
Abstract
An older adult affordable housing community and a Federally Qualified Health Center partnered to improve the health of low-income older adults. The Unite Care Model included establishing onsite primary care, wellness support, and social needs assistance. The RE-AIM framework guided our mixed-methods evaluation. We sought to determine whether the model was associated with change in blood pressure, social or physical environment and understand model reach and implementation. Of the 251 residents, 13.1% had a clinic visit, and of respondents 70% attended at least one wellness event, and 35% received social needs assistance (reach). Clinic utilization was not associated with improved blood pressure or environment change (effectiveness). Residents reported barriers to clinic utilization including an established provider, uncertainty in transferring care, lack of urgent visits, and insurance barriers. Administrators echoed policy, staffing, and patient barriers to utilization (implementation). Expanding appointment options, increasing staffing, and overcoming insurance barriers may increase effectiveness.
Introduction
The US is aging and racially diversifying (Mather et al., 2015). Poverty is associated with poorer health and increased mortality. Older Americans in the top income group live over 10 years longer than their counterparts in the lowest income group (Chetty et al., 2016). Improving the health and well-being of low-income older adults, who are more likely to be from historically disadvantaged racial and ethnic groups, requires innovative approaches (Fulmer et al., 2021).
Differences in chronic diseases, such as hypertension, along with behavioral risk factors, such as physical activity and smoking, are mediators of health (Chetty et al., 2016; Dwyer-Lindgren et al., 2017; V. J. Howard et al., 2011; G. Howard et al., 2017; Mensah et al., 2005; Wong et al., 2002). High blood pressure (BP) is the strongest predictor of stroke and coronary heart disease and is an important risk factor for dementia, atrial fibrillation, heart failure, and chronic kidney disease (Fuchs & Whelton, 2020). High BP is managed by—and healthy behaviors are promoted via—primary care. Given that older adults with low income have less access to primary care than their counterparts (Cunningham et al., 2017), improving access to primary care among these Americans may improve the health of older adults (Dwyer-Lindgren et al., 2017; Healthy People 2020: Access to Health Services, 2019).
In response to the community-identified priorities related to housing and healthcare, housing and healthcare partners collaborated over a 2-year planning process to design and establish the Unite Care Model. As part of the care model, collaborators established a Federally Qualified Health Center (FQHC) clinic co-located within an older adult affordable housing community. The goal of the project, Unite, was to flip the paradigm that asks the most vulnerable older adults to seek out the medical safety net. Instead, the healthcare safety net is being brought to older adults.
FQHCs are federally funded, non-profit clinics designed to provide care to medically underserved populations, delivering primary care to 30 million Americans, many of whom experience significant social risks. Care is provided on a sliding scale fee (Nguyen et al., 2024). FQHCs are often trusted pillars of care in their communities and are at the forefront of health equity (Lalika et al., 2024).
Studies have shown that onsite clinics increased engagement with primary care among tenants residing in permanent supportive housing (McCall et al., 2021; Redline et al., 2025). Additional studies have explored the impact of home health services on health outcomes. Older adults with traditional Medicare received more home health care and had better functional outcomes (self-care and mobility) than those with Medicare Advantage plans, suggesting that home health may improve functional outcomes (Prusynski et al., 2024). Finally, Community Aging in Place-Advancing Better Living for Elders (CAPABLE) was a randomized trial of home occupational therapy and nursing sessions and home repairs to reduce disability and promote aging in place through physical environmental optimization. The CAPABLE intervention resulted in a 30% decrease in disability compared to controls at 5 months, although the improvement was not sustained at 1 year (Aliberti & Covinsky, 2019; Szanton et al., 2019). The authors suggest that continued support through booster visits, social service screening, and community health worker support may improve sustainability. Overall, components of integrated care models involving healthcare and housing-based services have demonstrated promise; however, few studies have directly embedded an FQHC clinic within an older adult housing complex to provide longitudinal, on-site primary care and supportive services over time.
A barrier in cross-sector collaboration is that investment in one sector often accrues benefits in another sector, while increasing costs and resource utilization in the investing sector (Artiga & Hinton, 2018; Brown et al., 2019; Gottlieb et al., 2017). In most cross-sector collaborations, healthcare initiates and funds the collaboration (Fichtenberg et al., 2020).The Unite Care Model sought to overcome this barrier. Grant funding financially supported the construction of the co-located clinic. The healthcare organization and housing facility maintained separate staff and finances.
