
Abstract
Purpose:
The benefits and harms of medical interventions shift as patients age, calling for re-evaluation of each intervention’s appropriateness and alignment with patients’ preferences. Continued use of medical interventions when harms outweigh benefits is common in older adults with limited life expectancy. This critical review aims to describe the opportunities and challenges of de-implementation in older adults with limited life expectancy, focusing on the role of patient preference and shared decision making.
Findings:
We describe three examples where de-implementation may be considered in older adults with limited life expectancy—cancer screening, polypharmacy, end-of-life care—and the associated de-implementation challenges. The challenges stem from the need to change established behavior and shift from age-based to life expectancy-based decision making. Existing de-implementation frameworks do not incorporate patient preferences whereas shared decision-making frameworks do not consider the challenges specific to de-implementation.
Conclusions:
Significant research gaps exist at the intersection of de-implementation, shared decision making, and aging research. Considerations for de-implementation would benefit from evaluating the preference sensitivity of the decision. This should be informed by the strength of evidence, the extent that the potential harms outweigh the benefits, and whether the intervention is life-sustaining where de-implementation would be irreversible.
Keywords
Introduction
Older age, frailty, accumulation of chronic conditions, and decline in cognitive and/or functional status all increase the risk of complications and treatment burden from medical interventions (Boyd et al., 2019; Hoogendijk et al., 2019). The same factors also diminish the net benefits of some medical interventions because limited life expectancy increases competing risks of morbidity and mortality (Boyd et al., 2019; Hoogendijk et al., 2019; Lee, Leipzig, & Walter, 2013). Medical interventions are considered low value if available evidence demonstrates little to no benefit for the patient or that harms likely outweigh benefits (Chassin, 1998; A. L. Schwartz et al., 2014). Among older adults with limited life expectancy, continued use of medical interventions where the expected time to benefit is longer than the patient’s life expectancy is often considered low value. This is because the patient has minimal chance to accrue the delayed benefit but is exposed to the intervention’s harms and burdens in the short-term (Boyd et al., 2019; Chassin, 1998; Lee, Leipzig, & Walter, 2013; A. L. Schwartz et al., 2014). We describe below three examples of common low-value medical interventions in which harms likely outweigh benefits (Arnold et al., 2018; Deardorff et al., 2023; Earle et al., 2004; Evers et al., 2002; Hanna et al., 2020; Kraut et al., 2022; Lipska et al., 2015; Opondo et al., 2012; Yourman et al., 2023), and for which guidelines recommend de-implementation in older adults with limited life expectancy (Carter et al., 2013; ElSayed et al., 2022; Harris, Wilt, & Qaseem, 2015; James et al., 2013; National Coalition for Hospice and Palliative Care, 2018; Oeffinger et al., 2015; Qaseem, Barry, et al., 2013; Qaseem, Crandall, et al., 2019; Rex et al., 2017; Tschanz et al., 2020; Unger et al., 2020; Wolf et al., 2018).
De-implementation, a planned process that uses targeted strategies to reduce utilization of low-value medical interventions, is an emerging field of implementation science (Norton, Chambers, & Kramer, 2018). Although multiple de-implementation frameworks exist, the unique challenges faced by older adults with limited life expectancy are not adequately addressed. In a recent scoping review, 27 unique de-implementation frameworks and models were identified; only two focused on older adults and both were in the context of deprescribing medications (Walsh-Bailey et al., 2021). Most, including the two that focused on older adults, were process models that provided a step-by-step guide on the process of de-implementation but did not discuss the challenges or barriers to de-implementation, how to overcome those, or considerations specific to older adults with limited life expectancy (Walsh-Bailey et al., 2021).
We provide a critical review of the literature and provide examples of medical interventions where harms likely outweigh benefits in older adults with limited life expectancy. We describe the clinical discussion and decision-making challenges for de-implementation in these examples, highlight the role of patient preference in de-implementation, and offer suggestions for future directions for de-implementation research.
