
Abstract
Objectives:
This study investigated the longitudinal relationship between participation in Cognitively Stimulating Leisure Activities (CSLAs) and the risk of Alzheimer’s Disease and Related Dementias (ADRD) in two different groups of older adults with and without Mild Cognitive Impairment (MCI).
Methods:
We analyzed data from the Health and Retirement Study, a nationally representative survey of adults in the United States from 2012 to 2020 (MCI = 14,280; without MCI = 13,695) using a Generalized Estimated Equation. The Telephone Interview for Cognitive Status-27 was used to identify samples with MCI, with scores ranging from 7 to 11.
Results:
Study findings show that CSLA participation was associated with a reduced probability of reporting the presence of ADRD in both groups. Older adults both with and without MCI who frequently participated in CSLAs were less likely to develop ADRD over an 8 year timeframe.
Conclusions:
Our study findings suggest that CSLAs can serve as an effective intervention to reduce the risk of developing ADRD. Importantly, our findings suggest that CSLAs have a higher probability of reducing the incidence of ADRD in older adults who are experiencing MCI than those who are not.
Keywords
Introduction
Delaying cognitive decline and improving cognitive functioning have long been a central focus in aging research (Centers for Disease Control and Prevention [CDC], 2021). Older adults with mild cognitive impairment (MCI) are considered a vulnerable group at risk of developing Alzheimer’s disease and Related Dementias (ADRD; Alzheimer’s Association, 2023). Recent studies have indicated that over 20% of older adults with MCI are at increased risk of developing ADRD within 2 to 5 years (Koliatsos, 2016; Sanford, 2017; Vemuri et al., 2011). Thus, older adults with MCI report higher levels of psychological challenges and concerns such as depression and loneliness (Campbell et al., 2013; Langa & Levine, 2014; Petersen, 2011).
According to the cognitive reserve theory, cognitive reserve is an important factor in strengthening cognitive function against the effects of normal and pathological aging (Scarmeas & Stern, 2004; Stern, 2002). Participation in various types of leisure activities serves as an important catalyst in improving cognitive reserve and subsequently delaying cognitive decline and the onset of dementia (Clare et al., 2013; Gunning-Dixon & Raz, 2000; Lövdén et al., 2013). The literature shows that leisure activity interventions and programs prevent and delay cognitive impairment and MCI degeneration among older adults (Ball et al., 2018; Kulason et al., 2016; Stern & Munn, 2010).
Among various types of leisure activities, Cognitively Stimulating Leisure Activities (CSLAs) are defined as any activities that require a mental response from active participation in pursuits such as reading books, writing, playing board games, and watching movies and television (Huang et al., 2015; Wilson et al., 2013). Prior studies have found that frequent CSLA participation during mid or later life has been associated with better cognitive functioning, slower cognitive decline, and a lower risk of cognitive impairment (Carlson et al., 2009; Gidicsin et al., 2015; Reed et al., 2011; Wilson et al., 2002). Specifically, weekly engagement in reading, writing, puzzles, and artistic activities has been associated with higher working memory performance, memory, and visuomotor speed (e.g., attention and processing speed; Hertzog et al., 2008; McAuley et al., 2004). While there are underlying similarities between sedentary activities and CSLAs based on the metabolic equivalent of task measurements below 1.5 (Tremblay et al., 2017). CSLAs require participants to stimulate specific cognitive domains including memory, working memory, and information processing (Kesse-Guyot et al., 2012).
Despite the importance of CSLAs in preserving cognitive function in later life, little research has been conducted to investigate and compare the effects of CSLAs on the risk of ADRD in older adults with and without MCI. In this study, we investigated the longitudinal relationship between CSLA participation and the prevalence of ADRD in older adults (those with and without MCI. The results of this investigation provide evidence related to the optimal amount of CSLA participation needed to reduce ADRD risk, and provide practical implications for developing differentiated CSLA programs for older adults with and without MCI.
Methods
Data Source
This study used five waves (2012–2020) of the Health and Retirement Study (HRS) Core data, a national longitudinal study of community-dwelling older adults aged 50 and above in the United States that spanned the years 2012, 2014, 2016, 2018, and 2020. The HRS, conducted through biennial surveys administered via telephone or face-to-face interviews, a comprehensive dataset comprised of multidomain aging research data that includes health status, cognitive functioning, leisure behaviors, biomarkers, and socio-economic status. HRS self-reported data are collected through a self-administered paper-and-pencil survey and in-depth phone interviews.