We present findings from an initial evaluation of the Unite Care Model, a community-led, cross-sector collaboration between an older adult affordable housing community and an FQHC. We hypothesize that establishing a primary care clinic removes the transportation barrier to accessing care, which could directly improve health and well-being and indirectly benefit the community by fostering a culture of health. Utilizing the RE-AIM evaluation framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance), focusing on reach, effectiveness, and implementation, we evaluated the Unite Care Model at both the individual and organizational levels. Specifically, we sought to determine whether the Unite Care Model was associated with a change in BP, social environment, or physical environment, and to understand the utilization and implementation of the Unite Care Model. We hypothesized that with adequate reach and implementation, the Unite Care Model would decrease BP, enhance the social environment, and increase home modifications.
Methods
This was a mixed-methods evaluation grounded in the RE-AIM framework. We assessed the Unite Care Model’s Reach, Effectiveness, and Implementation (Glasgow et al., 1999, 2003, 2019).
The Unite Care Model
The Unite Care Model was conceptualized as: (1) the Unite primary care clinic in the housing community that would provide scheduled, urgent, and home visits; (2) health and wellness supportive services led by a wellness coordinator; and (3) assistance with health-related social needs facilitated by a community health worker (CHW). The housing partner was an older adult, affordable, independent housing community (housing community) home to 251 adults ages 55 and older, most of whom self-identify as Black. The healthcare partner was the largest FQHC network in Flint, Michigan. The Unite Care Model was initiated in July 2021 with the opening of the primary care clinic, about 6 months after COVID-19 vaccines were available. It was staffed by a medical assistant and a nurse practitioner who were available 5 days a week. The clinic was available by appointment to older adult community members who did not reside at the housing facility. Non-resident clinic users did not have access to housing-sponsored health and wellness services nor CHW assistance and therefore were not intended recipients of the Unite Care Model. Wellness coordinator support and CHW assistance predated Unite as full-time positions with the housing partner. The Unite protocol has been published (L. Skolarus et al., 2023).
Study Populations
Our evaluation included four study populations: (1) Unite Clinic patients to assess clinic reach; (2) Residents of the housing community to assess utilization and effectiveness of the Unite Care Model (Figure 1); (3) a purposively selected subset of the resident cohort, stratified by clinic utilization (users, attempted or did not use) who completed semi-structured interviews to understand Unite implementation; (4) administrators from the housing and healthcare organizations who completed semi-structured interviews to characterize organizational-level implementation.
