
Abstract
Introduction:
Functional decline is a common risk among hospitalized older adults. Comprehensive Geriatric Care (CGC) has been shown to improve clinical outcomes in this population. However, beneficial predictors are not fully known.
Methods:
This study was conducted at the Department of Geriatrics, University Hospital Jena, Germany. Data were collected from 2014 to 2023. Functional improvement was defined as a positive change in the Barthel Index from admission to discharge. Covariates included age, sex, body mass index (BMI), number of functional disabilities (Lachs screening), cognition, depressive symptoms, mobility, and treatment duration. Statistical analyses were conducted using binominal logistic regression to identify predictors of functional improvement.
Results:
Of 3,990 patients, functional improvement was observed in 85.2%, which was associated with female sex (OR = 1.352; p = .007), fewer functional disabilities (OR = 0.905; p = .007), better cognition (OR = 1.130; p < .001), better mobility (OR = 1.114; p < .001), lower Barthel Index at admission (OR = 0.964; p < .001), and longer treatment duration (OR = 1.987; p < .001; χ2(6) = 181.32, p < .001, Nagelkerke’s R2 = 0.104). No significant associations were found for age, BMI, or depressive symptoms.
Conclusion:
Most patients experienced a functional improvement during CGC. However, commonly used predictors explain only a small proportion of the variance, suggesting that additional biopsychosocial factors need to be explored to better predict outcomes after CGC.
Introduction
Older adults admitted to hospitals for acute conditions such as illnesses or injuries face a high risk of functional decline and other complications as a long-term consequence. This can result in increased hospital costs, the necessity for long-term care, and higher mortality rates (Covinsky et al., 2003). To address this issue, acute geriatric units have been established for the exclusive care of these patients (Amador et al., 2007). Several meta-analyses have determined the efficacy of admission to an acute geriatric unit and comprehensive geriatric care (CGC) in comparison to conventional hospital care with regard to clinical outcomes (e.g., functional decline, living at home; Baztán et al., 2009; Fox et al., 2012; O’Shaughnessy et al., 2022). However, further research is necessary to identify specific factors contributing to these positive outcomes.
In Germany, CGC on acute geriatric units is referred to as complex geriatric rehabilitation therapy and recorded under the Operations and Procedures classification System (OPS) 8-550 (Kolb et al., 2014). Over the past decade, this procedure has been increasingly applied with over 300,000 admissions in 2022 (Statistisches Bundesamt (Destatis), 2023). This has rendered CGC a highly pertinent treatment approach within the German healthcare system. According to the specifications of the OPS 8-550, CGC involves a multidisciplinary team including geriatricians, nurses, physiotherapists, occupational therapists, speech therapists, social workers, psychologist, and other professionals. These professionals collaborate on personalized treatment plans to enhance the patient’s physical, psychological, and social abilities. The duration of the treatment can vary between 7 and 13 days (OPS 8-550.0), 14 to 20 days (OPS 8-550.1), and more than 20 days (OPS 8-550.2). As part of the CGC and in accordance with the specifications of the OPS 8-550, the ability to perform activities of daily living (ADLs) is evaluated on a weekly basis. For this purpose, the Barthel Index is a suitable assessment tool (Mahoney & Barthel, 1965). Therefore, the Barthel Index is the most commonly used instrument for the assessment of functional impairment on geriatric wards in Germany (Kudelka et al., 2024). In addition, a comprehensive geriatric assessment is mandatory on admission to the hospital to evaluate the patient’s initial mobility, cognition, depression, and social functioning due to the increasing prevalence of these complaints in older age. Furthermore, the identification of certain geriatric syndromes within CGC allows for individualized treatment, which goes beyond the use of classical biomedical variables (e.g., age, sex, Body Mass Index). Therefore, it is useful to screen for the presence of geriatric syndromes or functional disabilities. Upon discharge, the Barthel Index is reassessed to ascertain functional improvement. While the beneficial impact of CGC (OPS 8-550) on functional outcomes has been substantiated (Kwetkat et al., 2014; Niemöller, Arnold, Stein, Juenemann, Farzat, et al., 2023; Niemöller, Arnold, Stein, Juenemann, Erkapic, et al., 2023; Werner et al., 2024), a more profound comprehension of predictive variables is imperative to facilitate enhanced personalized treatment strategies. Of particular interest is whether physical or psychosocial aspects of health (e.g., depressive symptoms) can predict treatment success.
It is already known that the prevalence of certain geriatric syndromes differs between the sexes, with higher rates of mental disorders, depression, dementia, impaired physical movement and instrumental activities of daily living, and frailty in woman than in men (Gong et al., 2023; Lin et al., 2022; Park & Ko, 2021; J.-K. Wang et al., 2010). However, for several acute and chronic conditions, male patients face a higher risk of worse health outcomes compared to female patients (e.g., acute and chronic heart diseases, cerebrovascular diseases, chronic bronchitis, or hearing impairments; Verbrugge, 1982). Accordingly, a deeper understanding of possible differences in functional dependency between female and male geriatric patients, specific risk factors, and individualized treatment approaches within CGC is needed.