Examples of Medical Interventions Where Harms Likely Outweigh Benefits in Older Adults with Limited Life Expectancy
Cancer over-screening in older adults with limited life expectancy is highly prevalent. Routine screening for breast, colorectal, or prostate cancers can reduce cancer-specific mortality and morbidity, but these potential benefits are delayed for up to 10 years (Ilic et al., 2013; Lee et al., 2012). Older adults with multiple chronic conditions, functional impairment, and limited life expectancy are unlikely to accrue the benefits of screening and are at higher risk for short-term harms of screening (Lee, Leipzig, & Walter, 2013). Regarding breast cancer screening, for example, short-term harms include complications from screening and follow-up tests, psychological stress from false positive results, diverted attention away from existing health conditions and increased time and financial burden, particularly among patients who already have complex care needs and functional limitations (Eckstrom et al., 2012; Guiding Principles for the Care of Older Adults with Multimorbidity: An Approach for Clinicians, 2012; Harris, Wilt, & Qaseem, 2015; Harris, 2016; Lansdorp-Vogelaar et al., 2014; Morris et al., 2015; Saini et al., 2014; Schonberg et al., 2014; Soung, 2014; Walter & Covinsky, 2001; Walter & Schonberg, 2014). Further, breast cancer screening in older women with limited life expectancy can lead to over-diagnosis and over-treatment of cancers that are unlikely to impact mortality or morbidity in a patient’s lifetime (Davies et al., 2018). Despite multiple national guidelines recommending against routine cancer screening in average-risk older adults with limited life expectancy (Carter et al., 2013; Harris, Wilt, & Qaseem, 2015; Oeffinger et al., 2015; Qaseem, Barry, et al., 2013; Qaseem, Crandall, et al., 2019; Rex et al., 2017; Wolf et al., 2018), national screening rates in this group remain high. In a nationally representative sample, adults 75+ who had <10-year life expectancy had screening rates of 38.3% for breast cancer, 47.5% for prostate cancer, and 57.0% for colorectal cancer (Yourman et al., 2023). Although there is no consensus regarding an acceptable rate of over-screening, these current rates are excessively high in older adults with limited life expectancy and warrant reduction. We describe an exemplar patient for whom the harms of breast cancer screening likely outweigh the benefits in Box 1.
Vignette of an exemplar older patient with limited life expectancy for whom the harms of breast cancer screening may outweigh the benefits, and the challenges to de-implementing breast cancer screening.

Medication over-treatment, defined as overly intensive treatment of chronic conditions such as hypertension or diabetes, is another prevalent example of low-value medical intervention in older adults with limited life expectancy. Using diabetes as an example, guidelines recommend more lenient glycemic control in older adults, especially those with poorer health and limited life expectancy (ElSayed et al., 2022). Similar to cancer screening, the benefits from intensive glycemic control takes close to 10 years to accrue but can lead to short-term harms (King et al., 1999; Lee & Kim, 2017). Older adults with limited life expectancies are unlikely to derive benefit from intensive glycemic control but are more susceptible to its harms such as hypoglycemia compared to younger, healthier persons (Miller et al., 2010). Nearly one-fourth of emergency hospitalizations for adverse drug events in U.S. older adults are related to hypoglycemia (Budnitz et al., 2011). Hypoglycemic episodes have also been linked to increased risk of dementia (Huang et al., 2022). Further, over-treatment contributes to overall polypharmacy, which is associated with high risk of drug interactions, treatment burden, and adverse drug events (Jyrkkä et al., 2009; Opondo et al., 2012; Wimmer et al., 2016). Despite these harms, over half of US older adults with diabetes are treated to a hemoglobin A1c of <7% regardless of health status, typically by using hypoglycemia-causing medications (Arnold et al., 2018; Lipska et al., 2015).
