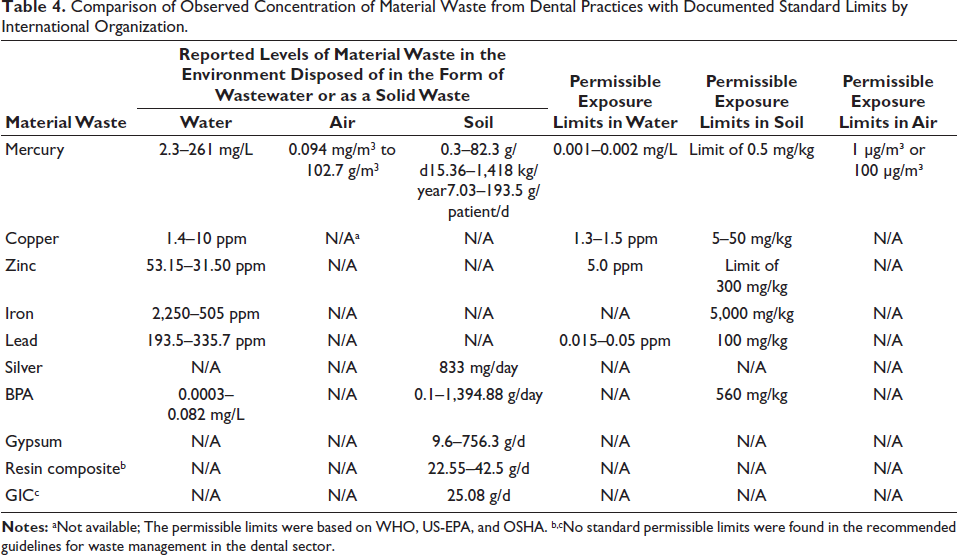
Table 4 compares the analysis performed on the concentration of material waste released from dental facilities reported by the included studies and standard threshold limits. These limits were set by the US-EPA, OSHA (Occupational Safety and Health Administration), World Health Organization (WHO) and EEA.60, 61 On observing the data from Table 4, it can be seen that the concentration of DMWs in the environment has been substantially high, indicating potential hazards to environmental and human health. Clearly, mercury from amalgams has shown significant concentration levels in air, water and soil. Also, resin and glass ionomer cement were considered substitutes for amalgams. However, the release of chemicals from them did not have standard benchmark limits to compare the actual observed concentration in the environment.
Comparison of Observed Concentration of Material Waste from Dental Practices with Documented Standard Limits by International Organization.
Environmental Impact of DMW
Water, air and soil contamination: Tables 3 and 4 illustrate the concentration of different material waste from dental procedures on the water resources (nearby waterbodies or groundwater). Upon examination of the reported evidence from included studies (Table 2), it was found that 19 of them highlighted the risk of water contamination, 7 studies emphasized the increased risk of air contamination, and 4 of them showed the risk of soil contamination in the form of pH decrease, increased levels of biochemical oxygen demand, COD, bioaccumulation and total suspended solids (TSS); and increased concentration of heavy metals resulting in metal toxicity. This indicates that dental materials have significantly impacted the ecosystem as well as the communities surrounding them.
Greenhouse gas emissions: Table 3 demonstrates the emission rates of greenhouse gases in the form of carbon equivalents released when the material waste was disposed of without pre-treatment. Out of all the included studies, only four of them document greenhouse gas emissions (either narratively or quantitatively) due to DMW disposed of directly into the environment. From Table 3, it can be observed that dental amalgams have the highest carbon footprints, ranging between 0.109 and 14.8 kg CO2-eq, compared to other material waste. However, a research report by the National Health Service (2018) highlighted that amalgams and composite waste represent carbon footprints of 14.76 kgCO2e and 14.75 kgCO2e, respectively, each year in England, which were almost similar to one another. This indicates that a significant proportion of carbon dioxide was emitted from dental treatment, where dental restorations were performed.
