
Abstract
Older adults are increasingly using cannabis medicinally, including for the treatment of mental health symptoms. The purpose of this report was to characterize cannabis use and perceptions of cannabis safety and effectiveness amongst older adults who use cannabis for the treatment of mental health symptoms. An online survey of cannabis usage and perceptions was conducted between February 2022 to September 2022. This report analyzes older adults currently using cannabis for self-reported mental health symptoms or conditions. A total of 1,615 older Canadians completed the survey, of whom 322 (19.9%) reported using cannabis for mental health symptoms. Most (70.8%) found cannabis somewhat or extremely helpful in managing their symptoms and 73.8% viewed cannabis as safe or very safe compared to pharmaceutical medications. Within the past year, 62.4% reported having experienced an adverse effect of cannabis. Older adults who use cannabis for mental health symptoms view it positively, despite the high prevalence of self-reported adverse effects.
Introduction
In Canada, 1 in 10 older adults has a mood or anxiety disorder, 1 in 5 has insomnia, and nearly half report difficulty with sleep initiation (Public Health Agency of Canada, 2020). Older adults are less likely than younger individuals to seek mental health care or be referred to psychotherapy, leaving many to manage their symptoms independently (Byers et al., 2012; Pettit et al., 2017). One therapy increasingly used by older adults for symptom management is cannabis (Kosiba et al., 2019). Cannabis use is increasing faster among older Canadians than any other age group, predominantly for medicinal purposes (Statistics Canada, 2019).
Older adults may use cannabis to treat symptoms of acute or chronic conditions, such as pain, insomnia, anxiety, or depression (Yang et al., 2021). The effectiveness of cannabis for mental health indications is equivocal (Wolfe et al., 2023). Cannabis has been found to decrease negative affect and likelihood of major depressive episodes, while also being associated with increased risk of anxiety, panic attacks, depression, mood disorders, and worsened post-traumatic stress disorder (Walsh et al., 2017; Wolfe et al., 2023). Some studies have found cannabis effective for improving sleep, while others have found no significant difference (Maddison et al., 2022). Observational data suggests that many older adults who use cannabis for the treatment of mental health symptoms find it effective and safe, with some reporting a decreased reliance on pharmaceuticals (Kaufmann et al., 2023; Reynolds et al., 2018; Tumati et al., 2022; Vaillancourt et al., 2022; Yang et al., 2021). However, much of the data on older adults’ experience with cannabis for mental health conditions is from clinical settings and may not apply to community-dwelling older adults where cannabis may be used without guidance or oversight from healthcare professionals. Cannabidiol (CBD) and delta-9-tetrahydrocannabinol (THC) are known to be inhibitors of enzymes within the cytochrome P-450 system, which metabolizes some medications used for mental health conditions, including some selective serotonin reuptake inhibitors and benzodiazepines (Ho et al., 2024). While there is a paucity of research on the clinical effects of such interactions, limited evidence suggests that pharmacokinetic interactions with cannabis may be clinically relevant for certain medications (Ho et al., 2024).
The increased use of cannabis by older adults, coupled with the prevalence of mental health conditions in this population and the possibility for cannabis both to worsen mental health symptoms and interact with mental health medications, makes it important to understand older adults use and perceptions of cannabis for the treatment of mental health symptoms. The purpose of this study is to describe the experiences of older adults who use cannabis for the treatment of mental health conditions. The objectives are to describe the prevalence of cannabis use for mental health in older adults, the self-reported effectiveness of cannabis, and the adverse effects experienced by this population.