High-intensity end-of-life treatments in the last 6 months of life include chemotherapy, intubation and mechanical ventilation, cardiopulmonary resuscitation, tracheostomy, gastrostomy feeding tube placement, hemodialysis, and enteral and parenteral nutrition (Barnato et al., 2009; Earle, Neville, et al., 2004; Earle, Landrum, et al., 2008; Evers et al., 2002; Gallo et al., 2018). There is also evidence that frequent hospitalizations or emergency room visits at the end-of-life can be burdensome for patients and families (Gozalo et al., 2011; Hanna et al., 2020). High-intensity end-of life care has been linked to decreased quality of life and care satisfaction, prolonged bereavement, and increased health utilization and cost (Cheung et al., 2015; Prigerson et al., 2015; Wright, 2008). In contrast, earlier hospice enrollment and avoidance of highly intensive care within 30 days of death were associated with families’ perceptions of better end-of-life care (Wright et al., 2016). National data demonstrate high rates of high-intensity end-of-life treatments and, at the same time, underuse of palliative care and hospice, which have been associated with improved quality of life outcomes (Khandelwal et al., 2017; Morden et al., 2012; Ornstein et al., 2020). For instance, 58% of Medicare beneficiaries with cancer were enrolled in hospice for only an average of 8 days at the end-of-life. In contrast, one quarter of Medicare beneficiaries with cancer were in the intensive care unit in the last month of life and 6% received chemotherapy in the last 14 days of life (Morden et al., 2012). In a nationally representative survey, about one-quarter of Medicare beneficiaries died in the hospital and those who did, compared to those who died at home, were more likely to have their family members report that care in the last months of life was inconsistent with patients’ wishes (Khandelwal et al., 2017).
Benefits and Challenges of De-Implementation in Older Adults with Limited Life Expectancy
De-implementation, defined as discontinuing or reducing the use of low-value healthcare services, is a relatively new area within the field of implementation science (Norton et al., 2018). The goal of de-implementation is to minimize iatrogenic harm and maximize use of resources, which are not only limited to healthcare costs but also patients’ out-of-pocket expenses, time, and effort (Advani & McKay, 2023). De-implementation in older adults with limited life expectancy has the potential to reduce treatment and financial burden on patients and care partners and improve patients’ ability to focus on their personal health priorities.
Clinical Decision-Making Challenges Related to De-Implementation
The challenges of de-implementation have been described in the literature and include systemic, clinician, and patient related factors (Norton et al., 2018; Norton & Chambers, 2020). Here we provide a brief overview of the clinician and patient related factors most relevant to clinical decision making.
De-implementing existing interventions (e.g., stopping routine cancer screening or a long-term diabetes medication) poses unique challenges compared to implementing new interventions (e.g., doing a new diagnostic test or starting a new medication, Table 1; Norton & Chambers, 2020; Parker et al., 2022). De-implementation involves a reversal of behavior that counters existing attitudes and beliefs which have supported the ongoing intervention. Clinicians and patients may not perceive or be aware of the need for de-implementation due to clinical inertia (Pilla, Pilla, Jalalzai, Tang, Schoenborn, Boyd, Bancks, et al., 2023). Even when they are made aware of the option to de-implement, attempting to change established attitudes and beliefs can lead to skepticism and reluctance on the part of both clinicians and patients (Chimonas et al., 2020; Geijteman et al., 2016; Gross et al., 2014; Housten et al., 2022; Norton & Chambers, 2020; Pilla et al., 2022; Piper et al., 2018; Rowe et al., 2021; Schwartz et al., 2004; Zikmund-Fisher et al., 2016). For example, in a survey of 1,054 older veterans, almost half (45.6%) were not comfortable with stopping colorectal cancer screening even if their doctor did not think screening would benefit their health (Piper et al., 2018). In a national survey of physicians, only 4% would deprescribe hypoglycemia-inducing medications in a hypothetical 77-year-old with multiple chronic conditions and functional impairment whose hemoglobin A1c was 7.3% (Pilla, illa, Jalalzai, Tang, Schoenborn, Boyd, Bancks, et al., 2023).
