
Abstract
Objective:
Global healthcare systems face growing challenges from aging populations and chronic diseases. Although digital health technologies provide innovative disease management solutions, elderly patients often experience technology-related anxiety due to operational barriers and privacy concerns, hindering adoption. Current research lacks focus on elderly patients’ emotional responses during technology-assisted medical visits, particularly regarding family support and professional escort services.
Methods:
A cross-sectional study was conducted with 241 elderly chronic disease patients from five Sichuan Province hospitals. Using validated scales (APGAR Family Function, Technology Anxiety, and Escort Service Willingness), data were analyzed through SPSS PROCESS macro and Bootstrap methods to examine mediating effects.
Results:
Key findings confirmed: (1) Family care negatively correlated with technology anxiety; (2) Technology anxiety positively correlated with escort service willingness; (3) Family care negatively correlated with escort service willingness; (4) Escort service willingness mediated between family care and technology anxiety, with the “subjective norms” dimension showing the strongest mediation (40.37% of total effect).
Conclusion:
Family care plays a dual role—directly reducing technology anxiety and indirectly decreasing reliance on escort services. The significant mediation through “subjective norms” highlights how social networks shape elderly patients’ technology acceptance.
Keywords
Introduction
The world’s population is aging rapidly, leading to a steady increase in chronic disease patients, which is a major public health challenge. According to China’s National Bureau of Statistics, the elderly population has surpassed 300 million, and about 75.8% of them have at least one chronic condition (The Lancet, 2022; Wu, 2023). Digital health technologies, a key part of smart healthcare, use advanced tools like artificial intelligence and big data to help monitor, assess, and manage individual health (Lott et al., 2024). For example, wearable devices and self-service equipment offer elderly patients more personalized health management and make it easier for them to get medical resources (Jimenez et al., 2023). However, studies show that older adults often feel very anxious about using new digital health tools because they find them hard to use, worry about privacy, or doubt their effectiveness (Badr et al., 2024; De Santis et al., 2023). This anxiety can make their healthcare experience worse and is a major reason they might avoid using these technologies.
Digital health technology anxiety refers to the fear or worry people feel about digital technologies, which makes them want to avoid using them (Hsieh et al., 2020). Research confirms that older adults with chronic diseases are especially likely to feel negative emotions like depression and anxiety (Hoque & Sorwar, 2017). Social support theory suggests that when people face stress or challenges, they can reduce their psychological burden and cope better with help from relationships that provide emotional, informational, material, and instrumental support (Heaney & Israel, 2008). This support can come from informal sources, like family and friends, or formal sources, like healthcare professionals.
Family care, a core part of social support for elderly patients, is essential for reducing psychological distress and improving their quality of life (Aass et al., 2022). It is defined as a support system that includes emotional bonding, practical help, and providing resources (Cantor, 1989). Strong family care not only improves mental health but may also help patients accept technology more readily (Lin et al., 2022). When family members help older adults use digital tools, it can improve their technical skills and reduce anxiety indirectly (Dermody et al., 2024). Moreover, emotional support from family reduces loneliness and anxiety while building psychological resilience, creating a sense of security that directly lowers resistance to new technologies (Williams, 2005).
At the same time, professional escort medical services—a key form of support during hospital visits—have been shown to help reduce technology-related anxiety (Xu et al., 2024). These services, offered by trained medical escorts or social workers, include help with booking appointments, going with patients to consultations, and providing medical guidance, combining professional assistance with emotional support (Deng & Liu, 2023). Often, family members arrange these services. Escorts not only give technical support but also provide emotional comfort when family is not available, reducing feelings of isolation and helplessness in unfamiliar technological settings. However, research on escort services is still limited, and no study has systematically examined how family care influences the use of these services to reduce digital health anxiety.
Based on social support theory, family care (informal support) and escort services (formal support) together form the social support network for elderly patients. Family care may directly reduce anxiety through emotional comfort and technical guidance, and it may also indirectly encourage the use of escort services. Conversely, escort services offer specialized help that families might not be able to provide. To explore these relationships systematically, this study set the following goals: (1) To examine the direct links between family care, digital health technology anxiety, and willingness to use escort services in elderly chronic disease patients; (2) To test whether willingness to use escort services mediates the relationship between family care and digital health technology anxiety; and (3) To identify which specific aspect of escort service willingness (e.g., subjective norms, perceived usefulness) contributes most to this mediation. Therefore, this study proposes:
Method
Participants
This cross-sectional study used convenience sampling to recruit 241 elderly chronic disease patients from five tertiary hospitals in Sichuan Province between September and November 2024. Patients were included if they: (1) Were diagnosed with one or more chronic diseases based on standard criteria (Diet, 2003); (2) Age ≥ 60 years; (3) Could communicate effectively with researchers; (4) Provided informed consent themselves or through a family member. Patients were excluded if they: (1) Could not understand the study’s purpose and procedures even after detailed explanation, making informed consent impossible. The study was approved by the Medical Ethics Committee (Approval No.: 2024-04-087-K01).
