
Abstract
Background:
Memory impairments are among the most common and disabling consequences of stroke, significantly affecting cognitive recovery and daily independence. Structured memory training strategies offer a promising, non-pharmacological approach to cognitive rehabilitation.
Purpose:
This study investigated the effects of a 14-day memory training program grounded in five core strategies—repetition, association, method of loci, chunking, and attention training—on cognitive and functional outcomes in stroke survivors.
Methods:
In a quasi-experimental design, 60 participants were assigned to either a memory strategy training group or a control group receiving standard care. Cognitive performance was evaluated using the MMSE and RBMT-II, while functional ability was assessed with the Barthel Index, pre- and post-intervention.
Results:
The memory training strategy group showed significant improvements in MMSE (t = −10.29, p < .001) and RBMT-II (t = −11.52, p < .001) compared to controls. No significant difference was observed in Barthel Index scores.
Conclusions:
Memory training strategies are effective in enhancing post-stroke memory and cognitive function. These findings support the integration of mnemonic-based education into early rehabilitation programs for stroke patients.
Introduction
Stroke remains a major global health concern and is one of the leading causes of long-term disability worldwide. Cognitive impairments are among the most prevalent sequelae of stroke, affecting domains such as attention, memory, executive function, and processing speed. These deficits significantly hinder community reintegration and the ability to regain independence in daily activities. Recent studies report that more than half of stroke survivors continue to experience cognitive impairment months or even years after the event (Einstad et al., 2021; Gallucci et al., 2024).
In recent years, post-stroke cognitive interventions have gained robust empirical support. International and national clinical guidelines—including those from the American Heart Association/American Stroke Association (Winstein et al., 2016) and the Taiwan Stroke Society (Chi et al., 2022)—recommend incorporating structured cognitive rehabilitation early in the recovery process. The landscape of cognitive rehabilitation has evolved from general mental stimulation toward more targeted restorative and compensatory frameworks. Restorative approaches aim to reinforce or re-establish previously intact patterns of behavior through repetitive, task-specific practice, while compensatory strategies focus on teaching patients new ways to perform tasks by bypassing their cognitive deficits. Meta-analyses demonstrate that these structured interventions can induce neuroplastic changes, strengthening functional connectivity in residual neural networks and leading to meaningful gains in participation and quality of life (Cicerone et al., 2019; Golijani-Moghaddam et al., 2022; Kersey et al., 2025).
Among available techniques, memory strategy training has shown particularly promising results. Mnemonic approaches—such as repetition, association, chunking, and method of loci—facilitate information encoding and retrieval by strengthening neural processing pathways and promoting compensatory mechanisms. Studies have demonstrated that structured memory strategy programs can improve verbal recall, prospective memory, and everyday memory performance in adults with neurological impairment, including stroke survivors (Aben et al., 2009; Chen et al., 2012; Kong et al., 2024; Landínez-Martínez & Grisales-Aguirre, 2025; Miotto et al., 2021; Olabarrieta-Landa et al., 2021; Poulin et al., 2012; Scheffler et al., 2025; Studer et al., 2021; van Heugten et al., 2000; Withiel et al., 2020; Wong et al., 2021). However, a critical limitation in current literature is the scarcity of methodological detail regarding intervention intensity, the role of independent practice (homework), and how recovery correlates with lesion-specific characteristics.
Despite increasing international evidence, research on structured, multi-strategy memory interventions in Taiwan remains limited, especially during early inpatient rehabilitation where neuroplasticity is most active. This gap is clinically relevant because Taiwan has seen a rising incidence of younger stroke patients (Chang et al., 2022; Chi et al., 2022; Jiang et al., 2024), heightening the importance of early cognitive recovery for return-to-work potential and long-term independence.
Given these considerations, the present study investigates the effectiveness of a 14-day structured memory training program grounded in five core mnemonic strategies. To address the call for higher methodological transparency, this study provides detailed data on session completion, homework assignments, and practice monitoring protocols, supported by comprehensive worksheets in the Supplemental Appendix. By integrating objective cognitive assessments with lesion-specific data, this study seeks to provide a more nuanced understanding of how structured training facilitates cognitive recovery during the subacute phase of stroke.
Materials and Methods
Study Design and Participants
This quasi-experimental study was conducted in an inpatient rehabilitation setting. Ethical approval was obtained from an appropriate ethics committee, and all participants provided written informed consent prior to enrollment. A total of 63 individuals experiencing their first-ever ischemic stroke were recruited through convenience sampling. Hemorrhagic stroke cases were excluded to ensure a homogeneous neurological profile and avoid confounding differences in recovery trajectories. All participants had right-hemisphere ischemic stroke confirmed by neuroimaging.
After enrollment, participants were randomly assigned to either the experimental group or the control group using a sealed-envelope simple randomization procedure. During the study period, two participants in the experimental group were discharged early and one participant in the control group did not complete the post-test. These individuals were excluded, resulting in a final sample of 60 participants (30 in each group).