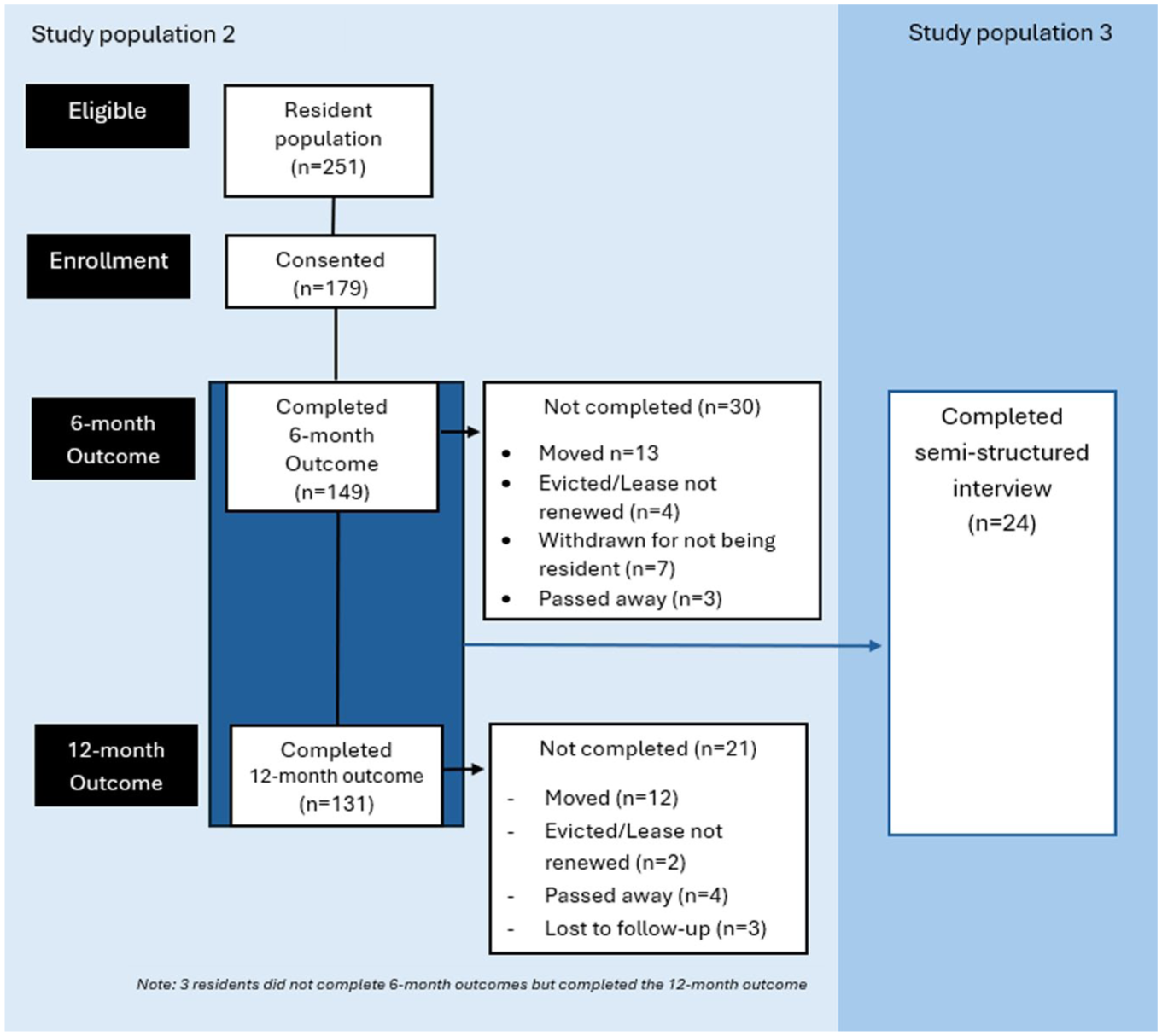
Participant flow diagram of study populations 2 and 3: residents of older adult affordable housing community.
Unite clinic patients were identified from the FQHC electronic medical record (EMR) and geocoded by housing community residence (resident vs. non-resident) for visits occurring between July 2021 and December 2022. The housing community residents (Study population 2) were enrolled from June to October 2021. In addition to researcher-led recruitment, housing staff introduced the study and encouraged resident participation; fliers were distributed, and selective door-to-door knocking was instituted near the end of the recruitment period. The housing staff aided the research team in contacting hard-to-reach residents. Recruitment concluded after all residents had been contacted and provided the opportunity to consent or decline to participate in the study. Eligibility included adults without hearing or speech impairment who spoke English (<1% of the community does not speak English). Data was collected at baseline, 6- and 12-months via in-person structured assessments. To characterize residents, we measured resident cognition (Callahan et al., 2002), activity limitations (Katz, 1963; Lawton & Brody, 1969), health-related social needs including the four core domains (food, housing, transportation, and utilities; Billioux et al., 2017; Health Leads, 2018), cost-related medication nonadherence (Levine et al., 2013), and financial strain (Centers for Medicare & Medicaid Services et al., 2021). Participants received $20 at baseline and $25 for each outcome assessment.
Interviews with purposively selected residents were conducted from August 2022 to February 2023 (Study population 3). Participants were sampled across three categories: residents who reported using the clinic (clinic users), residents who reported not using the clinic (non-users), and residents who reported attempting to utilize the clinic but did not receive care (attempted users). Attempted users were defined as residents who faced clinic-related barriers to access (insurance, appointment availability) and residents who sought out the clinic but ultimately decided not to utilize it. Interviews were grounded in the Theoretical Domains Framework (TDF) and Proctor’s definition of acceptability (Atkins et al., 2017; Proctor et al., 2011). Interviews explored constructs including beliefs/expectancies, intentions, social norms, affect, and incentives regarding the housing environment and co-located clinic. Recruitment continued until thematic saturation was achieved, defined as no new themes emerging in additional interviews. All resident interviews were conducted in-person, audio recorded and transcribed for analysis. Participants received $40 for completing the interview.