Sample Size Determination
This study had 26 observed variables. We used G*Power 3.1 software to calculate the required sample size (Faul et al., 2007). Assuming a medium effect size (f² = 0.15), α = .05, and power (1 − β) = 0.80, the analysis showed we needed at least 176 participants. To account for potential issues like non-response (estimated 10%), incomplete data (5%), and the need to control for covariates (5% buffer), we increased the sample size by 20% based on common research practice. The final target sample size was 211 participants.
Demographics
The research team created a questionnaire with 11 items covering: gender, age, marital status, education level, pre-retirement job, type of health insurance, living situation, average monthly household income, main source of income, number of medical visits in the past year, and whether someone usually accompanied them to visits.
Family Care Degree Questionnaire, APGAR
We used the Family Care Degree Questionnaire, originally created by Smilkstein (1978) and and later translated into Chinese by Lv et al. (1999), to measure family functioning. The scale has five items: adaptability, partnership, growth, affection, and resolve. Each item is rated on a 3-point scale: “almost never” (0 points), “sometimes” (1 point), or “often” (2 points). A total score of 0 to 3 suggests severe family dysfunction, 4 to 6 indicates moderate dysfunction, and 7 to 10 means good family functioning. Higher scores mean better family functioning. The original scale was highly reliable, with Cronbach’s α between .880 and .883. In our study, the scale also showed acceptable reliability, with a Cronbach’s α of .723.
Technophobia Scale
We used the Technophobia Scale, developed by Khasawneh (2018) and translated into Chinese by Sun et al. (2022). It has 13 items across three areas: technology tension, technology fear, and privacy concerns. We used a 5-point Likert scale, from “completely disagree” (1 point) to “completely agree” (5 points). Higher scores indicate greater technology-related anxiety. The Chinese version has good reliability and validity, with Cronbach’s α for the total scale and subscales ranging from .759 to .911, and all content validity indices were above 0.800. In our study, the Cronbach’s α was .903.
Willingness to Use Accompanying Medical Services Scale
We used a scale developed by Wang et al. (2024) to measure how willing elderly individuals were to use accompanying medical services. It uses a 5-point Likert scale and covers seven aspects: subjective norms, perceived behavioral control, perceived usefulness, perceived ease of use, trust, attitude, and behavioral intention, with 22 items in total. Higher scores mean a stronger willingness to use these services. The original subscales had Cronbach’s α between .764 and .845, and all content validity indices were above 0.700. In our study, the scale showed similar reliability (α = .796).
Data Collection and Quality Control
We implemented strict quality control to ensure good data. All researchers received the same training and used standard instructions to survey patients on the day of their medical visit. We obtained informed consent from participants before starting and collected signed consent forms. We collected questionnaires on the spot and checked them for completeness, removing any that were invalid. Two people entered the data separately and then cross-checked it to ensure accuracy, making the study findings more reliable and rigorous.
Analysis Strategy
We performed statistical analysis using the Process macro program in SPSS 27.0. We described categorical data using frequencies and percentages (%), and normally distributed data as mean ± standard deviation. We used t-tests or one-way ANOVA to compare groups. We used Pearson correlation coefficient to examine relationships between variables. We tested mediation effects using the Bootstrap method and calculated 95% confidence intervals. We set the significance level at α = .05, considering a p-value <.05 as statistically significant.
Results
Common Method Bias Test
We used Harman’s single-factor test to check for common method bias. The results showed that the first factor explained only 28.2% of the variance, which is well below the 40% threshold, indicating no significant common method bias (Tang & Wen, 2020).