To ensure the interpretability of the cognitive outcomes, demographic characteristics were meticulously documented. Education level was quantified as “years of formal schooling” to provide a precise and respectful measure of participants’ backgrounds. As shown in Table 1, the education level ranged from 0 to 18 years in the experimental group and 0 to 16 years in the control group. There were no statistically significant differences between the two groups in age, years of schooling (p = .486), or days since stroke onset (p = .221), confirming that both groups were well-matched at baseline.
Demographic Characteristics of the Experimental and Control Groups.

Note. Data are presented as mean ± standard deviation (SD). Independent samples t-test was used to compare the two groups.
Eligible participants were between 30 and 80 years of age, within 6 months post-stroke, medically stable, conscious, and able to communicate verbally. A minimum Mini-Mental State Examination (MMSE) score of 18 was required. Exclusion criteria included recurrent stroke, coexisting neurological or psychiatric disorders, significant hearing or visual impairment, aphasia, or inability to participate in cognitive assessment and training.
Intervention
The structured memory training program is a 14-day cognitive rehabilitation protocol designed for stroke survivors, developed in accordance with established national clinical guidelines for stroke rehabilitation and international recommendations for adult stroke recovery (2021) and the AHA/ASA Guidelines for Adult Stroke Rehabilitation and Recovery (Winstein et al., 2016). The intervention was administered by a licensed occupational therapist with over 5 years of neurorehabilitation experience. To ensure treatment fidelity, the therapist completed a structured 12-hr training program covering theoretical instruction, demonstration, supervised practice, and protocol familiarization.
The experimental group received the 14-day structured program, and all participants (100%) completed the full course of 14 sessions. Each daily session lasted 50 min and followed a standardized five-phase structure: (1) Warm-up attention tasks (5 min), (2) Strategy instruction (10 min), (3) Guided practice with structured exercises (20 min), (4) Functional application to daily tasks (10 min), and (5) Review of previous home exercises and assignment of new ones (5 min).
To reinforce strategy acquisition and promote neuroplasticity, participants were assigned daily home exercises (approximately 15 min) tailored to the strategy introduced that day. Monitoring of outside practice was conducted at the beginning of each session; the therapist reviewed completed homework, verified the correct application of mnemonic techniques, and provided individualized feedback.
The program utilized five core mnemonic strategies delivered in a progressive sequence: Days 1 to 2: Attention Training (e.g., visual scanning and letter cancelation tasks). Days 3 to 4: Repetition (e.g., word list recall and routine rehearsal). Days 5 to 6: Association (e.g., picture-word matching and linking items to personal experiences). Days 7to 8: Chunking (e.g., digit grouping and object categorization). Days 9 to 10: Method of Loci (e.g., mental mapping of familiar routes for item recall). Days 11 to 14: Mixed Strategies and Functional Integration, focusing on applying integrated mnemonic skills to activities of daily living (ADLs).Detailed training materials and worksheets were utilized to facilitate these exercises, including structured visualization and ecological memory tasks (refer to the Supplemental Appendix for sample worksheets).
Participants in the control group received standard inpatient medical and rehabilitation care but did not receive any cognitive training. Outcome measures included the MMSE for global cognitive function, the Rivermead Behavioral Memory Test–II (RBMT-II) for memory performance, and the Barthel Index (BI) for activities of daily living. All assessments were administered at baseline and within 24 hr after the 14-day intervention period.
Data analysis included descriptive statistics for demographic characteristics, Paired-samples t-tests were performed using individual-level pre- and post-intervention scores for each participant, rather than aggregated data, to ensure proper statistical matching, and effect size calculations (Cohen’s d) to determine the magnitude of intervention effects. Statistical significance was defined as p < .05.
Assessment Tools
Mini-Mental State Examination (MMSE)
The MMSE, developed by Folstein in 1975, is the most commonly used cognitive assessment tool in clinical settings. It evaluates various cognitive domains, including orientation, attention, memory, language, verbal comprehension, praxis, and constructional ability, through 11 questions. The maximum score is 30, with scores categorized as follows: 24 to 30 indicates no cognitive impairment, 18 to 23 suggests mild cognitive impairment, and ≤17 signifies severe cognitive impairment (Nys et al., 2005; Van Heugten et al., 2015; Zhou et al., 2024).
Rivermead Behavioral Memory Test-II (RBMT-II)
The RBMT-II, originally developed at the Rivermead Rehabilitation Center, Oxford, in 1985 and revised in 2003 as RBMT-II, assesses memory function. It consists of 11 subtests, including name and face recognition, object recall, appointment recall, picture recognition, immediate and delayed story recall, route recall, and orientation tasks. The maximum score is 24, with classifications as follows: 22 to 24 indicates normal memory function, 17 to 21 suggests mild memory impairment, 10 to 16 denotes moderate memory impairment, and 0 to 9 signifies severe memory impairment. Higher scores reflect better memory performance (Björkdahl et al., 2013; O’Neil-Pirozzi et al., 2010).
