
Abstract
Purpose:
To evaluate participant demographics and program distributions and understand characteristics of access in an older adult exercise program in Saskatchewan, Canada.
Methods:
A cross-sectional survey was circulated to exercise participants and leaders to understand and evaluate demographics, program locations, and characteristics of participant access.
Results:
Of 589 complete participant and 207 leader surveys, most respondents were female (87% and 94%, respectively) and white (97% for both groups), with 68% of participants and 49% of leaders being urban residents. Some equity-deserving groups such as widows and low-income earners were well-represented. Program density was higher in regions with dedicated implementation staffing, and travel was the most agreed-upon barrier to access.
Conclusion:
There is evidence of under- and over-representation of certain equity-deserving populations in this exercise program, as well as regional differences in program availability. Future research could explore system-wide factors that support ongoing program implementation while reducing equity-related gaps.
Introduction
Canada’s population is aging, with the percent of Canadians aged 65 and over increasing from approximately 13.4% in 2007 to upward of 25% by around 2036 (Government of Canada, 2014; Rosenberg et al., 2022). This growing demographic will experience diverse health concerns such as increased rates of chronic conditions, cognitive impairments and disability which will impact functional independence and overall quality of life and cause widespread social and economic consequences (Government of Canada, 2014; Kuh, 2007; Rowe & Kahn, 1997). Providing for the unique social and physical needs of older adults in Canada is important to promote aging in place and facilitate the greatest quality of life possible for these important community members (Pace & Grenier, 2016; Visconti & Neiterman, 2021; Walker, 2002).
Group-based exercise programing offers many health benefits for older adults, including reductions in cognitive decline and falls, prevention and management of chronic conditions, improved mental health, and promotion of social connectedness (Bauman et al., 2016; Sherrington et al., 2017). The supportive atmosphere of group-based exercise programing also improves motivation to exercise, (Royse et al., 2023) and is more cost-effective compared to one-on-one approaches (Aranda-Reneo et al., 2021).
Unfortunately, studies that implement exercise programs for older adults in the community have frequently recruited over-represented populations of urban and white participants (Brown et al., 2009; Farrance et al., 2016; Oken et al., 2006). Other studies have intentionally recruited Indigenous, immigrant, or low-income participants using participatory methods (Crist et al., 2022; Gidgup, Kickett, Jacques, Weselman, et al., 2022; Sin et al., 2005). Studies investigating equitable distribution of exercise programs are scarce, but research on health promotion programs such as immunizations or cancer screening reveal inequitable program distribution and lower rates of service use by equity-deserving groups (Bandara, 2019; Honein-AbouHaidar et al., 2013). Exercise programs for older adults may show similar inequities either by geographical distribution or by participant demographics.
Levesque’s Access to Healthcare Framework
Inequities in health promotion programing may be understood using theories or frameworks such as Levesque’s access to healthcare framework (Levesque et al., 2013). These authors define access to healthcare as “the opportunity to reach and obtain appropriate health care services in situations of perceived need for care” (Levesque et al., 2013, p. 19) and conceptualize access as an intersection of both system and participant factors which are grouped into five dimensions each. The system-level dimensions include approachability, acceptability, availability and accommodation, affordability, and appropriateness; the participant-level dimensions mirror the system-level dimensions and include ability to perceive, seek, reach, pay, and engage with the healthcare service.
To our knowledge, no studies regarding exercise programs for older adults have described access using all five dimensions of Levesque’s framework, though an abundance of exercise research has explored factors within each dimension. For instance, in the approachability/ability to perceive dimension, studies have explored advertising campaigns (John-Leader et al., 2008) and perceived benefits of exercise programing (Dunlop & Beauchamp, 2013; Gidgup, Kickett, Hill, Francis-Coad, et al., 2022). Acceptability and ability to seek may relate to cultural appropriateness or gender norms (Argyle et al., 2022; Brooks-Cleator & Giles, 2016; Dunlop & Beauchamp, 2013; Gidgup, Kickett, Hill, Francis-Coad, et al., 2022). Travel, time, and mobility constraints fall under the availability/accommodation and ability to seek dimensions (Ades et al., 2017; Bethancourt et al., 2014), while affordability and ability to pay relate to the costs of participating in a program, such as program fees or loss of income from missing work to attend (Ades et al., 2017; Gidgup, Kickett, Weselman, Hill, et al., 2022). Finally, appropriateness and ability to engage refer to how well the service fits with participant needs or preferences, which may be an especially important determinant for long-term engagement (Levesque et al., 2013). Considerations under this dimension are numerous and include exercise leader qualities and exercise mode and environment (Bethancourt et al., 2014; Dunlop & Beauchamp, 2013; Liu et al., 2022).