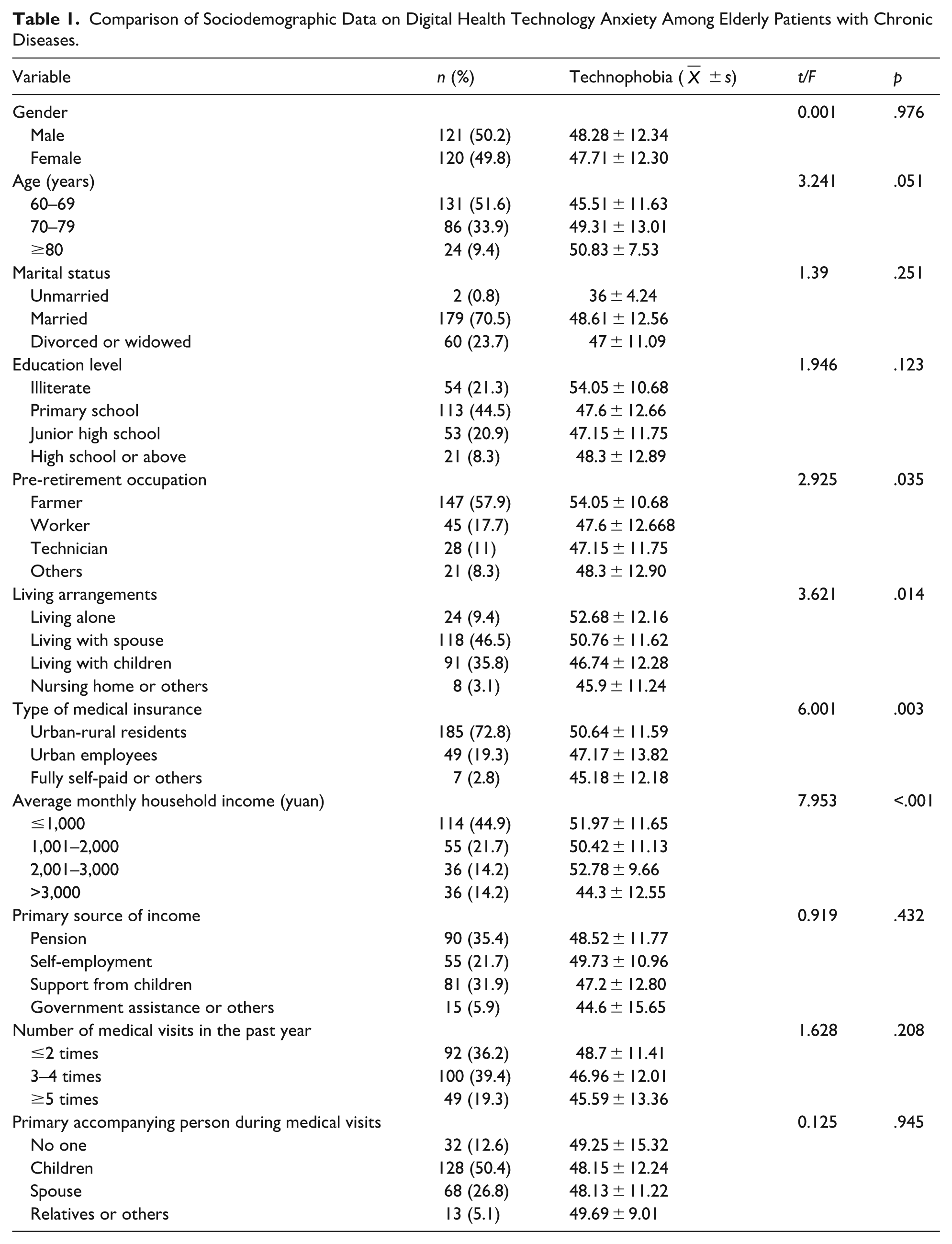
Comparison of Sociodemographic Data on Digital Health Technology Anxiety Among Elderly Patients with Chronic Diseases
We collected 260 questionnaires. After excluding 19 that were incomplete or invalid, we had 241 valid responses. Among these, 121 were from men (50.2%) and 120 from women (49.8%). For age, 131 participants (51.6%) were 60 to 69 years old, 86 (33.9%) were 70 to 79, and 24 (9.4%) were 80 or older. For education, 54 (21.3%) had no formal education, 113 (44.5%) had primary education, 53 (20.9%) had junior high school education, and 21 (8.3%) had high school education or more. The average digital health technology anxiety score was 48 ± 12.29. We found that 77.59% of patients reported some level of digital health anxiety. Detailed data are in Table 1.
Comparison of Sociodemographic Data on Digital Health Technology Anxiety Among Elderly Patients with Chronic Diseases.