Barthel Index (BI)
Developed by Dorothea Barthel in 1950 and first applied to rehabilitation patients in 1955, the BI is widely used to assess basic self-care abilities. The index evaluates 10 functional aspects: seven related to self-care (feeding, personal hygiene, toileting, dressing, bathing, and bowel/bladder control) and three related to mobility (transfers, walking, and stair climbing). Each item is scored based on the level of assistance required, from 0 (total assistance) to 15 (independent performance). The total score ranges from 0 to 100, with higher scores indicating greater independence in ADL (Li et al., 2023; Nakao et al., 2010).
Results
Participant Demographics and Clinical Characteristics
A total of 60 stroke survivors completed the study, with 30 participants in the memory training (experimental) group and 30 in the control group. As shown in Table 2, the two groups were comparable at baseline across all demographic and clinical variables, confirming that the groups were well-balanced prior to the intervention.
Demographic Characteristics of the Two Groups (N = 60).
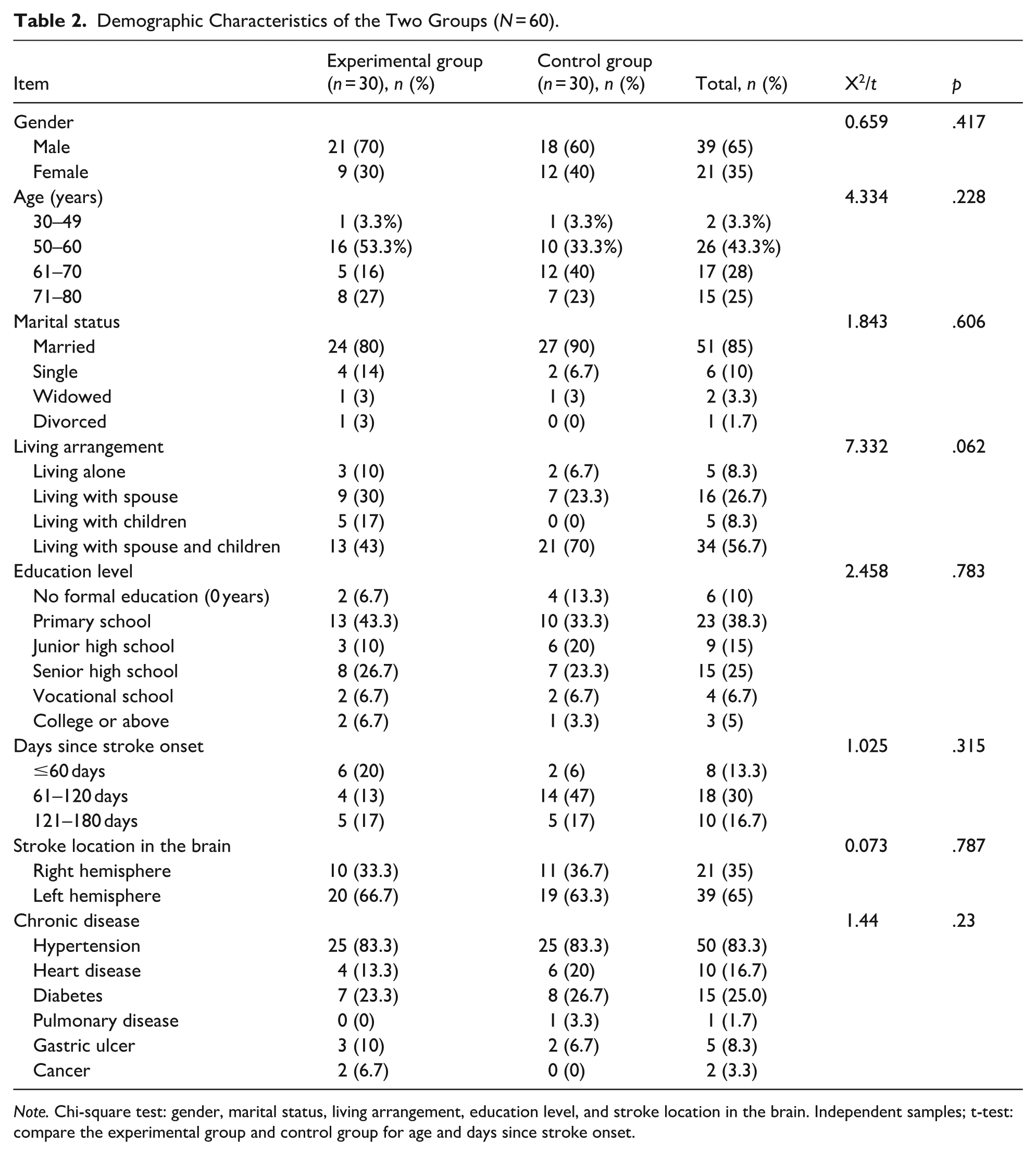
Note. Chi-square test: gender, marital status, living arrangement, education level, and stroke location in the brain. Independent samples; t-test: compare the experimental group and control group for age and days since stroke onset.