Since some health promotion programs have not reached participants equitably by geographic region or demographic characteristics, we are concerned that exercise programs for older adults may follow similar patterns. Levesque’s framework might advance our understanding of personal and system-level factors that promote or prohibit participation. Our objective, therefore, was to describe the demographic characteristics of participants and exercise leaders in a provincial older adult exercise program in Saskatchewan, to examine distribution of programs across the province, and to identify barriers to accessing the program.
Methods
Study Context
The Saskatchewan Forever. . .in motion (FIM) older adult exercise program is a peer-led exercise program delivered in recreation centers, seniors’ housing complexes, churches, and community facilities across the province of Saskatchewan, Canada. The program’s primary exercise components are strength and balance but also incorporate cardiovascular and flexibility training. Exercise sessions are 30 to 60 min and occur at least once per week based on leader availability. Exercise leaders are primarily retirees who have completed a 20+-hour training program, most of whom serve in a volunteer capacity.
The FIM program started as a pilot project within one primarily urban health region in Saskatchewan. Currently, the FIM program is implemented across the province through two organizations: the Saskatchewan Health Authority (SHA), whose FIM jurisdiction includes the health regions of Saskatoon and Regina, and the Saskatchewan Parks and Recreation Association (SPRA), which serves the rest of the province. The SHA employs staff in the Saskatoon and Regina health regions to train exercise leaders and provide ongoing program support. The SPRA has staff who coordinate the FIM leader training courses, but communities must self-fund or apply for an SPRA grant to pay for training. Unlike the SHA, the SPRA does not have funds to help facilitate FIM site start-ups or provide ongoing support for leaders. Initiative and ongoing support instead comes from recreation coordinators or through highly-motivated community members.
Study Design
This study used a single cross-sectional survey design, which collected program and participation details from participants and exercise leaders currently involved in FIM programs across Saskatchewan.
Participants
FIM exercise leaders and participants were recruited to participate in this study. Inclusion criteria for participation was having participated in at least one FIM exercise session in the past 2 months, and able to complete a survey in English.
Recruitment
Recruitment occurred from April 2023 to July 2023 through distributing survey invitations to all known FIM leaders across the province, who then shared the invitations with their participants. To prevent response-bias from online-only surveys, the invitations included a web link to access the survey online as well as a phone number to request a paper survey to complete with return postage. The sample size was initially set at a target of 500 exercise participants and 50 exercise leaders, but no cap on sample size was placed as the goal was to recruit as representative as possible and to allow for multiple statistical comparisons.
Surveys
Participants and leaders completed separate surveys. Both surveys included demographic questions from the 2021 Canadian census:(Statistics Canada, 2021) age, gender, town/city of residence, ethnicity, education, years living in Canada, driving status, caregiver, and marital status, as well as a categorical response for income (in $25,000 increments). Yes/no responses for six common chronic condition categories (cardiovascular disease, chronic respiratory disease, diabetes, mental illness, musculoskeletal disorders and neurological disease) were derived from the Canadian Community Health Survey (Statistics Canada, 2022a). We self-generated questions regarding FIM participation (program location, how often they attend each week, etc.) and program access relating to Levesque’s framework, including multiple-choice questions regarding how far they travel to reach the program, how they found out about the program, and open-ended reasons for joining. We also generated 5-point Likert-scale questions on the extent to which hypothetical program characteristics relating to Levesque’s dimensions of access would impact participants’ willingness to join the FIM program. Responses ranged from strongly disagree to strongly agree, as well as a sixth, “not applicable” option. Responses were scored as bivariates, with agree/strongly agree coded as “1,” which meant they viewed the circumstance as a barrier, and all other responses coded as “0,” meaning they did not see the circumstance as a barrier.
Provincial statistics
Demographic data and populations of adults aged 65 and over within each health region in Saskatchewan was obtained from Statistics Canada (Statistics Canada, 2015, 2020b, 2022b, 2022c, 2023a, 2023b), this data was used to compare the relative representation of the various demographic characteristics of FIM participants and leaders.