Public-health hazard: A total of 25 studies in Table 3 have mentioned that as the untreated wastewater enters the surrounding natural resources, the risk of contamination subsequently increases. This affects the health and well-being of the nearby communities, especially in cases of bisphenol A and lead toxicity. It was interesting to note that one of the studies by Shahheidarypoor et al. (2018) highlighted the risk of radiation exposure due to the radioactive properties of Ceramco material used in the dental filling because of the element K40 (radioactive potassium isotope) present in it. 46 This indicates the risk of serious health hazards due to radiation exposure from the environment.
Trends in DMW Production Over the Years Among Different Countries
Comparison of Amalgam Waste Produced Across Different Countries Over the Years: Figure 2 represents a global hotspot map indicating major dental amalgam produced from 1996 to 2018. The figure shows that Iran remained the most significant generator of amalgam waste compared to others. However, evidence has demonstrated that overall, waste generation in Iran was reportedly low. This indicates that the amount of DMW produced by this country demonstrates variability due to differences in the total number of dental facilities present in different areas.49, 51 This map represents a global overview of dental amalgams, indicating better performance in Western countries than in other regions. It is noteworthy that despite the availability of quantitative evidence on other material waste, hotspot maps were only generated for dental amalgams due to non-uniformity in the reported data across different geographical regions.
Major Hotspots of Average Dental Amalgam Waste Produced Between 1996 and 2018.

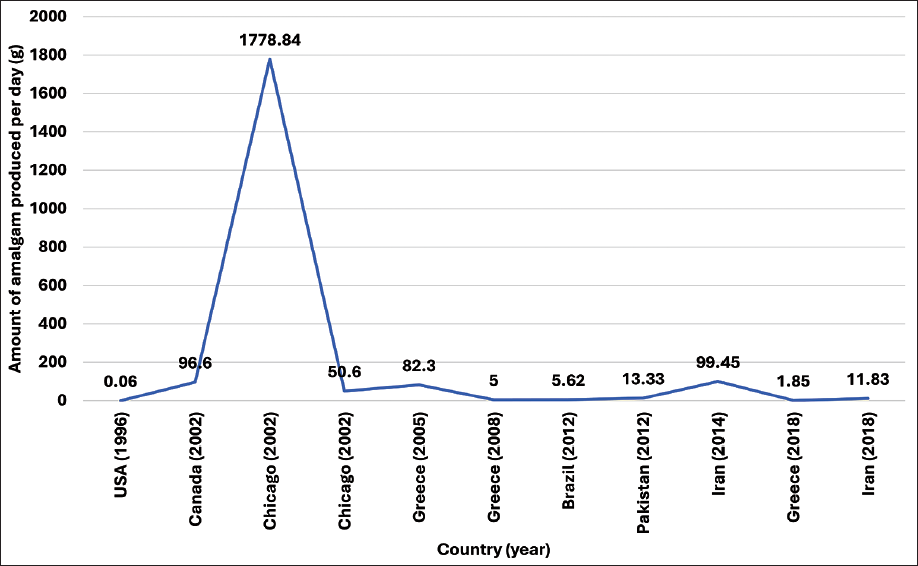
Trend analysis of waste generated over the years in different parts of the world: Figure 3 represents the trends in the amount of amalgam waste generated over the years across different countries. The figure shows that Chicago in 2002 remained the highest amalgam producer with an average of 1,778.84 g/d; however, by 2003, it had been reduced to 50.6 g/d. This can be due to the variability in measuring the data or the significant implementation of management strategies in dental facilities. 61 Also, the USA was observed to generate less amalgam waste (<1 g/d) compared to others. Iran has substantially reduced amalgam waste generation from 2014 (99.45 g/d) to 11.83 g/d (2018). This indicates that those countries that were aware of amalgam waste management strategies have managed to reduce the waste produced per day compared to others.
Trends in Amalgam Waste Produced in Different Countries Over the Years.