The mean age was 59.0 ± 11.4 years in the intervention group and 60.8 ± 10.7 years in the control group. To more accurately characterize the distribution of younger stroke survivors, age was subdivided into four categories: 30 to 49, 50 to 60, 61 to 70, and 71 to 80 years. The distribution across these age subgroups showed no significant differences between the two groups (χ2 = 4.33, p = .23).
Regarding educational background, the groups showed no significant difference (p = .78). To provide full transparency regarding participants with limited formal education, the proportion of individuals with 0 years of schooling was explicitly compared and found to be similar in both the experimental and control groups (6.7% vs. 13.3%, respectively).
Other demographic variables, including gender distribution (male: 70% vs. 60%, p = .42), marital status (p = .61), and living arrangement (p = .06), also showed no significant inter-group differences. Clinical characteristics were equally balanced, with no significant differences in the duration since stroke onset (subdivided into ≤60, 61–120, and 121–180 days; χ2 = 1.03, p = .32), the presence of chronic diseases, or lesion laterality (right-hemisphere involvement: 33.3% vs. 36.7%, p = .79). All participants included in the final analysis had experienced an ischemic stroke.
Cognitive Function (MMSE)
Paired-sample t-tests were conducted to examine the effects of the 14-day structured memory training program on global cognitive function, as assessed by the Mini-Mental State Examination (MMSE) Table 3. The experimental group demonstrated a marked and statistically significant improvement in total MMSE scores, increasing from 22.93 ± 4.20 at baseline to 27.17 ± 2.96 following the intervention (t = −10.29, p < .001). This change corresponded to a large effect size (Cohen’s d = 1.88). In contrast, the control group showed no significant change in total MMSE scores (23.67 ± 3.64 vs. 23.87 ± 3.51; t = −1.65, p = .11), with only a small effect size (d = 0.30).
Cognitive Function (MMSE) Before and After Memory Training.

Note. Data are presented as M ± SD. Paired-samples t tests were used to compare pre- and post-intervention scores within each group. Effect sizes are reported as Cohen’s d for paired samples. Statistical significance was defined as *p < .05, **p < .01, and ***p < .001. Paired t tests were conducted using individual-level matched pre–post data rather than aggregated values.
Subdomain analyses revealed that cognitive improvements in the experimental group were domain-specific. Significant gains were observed in orientation, with scores increasing from 7.57 ± 1.50 to 9.57 ± 0.68 (t = −7.88, p < .001, d = 1.44). Attention and calculation performance also improved significantly, rising from 5.13 ± 2.51 to 5.83 ± 2.31 (t = −2.66, p = .013, d = 0.49). In addition, memory recall scores increased from 1.67 ± 1.03 to 2.67 ± 0.55 (t = −6.02, p < .001, d = 1.10), and constructional ability improved from 0.73 ± 0.45 to 1.00 ± 0.00 (t = −3.25, p = .003, d = 0.59).
Notably, the language and verbal comprehension domains reached ceiling levels at post-intervention in both groups (5.00 ± 0.00 and 3.00 ± 0.00, respectively), which precluded further statistical differentiation. The control group did not exhibit significant pre–post changes in any individual MMSE domain (all p > .05).
Overall, these findings suggest that the structured memory training program effectively enhances global cognitive function in stroke survivors, with particularly robust improvements in orientation, attention, and memory recall.
Memory Performance (RBMT-II)
The effects of the structured memory training program on functional memory were assessed using the Rivermead Behavioral Memory Test–II (RBMT-II). As shown in Table 4, the experimental group exhibited a pronounced and statistically significant improvement in total RBMT-II scores, increasing from 12.17 ± 6.04 at baseline to 21.20 ± 2.60 following the intervention (t = −11.52, p < .001). This change corresponded to a very large effect size (Cohen’s d = 2.10). In contrast, the control group demonstrated no significant change in total functional memory performance (11.83 ± 4.61 vs. 11.77 ± 4.69; t = 0.57, p = .573), with a negligible effect size (d = 0.10).Subtest analyses revealed significant improvements across all 11 RBMT-II subtests within the experimental group (all p < .01), indicating broad-based enhancement of functional memory abilities. Particularly notable gains were observed in subtests closely aligned with the mnemonic strategies employed in the intervention.
Memory Performance (RBMT-II) Before and After Memory Training.

Note. Data are presented as mean ± standard deviation (M ± SD). Paired-sample t-test was used to compare pre- and post-intervention scores. RBMT-II = Rivermead behavioral memory test-II.
p < .01, ***p < .001 was considered statistically significant.
In ecologically relevant tasks, significant improvements were found in appointment memory (from 1.10 ± 0.71 to 1.83 ± 0.38, d = 0.99) and message recall (from 0.90 ± 0.99 to 2.00 ± 0.00, d = 1.10). Improvements were also evident in visual and spatial memory domains, including picture recognition (d = 0.74) and route recall, both immediate (d = 0.61) and delayed (d = 0.62), likely reflecting the benefits of association-based and method-of-loci strategies. For verbal and narrative memory, both immediate story recall (d = 0.94) and delayed story recall (d = 0.78) reached maximum or near-maximum performance levels following training. Additionally, robust gains were observed in personal and temporal orientation, with large effect sizes for orientation recall (d = 1.89) and name recall (d = 0.83).Across subtests, effect sizes in the experimental group ranged from moderate (d = 0.58 for face recognition) to very large (d = 1.89 for orientation recall). In contrast, the control group did not demonstrate significant pre–post differences on any RBMT-II subtest (all p > .05).