Clinician and Patient Related Challenges in De-Implementation Among Older Adults with Limited Life Expectancy.

De-implementing an existing intervention that has been ingrained over a long period of time may trigger loss aversion on the part of the patient and lead to negative reactions that something is being taken away or withheld (Fraser et al., 2024). Patients and clinicians may also be reluctant to forgo interventions for fear of uncertainty or worse health outcomes (Fraser et al., 2024; Norton & Chambers, 2020; Pilla et al., 2022). Negative health outcomes that are not necessarily related to de-implementation can nonetheless be perceived as an error whereas harm resulting from an intervention is often perceived as an unfortunate but acceptable side effect (Norton & Chambers, 2020). In addition, American social norms equate more care with better care, so stopping medical intervention can be viewed as not caring, giving up, or discrimination (Geijteman et al., 2016; Pilla, Jalalzai, Tang, Schoenborn, Boyd, Golden, et al., 2023; Schoenborn et al., 2016; Shelton et al., 2021). This is especially problematic for groups that historically and/or actively have inadequate access to high-value care. In the context of widely documented healthcare disparities, patients who have experienced unequal treatment and have lower trust in healthcare may perceive de-implementation as a perpetuation of that unequal treatment or be concerned that the definition of low-value care stems from the devaluation of their lives. These challenges, coupled with potentially misaligned incentives for clinicians and clinicians’ fear of medical malpractice (Schoenborn et al., 2016), can be strong motivations against de-implementation.
De-Implementation Challenges Specific to Older Adults with Limited Life Expectancy
De-implementing medical interventions in older adults with limited life expectancy poses additional challenges. First, some medical interventions are considered low value only in older adults with limited life expectancy but are still appropriate for healthy older adults. This conditional de-implementation can be much more challenging to operationalize and explain to patients due to competing messages within public health and healthcare systems that encourage the same interventions, for example, cancer screening and intensive control of chronic conditions. Such competing messages can cause confusion for patients and families, accentuating the feeling of “taking away” or “giving up.” For example, one-third of older adults in a study on deprescribing diabetes medications were confused about why one would allow less intensive glycemic control: “It would be counterintuitive to everything [my doctor] has been saying for 25 years. . . It’s a hypothetical that I just can’t relate to” (Pilla et al., 2022). Conditional de-implementation also raises concerns for the potential of exacerbating health disparities, specifically that prediction algorithms for life expectancy may introduce bias when the cause for lower life expectancy prediction is due to social determinants of health rather than biological differences. In a national survey of 791 physicians, although 75% supported stopping cancer screening in older adults with limited life expectancy, 48% worried that doing so would introduce bias against racial/ethnic minorities and 52% worried that doing so would introduce bias against those with low socioeconomic status (Schoenborn, Boyd, & Pollack, 2022).
Another challenge is that the threshold for conditional de-implementation is based on limited life expectancy, a topic that clinicians are reluctant to discuss, and many patients are resistant to hearing, especially outside of a trusting, established relationship (Schoenborn, Bowman, et al., 2016; Schoenborn, Lee, et al., 2017; Schoenborn, Janssen, et al., 2018). Although there are a growing number of prognostic tools to help clinicians estimate life expectancy, the tools are not routinely incorporated into clinical workflows (Schoenborn, Bowman, et al., 2016). Clinicians report skepticism about the accuracy of these tools even though the tools have similar measures of accuracy as other commonly used predictive tools in clinical practice, such as the atherosclerotic cardiovascular disease (ASCVD) risk calculator (ePrognosis, n.d.; Schoenborn, Boyd, & Pollack, 2022). Additionally, older adults, especially those with limited life expectancy, frequently involve care partners (e.g., family, friend) in their health decisions (National Research Council [US] Committee on the Role of Human Factors in Home Health Care. The Role of Human Factors in Home Health Care: Workshop Summary. Washington [DC]: National Academies Press [US], 2010). Decision making may be more complex when the beliefs and expectations of both the patient and their care partners need to be considered (Green et al., 2019). Lastly, although there is always uncertainty when applying population-level evidence to individual patients, the degree of such uncertainty is greater for older adults who have often been excluded from clinical trials. These unique challenges of de-implementing medical interventions in older adults with limited life expectancy are illustrated in Box 1.