Correlation Analysis of Family Care, Digital Health Technology Anxiety, and Accompanying Medical Services
In elderly chronic disease patients, family care was significantly negatively correlated with digital health technology anxiety (r = −.22, p < .01). Digital health technology anxiety was significantly positively correlated with the overall willingness to use accompanying medical services (r = .33) and all its subscales: subjective norms (r = .32), perceived behavioral control (r = .30), perceived usefulness (r = .31), perceived ease of use (r = .31), trust (r = .29), attitude (r = .30), and behavioral intention (r = .34; all p-values <.01). Family care was significantly negatively correlated with the overall willingness to use accompanying medical services (r = −.33) and all its subscales (all p-values < .01). Detailed data are in Table 2.
Correlation Analysis of Family Care, Digital Health Technology Anxiety, and Accompanying Medical Services.

p < .01.
Mediation Effect Analysis of the Total Score and Subscales of Willingness to Use Accompanying Medical Services
The study found correlations between family care, digital health technology anxiety, and willingness to use accompanying medical services. The overall score and all subscales of willingness were significantly correlated. We used the SPSS macro PROCESS to test for mediation effects. The results showed that the overall willingness to use accompanying medical services partially mediated the relationship between family care (independent variable) and digital health technology anxiety (dependent variable). This finding held true even after controlling for covariates like pre-retirement job, living situation, type of health insurance, and average monthly household income (Figure 1). When we looked at the specific subscales, we found that all except the behavioral intention subscale showed significant mediation effects. Among these, the subjective norms subscale had the strongest mediation effect (Figure 2).

Partial mediation effect of the total score of accompanying medical services between family care and digital health technology anxiety.

Partial mediation effect of the subscale between family care and digital health technology anxiety.
We used the Bootstrap method for further validation. The results showed that for the overall willingness score and its six subscales (all except behavioral intention), the total effect, direct effect, and indirect effect all had 95% confidence intervals that did not include zero. This strongly supports the existence of partial mediation effects (detailed data are presented in Table 3). Further analysis revealed that the subjective norms subscale contributed the most to the mediation effect, accounting for 40.37% of the total effect. This suggests that subjective norms are not only a key part of the willingness structure but also a crucial pathway in how these variables influence each other.
Mediation Effect Analysis of the Total Score and Subscales of Willingness to Use Accompanying Medical Services.
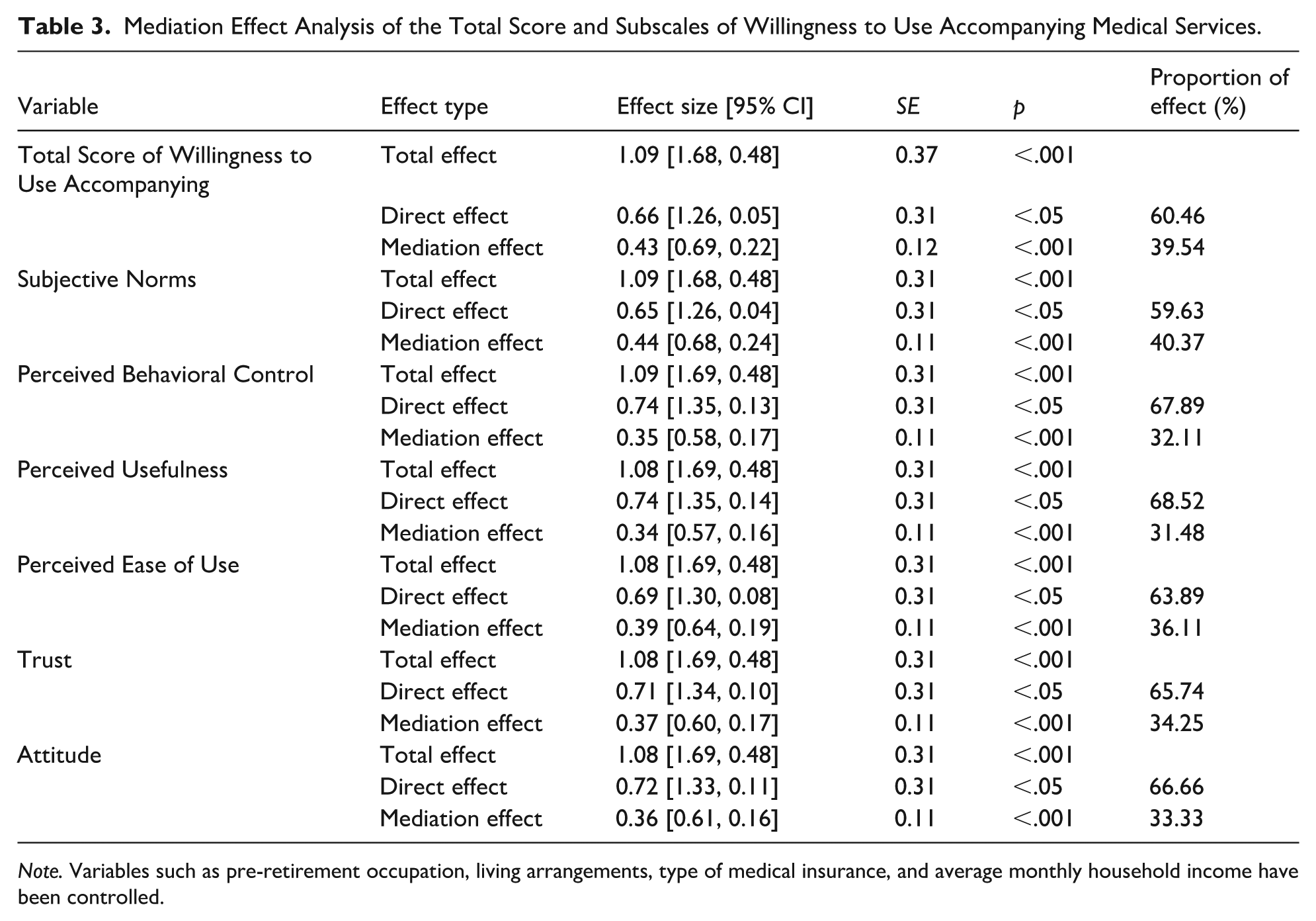
Note. Variables such as pre-retirement occupation, living arrangements, type of medical insurance, and average monthly household income have been controlled.
Discussion