Data Reliability
The HRS collected data employing Patient-Reported Outcome (PRO) and Proxy-Measured Outcome (PMO) methodologies. The determination to use PRO of PMO was made by the HRS interviewer, based upon the responsiveness of the interviewee. If the interviewee exhibited consistent responsiveness to the questionnaire, the interviewer selected PRO. However, if the interviewee was unresponsive or unreliable in answering the questions, the interviewer used PMO, which involves support from caregivers. Consequently, PRO data indicates that interviewees could autonomously respond to the questions that allows users of the data to anticipate the reliability of PRO responses. Conversely, respondents that required a PMO approach can be regarded as providing dependable answers, regardless of whether they have received a diagnosis of dementia.
Study Sample
We formed two distinct groups within our study sample to fulfill our main research objectives: older adults living with MCI and older adults without MCI. The HRS utilizes a single cognitive assessment strategy, namely the Telephone Interview for Cognitive Status-27 (TICS-27). A TICS-27 score of 6 or below indicates the presence of dementia, while a score in the range of 7 to 11 suggests cognitive impairment without meeting the dementia threshold, which is commonly referred to as MCI. Scores falling between 12 and 27 are deemed within the normal range of cognitive status (Crimmins et al., 2012; Herzog & Wallace, 1997; Y. Lee et al., 2019). Therefore, the sample for this study was comprised of an MCI group ranging the score from 7 to 11 and a without MCI group ranging from 12 to 27 on the TICS-27.
The TICS-27 test includes three cognitive tests: memory, working memory, and attention and processing speed. Memory was assessed through both immediate and delayed recall tests. In the immediate memory test, participants were tasked with remembering as many words as possible from a list of 10 random words (e.g., coffee, apple, flower). Subsequently, in the delayed memory test, participants were required to recall as many words as they could after a 5-min interval had passed. Each correctly recalled word earned one point on the test, which had a scoring range of zero to 20 points for both recall tests. The working memory domain assessed the capacity of participants to process and store information simultaneously. A seven-stage subtraction test was employed for measuring working memory, wherein participants continuously subtracted seven from 100 in five increments (e.g., 100–7 = 93, 93 −7 = 86, 86–7 = 73). The test had a total possible score of five for five correct answers. To evaluate attention and processing speed, a reverse counting test was administered (Ofstedal et al., 2005; Williams et al., 1996). Participants were instructed to count backward from 20 in 10 continuous numbers in two trials (e.g., 20, 19, 18, 17). Each correct trial scored one point, contributing to a total possible score of two. Thus, the total score of the TICS-27 test ranges from zero to 27.
Instruments
Independent Variable
The psych-social data section of the HRS includes 21 types of leisure activities. CSLA criteria are referenced in multiple previous studies based on HRS data (Kim, Lee, Kim, & Park, 2022; J. Lee et al., 2022). We selected and used nine CSLA items: “Read books, magazines, newspapers?,” “Do word games such as crossword puzzles or scrabble?,” “Play cards or games such as chess?,” “Do writing?,” “Do educational training courses?,” “Make clothes, knit?” A seven-point Likert scale ranging from one = “Daily” to seven = “Never” was used to measure how often participants engaged in the intellectually stimulating activities. We reverse-coded (i.e., one = “Never relevant”, seven = “Daily”) to produce a high score indicating a high CSLA engagement (Kim, Lee, Kim, & Park, 2022; Kim, Lee, Ko, & Min Oh, 2022; J. Lee et al., 2022; Liu et al., 2021; Rimmele et al., 2009). The sum of the nine types of CSLA participation was calculated annually. The CSLA participation as an independent variable consisted of five time indexes (i.e., 2012, 2014, 2016, 2018, 2020), that encompassing participant CSLA participation during five different time frames.
Dependent Variable
Our study sample included individuals diagnosed with either Alzheimer’s disease or related dementias between 2012 and 2020, and only consistent responses to questionnaires about diagnosis history from respondents were used to satisfy the reliability and validity of the inclusion criteria. The diagnosis responses needed to be consistent and in the correct order, such as confirming a dementia diagnosis both in an earlier and later year.