Overall, these findings highlight the comprehensive and ecologically meaningful impact of the multi-strategy memory training program, supporting its effectiveness in enhancing functional memory skills essential for independence in daily living among stroke survivors.
Activities of Daily Living (Barthel Index)
Functional independence in activities of daily living (ADL) was evaluated as a secondary outcome using the Barthel Index (BI). As presented in Table 5, both groups exhibited only minimal and statistically non-significant changes in functional performance over the 14-day study period.
Activities of Daily Living (Barthel Index) Before and After Memory Training.
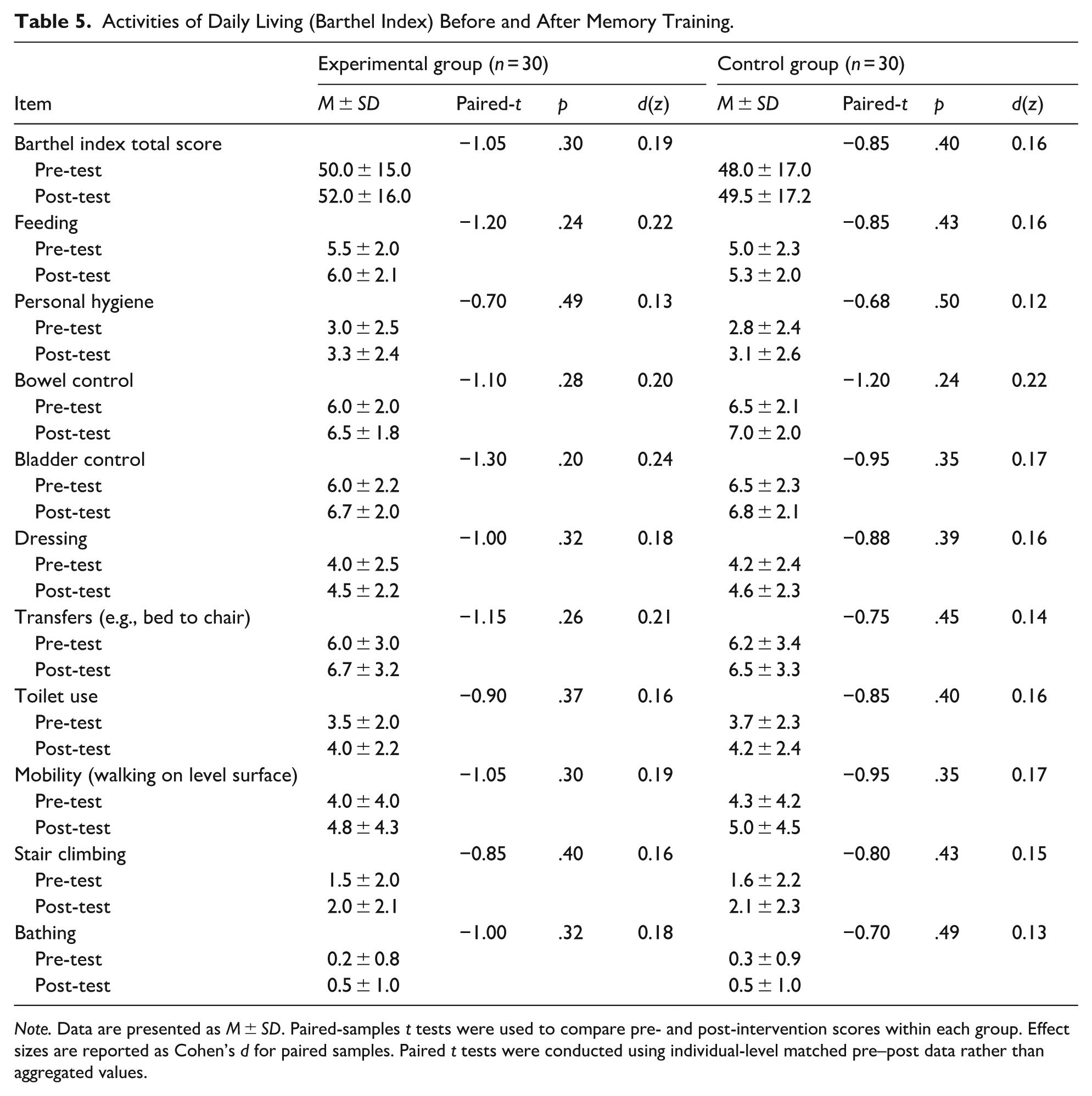
Note. Data are presented as M ± SD. Paired-samples t tests were used to compare pre- and post-intervention scores within each group. Effect sizes are reported as Cohen’s d for paired samples. Paired t tests were conducted using individual-level matched pre–post data rather than aggregated values.