Lastly, we purposively sampled key housing and healthcare personnel and used snowball sampling to recruit additional staff identified as involved in clinic operations. Interviews were conducted from December 2022 to March 2023, 18 to 21 months from the clinic opening. Interviews with housing and healthcare personnel were conducted via Zoom, telephone, or in-person depending on availability and participant preference. Interviews were grounded in the TDF and Tailored Implementation in Chronic Diseases (TICD) Framework, assessing intervention coherence, affective attitude, opportunity costs, perceived effectiveness, and capacity for organizational change (Flottorp et al., 2013). Interviews were audio recorded and transcribed for analysis. Participants received $40 for completing the interview.
Measures
Reach Measures
Our primary measure of reach was the proportion of individuals receiving care at the Unite clinic who were housing residents, as documented in the clinic EMR. Clinic utilization metrics, total visits, new patient appointments, return visits, and missed appointments, were also derived from the clinic EMR. Secondary measures of reach were evaluated in the resident cohort and included self-reported use of the clinic, participation in health and social programing, interactions with the CHW, and use of the food pantry.
Effectiveness Measures
The primary effectiveness outcome was the change in systolic blood pressure (SBP) from baseline to 12 months among residents. BP was measured by research staff using the OMRON 7 Series Upper Arm BP Monitor in accordance with national standards for measurement (Pickering et al., 2005). Secondary effectiveness outcomes included counts of physical and social environment modification. Physical environment was assessed via common home hazards checklists (range 0–10; Szanton et al., 2015; CDC, 2017). Higher total counts indicated more home hazards. Social environment was measured using the social isolation scale (range 0–30; Nicholson et al., 2020). Lower counts indicate greater social isolation (Supplemental Table 1).
Implementation Measures
We measured implementation at the setting level, focusing on the extent to which housing and healthcare staff delivered the Unite Care Model components as intended. Data was obtained through housing and healthcare logs, direct observations, and semi-structured interviews with housing and healthcare personnel and residents. The primary implementation measures were the services provided by the clinic, the proportion of weekdays where a social or health/physical activity event occurred, and the number of interactions with a CHW for assistance with health-related social needs. Additional implementation measures included the duration of gaps in the employment of the wellness coordinator or CHW and the persistence of wellness checks (defined as housing staff entering the resident’s apartment) during the study period.
Sample Size and Quantitative Statistical Analyses
For the primary effectiveness analysis, we estimated we needed 240 participants to have 85% power to detect a 2-point change in SBP within older adults assuming a mean baseline SBP of 162 mmHg and Standard Deviation of 10 mmHg. This relatively high baseline BP reflects preliminary data from the Flint community rather than national averages (L. E. Skolarus et al., 2018; Victor et al., 2018).
To evaluate the Unite Care Model reach, we first compared the patient characteristics and clinic utilization between individuals residing in the housing community and those living outside the community. We then used descriptive statistics to characterize residents and their self-reported Unite Care Model utilization. To identify factors associated with Unite clinic use among residents, we fit logistic regression models examining whether demographics, cognitive impairment, activity limitations, hypertension diagnosis, and transportation needs were associated with self-reported clinic utilization.
To explore the effectiveness of the Unite Care Model, we compared change in BP (primary effectiveness outcome), physical environment, and social environment between residents who did and did not utilize the Unite clinic (Study Population 2). We used linear regression to model 12-month SBP as the outcome variable, adjusting for baseline SBP and a binary indicator of Unite clinic utilization within 12 months. We also fit Poisson regression models for physical environment modifications and social environment, adjusting for baseline values and Unite clinic utilization status. Multiple imputation was used to account for missing data. Imputation models included all analysis variables and characteristics we hypothesized to be associated with outcomes including baseline values, age, sex, race/ethnicity, prior history of hypertension, medication affordability, cognitive status, activity limitations, cognitive limitations, and 6-month BP (for BP models only). To assess the potential impact of missing outcome data, we conducted sensitivity analyses restricted to participants with complete outcome data. Statistical significance was set at p < .05, and all p values were two-tailed. Analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC) and STATA 17 (Stata Corporation LLC, College Station, USA). This study was approved by the University of Michigan Institutional Review Board.
Qualitative Analysis
We conducted a qualitative analysis using a deductive coding approach. We applied the TDF as the initial codes. A qualitative codebook was created that defined the application of each code. Qualitative analysis software, ATLAS.ti Qualitative Data Analysis software (Atlas.ti Scientific Software Development GmbH) was used to organize and review coded data. Two researchers double-coded 20% of transcripts, discussing discrepancies until a consensus was reached. The remaining transcripts were divided between researchers to complete. Queries of the codes were exported in Microsoft Excel documents and reconciled. After coding, we synthesized the findings by mapping the TDF domains to the Capability, Opportunity, and Motivation (COM-B) Model. This cross-walking allowed us to understand how behavioral determinants impacted the uptake of the Unite Care Model.