Two questions were used to screen for individuals with ADRD. The Alzheimer’s disease questionnaire inquired whether participants had ever been informed by a doctor that they had Alzheimer’s disease that could be answered either “Yes” or “No” (coded as one for diagnosed, zero for non-diagnosed). Similarly, the dementia question asked participants whether a doctor had ever informed them that they had dementia, senility, or any other significant memory impairment, with responses recorded as “Yes” or “No” (coded as one for diagnosed, zero for non-diagnosed). Recognition that ADRD occurred was made if participants answered “Yes” to either question, aligning with a previous study that conducted a regression model to calculate the risk of ADRD in older adults (Y. Lee et al., 2019).
Covariates
Age and sex were included in the covariance to control confounders that might affect the analysis. Covariance analysis is used not only to reveal the relationship between a covariate variable and the dependent variables but also to control for the effects of the covariates in the analysis (Moyle & Murfield, 2013; Strawbridge & Wallhagen, 1999).
Analysis
In the first step, we explored the demographic characteristics of participants with and without MCI. Secondly, a regression model was tested to investigate the relationship between the predictors and the dependent variable based on the Wald Chi-square value, after confirming that the coefficient was not zero. Lastly, we conducted a Generalized Estimating Equation (GEE) analysis to examine the odds ratio (OR) of ADRD within a 95% Confidence Interval (CI) based on the CSLA participation, in our comparison of the MCI and the non-MCI groups. The use of GEE was based on the following assumptions: (a) the responses by study participants are dependent within subjects and independent between subjects, with within-subject dependencies estimated as part of the correlation matrix; and (b) GEE emphasizes the population average effect rather than focusing on subject-specific random effects. We used GEE because the HRS has tracked participants and collected data since 1992, which allowing us to focus on the population average effect. The analysis was conducted using SPSS 28 statistical software. The regression equation used was as follows:

Results
Table 1 provides an overview of the demographic characteristics of study participants. The merged longitudinal dataset is divided into two groups: MCI and without MCI. The with MCI group was composed of 14,280 participants (total cases: 39,260) and the without MCI group was composed of 13,695 participants (total cases: 39,963). At baseline (2012), participants with MCI were 39.8% male and 60.2% female and ranged from 50 to 109 years of age (M = 74.4). Over half of participants reported being married (58.2%), while 18.2% reported being divorced, and 6.6% widowed. Nearly half of study participants reported having either a partial university education (20.1%) and or a university degree (28.1%). 1.5% of participants with MCI reported having been diagnosed with Alzheimer’s disease (n = 215) and 2.8% reported having been diagnosed with a related dementia (n = 399) from 2012 to 2020. Among the participants without MCI, 0.9% reported having been diagnosed with Alzheimer’s disease (n = 123), and 1.4% having been diagnosed with a related dementia (n = 191). The total number of participants diagnosed with ADRD included 600 with MCI (4.2%) and 301 without MCI (2.2%). For the independent variable (CSLA), participants with MCI (M = 10.01, SD = 16.0) and those without MCI (M = 11.8, SD = 17.7) are reported, noting that CSLA scores ranged from 0 to 63.
Study Characteristics by MCI Status.