The Role of Patient Preference and Shared Decision Making in De-Implementation
Patient Preference is Not Currently Incorporated in De-Implementation Frameworks
Box 1 illustrates a dilemma in de-implementation efforts in older adults with limited life expectancy—that is, when patient prefers to continue the medical intervention after being informed of the rationales for de-implementation. Among de-implementation frameworks and models to date, patient preference is rarely addressed (Table 2; Walsh-Bailey et al., 2021). A scoping review identified that some de-implementation strategies incorporated communication tools to facilitate shared decision making but we did not find any de-implementation frameworks that explicitly addressed or included shared decision making or patient preference (Ingvarsson et al., 2022). The frameworks identify targets for de-implementation based on research or guidelines. Patient beliefs and attitudes are viewed through the lens of barriers or facilitators for de-implementation and patient education and engagement are used to achieve de-implementation but not to establish whether de-implementation is appropriate (Norton, Chambers, & Kramer, 2018; Norton & Chambers, 2020; Sypes et al., 2020; Walsh-Bailey et al., 2021).
Key Components of De-Implementation and Shared Decision-Making Frameworks.

Situations where harms outweigh benefits only when life expectancy is limited and there may be uncertainty in the evidence.
The Importance of Patient Preference and Shared Decision Making
Respecting patient preference has been recognized as an integral element of patient-centered care (Barry & Edgman-Levitan, 2012). Patient preference is especially important when there is uncertainty in the evidence (Thériault et al., 2020), and/or when the benefits and harms of the intervention are dependent on patient values, both of which are relevant in decision making among older adults with limited life expectancy. For example, in end-of-life care, the meaning of a “good death” has significant cultural and personal variations (Cottrell & Duggleby, 2016; Hauschildt, 2022). A preference for more intensive interventions that are not clearly futile, after being fully informed of the benefits and harms, should be respected. Failing to do so could be deeply disrespectful and contribute to marginalizing patients and families with different values and preferences.
Eliciting and supporting patient preference is central in frameworks on shared decision making. Shared decision making has traditionally been used to engage and support patients to decide between healthcare options that are in equipoise or preference-sensitive, defined as situations in which one option is not considered superior to another, but the decision rather depends on individuals’ personal values regarding the tradeoffs inherent in each option (Elwyn, Frosch, & Rollnick, 2009; Elwyn, Frosch, Thomson, et al., 2012). Compared to de-implementation frameworks, shared decision-making frameworks view patient preference as central to decision making and include explicit steps for eliciting, clarifying, and supporting patient preferences (Elwyn, Frosch, Thomson, et al., 2012).
How to Consider Patient Preference and Shared Decision Making Within De-Implementation of Low-Value Interventions is Not Clear
There is no clear guidance in the literature on how to consider patient preference or shared decision making in de-implementation of low-value medical interventions in older adults with limited life expectancy. In fact, recommendations are contradictory.