Results
Reach
Overall, 617 appointments were scheduled at the Unite clinic (completed or missed) during the first 18 months. These appointments were scheduled by 217 people, and 188 people (86.6%) completed at least one visit (Study Population 1). Of the 251 residents, 33 (13.1%) completed at least one Unite clinic visit. Among clinic users, residents were older on average (67.2 vs. 41.9, p < .01) and more likely to be Medicare recipients (60.6% vs. 12.0%, p < .01, Supplemental Table 2) than people living outside the housing community. Compared with non-residents, housing community residents completed a slightly higher mean number of visits (3.7 vs. 2.2, p = .055). There was no statistically significant difference in the proportion of missed appointments between groups (51.5% vs. 46.7%, p = .61).
Of the 251 older adults who resided in the housing community, 179 (71.3%) enrolled in the study and 131 (52%) completed the 12-month outcome (Figure 1). Thus, 29% did not enroll and 48% did not complete the 12-month outcome. The baseline characteristics are shown in Table 1. About 26.8% (48/179) self-reported a Unite clinic visit (this is higher than the EMR data, Study Population 1, as likely respondents may have reported attending clinic information sessions as clinic visits). There were no significant differences in sociodemographic characteristics, comorbidities, or disability between residents who utilized the clinic and residents who did not. Residents who used the clinic were more likely to have transportation needs than those who did not (22.9% vs. 9.9%, p = .02, adjusted OR = 2.8, 95% CI: [1.1, 7.4], p = .02, Table 2).
Characteristics of Older Adult Participants Residing in the Unite Housing Community (N = 179 Respondents to Study).

Other includes participants who identified as American Indian, Alaska Native, or did not specify.
Participant Characteristics Associated with Unite Clinic Utilization.

In total, 70.4% of respondents attended at least 1 social or health event, with health and physical activity being the most frequently attended. 34.9% of respondents reported working with the CHW to address social needs. The most common services received were assistance with government benefits (41.5%), bills (35.9%), counseling or support (24.5%), or health advocacy (22.6%). In addition, 73.0% of respondents reported utilizing the food pantry, and 20.6% reported getting to know the students residing on the housing campus.
Effectiveness
On average, SBP (baseline: 133.1 vs. 12-month: 135.6, p = .87), physical environment modifications (baseline: 2.0 vs. 12-month: 2.0, p = .58), and social environment (baseline: 22.3 vs. 12-month: 23.5, p = .99) did not change during the study. There were no statistically significant associations between Unite clinic utilization and change in SBP (PE = −2.3 (95% CI: [−9.9, 5.3], p = .54)), physical environment (IRR = 1.2 (95% CI: [0.9, 1.5], p = .29)), or social environmental (IRR = 1.0 (95% CI: [0.9, 1.1], p = .61, Table 3). The results of sensitivity analyses using completed cases were similar to the primary analyses (Supplemental Tables 3–6).
Association of Unite Clinic Utilization with Systolic Blood Pressure and Physical and Social Environments at 12 Months. a

Missing outcomes imputed.
Parameter estimate.
Adjusted incidence rate ratio.
Unite Model Implementation
Care at the clinic was limited to scheduled, in-person visits and did not include home, urgent, or remote visits, as originally conceptualized. The wellness coordinator hosted social events (64.2%) or health/physical activity events (34.0%) of weekdays. A CHW was present at the start of the Unite Care Model but subsequently left the role, resulting in a 6-month gap before the position was filled. Overall, when in place, the CHW averaged four resident interactions per day. During the study period, 23 wellness checks were recorded. Most were initiated by the resident receiving the wellness check (47.8%), followed by family members of the residents (21.7%) and another resident (17.4%). The most common reasons for wellness checks were residents not in contact with their social network (56.5%) and physical health concerns (21.7%). A total of 17.4% of wellness checks resulted in the residents being taken to the emergency room, and 30.4% involved continued assistance from CHW or housing administration.