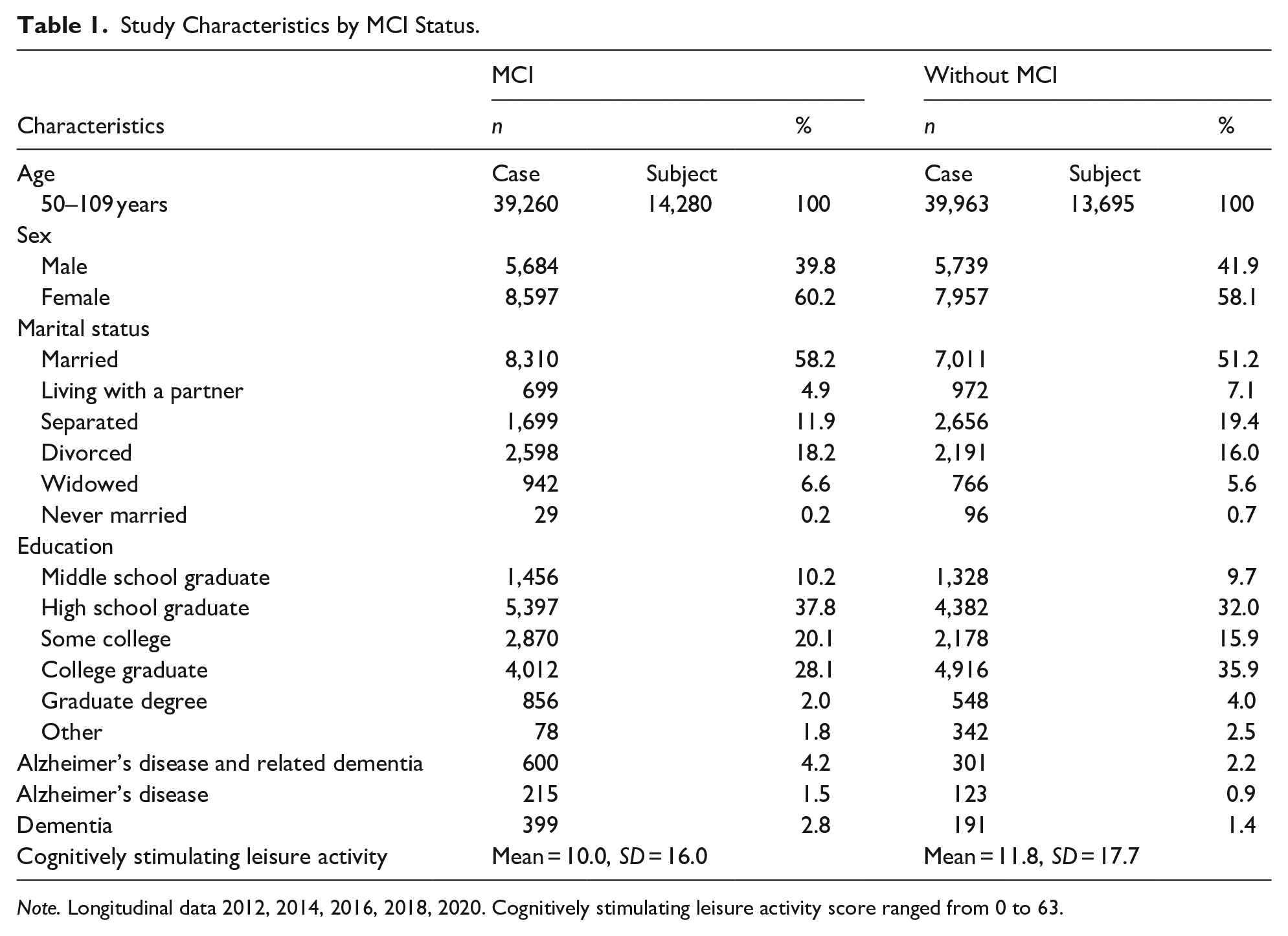
Note. Longitudinal data 2012, 2014, 2016, 2018, 2020. Cognitively stimulating leisure activity score ranged from 0 to 63.
Table 2 summarized the regression model test. Among the MCI group, index (Wald Chi-square = 17.37, df = 4, p < .05), CSLA (Wald Chi-square = 138.28, df = 37, p < .05), age (Wald Chi-square = 5.90, df = 1, p < .05), and sex (Wald Chi-square = 1.60, df = 1, p > .05). For the without MCI group, index (Wald Chi-square = 276.12, df = 4, p < .05), CSLA (Wald Chi-square = 2,203.19, df = 36, p < .05), age (Wald Chi-square = 13.31, df = 1, p < .05), and sex (Wald Chi-square = 0.00, df = 1, p > .05).
Regression Model Tests Between With MCI and Without MCI .

Note. CSLA = cognitively stimulating leisure activity; MCI = mild cognitive impairment.
p < .05.