One article suggested that de-implementation and shared decision-making strategies have fundamental differences and can be at odds with each other. When a low-value intervention is conditional (i.e., allows for exceptions in some patients) or when there is uncertainty in the evidence, the authors suggested that de-implementation was not appropriate and shared decision making should be used (Riganti et al., 2023). However, as discussed above, all examples of low-value interventions in older adults with limited life expectancy are conditional and involve uncertainty. Further, as outlined in Table 1 and illustrated in the vignette (Box 1), these decisions involve reversal of social norms and established beliefs, attitudes, and behaviors and, as such, can be challenging scenarios for applying conventional shared decision-making frameworks. For example, multiple studies demonstrate that older adults view cancer screening as a moral obligation and not a healthcare decision (Gram et al., 2023; Torke et al., 2013). Others argue that shared decision making is probably not the appropriate approach in these scenarios because of the lack of equipoise, given that there is evidence suggesting harms likely outweigh the benefits (Elwyn, Price, et al., 2022; Thériault et al., 2020). How to best incorporate shared decision making in de-implementation strategies is not known.
How Do We Move Forward—Recommendations for De-Implementation in Older Adults with Limited Life Expectancy
We suggest that de-implementation of medical interventions in older adults with limited life expectancy acknowledge both the challenges of de-implementation and the importance of patient preference. First, we propose that key tenets from shared decision making—understanding patients’ lived experiences, values, and priorities—should be applied in all de-implementation discussions with older adults with limited life expectancy, with attention to highlighting specific harms and burdens that may be unique or accentuated. For example, the opportunity costs of low-value medical interventions and the distraction from other more impactful health issues may be magnified among older adults with limited life expectancy. A low-value intervention such as intensive diabetes treatment can result in treatment burden (e.g., multiple laboratory tests and medical appointments) and side effects (e.g., hypoglycemia) that in turn can distract from appropriate treatment of other conditions that limit quality of life and function. Another important consideration is the concept of “time toxicity,” that time spent in scheduling, traveling, and receiving interventions is a valuable resource on the part of the patient and families and should be considered in decision making (Gupta et al., 2024). This is particularly relevant in patients with limited life expectancy.