Methods
An anonymous survey was developed through a comprehensive and inclusive process of reviewing relevant literature and obtaining input and feedback from older adults and clinicians. After reiterations and piloting with a small group of older adults online, the survey was formerly released and conducted online using the Qualtrics XM platform. A convenience sample of older Canadians was recruited through advertisements on social media, websites, and email distribution lists of the Aging in Place Research Cluster, the Institute for Healthy Living and Chronic Disease Prevention, and the National Association of Federal Retirees, and further spread through a snowball effect. Prospective participants were eligible for inclusion if they were English or French-speaking Canadians aged 50 years or older, regardless of cannabis use patterns or past medical history. There were no health, medication, or cannabis experience exclusion criteria. Eligible individuals were invited to complete a survey on their perceptions of, knowledge about, and experience with cannabis, regardless of whether they had current or previous experience with cannabis. The survey consisted of 45 multiple-choice and open-ended questions (Appendix 1). Survey questions were drafted based on a review of the literature, including other surveys assessing older adults use and perceptions of cannabis, as well as the researcher’s clinical experience working with community-dwelling older adults. Several older adults reviewed the survey before its launch for readability and skip logic. Data was collected on demographics and the perceptions of, knowledge about, and experiences with cannabis. The survey was available from February 5, 2022, to September 6, 2022. Ethical approval was granted by the harmonized ethics board of the Interior Health Authority and the University of British Columbia’s Behavioral Research Ethics Boards (H21-03287). Consent was electronically documented.
Participant demographics were used to determine the presence of multimorbidity, defined as having three or more chronic medical conditions (Johnston et al., 2019), and polypharmacy, defined as taking five or more medications concurrently (Masnoon et al., 2017). Participants reported their reasons for cannabis use as recreational, medicinal, or both. Those who selected medicinal use of cannabis alone or in combination with recreational use were asked to indicate the specific conditions for medicinal use from a list of potential health indications with a free-text box available for additional health indications. Cannabis use for mental health purposes was defined as self-reported use for any condition within the Diagnostic and Statistical Manual of Mental Disorders (DSM-5 TR; American Psychiatric Association, 2022). Participants were asked to select any adverse or unwanted effects experienced following cannabis use within the past year from a list of possible adverse effects, and a free-text box was provided for documentation of other adverse effects. Adverse effects were collapsed into categories, including adverse effects impacting balance, such as dizziness, lightheadedness, or feeling off balance, and adverse effects impacting mental alertness, including confusion, grogginess, and sedation.
Perceptions of cannabis effectiveness and safety were assessed using a 5-point Likert scale. Open-ended questions were coded using a standardized codebook. Less than 1% of the data was missing in the response variables. To ensure a complete dataset, missing data was estimated with multiple imputations. Data was considered missing at random, and a Markov chain Monte Carlo imputation algorithm was used to estimate missing variables. Categorical data was described with percentages. Chi-squared analysis was used to compare categorical data. A p-value of <.05 was considered statistically significant. Data analysis was completed with SPSS version 29.0.1.0.
Results
A total of 1,615 older Canadians completed the survey. Overall, 906 respondents were current non-users of cannabis (lifetime non-users and previous users) and 709 reported current use of cannabis, 322 (19.9%) of whom indicated cannabis was being used, as least in part, to treat mental health symptoms. Respondents who use cannabis for the treatment of mental health symptoms were primarily Caucasian (94.7%), between the ages of 50 to 70 (61.8%), with an equal proportion of males and females (Table 1). Compared to those using cannabis for reasons other than mental health, a greater proportion of respondents using cannabis for mental health purposes were female (51.2% vs. 43.7%, p = .04) and were living with multimorbidity (39.8% vs. 19.6%, p < .001). Compared to non-users of cannabis, those using cannabis to treat mental health symptoms were younger (age 50–60 years: 21.4% vs. 9.5%, p < .001), fewer had a graduate or professional degree (34.8% vs. 44.4%, p = .003) and a greater proportion were living with multimorbidity (39.8% vs. 19.1%, p < .001) and polypharmacy (20.2% vs. 15.2%, p = .04). Respondents using cannabis for mental health purposes were doing so for strictly medicinal reasons (56.2%) or both medicinal and recreational purposes (43.8%; Table 2). Half of the participants first used cannabis within the last 5 years, including 20.5% who first tried cannabis within the past 12 months.
Participant Demographics.

The 906 respondents not using cannabis included 259 previous users of cannabis, 633 with no previous cannabis use experience, and 14 with unreported cannabis use history.
Patterns of Cannabis Use and Reported Adverse Effects (n = 322).

Note. THC = tetrahydrocannabinol; CBD = cannabidiol.
Adverse effects impacting balance include dizziness/light-headedness/feeling off balance.
Adverse effects impacting mental alertness include grogginess/confusion/feeling sleepy, weak or hungover.