Mapping
Exercise leaders and participants listed their facility name(s) and city; multiple location responses were permitted. We recorded addresses for each facility using Google Maps, created a list of unique locations, geocoded these addresses using the Google Sheets ad-on “Geocode for Google Sheets,” and reviewed the geocoded locations for accuracy. Vector files for the health region boundary lines in Saskatchewan were obtained from Stats Canada digital boundary files (Statistics Canada, 2020a). All data was added as separate layers into the geographic information system software QGIS (version 3.34.1) for visualization.
Analysis
Surveys with incomplete responses for demographics and bivariate access questions were excluded from subsequent analysis, except for variables such as income where the response rate was low, but the variable was seen as an important determinant. Exercise participant and leader demographics were analyzed as number and percent, unless otherwise stated. Provincial proportions of populations for adults aged 65 and over are listed alongside demographics of participants and leaders for descriptive comparison.
We used the “count by polygon” tool in QGIS to quantify the number of programs in each health region. We then divided each region’s program count by the number of residents over 65 in each health region to calculate population-standardized program densities per 10,000 adults aged 65 and over.
Access-related questions were first analyzed descriptively. Next, questions relating to access were consolidated into four of the five dimensions described by Levesque et al. (2013), and the “abilities” labels for each dimension are used to center participant perspectives. The bivariate scores for the questions in each dimension were summed and then coded as “Agreed to 1 or more barriers” or “Agreed to 0 barriers.” The ability to perceive dimension had no questions about barriers and was excluded from the bivariate analysis. Lastly, to assess whether certain demographic groups endorsed barriers more than their reference groups, we created 2 × 2 tables and conducted Pearson’s chi-squared tests for bivariate summary dimension scores and bivariate demographic characteristics: age, gender, urban/rural residence, caregiver status, driving status, education level, and number of chronic conditions. These demographic variables were chosen because they had at least 10% representation in at least two categories of the variable and because they have previously shown differing levels of exercise program participation (Klepac Pogrmilovic et al., 2021).
Ethics
Ethical approval was obtained from the University of Saskatchewan Behavioral Ethics Board (Certificate ID: BEH 4042). The consent form was attached to the beginning of each survey, and by completing the survey, participants implied consent.
Results
Respondent Characteristics
Of the 744 participant surveys returned, 589 had complete access and demographic data. Leaders submitted 231 surveys, 207 of which had complete demographic data. Pen-and-paper surveys were submitted by 320 (43%) of participants and 21 (9%) of leaders. Demographic characteristics in the participant and leader samples with complete data differed by no more than 2% compared to their respective total samples, except for participant education (3% absolute difference).
Characteristics of exercise participants and leaders are listed in Table 1. The mean age of participants was 75 years (range 47–96), the majority being white (96%), urban residents (69%), female (87%), current drivers (89%), without caregiving responsibilities (93%); these proportions were at least 5 absolute percentage points higher than provincial proportions. Widows constituted 27% of respondents, and 13% of respondents had an income less than $25,000; these characteristics are also higher-than-representative proportions. Over half (59%) of participants attended the program for over 12 months, and 66% of participants attended the program two or more times per week.
Respondent Characteristics.

Note. Variables are listed as n (%) unless otherwise specified. Participant data may not add to 589 in cases where demographic data is relevant but was not answered by all respondents (e.g., income, population group). Percents may not total 100 due to rounding. All data in the columns “SK average for adults ≥ 65” is listed as provincial percentages, unless otherwise specified.
Canadian statistic.
Provincial spread is $50,000 to 79,999 as stats Canada presents data in $10,000 increments past $50,000.
Provincial spread is $80,000+.
For exercise leaders, this category refers to the number of days the program runs at their site, not the number of days that they lead.
Communities of >10,000 people.
Exercise leaders were slightly younger than participants, with a mean age of 70 years (range 25–92), and were mainly white (94%), female (94%), current drivers (98%) with no caregiving responsibilities (92%). Urban leaders accounted for 49% of surveys submitted; leaders represented high proportions of widows and people with lower incomes.