This study found that the average digital health technology anxiety score among elderly chronic disease patients was 48 ± 12.29, and 77.59% of patients experienced some level of this anxiety. This result differs from a study by Peng et al., 2023) on community-dwelling older adults, possibly because our sample consisted of hospitalized patients with chronic diseases, and the medical environment itself might increase worries about not being able to use health monitoring tools correctly (Wenhua et al., 2023). Further analysis showed that retired farmers had the highest technology anxiety, which might be due to less exposure to digital devices (Yang et al., 2024). Elderly patients living alone also had higher anxiety, because they lacked immediate technical support and felt frustrated when trying to operate the technologies (Llorente-Barroso et al., 2021). Additionally, patients with urban-rural resident medical insurance and a monthly household income below 1,000 yuan showed pronounced anxiety, because financial constraints limited their access to digital health tools, making them more anxious when facing new technologies (Kaihlanen et al., 2022). Therefore, in the era of smart healthcare, we should pay special attention to the digital health challenges faced by elderly chronic disease patients in rural areas, those living alone, and those with low incomes, to ease their psychological concerns and help them benefit more from digital advances.
The study showed a significant negative correlation between family care and digital health technology anxiety, meaning that better family care was linked to lower anxiety. This aligns with research by Philippe et al. (2022), suggesting that family care provides emotional support and practical help, boosting patients’ confidence in managing their health and reducing their unease with digital tools (Taylor et al., 2023).
At the same time, digital health technology anxiety was positively correlated with the willingness to use escort services and all its aspects, meaning that more anxious patients were more willing to use these services. This matches findings by H. H. Zhou et al. (2022), because elderly patients feel uncertain and insecure with complex digital health technologies, and escort services offer professional, in-person support and guidance, which can reduce their anxiety (Bai, 2024). Furthermore, family care was negatively correlated with the willingness to use escort services and its subscales, suggesting that strong family support reduces the need for external escort services. This might be because family care provides enough emotional support, daily care, and health management help, making patients less reliant on outside services (H. H. Zhou et al., 2022). Therefore, when creating health management plans for elderly chronic disease patients, we should emphasize the role of family care, encouraging family members to take an active part in the patient’s health and provide necessary emotional and practical support to reduce digital health anxiety. It is important to note that as family structures change, relying only on better family care to reduce technology anxiety might be difficult in practice. The strong negative correlation between family care and the subjective norms dimension of willingness to use escort services is consistent with a 2018 study by Pal et al. (2018). Possible reasons include some elderly patients not fully understanding what escort services involve and their value, as well as differences between traditional family care ideas and modern escort services (Jiang et al., 2022). These factors together may affect patients’ willingness to accept escort services. Therefore, for elderly patients with little family support or high digital health anxiety, medical institutions and social service groups should improve and optimize escort services, offering personalized support to make up for the lack of family care and ensure patients get complete health management help.