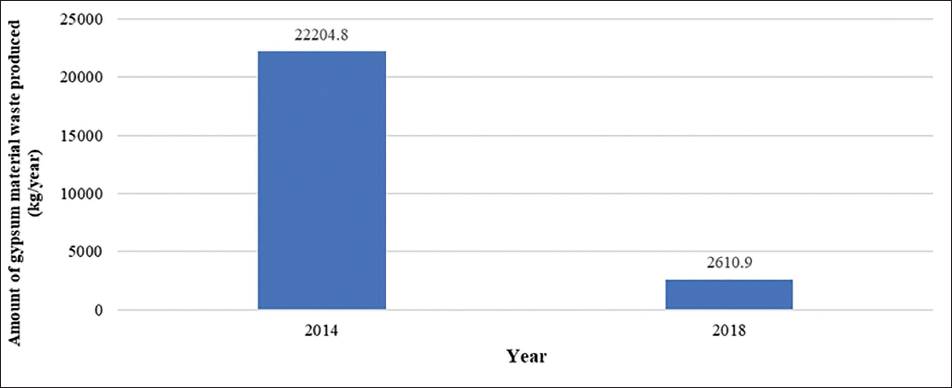
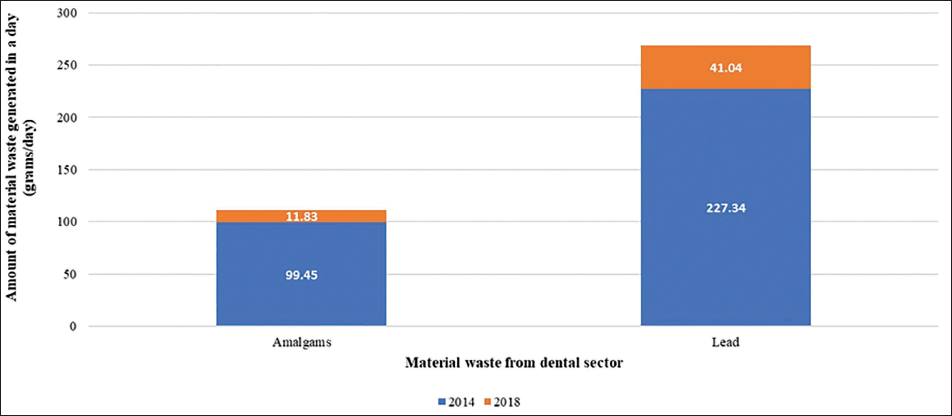
Case study of Iran: This country has demonstrated contrasting evidence in terms of waste generation rate. In analyzing Figures 4 and 5, it was found that the amount of mercury (from 99.45 g/day in 2012 to 11.83 g/day in 2018), lead (from 227.34 g/day in 2012 to 41.04 g/day in 2018) and gypsum material waste (from 22,204.8 kg/year in 2012 to 2,610.9 kg/year in 2018) produced has significantly reduced over the years. Hence, an individual analysis was carried out to establish the probable reason for such variability in the reporting. It indicates that in the categories of DMWs, production rates have reduced over the years, which would have contributed to the overall reduction rates in DW.
Variation in Amount of Gypsum Material Waste Generated in Iran in 2014 and 2018.
Variation in Amount of Amalgam and Lead Waste Generated in Iran in 2014 and 2018.
Discussion
The current trends in DMW management center around recycling, minimizing single-use plastics, regulation-compliant waste disposal and segregation and the adoption of digital technology to minimize material use and embrace green practices. While the quantitative findings are detailed in the Results section, the following discussion focuses on their broader implications for environmental stewardship, regulation, and future research directions rather than reiterating individual data points.
The findings of our study reveal that a substantial amount of material waste has been generated from the dental sector over the years. This has left an indelible carbon footprint on the environment by contaminating natural resources and causing microplastic pollution. Our findings highlight critical issues and the complexity of managing associated material waste sustainably.