Program Density and Geographic Spread Across Saskatchewan Health Regions
About 876/975 (90%) surveys had sufficient information to be geocoded; all 876 responses were retained regardless of complete demographics to get the most comprehensive assessment of number of active programs. Some respondents listed incomplete facility details (for instance, “Condo, Saskatoon”) or listed their program as “online/zoom,” and were excluded from analysis. Of the 99 excluded responses, 54 (55%) were from the Saskatoon region, 17 (17%) were from the Regina region, and 28 (28%) had insufficient details to determine the region. A total of 134 active program locations were listed. By health region, 50 sites (37%) were in the Saskatoon region, 41 (31%) in the Regina region, and 43 (32%) from other health regions. Seventy-four (55%) sites were in urban communities (>10,000 residents).
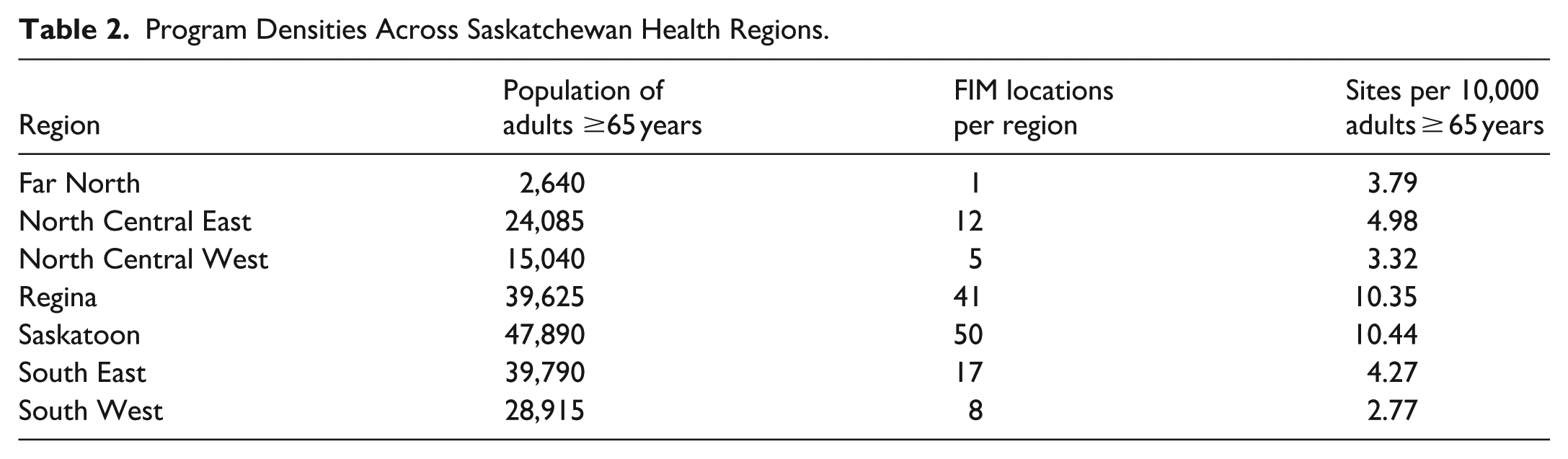
The Saskatoon and Regina health regions had the highest program densities, at 10.44 and 10.35 programs per 10,000 adults aged 65 and over, respectively. The lowest program density was in the Southwest region, at 2.77 programs per 10,000 adults. Program densities are listed in Table 2. Figure 1 displays programs mapped across Saskatchewan. Programs are highly concentrated within the Saskatoon and Regina health regions, with more spread between programs in other regions. There is at least one program in each of the province’s seven health regions. Five of the 12 communities in Saskatchewan with >10,000 people had no FIM programs reported.
Program Densities Across Saskatchewan Health Regions.

Saskatchewan Forever. . .in motion programs within health region boundaries.
Factors Relating to Program Access
Factors within the five dimensions of access are described in Table 3. In the “ability to perceive” dimension, the majority (66%) of participants heard about the program through word-of-mouth and most (89%) joined for health or fitness reasons. Within the “ability to seek” dimension, some participants (23%) agreed that exercising as the only person of one’s gender would prohibit their participation, as well as not knowing anyone in the program (13% agreed). Regarding “ability to reach,” most participants (88%) traveled less than 5 km to reach the program, with 25% of participants attending in the building where they live. Notably, 85% of participants agreed that they would not have joined if it was outside of their town or city. In the “ability to pay” dimension, 23% of participants agreed that a cost to the program would prohibit their involvement. Finally, in the “ability to engage” dimension, 17% of participants agreed that if the exercises were more difficult, they would not have joined the program.