Other adverse effects: Hungry (3), headache (2), nausea (2), bad taste (1), low blood glucose (1), burning throat (1), giggles (1), fear (1), tremor (1), vivid dreams (1), cough (1), sleep issues (1).
The most common mental health reasons for cannabis use were insomnia (n = 273, 84.8%), anxiety (n = 141, 43.8%), and depression (n = 72, 22.4%; Table 2). Most (87.9%) also used cannabis to treat other non-mental health conditions, most commonly pain or inflammation (75.2%). Over half (52.5%) reported using cannabis daily/almost every day and 22.4% used cannabis several days per week. Almost two-thirds (63.7%) said that their healthcare professionals were aware of their cannabis use.
Most respondents found cannabis somewhat or extremely helpful for treating their symptoms (70.8%) and over half (57.1%) perceived cannabis to be more or somewhat more effective than pharmaceuticals (Figure 1). Participants viewed cannabis as safe or very safe (73.8%) compared to pharmaceuticals and described the perceived risk of cannabis as low or very low (74.4%).
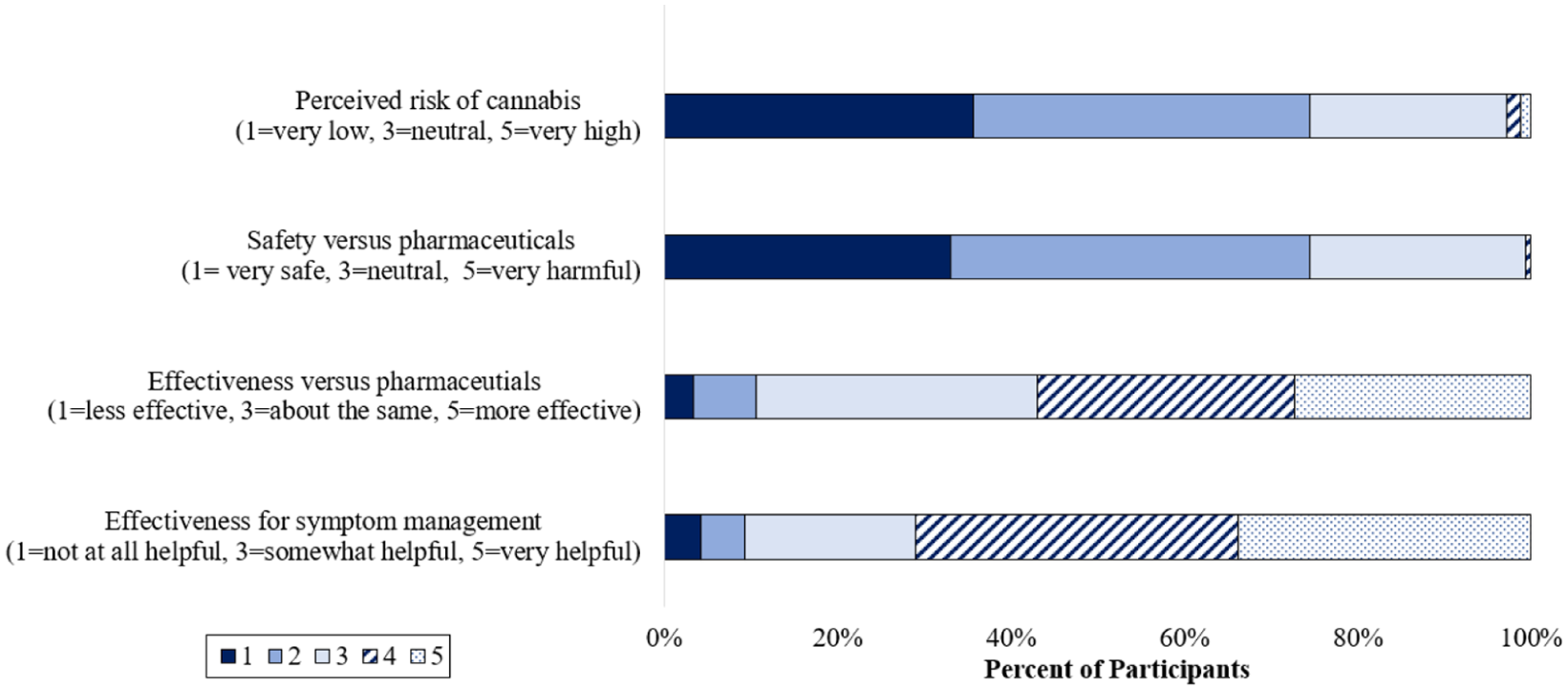
Perceptions of cannabis risk, safety, and symptom management by older Canadians who use cannabis for mental health purposes.