The review reveals that the environmental impact of dental materials is multifaceted, with significant contributions to environmental pollution throughout their lifecycle. The review highlighted that dental amalgam emerged as the main polluter due to mercury release in the environment, affecting air, water, and soil ecosystems significantly. The trend analysis demonstrated an overall reduction in dental amalgam over the years. However, a complete phase-out has been challenging. Bansal et al. observed that this indicated the lack of professional commitment to support environmental sustainability efforts. 62 A revelation while analyzing the studies was a marked shift in areas of research post-2010. Prior to 2010, literature on biomedical waste centered on amalgam pollution, while contemporary focus has shifted to carbon footprint, life cycle assessments, and plastic pollution. Iftikhar et al. noted that trends in research since 2012 have shifted toward biocompatible materials like resin composites and glass ionomer cements, with a substantial decrease in silver and mercury amalgam-based research. 63 Although resin-based composites are increasingly used as amalgam substitutes, emerging evidence shows leaching of monomers such as BPA and TEGDMA into wastewater, with demonstrated ecotoxicity in aquatic organisms. The environmental burden of resin materials, therefore, remains understudied and warrants urgent lifecycle assessments. This ongoing evolution in the priority of research harbingers the alignment of the dental field toward global sustainability, as attested by a working paper on “Sustainability in Dentistry” in 2017. 22
An analysis of material waste concentration in the environment highlighted significant breaches against threshold limits. However, there have been limitations in the generalization of these results due to the lack of availability of comprehensive data specific to DMW. This is in concurrence with the recent research related to the field by Shinkai et al. and Myszograj Martyna (2023).14, 64 It is noteworthy that higher concentration levels of toxic waste from dental practices compromise public health in contaminated areas, like an increase in the incidence of neurological problems and cognitive impairment, along with skin and respiratory problems. Several studies by Bates et al. (2006), Ekino et al. (2007), Mackey et al. (2014), and Babanyara et al. (2015) have reiterated similar concerns regarding the risk associated with public-health hazards.65–68 This has raised a pressing concern among experts regarding the detrimental effects of unregulated waste disposal. Several reviews have stressed the importance of sustainable practices and awareness among dental practitioners for effective management strategies for DMW.69, 70
In addition to the above observations, this scoping review also reflects upon the geographical landscape of evidence on DMW and its subsequent environmental impact. It has demonstrated a visible bias in the origin of the research, inclining toward Iran, the UK, and the USA. This observation was supported by Martin et al. (2021), indicating limitations in comprehensive coverage on this subject from across the world. 71 Furthermore, it has been noted that methodologies employed while conducting research vary significantly, especially in the classification of categories of DMW. Most of the studies have classified waste under the categories: infectious/potentially infectious and toxins/chemicals/pharmaceuticals. The lack of clear categorization hampers effective waste management strategies, and it is imperative to formulate clear guidelines suitable for the unique requirements of the dental sector.72, 73 Another important observation made was regarding methods employed in calculating waste generated by dental facilities in the included studies. There were different units in which the amount of waste generated was represented, which included “grams per day,” “milligrams per day,” “grams per patient per day,” or “grams per dental chair per day.” This variability has limited the generalizability of the findings in the context of the real world. This issue has also presented significant challenges in estimating the carbon footprints of dental materials due to the absence of standardized benchmarks, as attested by the National Health Service (2018). This is in concurrence with the observations of Duane et al. (2020), Khanna et al. (2023) and Mitsika et al. (2024), indicating criticality in selecting appropriate metrics while reporting data.10, 73, 74
Our review found that existing studies have reported the environmental implications of dental materials by covering different themes. The limited quantitative studies on the lifecycle of DMWs have constricted our understanding of their associated environmental impact.75, 76 There appears to be a dearth of published literature on DMW-like nano-composites, silver nano-particle-infused resins, bioactive glass, lithium disilicate glass ceramics and CAD/CAM-based restorative materials, and their contribution toward environmental pollution.13, 77–79 Supporting a similar view, Huerta et al. (2016) indicate the importance of exploring potential risks associated with the environment in the context of emerging technologies in dental restorative treatments. 80 It is pertinent to note that assessing the impact of training and awareness programs given to dental professionals in the area of biomedical DMW and environmental pollution has largely remained unexplored. This view was in accordance with the studies by Duane et al. (2020) and Martin et al. (2021), highlighting the focus required in outcome-based research to develop outcome-based training modules for dental staff.74, 81 Furthermore, this scoping review attempts to make an important contribution to the existing knowledge gap by quantifying the pollution footprints of DMW, which will be beneficial in shaping the direction of future research. There is a pressing need for novel studies to diversify their focus by performing detailed assessments of the lifecycle of individual dental materials to better understand their role in exacerbating environmental pollution. Lifecycle assessment of dental materials and heatmap analysis will significantly contribute to understanding the subject more appropriately.