Unite Model Implementation—Clinic and Housing Personnel
Eight housing and healthcare personnel completed interviews (50% (n = 4) housing, 50% (n = 4) healthcare). Clinic leaders noted that use of the clinic by housing residents was slower than anticipated, serving about one-half to two-thirds of their daily patient target, “[. . .] once we get into that 12 to 15 [patients a day] range, then we know we are moving in the right direction. [. . .] Right now, we’re somewhere between six and ten a day.” About 18 months after the clinic’s opening, housing and healthcare leaders maintained a positive attitude about the clinic and their partnership and remained motivated. Despite the slower-than-expected adoption of the clinic, administrators shared that they were still “excited,” viewed the partnership as a “source of pride,” and an asset that they believe will become more valuable’ over time. As one healthcare leader put it, “my faith has not waivered in this [. . .]” This positive attitude stemmed from several perspectives, including the knowledge that it takes time to grow a practice, “My feeling, there again, as I said, I think it takes probably two years to see if a practice will really move, and I think it will and we’ll see numbers grow. [. . .] So, I-I don’t really look at any failure. . .I mean, I don’t think there is an impediment to succeeding with the clinic. [. . .] I-I I’m very optimistic about it.” Leaders also universally perceived the clinic as effective. As one housing leader put it, “From a healthcare delivery perspective, it has done everything we wanted it to do. We’ve had. . .I mean I’ve got a lot of anecdotal stories about how, oh my God, this person almost had this bad issue or that bad issue, and being a patient of the clinic, they were able to be helped. So, it is. . .it is doing. . .and it is getting to the people who have not been to a doctor in 12 years and it is definitely doing exactly what it needs to do in the way that it really does need to do it.” A housing leader related an event where the medical provider delivered emergency care and accompanied a resident to the hospital. “[the provider] took him to the hospital herself, waited there for him [. . .] . . .and then brought him home, which I thought was amazing.”
Regarding capability, healthcare administrators acknowledged that the clinic’s provider took on a large workload as the medical assistant was frequently moved to other clinics due to industry-wide short staffing related in part to COVID-19. In this situation, the nurse practitioner assumed a variety of roles including “the front desk person, the medical assistant, the provider, the person that checks somebody out, the security guard [. . .]” In addition, another healthcare leader shared that the clinic’s small scale doesn’t always translate to a smaller workload: “[The clinic's] taken up time. [. . .] Talking about ROI [return on investment] and the time that you spend on something, it takes just as much time to plan an event for a couple of people versus 100 people or 200 people [. . .] you know, just because it’s a small clinic doesn’t mean that it takes less work.”
Leaders at both organizations shared several patient barriers to clinic use, including residents already having established primary care providers (PCP), knowledge barriers about primary care in general, mid-level providers, how to change providers, and changes in routine care-seeking behavior since COVID-19. As one leader detailed, residents’ lifetime experiences with healthcare disparities or lack of a true PCP relationship make it challenging to emphasize the value of the clinic, “[. . .]we’re trying to [. . .] undo a lifetime of health and healthcare disparity. [. . .] you gotta think really out of the box to get people to peel back all the layers and things for people who never had the-the type of engagement with providers [. . .].” Leaders also described that changing providers is difficult and overwhelming, and that many older adults are loyal to their PCP even if they aren’t receiving health benefits, “[. . .] even if you talk to somebody and they said, you know, ‘No, I don’t really like this doctor.’ [. . .] It’s almost like they’re in a bad marriage even, you know what I mean?.”
Policy level barriers were exclusively noted by housing leaders, specifically, the FQHC’s Patient-Centered Medical Home (PCMH) model, which requires patients to fully transfer their primary care, “I think there’s been a difficulty with some of the clients going to the. . .to the clinic because they have. . .they have to leave their doctor to. . .you know, their doctor that maybe has been their doctor for years and years and years, in order to be a. . .you know, receive services through the clinic and-and from their doctor.” Notably, the housing organization shared wanting to take on additional costs to incentivize clinic growth in the form of a rent credit to resident-users but could not do so due to regulations. One housing administrator noted, “I was willing to give $25.00 a month of rent for a year for anybody who signed up [for the clinic]. And I saw that still as an awesome win for us, because it. . .when people have to move out, it costs us so much [. . .] So, those little bits of money, I could save by improving somebody’s health [. . .], you know, prolong their time being independent. I was really, like, okay with the financial piece, but because we have this partnership with them [FQHC], we would have violated [. . .]. . .we can’t incentivize people to use the health center.”