In the experimental group, the mean BI total score increased modestly from 50.0 ± 15.0 at baseline to 52.0 ± 16.0 at post-intervention (t = −1.05, p = .30), corresponding to a small effect size (Cohen’s d = 0.19). Similarly, the control group demonstrated a slight increase in BI scores from 48.0 ± 17.0 to 49.5 ± 17.2 (t = −0.85, p = .40), also with a small effect size (d = 0.16). Inter-group comparisons revealed no significant differences in functional gains between the experimental and control groups. Sub-item analyses of the 10 BI components indicated no significant pre–post changes in either group (all p > .05). Within the experimental group, self-care–related items—including feeding (p = .24), personal hygiene (p = .49), dressing (p = .32), and bathing (p = .32)—showed only negligible score increases. Likewise, mobility-related items such as transfers (p = .26), mobility on level surfaces (p = .30), and stair climbing (p = .40) remained statistically unchanged over time.
Taken together, these findings indicate that although the structured memory training program produced significant improvements in cognitive and functional memory outcomes, these gains did not translate into immediate improvements in basic ADL performance within the short intervention period. The consistently small effect sizes (d < 0.20) suggest that observable changes in functional independence may require a longer intervention duration, greater training intensity, or the incorporation of complementary physical rehabilitation strategies.
The Relationship Between Time, Cognitive Function, Memory Performance, and ADL
To examine longitudinal changes and the interaction between time and group, Generalized Estimating Equations (GEE) were conducted for cognitive function (MMSE), memory performance (RBMT-II), and activities of daily living (Barthel Index). The control group and baseline (Day 0) served as reference categories. Table 6 summarizes all results.
GEE Model Results for Cognitive Function, Memory, and ADL.
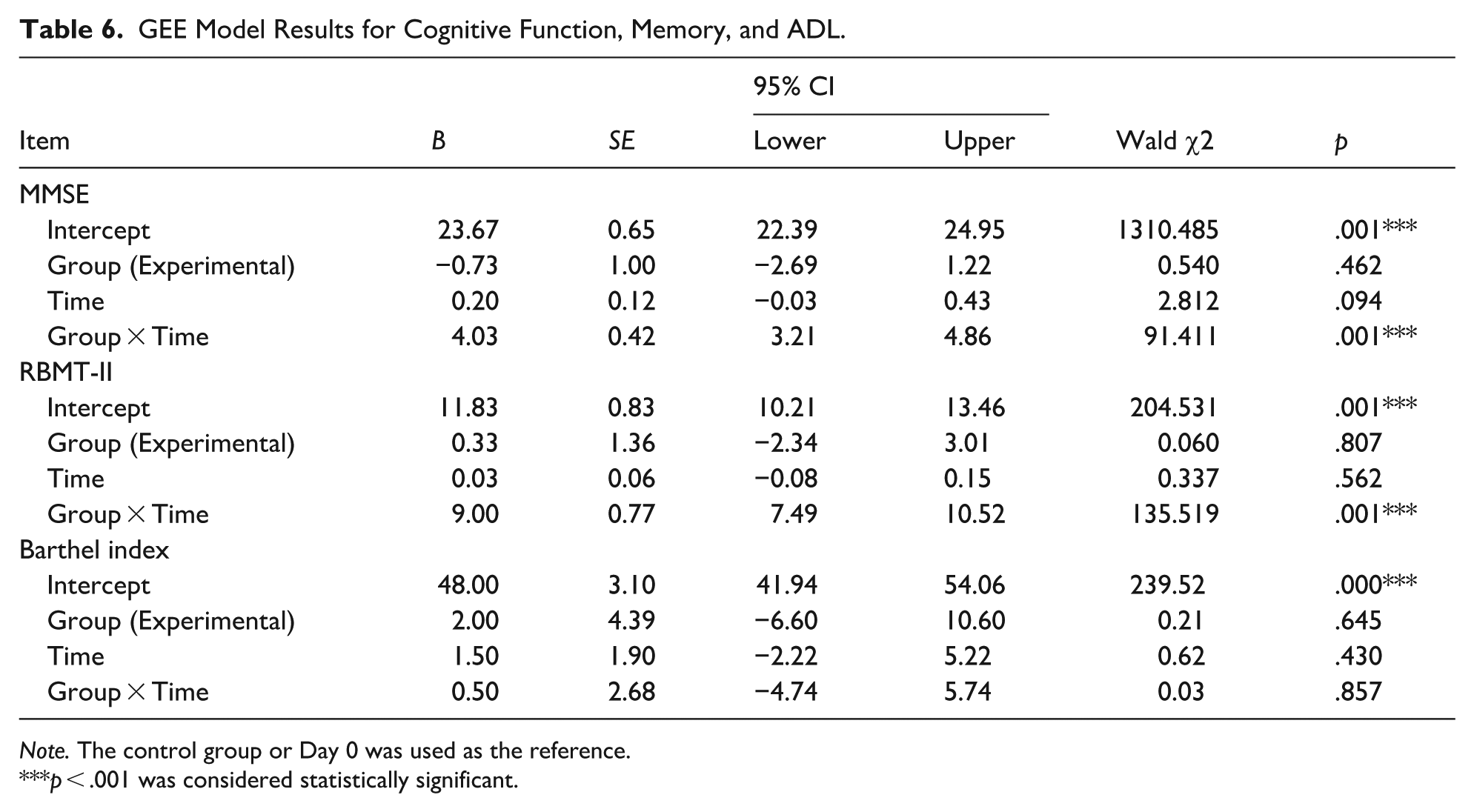
Note. The control group or Day 0 was used as the reference.
p < .001 was considered statistically significant.