Among elderly chronic disease patients, the willingness to use escort services significantly mediated the relationship between family care and digital health technology anxiety. This means that family care not only directly affects digital health anxiety levels but also does so indirectly by influencing how willing patients are to use escort services. This finding fits with ecological systems theory, which states that individual behavior is shaped not just by personal ability, knowledge, and motivation, but also by factors in the social environment at different levels (McLeroy et al., 1988). Specifically, the amount of family care directly affects elderly patients’ confidence and sense of security in managing their health (Abulaiti et al., 2022; Juba et al., 2024): when family care is sufficient, patients need escort services less, which reduces their reliance on and anxiety about digital health technologies. On the other hand, when family care is lacking, patients are more likely to seek external escort services and feel more anxious due to the absence of family support.
The study found that the subjective norms subscale of the willingness to use escort services contributed the most to the mediation effect, making up 40.37% of the total effect. The subjective norms subscale measures how much influence important people in a patient’s life have on their decision to use escort services. This finding might be because elderly patients are more influenced by the opinions and actions of people close to them in social situations, especially regarding health matters (Van Orden et al., 2021). They often depend on advice and support from family, friends, or peers to reduce uncertainty and anxiety when making decisions (Maier et al., 2021). Therefore, recommendations and support from others can greatly increase elderly patients’ acceptance and willingness to use escort services. This suggests that when promoting escort services, we should fully utilize the power of social networks. Specifically, we can take the following steps to improve service effectiveness: First, encourage family, friends, and peers to be involved in elderly patients’ health management decisions, increasing their awareness and trust in escort services; Second, improve family care by offering training on health management skills for family members and providing family support services; Additionally, for elderly patients with insufficient family care, provide flexible and convenient escort services, along with guidance on using digital health technologies, to ease their technology-related anxiety. Meanwhile, healthcare institutions and service providers can use community activities and health education to create a supportive social environment for escort services, further increasing elderly patients’ willingness to use them and optimizing health management outcomes.
Limitations and Future Directions
This study has some limitations: (1) Using questionnaires for data collection might lead to reporting and recall biases; future studies could include behavioral experiments, like observing how elderly patients actually use digital health technologies, and physiological measures, like heart rate variability, to get more objective data; (2) The cross-sectional design means we cannot determine cause and effect; longitudinal studies with multiple assessments over time are needed to establish causal relationships; (3) Recruiting patients from hospitals in one region may limit how widely the findings can be applied; future research should include participants from different regions and various healthcare settings. Based on these findings, future research should: (1) Investigate how different types of digital health technologies, like remote consultations versus health monitoring devices, affect technology anxiety differently; and (2) Develop specific interventions to improve family support and optimize escort services for reducing digital health anxiety in elderly patients. These steps will help advance health management models for elderly chronic disease patients and improve the adoption of digital health technologies.
Footnotes
Acknowledgements
The authors gratefully acknowledge the financial assistance provided, which enabled the successful completion of this research. Sincere thanks to all nurses who participated in this study, as well as colleagues and institutions for their support. Special gratitude to my supervisor for guidance and team members for collaborate.
Ethical Considerations
This study was approved by the Medical Ethics Committee (No: 2024-04-087-K01). The study was carried out in compliance with the Helsinki Declaration, and all the participants provided written informed consent prior to enrollment.
Author Contributions
Furong Jiang (the first author) was responsible for research design, data collection and analysis, initial draft writing, and team coordination, while Tianxia Zhao participated in research design, data collection and analysis, as well as the writing of the methodology section. Yao Liu took charge of in-depth data analysis, results presentation, literature review updating, and format adjustment. Ping Dai provided the research background, constructed the theoretical framework, wrote the introduction and conclusion, and organized the references.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Sichuan Applied Psychology Research Center Project (CSXL-25315) and the Deyang Science and Technology Bureau Project (2024SZY076).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during this study are not publicly available due to participants’ non-consent for public data sharing. However, anonymized data or analytical details may be made available by the corresponding author upon reasonable request and subject to ethical approvals.
Generative AI Statement
The authors declare that no Generative AI was used in the creation of this manuscript.