Next, we posit that there is a range of preference sensitivity with regards to decisions about medical interventions in older adults with limited life expectancy. Preference sensitivity is often depicted in literature as binary, where those decisions that involve options with equipoise in the benefits and harms are considered preference sensitive (Elwyn, Frosch, & Rollnick, 2009; Elwyn, Frosch, Thomson, et al., 2012). We propose that preference sensitivity is better conceptualized as a continuous spectrum where patient preference should carry more weight in more preference-sensitive decisions while efforts should be directed to discouraging interventions that are less preference-sensitive and low-value (Figure 1). We clarify that, as stated above, shared decision-making strategies regarding eliciting and discussing patient preferences should be applied regardless of preference sensitivity. Rather, the preference sensitivity of the decision helps to inform the magnitude of behavior change efforts.

Proposed framework for considering preference sensitivity in de-implementation decisions among older adults with limited life expectancy.
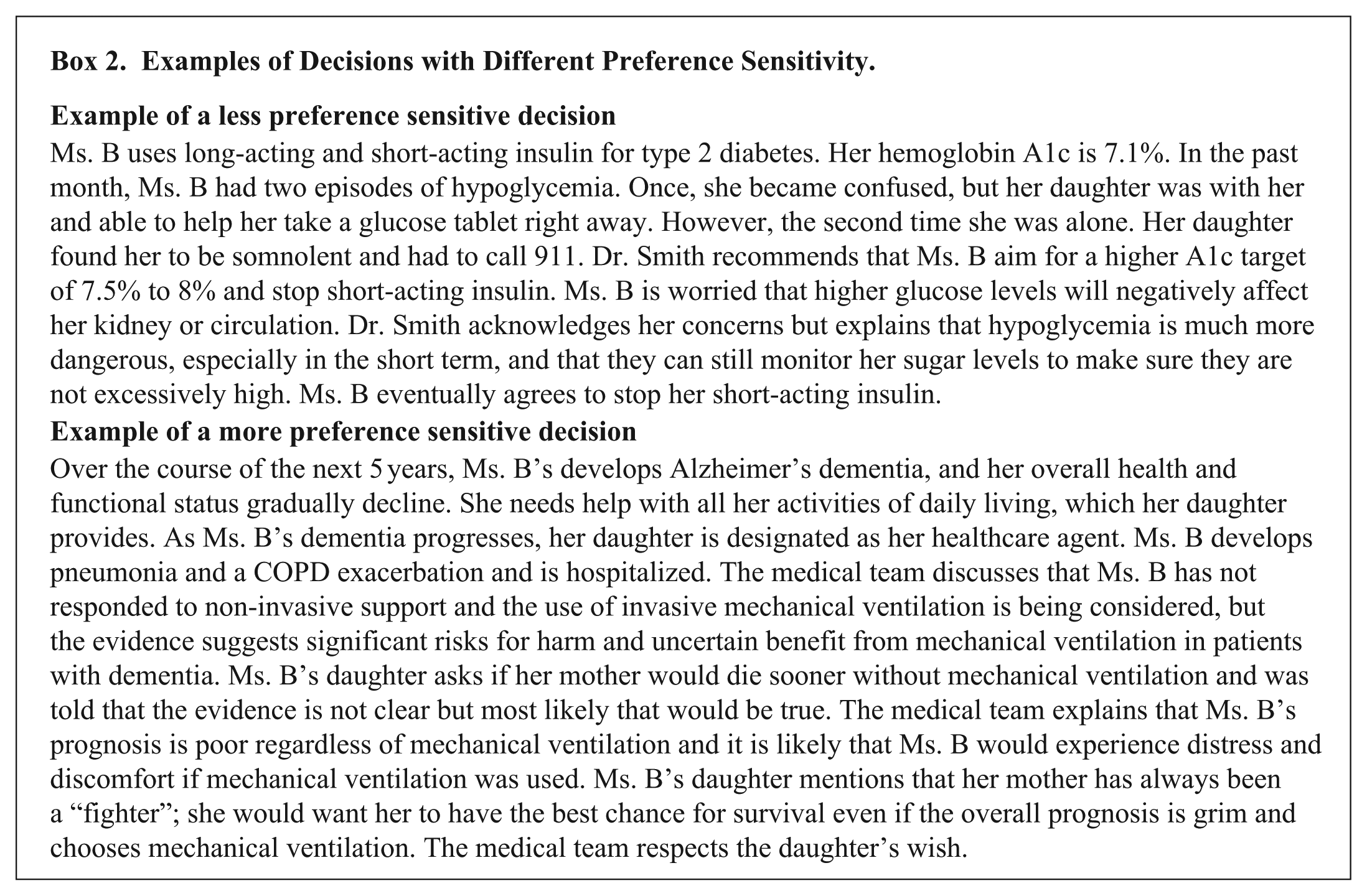
We suggest that three considerations are relevant to determining the preference sensitivity of a decision (Figure 1); these include: (1) the strength and certainty of evidence—specifically for patients with limited life expectancy; (2) the extent and gravity of potential harms from the intervention relative to the potential benefits; and (3) whether the intervention is life-sustaining where de-implementation would be irreversible. First, when the strength and certainty of evidence for ineffectiveness or harm of an intervention is strong, the decision should be less preference-sensitive and more geared towards de-implementation. For example, the ineffectiveness and harm from tube feeding in patients with advanced dementia is well-documented in the literature (American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee, 2014). Therefore, relative to other invasive interventions, feeding tube placement in patients with advanced dementia is less preference sensitive. Second, when the potential for harm from an intervention is greater and/or when the gravity of the harm is more severe and the potential benefit is minimal and/or highly unlikely, the decision should be less preference sensitive, leaning towards de-implementation. For example, benzodiazepine use for insomnia in older adults have well-established and significant risks, including falls, hip fractures, memory loss, confusion, and motor vehicle crashes, whereas the benefits are negligible (American Geriatrics Society Beers Criteria® Update Expert Panel, 2023; Glass et al., 2005). These adverse events have been described after older adults have been exposed to benzodiazepines for as few as five nights (Glass et al., 2005). Therefore, compared to medications that have less significant or less immediate harms, de-implementing benzodiazepines is less preference sensitive. Lastly, we consider life-sustaining interventions to be more preference-sensitive because of the inherent irreversibility and gravity of the decision and because death and dying are deeply intertwined with one’s cultural, racial/ethnic, and spiritual traditions and values. We continue the vignette about Ms. B to illustrate decisions with variable preference sensitivity (Box 2).