Table 3 describes the result of the regression analysis of the participants with MCI. First, we investigated the impact of different years on the risk of ADRD with 2012 serving as the reference year. The intercept is significant, indicating that the baseline OR of the ADRD in 2012 is low (OR = 0.03; Wald = 263.84, 95% CI [0.02, 0.05]). For the subsequent years, none of the coefficients from 2014 to 2020 were significant. The OR for 2020 is slightly below one, suggesting a minor decrease in ADRD risk compared to 2012, but this change is not statistically meaningful. Second, we determined the longitudinal impact of CSLA on the OR of ADRD, while considering the covariates of age and sex. Multiple CSLA participation levels were significantly associated with reduced risk of ADRD, providing evidence that higher engagement in CSLA lowers the risk. The lowest OR was 0.29 when the respondent had a CSLA value of 44 (Wald: 7.61; 95% CI [0.12, 0.71]), which means that participants will experience the lowest risk of ADRD when their CSLA engagement is score of 44. Age was found to be a significant estimator (OR = 1.02, Wald: 5.90; 95% CI [1.00, 1.04]), indicating that the risk of ADRD increases with each additional year of age. In contrast, sex was not found to significantly influence the risk of ADRD (p > .05, Wald: 1.59).
The Risk of Alzheimer’s Disease and Related Dementias in Individuals With MCI.

Note. CSLA = cognitively stimulating leisure activity; MCI = mild cognitive impairment; CI = confidence interval.
p < .05.
Table 4 summarizes the result of the regression analysis of participants without MCI. First, our findings indicate that the risk of ADRD significantly decreased from 2012 to 2020 (OR = 0.24, Wald: 63.71; 95% CI [0.17, 0.34]), with each subsequent year showing a lower OR compared to the baseline year of 2012. Second, we found that engagement in CSLA was not significantly associated with varying levels of risk reduction, except for CSLA scores of 37 (Wald: 5.81; 95% CI [0.13, 0.81]) and 38 (Wald: 3.61; 95% CI [0.27, 1.02]). We did determine that age was a significant predictor, with the risk of ADRD rising as individuals aged (OR = 1.01, Wald: 13.31; 95% CI [1.00, 1.02]). However, sex did not have a significant impact on ADRD risk (Wald: 0.01; 95% CI [0.85, 1.16]).
The Risk of Alzheimer’s Disease and Related Dementias in Individuals Without MCI.

Note. CSLA = cognitively stimulating leisure activity; MCI = mild cognitive impairment; CI = confidence interval.
p < .05.
Discussion
We investigated the longitudinal impact of CSLA engagement on the risk of ADRD among older adults with and without MCI. Among participants with MCI, higher CSLA participation were significantly and linearly associated with a reduced risk of ADRD in the MCI group with the lowest OR (0.29) at a CSLA score of 44, and an increased risk for ADRD with advancing age. In contrast, among participants without MCI, most CSLA engagement were not significantly associated with a reduction in ADRD risk, but age increased ADRD risk without a significant impact of sex. These findings highlight the protective role of CSLA engagement in reducing ADRD risk, especially for individuals with MCI, and emphasize the importance of age as a risk factor, suggesting that clinical interventions could be beneficial in mitigating the ADRD risk of older adults, particularly those with MCI (Appendix 1).
Recent research has shown that MCI is potentially reversible, with 44% of participants returning to a normal cognitive state after engaging in an intervention for 1 year (Belleville et al., 2007; Fitzpatrick et al., 2009; Ngandu et al., 2015). The findings of these studies provide evidence of the importance of interventions in maintaining and improving the cognitive performance and cognitive function of older adults with MCI. The results of our study suggest that the design and implementation of CSLA interventions have the potential to reduce the probability of progressing to ADRD by older adults with MCI.
The findings of some prior studies have indicated that frequent participation in leisure activities serves as a potential protective factor against the risk of dementia (Buchman et al., 2018; Verghese et al., 2003), on the other hand, other studies have reported no significant relationship between leisure activity engagement and the progression of ADRD (Kivimäki et al., 2019; Vemuri et al., 2014). The findings of our study support the concept that CSLA participation as a type of leisure activity may serve as a catalyst for decreasing the risk of ADRD development among older adults, and especially for older adults with MCI. Our findings extend the body of literature that leisure activities like CSLA participation play an important role in reducing the progression of ADRD in older adults.