These results are consistent with broader environmental health literature, which highlights the absence of standardized pollutant metrics, fragmented waste categorization, and weak regulatory enforcement across healthcare sectors. Standard guidelines given by the WHO on medical waste management should be adhered to. Studies by Subramanian et al. (2021), Zaharieva et al. (2022), and Billo et al. (2024) have indicated best practices like waste minimization and recycling to avoid point source pollution due to monomers from resin-based restorative material waste.82–84 Previous studies have also emphasized this recommendation, highlighting the importance of environmental stewardship and a sustainable future. Interventions mentioned by Alharbi et al. (2021) and Shinkai et al. (2023), such as utilizing BPA-free resin composites, ceramic endosseous implant materials, and installing recycling and waste processing units, are crucial initiatives in reducing the environmental footprint of DMWs.14, 85 Clark et al. (2002) and the WHO (2010) have noted that such practices will potentially reduce the dangers of “community contamination.”86, 87 Dobrzański et al. (2020), Martin et al. (2021), and Chanioti et al. (2024) are in favor of a policy-based approach emphasizing the importance of collaboration between dental professionals, manufacturers, and the government to incorporate principles of public-private partnership in mitigating environmental damage. Strict norms to regulate disposing of hazardous material wastes from dental facilities would foster positive change in the practice of dental professionals and encourage constructive transformation in this domain.71, 88–91 As the demand for eco-conscious dentistry grows, these efforts are likely to continue evolving, balancing clinical efficacy with environmental responsibility. The FDI Sustainability in Dentistry initiative and WHO green-healthcare guidance offer structured frameworks for reducing waste, implementing closed-loop systems, and standardizing environmental indicators across dental settings. However, adoption remains variable.
Limitations
The study identified no usable benchmark for carbon-emission estimations for DMW. More broadly, the quantification of environmental impacts was constrained by the absence of standardized reporting metrics across studies. Pollutant concentrations were expressed in heterogeneous units (e.g., mg/L, µg/m³, g/day), carbon footprints were calculated using different lifecycle assumptions, and several materials lacked any internationally accepted reference thresholds. This lack of harmonization limited the comparability of environmental indicators and complicates the interpretation of the magnitude of pollution. The study aimed to present a global perspective, but there was a marked geographical bias in the evidence, as most of the studies included belonged to Iran, the UK, or the USA. Some studies painted a hypothetical picture with laboratory examinations rather than real-world estimations. Temporal gaps in the reviewed literature may undermine the current image of DMW management practices. The data available for assessment were not uniform; therefore, generalization of the obtained results is not guaranteed.
Conclusion
This scoping review demonstrates that DMW poses measurable environmental risks, underscoring deficiencies in current waste management and regulatory systems. The findings point to the need for actionable changes, including stricter enforcement of amalgam-related controls, standardized monitoring of wastewater and solid-waste outputs, and broader adoption of sustainable material alternatives. Critical research gaps remain, particularly in the absence of universally accepted metrics for environmental impact, limited real-world lifecycle assessments of contemporary restorative materials, and a lack of longitudinal evidence quantifying cumulative ecological burdens. Future work should prioritize harmonized environmental indicators, multicenter studies that reflect diverse practice contexts, and integrated policy frameworks that align dental care with broader health-sector sustainability goals.
Footnotes
Authors’ Contribution
Conceptualization; protocol development; database search; data extraction; drafting of manuscript-VM; Methodology; validation; critical review of content-LF; Data analysis; interpretation; manuscript refinement- CG; Independent screening; data extraction; verification- AM; Supervision; expert input; final manuscript approval- JFF.
Data Availability Statement
All data used in this scoping review were extracted from publicly available studies. No new datasets were generated. Supplementary materials (search strategy, PRISMA-ScR checklist) are provided as additional files.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
This study is a scoping review synthesizing previously published data. No ethics approval was required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.