Within the past year, 62.4% of respondents reported experiencing unwanted or adverse effects of cannabis, most commonly dry mouth (34.5%), followed by adverse effects impacting balance (22%) or mental alertness (20.2%) and feeling high or hallucinating (20.8%; Table 2).
Discussion
Within this cohort of 1,615 older Canadians, 322 (19.9%) reported using cannabis, at least in part, to treat mental health symptoms. Half of individuals using cannabis for mental health symptoms started within the past 5 years and the majority used cannabis regularly. Most participants had a positive view of cannabis’ effectiveness and safety. However, almost 2/3 reported experiencing an unwanted or adverse effect of cannabis in the past year.
The use of cannabis for mental health purposes in this study was higher than previously reported. Of the 1,615 older Canadians who completed the survey, 16.9% used cannabis for insomnia, 8.7% for anxiety, and 4.5% for depression. Previous surveys indicate that 4% to 6% of older adults use cannabis for insomnia, 4% for anxiety, and 3% for depression (Reynolds et al., 2018; Yang et al., 2021). These differences may be due to the populations surveyed, as previous studies included individuals aged 65 and older at US geriatric or primary care clinics, while we electronically recruited community-dwelling Canadians aged 50 and older to reflect those described to be more sensitive to and higher risk of experienced side effects by in Canadian government publications (Government of Canada, 2022; Reynolds et al., 2018; Yang et al., 2021). This survey also had a higher proportion of current cannabis users (709/1,615, 43.9%) than previous studies (15%) (Reynolds et al., 2018; Yang et al., 2021). The greater proportion of cannabis use for mental health purposes in this study was likely reflective of the higher prevalence of cannabis use in the full study cohort. A greater proportion of individuals using cannabis for mental health purposes were female, of younger age, and living with multimorbidity and polypharmacy. A gender-based difference in the prevalence of mental health conditions exists in Canada, with women reporting a higher prevalence of both mood and sleep disorders (Public Health Agency of Canada, 2020). Similarly, literature suggests an association between the presence of mental health conditions and multimorbidity (Castro-de-Araujo et al., 2022), polypharmacy (Palapinyo et al., 2021), and lower educational achievement (Mojtabai et al., 2015), which may have contributed to greater use in these populations.
Most respondents who used cannabis for mental health purposes had a positive view of its effectiveness and safety. In a previous survey of community-dwelling older adults, most respondents found cannabis helpful for symptoms such as insomnia, anxiety, or depression (Reynolds et al., 2018; Yang et al., 2021). Data including younger populations has found that the majority of those who use cannabis medicinally find it to be more effective than prescription medications, better tolerated, and helpful in reducing or eliminating reliance on prescription medications (Corroon et al., 2017; Kvamme et al., 2021; Tumati et al., 2022). The predominant comparison has been to opioid medications; however, similar reductions in the use of antidepressants, anxiolytics, and benzodiazepines have been reported with cannabis (Corroon et al., 2017; Kvamme et al., 2021; Vaillancourt et al., 2022). While we did not specifically ask if cannabis was a substitute for pharmaceuticals, it is reasonable to assume that a portion may be, given the positive cannabis perceptions of respondents.
Nearly two-thirds (62.8%) of respondents experienced at least one unwanted or adverse effect in the past year. This is higher than other surveys of community-dwelling older adults, which found approximately 15% of cannabis users had ever experienced an adverse effect. This difference may be methodological. We asked participants to select any adverse effects that they experienced in the past year from a list of potential negative health effects while other surveys first asked if participants had experienced an adverse effect before prompting them to select the adverse effect experienced (Reynolds et al., 2018; Yang et al., 2021). Adverse effects impacting balance and mental alertness were reported by 22.2% and 20.3% of our respondents, respectively. This is in alignment with another survey that found 27% of older American cannabis users experienced some or a lot of memory impairment, and 12% experienced some or a lot of balance impairment/falls (Lum et al., 2019). Adverse effects impacting cognition and balance are concerning in older adults due to the increased risks of cognitive impairment and falls in this demographic (Wieghorst et al., 2022; Workman et al., 2021).