Participant Descriptives on Access to the Forever. . .in motion Program.

Note. n = 589 unless otherwise specified. Percentages may not add up to 100 due to rounding. All Likert-scale questions had 4% or fewer participants select “Not Applicable,” except for item N regarding caregiving support, where 373 (63%) of participants responded, “Not Applicable.”
Two-by-two comparisons between demographic groups and perceived barriers within the four summarized dimensions of access are shown in Figure 2. The dimension which participants endorsed barriers most frequently was “ability to reach,” with 89% of all participants agreeing to at least one barrier. Three significant differences in barriers between bivariate demographic groups were identified. In the “ability to engage” dimension, people 75 years or older were more likely to agree to a barrier compared to their younger counterparts (OR = 2.15, χ2 = 11.15, p = .001). In the “ability to reach” dimension, fewer rural participants agreed to a barrier compared to urban participants (Odds ratio (OR) = 0.35, χ2 = 15.60, p < .001), and people with multiple chronic conditions were less likely to agree to a barrier in this dimension compared to those with 0 or 1 conditions (OR = 0.52, χ2 = 6.18, p = .01).

Perceived barriers to access by demographic characteristics.
Discussion
This study aimed to understand the demographic representation of exercise participants and leaders, the distribution of FIM programs in Saskatchewan and factors related to accessing the program. Overall, the sample of respondents were primarily white females aged 65 and older who were current drivers and who did not have caregiving responsibilities. The sample of exercise leaders and participants also represented a higher proportion of low-income adults and widows compared to provincial averages. Exercise participants were over-representative of urban residents, while exercise leaders were over-representative of rural residents. There was a higher density of programs in the Saskatoon and Regina health regions compared to all other regions, and mapping showed implementation gaps in locations with populations that would warrant programing. The ability to reach dimension had the highest proportion of participants agreeing to at least one barrier, mostly due to a high proportion of participants agreeing that a program outside of their home community would be a barrier. Demographic characteristics largely did not contribute to differences in perceived barriers to access, except that rural residents and people with multiple chronic conditions were less likely to agree to a barrier within the “ability to reach” dimension, and those aged 75 years or older were more likely to agree to a barrier in the “ability to engage” dimension compared to their bivariate counterparts.
The over-representation of white, urban, and female exercise participants in our study is a finding that has been seen in other exercise and health promotion research (Brown et al., 2009; Farrance et al., 2016; Oken et al., 2006). While white and urban residents represent groups that have historically received relative advantage compared to their counterparts, we are encouraged that women, who in other sport or exercise contexts may participate less often than men (Khan et al., 2012), represent a high proportion of participants. The lower proportion of urban exercise leaders may be due to fewer leaders or larger class sizes in urban locations compared to rural, or differences in response rates.
While some equity-deserving groups were well-represented by survey respondents, others such as caregivers, people who do not drive, visible minorities, and rural residents were less represented in our participant sample. Previous health promotion research has placed considerable emphasis on altering behavioral factors to improve participation (Barry, 2021), but an equity lens understands that program or system-level implementation features play a large role in preventing access for some populations (Brownson et al., 2021). The FIM program currently incorporates many features that reduce barriers, such as using low-impact exercises and a supportive group atmosphere at low or no cost (Ades et al., 2017; Bethancourt et al., 2014; Farrance et al., 2016), and these should continue to be emphasized as the program spreads. Conversely, Saskatchewan’s largely rural landscape creates a programing challenge, and other factors such as cultural or gender preferences require further consideration. Future research could involve participatory methods to design programs that reach the various equity-deserving groups that were less represented in this study.
Program densities in the Saskatoon and Regina health regions were at least two times higher than any other regions. Saskatoon and Regina regions are the only regions in Saskatchewan that employ dedicated staff to provide training, support continuous implementation of the program, and purchase exercise supplies. A lack of funding paired with gaps in policy and practice can result in failures in widespread health promotion program implementation (Barry, 2021). In our study, the lack of funding for long-term implementation support in the regions outside of Saskatoon and Regina may be a primary reason for the disparity in program densities seen between regions and for the absence of programing in urban centers where population numbers would warrant programing. More research is needed to determine the effect of disparities in regional healthcare services on older adult health or aging in place.