Examples of Decisions with Different Preference Sensitivity.
Implications and Suggestions for De-Implementation Research
Outcome Selection in Research
Given the preference sensitivity of decision making in older adults with limited life expectancy, outcome measures in research need to account for this complexity. Outcomes focused solely on de-implementation may mis-categorize respecting patient choice in a preference sensitive decision as failure to de-implement. For example, a recent publication found that interventions aimed at improving advance care planning increased “potentially burdensome care” (Wolff et al., 2024), raising questions about whether the current definition of “potentially burdensome care” is aligned with patients’ preferences and goals (Santoyo-Olsson, Li, & Harrison, 2024). On the other hand, outcomes focused solely on shared decision making may fail to capture overuse of low-value care when the decision is less preference sensitive. We suggest that de-implementation research consider both utilization outcomes (e.g., reduced use of low-value interventions) and shared decision making-related outcomes (e.g., goal-concordance and decisional quality).
There is also growing recognition that the costs and harms of low-value interventions are not currently measured in a comprehensive and patient-centered way. For example, financial toxicity and time toxicity related to medical interventions are relatively new measures of harm that are mostly being studied in cancer care, but the same concepts are also relevant to all older adults with limited life expectancy (Gupta et al., 2024; McDermott, 2017). It is important to better quantify such costs and burdens to everyone involved in the context of testing or treatment cascades that often result from low-value interventions.
Additional Research Gaps
Clinician decision support tools and patient decision aids are evidence-based tools that can help raise awareness of the option for de-implementation, provide point-of-care resources on the benefits and harms of an intervention, and help enhance patient knowledge, self-efficacy and value clarification (Stacey et al., 2017; Sutton et al., 2020). However, tools designed for older adults with multiple chronic conditions and limited life expectancy are rare and needed. For example, a breast cancer screening decision aid for older women included information about competing mortality risks from multiple chronic conditions and presented individualized screening benefits by predicted life expectancy (Schonberg, Kistler, et al., 2020).
Another important gap is the need for broader messaging that can raise public awareness of the changing benefit/harm balance of interventions over time and familiarize the public with the concept of de-implementation. A recent literature review highlighted the lack of public messaging as a significant intervention gap in deprescribing (Fried et al., 2024). Our recent work tested a message aimed at raising awareness about breast cancer over-screening in older women. We found that messaging can improve support for screening cessation, and lead to more careful deliberation about the screening decision and increased interest in seeking information about the benefits and harms of screening (Schoenborn, Gollust, Nagler, et al., 2024; Schoenborn, Gollust, Schonberg, et al., 2024). More of this type of work is needed in other decisional contexts.
More efforts are needed to integrate and implement prognostic tools into routine clinical practice and address barriers to use among clinicians. Policies are also needed to incentivize clinicians for potentially lengthy, longitudinal discussions around these decisions to prevent low-value care.
Summary and Conclusions
In summary, the balance of benefits and harms of medical interventions change with older age, worse health and function and limited life expectancy. Multiple medical interventions pose more harm than benefits in older adults with limited life expectancy and should be considered for de-implementation. However, patient preference needs to be central in de-implementation, especially when the evidence is more uncertain, harms are more grave, or when the intervention is life-sustaining. Numerous research gaps exist that must be addressed to ensure high-value care for older adults with limited life expectancy.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.