Despite the frequency of adverse effects, cannabis was generally considered safe by most respondents. However, evidence suggests some individuals may experience worsening mental health conditions with cannabis use, including anxiety, depression, and post-traumatic stress disorder (Wolfe et al., 2023). Additionally, cannabis may interact with some medications commonly used for the treatment of mental health conditions (Ho et al., 2024). CBD and THC are known to inhibit certain cytochrome P450 isoenzymes (Ho et al., 2024), which metabolize some common mental health medications, including several selective serotonin reuptake inhibitors (Edinoff et al., 2021) and benzodiazepines (Griffin et al., 2013). The risk of potential drug interactions and unrecognized adverse effects of cannabis may be even more important for the nearly 1/3 of respondents whose healthcare providers are unaware of their cannabis use. An increased public awareness of the potential safety concerns of using cannabis is necessary, including the importance of ensuring healthcare professionals’ awareness of cannabis use.
More research is warranted to determine the safety and effectiveness of cannabis for mental health purposes, particularly in older adults. Our research suggests that a growing number of older Canadians are using cannabis for mental health purposes, despite equivocal evidence on its safety and effectiveness. Additional research in older populations is required to determine the effectiveness of cannabis for mental health conditions and cannabis safety in the aging body and with concomitant medications commonly used by this population. As there is a growing number of older adults using cannabis, healthcare providers must inquire about cannabis use, particularly for those with mental health conditions or experiencing symptoms that may be attributable to or impacted by cannabis, such as impaired cognition or balance.
Limitations
This study involved the voluntary completion of an electronic survey by a convenience sample of older Canadians who were primarily Caucasian, cis-gender, and of higher socioeconomic status and does not necessarily represent the experiences and perceptions of older Canadians nationwide. As such, generalizability to people of other ethnicities, genders, or socioeconomic statuses or those with lower technological literacy is cautioned. Additionally, a responder bias may be present in our sample, with a greater representation of individuals who are currently using cannabis, have a positive view of cannabis, or are more interested in or educated on cannabis. Responses, such as adverse effects experienced in the past year, may be influenced by recall bias, and should be interpreted cautiously. Legalization in Canada likely impacted cannabis use and perceptions; thus, this data might not be applicable in countries where cannabis is not legal. Our survey questions were broad, and we were not able to identify some of the nuances of cannabis practices, such as the composition of cannabis currently being used, or if participants had a clinical diagnosis of a mental health condition from a medical provider. Further work is necessary to investigate the specific preferences and practices of cannabis use for mental health conditions in older adults.
Conclusions
Approximately one in five older Canadians reported using cannabis, at least in part, to manage mental health symptoms, the majority of whom have a positive view of its effectiveness and safety profile. However, adverse effects, including those impacting balance and mental alertness, are common within this population. It is important for healthcare professional to inquire about cannabis use when caring for older adults with mental health conditions.
Footnotes
Appendix 1: Survey Questions
________________________________________________________________
(1 = strongly disagree, 2 = somewhat disagree, 3 = neither agree nor disagree, 4 = somewhat agree, 5 = strongly agree)
Acknowledgements
We would like to acknowledge the contributions Jacob Movold, who assisted in methodology and analysis.
Ethical Considerations
All procedures performed in this study were in accordance with the ethical standards of the institutional research committees (Interior Health Authority and the University of British Columbia’s Behavioral Research Ethics Boards [H21-03287]) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained from all participants and documented electronically.
Author Contributions
Jennifer Bolt: Conceptualization, Methodology, Investigation, Writing—Review & Editing, Visualization. Megan Behm: Formal analysis, Writing—Original Draft. Melanie Fenton: Conceptualization, Methodology, Investigation, Writing—Review & Editing, Project Administration. Jennifer M. Jakobi: Conceptualization, Methodology, Investigation, Writing—Review & Editing, Visualization, Supervision.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work performed by JMJ, MB, and MF was funded by the Eminence Award from Vice President Research and Innovation at University of British Columbia Okanagan for Research Clusters of Excellence.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.