A recent scoping review by Cu et al. (2021) found that access to healthcare using the Levesque framework has been studied by researchers across many disciplines, from primary care to dentistry and school-based care. To our knowledge, this is the first study to systematically employ Levesque’s framework to understand access to exercise programing. Our findings agree with other research in that the location and distance to the program are major concerns, but other considerations such as cost, time of day, exercise mode, and facility characteristics are also important (Bethancourt et al., 2014; Corscadden et al., 2018; Cu et al., 2021; Royse et al., 2023). We saw few circumstances where participants differed in perceived barriers to access by demographic group. This shows that the participant sample largely endorses the same barriers but might also indicate that the questions in the survey do not account for all the reasons why equity-deserving groups do not participate. We also did not explore differences in barriers by Indigenous or visible minority status due to low proportions of respondents; these populations may experience different barriers to participating and future work is needed to ensure their perspectives are heard. Overall, the largely homogenous sample may not be diverse enough to indicate differences in access by demographic characteristics.
Strengths and Limitations
Our multiple lenses involved in evaluating access to a health promotion program is a notable strength. Through participant demographics, program density calculations, and examining dimensions of access using an existing framework, this work extends our evaluation of health promotion programing beyond the question, “Is the program effective?,” to, “To what extent can diverse populations across broad regions access this program, and as a result, experience its benefits?” Future work could replicate our research strategy in other healthcare contexts to measure and address disparities in service usage.
The high number of survey respondents from across the province is another strength and highlights the strong engagement between our research team and program implementers. It also shows high levels of enthusiasm and support for the program by exercise leaders and participants. A limitation of this work is that we may have excluded participants with limited ability to read and respond in English such as newcomers to Canada or visible minorities. Indigenous participants may also be under-represented. FIM programing in 11 communities of one tribal council in Saskatchewan was occurring at the time of the survey; a representative responded to the leader survey and the programs in that tribal council are included in the program density analysis and mapping, but the communities declined the participant survey and therefore are not represented in the participant sample. Our findings may therefore be limited in their generalizability in contexts different from our sample demographic. Further relationship-building with newcomer or Indigenous communities is necessary to build trusting research partnerships, increase survey engagement and promote a better understanding of program access in these contexts (Hayward et al., 2021).
We could not calculate program response rates for the program density calculations for health regions outside of Saskatoon and Region since the SPRA does not keep active program lists. Based on feedback from local implementers, we believe response rates are well over 50% and might approach 80 to 90% in some regions. The Saskatoon and Regina response rates were 50% and 71% for program sites, respectively; if the response rate was significantly higher in regions outside of Saskatoon and Regina, the true gap in program densities might be even wider.
Conclusion
For many older adults, group-based exercise programs help manage and reduce physical and mental health concerns, provide social connections and foster aging in place. The current FIM system provides opportunities for many older adults to exercise consistently each week and over long periods of time, but not all regions and population groups across the province appear to have proportionate access to the program. Future work could explore the system-wide features of the FIM program that might be adapted to help promote equitable participation and reduce health equity gaps.
Footnotes
Acknowledgements
Special thanks to Kimberly Willison, Marisol Molina-Smith and Candace Yuhacz for helping with participant recruitment.
Ethical Considerations
Ethical approval for this study was obtained from the University of Saskatchewan Behavioral Ethics Board, ethics ID: BEH 4042.
Consent to Participate
All participants read the consent form prior to filling out surveys. Completion of the surveys implied that they consented to participate.
Author Contributions
- WV: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; visualization; writing—original draft; and writing—review & editing.
- DF: conceptualization; methodology; supervision; writing—review & editing.
- HF: supervision; writing – review & editing.
- CM: supervision; writing – review & editing.
- AL: conceptualization; funding acquisition; methodology; supervision; writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a University of Saskatchewan College of Medicine Graduate Student (CoMGRAD) Award and a University of Saskatchewan College of Medicine Research Acceleration and Design (CoMRAD) Award.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Wendy Verity has served as a contracted instructor for exercise leader training for the Saskatchewan Parks and Recreation Association. The remaining authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We are unable to share datasets with researchers outside of our research team. Data is available as grouped means, as per the guidelines on our informed consent documents.