Unite Model Implementation—Residents
Twenty four residents completed semi-structured interviews (33.3% (n = 8) clinic users, 37.5% (n = 9) non clinic users, 29.2% (n = 7) attempted clinic users); half (50%) identified as Black and majority (63%) identified as female. All residents recognized the importance of primary care. Ease of transfer of care seemed to impact clinic utilization. Clinic users reported greater ease in transferring their care and insurance than attempted clinic users. One clinic user described the process as simple as showing up and presenting their insurance, “I just walked in, [. . .] introduced myself and said, “I’m so happy you’re here.” (Laughing) [. . .] I just showed them my [insurance] cards and everything went through fine. No problem. [. . .] She [Provider] just called my old doctor and requested my records, because I started going to her. [. . .] So, very smooth and simple.” On the other hand, attempted clinic users and non-clinic users were disappointed by limitations in insurance acceptance. One attempted user described, “And uh, they were showing some of the different insurances they took [at a clinic informational event]. I called my insurance company and they said no, they’re not. [. . .] I had the HMO, I had to be specifically with that nurse practitioner, and she wasn’t listed. [. . .] So, I did talk to them about it in the second meeting, that they. . .my insurance company told me they weren’t. . .she wasn’t connected with my insurance, so then I couldn’t come.”
Differences among residents were also noted in the importance of location of the clinic. Clinic users prioritized the co-location of the clinic as a major benefit, which only a few attempted clinic users and non-clinic users supported. As one clinic user reported, “And I can go, walk down the hall. Because I think I’m about three doors down the hall from the clinic, so if somethin’ bothers me, I can go down there and she, you know, she uh. . .I tell her what’s wrong [. . .] Then I have to have blood drawn once a month and she does that there. I used to have to go to a laboratory, and I’m relieved I don’t have to do that now, because they got it set up now where they can do it with me here. You know, do the job here.“ Some residents would have preferred using the clinic for more urgent needs, which was not accepted in the clinics Medical Home Model. [. . .] if I would be somebody that would have the clinic available to them [. . .] because I thought a clinic, okay. To me, it would be, like, for stitches or emergencies or whatever.”
Motivation was high among clinic users, and many non-clinic users shared that they had previously contemplated using the clinic. Attempted clinic users had low motivation, mostly from maintaining their current PCP and their negative interaction with the clinic during the initial attempt. As one attempted user shared, the challenges of changing their doctor outweighed some of the benefits of clinic co-location. A non-clinic user reported, “[My doctor] know more about me and he know my condition and he know what I need, what I supposed to be taking. Because if I go to the clinic, they probably give me something else that does not. . .is not agreeable to me.” These challenges were also reflected in the structured longitudinal surveys (Study population 2). For residents who saw a PCP other than the Unite Clinic (n = 86), reasons for seeing that provider were established prior relationship (n = 84), uncertainty or perception that the clinic did not accept their insurance (n = 16), or did not know how to make an appointment (n = 7).
Discussion
This study was an early evaluation of the Unite Care Model, a community-led, cross-sector initiative to improve access to care and, in turn, health among low-income older adults that combined two service sectors: housing and health care in a predominately Black, low-income community. There was no difference in the primary outcome, blood pressure, secondary outcomes, physical or social environment changes between residents who used the Unite clinic and those who did not. Overall, the reach of the clinic and social needs support was fair, while the reach of social and health events was higher. Implementation of the clinic was limited to scheduled visits (i.e., no urgent or home visits), and assistance with social needs was absent for 6 months. Healthcare and housing leaders maintained their motivation for the care model, perceived the clinic as effective, and acknowledged some patient and policy barriers to greater clinic reach. Expanding clinic services to include urgent and home visits may improve clinic reach. Additionally, improving implementation through adequate staffing and overcoming insurance barriers may increase the effectiveness of the Unite Care Model.
There are several hypotheses for the lack of change in BP and the physical and social environment. First, participants had lower SBP (133.2 mmHg (enrollment) vs. 162 mmHg (expected)), and enrollment was lower (179 (enrollment) vs. 285 (expected)) than anticipated. Thus, the study was underpowered to detect a 2 mmHg decrease in SBP. However, given the lack of the observed effect, it is unlikely that limited statistical power alone explains then null findings. Second, the reach and implementation of the Unite clinic were limited. Only about 13% of residents completed a clinic visit which may have limited the effectiveness of the Unite Care Model. Further, like many organizations during COVID, the Unite Care Model experienced changes in staffing during the evaluation period, which limited the implementation of the care model. In particular, the staffing gaps in the CHW and clinic staff may have left a void in addressing health-related social needs. In addition, the COVID pandemic may also have impacted the results, particularly environmental modifications and social environment, by limiting in-person interactions and restricting visitors to the housing facility.