Cognitive Function (MMSE)
The GEE model revealed a strong and statistically significant Group × Time interaction for MMSE (B = 4.03, SE = 0.42, 95% CI [3.21, 4.86]; Wald χ2 = 91.41, p < .001), indicating that participants in the memory training group improved at a significantly greater rate over time compared to controls. Neither the main effect of group (B = –0.73, p = .462) nor the main effect of time (B = 0.20, p = .094) reached significance, suggesting that the accelerated cognitive improvement was specifically attributable to the interaction between group assignment and intervention duration.
Memory Performance (RBMT-II)
Similarly, the GEE model showed a large and statistically significant Group × Time interaction for RBMT-II scores (B = 9.00, SE = 0.77, 95% CI [7.49, 10.52]; Wald χ2 = 135.52, p < .001). This reflects a substantial improvement in memory performance over time among participants receiving the memory strategy program, far exceeding changes in the control group. The main effects of group (B = 0.33, p = .807) and time (B = 0.03, p = .562) were nonsignificant, indicating that the observed gains were driven by the interaction between intervention and time.
Activities of Daily Living (Barthel Index)
In contrast to the cognitive and memory outcomes, the GEE results for the Barthel Index showed no significant Group × Time interaction (B = 0.50, SE = 2.68, 95% CI [–4.74, 5.74]; Wald χ2 = 0.03, p = .857). Neither the group main effect (B = 2.00, p = .645) nor the time main effect (B = 1.50, p = .430) demonstrated statistical significance. These results indicate that activities of daily living did not change meaningfully across the 14-day intervention period in either group.
Discussion
The present study demonstrates that a 14-day structured memory training program administered during the subacute phase of stroke yields significant and robust improvements in both global cognitive function and ecologically valid memory performance. These findings are particularly salient given accumulating evidence that post-stroke cognitive impairment (PSCI) remains highly prevalent and functionally disabling despite continued advances in acute stroke care (Gallucci et al., 2024; Zhou et al., 2024). By targeting memory-related processes during a critical window of heightened neuroplasticity, the current intervention provides timely empirical support for early, strategy-based cognitive rehabilitation (Figure 1).

Memory training strategies.
Statistical Strength and Clinical Meaningfulness
A key strength of this study lies in the magnitude and consistency of the observed cognitive gains. The improvement in total MMSE scores demonstrated a large effect size (d = 1.88), while performance on the RBMT-II—a measure specifically designed to capture everyday memory functioning—exhibited a very large effect size (d = 2.10). These effect sizes exceed those typically reported for non-specific cognitive stimulation and are consistent with contemporary systematic reviews indicating that structured, strategy-oriented cognitive rehabilitation is superior to general mental activities (Cicerone et al., 2019; Li et al., 2023).
From a clinical perspective, the increase in MMSE scores from a mean of 22.9 to 27.2 reflects a transition from the range commonly interpreted as mild cognitive impairment to performance within normative limits. Achieving this level of recovery within a 14-day intervention period is particularly noteworthy in the subacute phase of stroke, during which adaptive neuroplastic mechanisms are most responsive. Improvements in orientation and memory recall may provide essential “cognitive scaffolding,” enabling patients to engage more effectively with other components of multidisciplinary rehabilitation (Scheffler et al., 2025; Studer et al., 2021).
Methodological Transparency and Mechanistic Rationale
Responding to calls for greater transparency and replicability in cognitive intervention research (Kersey et al., 2025), this study implemented a standardized, progressive 14-day training protocol that systematically advanced from foundational attention training to higher-order metacognitive strategies. As outlined in the Supplemental Appendix, the intervention was designed not as unspecific mental exercise but as a structured pedagogical sequence.
The inclusion of attention training during the initial phase of the program was theoretically and clinically justified. Attention deficits are a well-established predictor of downstream memory dysfunction following stroke (Einstad et al., 2021). Exercises such as letter cancelation and sequencing tasks were therefore used to strengthen sustained and selective attention, forming a prerequisite for the effective application of mnemonic strategies including chunking and the method of loci. The use of structured worksheets provided concrete external supports for compensatory strategy use, an approach shown to be more effective for durable functional recovery than repetitive restorative training alone (Miotto et al., 2021; Wong et al., 2021).