Substantial evidence has established that cognitive training programs and cognitively intensive activities play an essential role in promoting the cognitive functioning and performance of older adults (Hill et al., 2017; Liu et al., 2021). While we focused on CSLA participation in the context of leisure activities, our findings support the findings of previous studies that provided evidence that CSLA participation can maintain or promote cognitive functioning that decrease the risk of ADRD onset in older adults. This finding is significant as it suggests that therapists and healthcare providers working with the geriatric population should recommend a variety of cognitive-related activities as a way of decreasing the risk of ADRD development.
There are several limitations inherent to our study. First, this study did not account for all potential confounding variables that may affect the relationship between CSLA participation and the risk of AD/ADRD. Factors such as respondents’ functional limitations, demographic characteristics linked to AD/ADRD risk (e.g., race/ethnicity and education), and living environments (e.g., assisted living facilities, private homes, or nursing homes) could affect both access to CSLA and the AD/ADRD risk. Future studies are encouraged to apply machine learning approaches, such as deep neural networks and random forest algorithms, to better analyze the complex structure of confounding variables. This would allow for a more comprehensive understanding of how socioeconomic status, cultural background, and comorbidities influence the relationship between CSLA participation and dementia risk. Second, this study did not distinguish between different subtypes of MCI or types of dementia, despite the known heterogeneity in symptoms and progression patterns. Given that preferences for CSLA participation may differ based on the type or severity of cognitive impairment, future research should conduct more detailed comparisons across various subtypes of MCI and dementia. Third, we did not incorporate baseline cognitive functioning for either MCI or non-MCI participants. As baseline cognitive status may influence both the motivation of engaging in CSLA and the risk of developing AD/ADRD, future studies should consider incorporating cognitive function as a covariate or weighting factor to allow for more accurate analyses.
Despite these limitations, we have successfully explored the relationship between CSLA participation and the likelihood of self-reported ADRD among older adults with and without MCI. Overall, frequent CSLA participation has been shown to be effective in decreasing the probability of ADRD onset, especially in older adults with MCI, which suggests that various types of CSLA participation can be an important addition to therapeutic programs for older adults that are designed to reduce the probability of ADRD progression. Thus, therapists and healthcare providers can use the new knowledge generated in this study to design and implement effective CSLA-based dementia prevention interventions for older adults with different levels of cognitive impairment.
Footnotes
Appendix
These First Questions Are About the Activities in Your Life Now. Please Tell Us “How Often You Do Each Activity.”.

| Care for a sick or disabled adult? | Daily | Several times a week | Once a week | Several times a month | At least once a month | Not in the last month | Never/ Not relevant |
|---|---|---|---|---|---|---|---|
| Do activities with grandchildren, nieces/nephews, or neighborhood children? | |||||||
| Do volunteer work with children or young people? | |||||||
| Do any other volunteer or charity work? | |||||||
| *Attend an educational or training course? | |||||||
| Go to a sport, social, or other club? | |||||||
| Attend meetings of non-religious organizations, such as political, community, or other interest groups? | |||||||
| *Pray privately in places other than a church or synagogue? | |||||||
| *Read books, magazines, or newspapers? | |||||||
| *Watch television? | |||||||
| *Do word games such as crossword puzzles or Scrabble? | |||||||
| *Play cards or games such as chess? | |||||||
| *Do writing (such as letters, stories, or journal entries)? | |||||||
| Do home or car maintenance or gardening? | |||||||
| *Bake or cook something special? | |||||||
| *Make clothes, knit, embroider, etc.? | |||||||
| Work on a hobby or project? | |||||||
| Play sports or exercise? | |||||||
| Walk for 20 min or more? | |||||||
| Participate in a local community arts group such as a choir, dance, photography, theatre, or music group? |
Marked activities indicate Cognitively Stimulating Leisure Activities (CSLA).
Author Note
This manuscript has not been published or will not be submitted elsewhere for publication while being considered by the Gerontology and Geriatric Medicine.
Ethical Consideration
This study utilized publicly available anonymized databases, and as such, was exempt from ethical compliance review.
Author Contributions
Junhyoung Kim: writing original draft, conceptualization. Jungjoo Lee: writing-original draft, investigation, methodology. Yongseop Kim: writing-original draft, investigation. Bomi Woo: writing-review, validation. Marcia Ory: project administration, validation, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.