The Unite Care Model evaluation was conducted over a short time frame. As noted by the clinic and housing leaders, it takes many years to fully establish a new clinic, especially one like the Unite Care Model. Engaging with elements of the care model, such as transitioning medical care to the Unite clinic, may require trust cultivated over time, physical and cognitive health changes, or changes in resources that previously facilitated access to medical care (i.e., transportation, care partner support). Thus, while this study was designed to measure the impact of the Unite Care Model during its first year, further analysis of the impact as it reaches a steady state is warranted.
Despite the limited reach and challenges with implementation, housing and healthcare leaders remained enthusiastic about the Unite Care Model. Resident attendance at social and health events is encouraging. Identifying content that resonates with residents may be one opportunity to enhance the impact of the Unite Care Model.
The Unite Care Model was designed to address challenges with access to care, including transportation, physical distance to services, and scheduling (Corscadden et al., 2018). We found that residents with transportation needs were more likely to utilize the clinic, suggesting that clinic co-location may improve access to care. However, our results suggest that improving health and healthcare utilization requires more than building infrastructure. Other barriers, such as insurance and care delivery models (i.e., the requirement to serve as a medical home), may have impeded the reach of the Unite Care Model. Our findings are similar to other programs that showed that physical location is important but also just one of many factors that predict uptake (Schneider et al., 2019). Like other cross-sector housing and healthcare collaborations, the Unite Care Model faced challenges with insurance policy, suggesting that even wider collaboration, with, for example, state and federal government, is needed (Sharpe et al., 2018).
Community-led projects are a form of community-engaged research with the greatest community ownership and facilitate building community power (Iton et al., 2022). Community members identify research priorities and implement the program with or without the support of academic partners. Establishing community-academic partnerships is influenced by the community’s history and built on trust, respect, and transparency. This process occurs over time and is facilitated by academic partners’ sustained commitment to the community, resource sharing, and capacity building (Key et al., 2019). We have partnered with housing and healthcare partners to promote health equity for over 14 years. The benefits of deep, sustained community-academic partnerships, including share resources, mutual influence, capacity growth, and longstanding trust, may have contributed to initiation of the Unite Care Model and its evaluation and provided a foundation with which future projects can be developed and tested (Fichtenberg et al., 2020).
Limitations
This study has limitations. This was an early evaluation of the Unite Care Model and does not reflect its steady state. A future study could follow both clinic users and non-users over time. Second, this was a non-randomized study design, and there are unadjusted confounders, such as people who selected to use the Unite clinic may have harder-to-control BP than those who did not. Third, the physical environment measures were adapted from a study that measured the most common repairs or modifications among older adults (Szanton et al., 2015). However, this measure has not been validated. Finally, our results are limited to one clinic and housing community.
Conclusion
The Unite Care Model was not associated with improved BP, or physical or social environment in its first year of implementation. Expanding the reach of the clinic through providing urgent care or home visits and implementation, through adequate staffing and overcoming insurance barriers, may increase the effectiveness of the Unite Care Model.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334261422615 – Supplemental material for Evaluation of a Community-Led, Cross Sector Partnership of Housing, and Healthcare to Optimize Aging: The Unite Care Model
Supplemental material, sj-docx-1-ggm-10.1177_30495334261422615 for Evaluation of a Community-Led, Cross Sector Partnership of Housing, and Healthcare to Optimize Aging: The Unite Care Model by Lesli E. Skolarus, Abby K. Hellem, Erica Thrash-Sall, Sarah Bailey, Michael Giacalone, Casey L. Corches, Chun Chieh Lin, Ran Bi, James F. Burke and Anne E. Sales in Sage Open Aging
Footnotes
Acknowledgements
We would like to thank our partners, Hamilton Community Health Network and McFarlan Villages.
Ethical Considerations
This research was approved by the University of Michigan (HUM00197049). The University of Michigan serves as the single Institutional Review Board. Northwestern University relies on this sIRB under reliance approval (STU00219180).
Consent to Participate
All participants provided informed consent prior to participating.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health: National Institutes on Aging [R21AG071796].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.