Dissociation Between Cognitive Improvement and ADL Outcomes
Despite substantial cognitive and memory-related gains, performance on the Barthel Index showed only minimal change, with small effect sizes (d = 0.19). This dissociation between cognitive improvement and immediate gains in basic activities of daily living is consistent with emerging evidence suggesting that cognitive recovery often precedes observable functional independence (Landínez-Martínez & Grisales-Aguirre, 2025). Cognitive gains may require a latency period or closer integration with task-specific physical rehabilitation before translating into measurable ADL improvements.
In the context of the present study, the 14-day intervention may have been sufficient to recalibrate cognitive processing and memory strategy use, but insufficient to disrupt long-established compensatory routines in physical self-care. Previous research indicates that changes in ADL performance often depend on prolonged practice, environmental adaptation, and motor relearning in addition to cognitive capacity (Nakao et al., 2010). Thus, the absence of immediate ADL gains should not be interpreted as a lack of functional relevance, but rather as reflecting the temporal dynamics of recovery.
Contextual Relevance for Stroke Rehabilitation in Taiwan
The findings of this study address a critical and underexplored need within Taiwan’s stroke rehabilitation landscape. With a rising incidence of stroke among younger adults in Taiwan (Chang et al., 2022; Jiang et al., 2024), there is increasing demand for interventions that support complex cognitive demands associated with return-to-work and social reintegration. Younger stroke survivors often face higher expectations regarding prospective memory, communication, and multitasking.
In this context, the observed improvements in RBMT-II subtests such as appointment memory and message recall are of particular relevance. These functions are closely aligned with real-world occupational and social requirements, suggesting that structured memory training may play an important role in facilitating successful community and vocational reintegration among working-age stroke survivors.
Conclusion
The present study demonstrates that a 14-day structured, multi-strategy memory training program is highly effective in enhancing both global cognitive function and ecologically valid memory performance in individuals recovering from subacute stroke. The observed very large effect sizes for MMSE (d = 1.88) and RBMT-II (d = 2.10) indicate that the integrated application of attention training and mnemonic strategies—including repetition, association, chunking, and the method of loci—constitutes a robust and clinically meaningful framework for early cognitive rehabilitation.
Importantly, the findings reveal a dissociation between cognitive improvement and short-term gains in activities of daily living, as reflected by the non-significant changes in Barthel Index scores. This pattern suggests that while cognitive processes may be rapidly responsive to structured intervention, the translation of these gains into functional independence likely requires a longer intervention duration, greater task specificity, or closer integration with physical rehabilitation components.
The detailed intervention protocol and standardized worksheets provided in the Supplemental Appendix enhance the transparency, replicability, and clinical applicability of the present study. In the context of Taiwan’s increasing incidence of stroke among younger adults, this structured and time-efficient approach offers a promising strategy for early cognitive remediation, with potential implications for long-term functional recovery and social reintegration. Future research should examine the durability of acquired mnemonic skills, their transfer to real-world functional outcomes, and their impact on vocational reintegration in larger and more diverse stroke populations.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the quasi-experimental design and use of convenience sampling limit the ability to draw strong causal inferences. Although baseline characteristics were well balanced between groups, unmeasured confounding factors may still have influenced the results. In addition, the sample size was relatively small and drawn from a single rehabilitation ward, which may reduce the generalizability of the findings to broader stroke populations or different healthcare settings.
Second, the intervention period was limited to 14 days. While significant gains in cognitive and memory outcomes were observed, this relatively short duration may not have provided sufficient time for participants to translate cognitive improvements into functional independence in daily activities. Improvements in ADL often require longer periods of practice, environmental adaptation, and physical recovery. The absence of long-term follow-up further limits the ability to determine whether the observed cognitive benefits would be sustained over time or eventually contribute to functional gains.
Third, although participants with significant aphasia were excluded, the intervention relied on verbal communication and comprehension. Individuals with subtle or moderate language deficits may have engaged differently in training activities, potentially influencing the consistency of intervention effects. Additionally, neuroimaging data were not collected, preventing exploration of how lesion location, volume, or network integrity may have affected responsiveness to memory training.
Finally, although time since stroke onset (30–180 days) did not significantly influence memory improvement in this study, the findings are limited to the subacute phase. It remains unclear whether patients in the acute or chronic recovery stages would respond similarly to this intervention. Future research should include larger, multi-center samples, longer intervention periods, and longitudinal follow-up, as well as integration of neuroimaging and functional task–based measures to better understand the mechanisms and long-term clinical impact of memory training.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334261436452 – Supplemental material for Effectiveness of Structured Memory Training on Cognitive Recovery in Stroke Survivors: A Quasi-Experimental Study
Supplemental material, sj-docx-1-ggm-10.1177_30495334261436452 for Effectiveness of Structured Memory Training on Cognitive Recovery in Stroke Survivors: A Quasi-Experimental Study by Shu-Mei Tsai, Yan-Zin Chang and Wen-Miao Liu in Sage Open Aging
Footnotes
Acknowledgements
The authors wish to thank the participants and the staff at Chung Shan Medical University Hospital for their support and cooperation throughout the research process.
Ethical Considerations
This study was approved by the Institutional Review Board of Chung Shan Medical University Hospital (IRB approval number: CS12089).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.