Therefore, the objective of our study was to determine which factors of the comprehensive geriatric assessment are associated with functional improvement at the end of CGC and to identify sex-specific differences. This knowledge could facilitate the development of tailored geriatric care in acute conditions through individualized treatment approaches.
Methods
Study Design
We conducted a monocentric retrospective analysis of routine data of patients treated within the CGC according to the requirements of the OPS 8-550 at the Department of Geriatrics, University Hospital Jena, Germany. Inclusion criteria were the completion of CGC over a period of 10 years between January 2014 and December 2023. Patients with severe cognitive impairment (Mini-Mental State Examination [MMSE] score of less than or equal to 16 points or an indeterminate score (Folstein et al., 1975)) were excluded from the study because screening instruments for depression have limited validity in patients with severe cognitive impairment (Kørner et al., 2006). The study was approved by the local ethics committee of the University Hospital Jena (registration number: 2024-3252-Daten). As this was a retrospective study with anonymous data, patient consent was waived by the ethics committee. Data were assessed for research purposes on March 27, 2024. The authors did not have access to any information that could be used to identify individual participants in the study.
Study Population
During the study period, 6,009 patients were treated within the CGC. Of the total number of patients, 2,019 (33.6%) patients were excluded due to severe cognitive impairment (MMSE < 16 points, N = 1,570, 26.1%; MMSE not determinable, N = 449, 7.5%; Folstein et al., 1975). Accordingly, 3,990 patients were included in further analyses.
Dependent Variable
The primary outcome was functional improvement within the CGC. This was defined as any positive change in the Barthel Index from admission to discharge (Mahoney & Barthel, 1965). The Barthel Index assesses 10 aspects of self-help capability, including feeding, bathing, grooming, dressing, bowel and bladder control, toilet use, transfers, mobility, and stair climbing. Each item is scored from 0 to 5, 10, or 15. The item scores are summed to give a total score between 0 (totally dependent) and 100 (totally independent).
Covariates
Based on the literature and in accordance with the requirements of the OPS-8-550, several additional variables were selected as covariates. These included age (metric), sex (male “0,” female “1”), Body Mass Index (BMI) as a measure of relative weight (metric; Keys et al., 1972), geriatric screening for functional disabilities according to Lachs et al. (metric; Lachs et al., 1990), cognition (MMSE, metric; Folstein et al., 1975), depressive symptoms (15-items Geriatric Depression Scale, GDS, metric; Yesavage et al., 1982), a performance-oriented mobility assessment (Tinetti test, metric; Tinetti, 1986), and activities of daily living at baseline (Barthel Index, metric; Mahoney & Barthel, 1965). In addition, the duration of the CGC was considered according to OPS 8-550. For regression analysis, a treatment duration of 7 to 13 days was classified as “short” (OPS 8-550.0), and a duration of 14 days or more as “long” (OPS 8-550.1 and OPS 8-550.2).
Statistical Analyses
IBM SPSS version 29 and jamovi version 2.2 were used for statistical analysis. Statistical significance was set at p < .05 for all tests. Data were tested for normality using the Shapiro-Wilk test. Results were reported as median and interquartile range (IQR) for non-normally distributed data and as counts and percentages for categorical variables. Group comparisons between independent variables were performed using the Mann-Whitney U test for non-normally distributed data and the Wilcoxon signed rank test for non-normally distributed differences. Effect sizes were reported as rank biserial correlation for non-normally distributed data. Binominal logistic regression with backward selection (likelihood ratio) was used to determine the predictive value of independent variables for functional improvement. For regression analyses, autocorrelation and multicollinearity were excluded (|r| < 0.8). Incomplete data sets were omitted. Linearity was assessed using the Box-Tidwell procedure. Outliers were identified by calculating the standard deviation of the studentized residuals (SD > 3) and leverages (>0.2), and were subsequently excluded.
Results
Baseline Characteristics
The majority of patients were female (65.7%), median age 83 years (IQR 79–87), mildly overweight (not age adjusted; median BMI 27; IQR 23–31), and had seven functional disabilities in the Lachs screening (IQR 5–8). The subjects exhibited a median GDS-15 sum score of 4 (IQR 2–6), indicating the absence of relevant depressive symptoms. They showed a high risk of falling (median Tinetti total score 14; IQR 7–19). According to the Barthel Index at admission, 848 patients (21.3%) had a high degree of dependency (Barthel Index range: 0–30), 2,953 patients (74.1%) required assistance (Barthel Index range: 35–80), and 185 patients (4.6%) had selective dependency (Barthel Index range: 85–95). No patient demonstrated full independence (Barthel Index: 100; Lübke et al., 2004). The majority of patients (N = 3,369; 84.4%) were treated for 14 to 20 days (OPS 8-550.1). Descriptive statistics of the patients are shown in Table 1.
Characteristics of the Baseline Study Population.
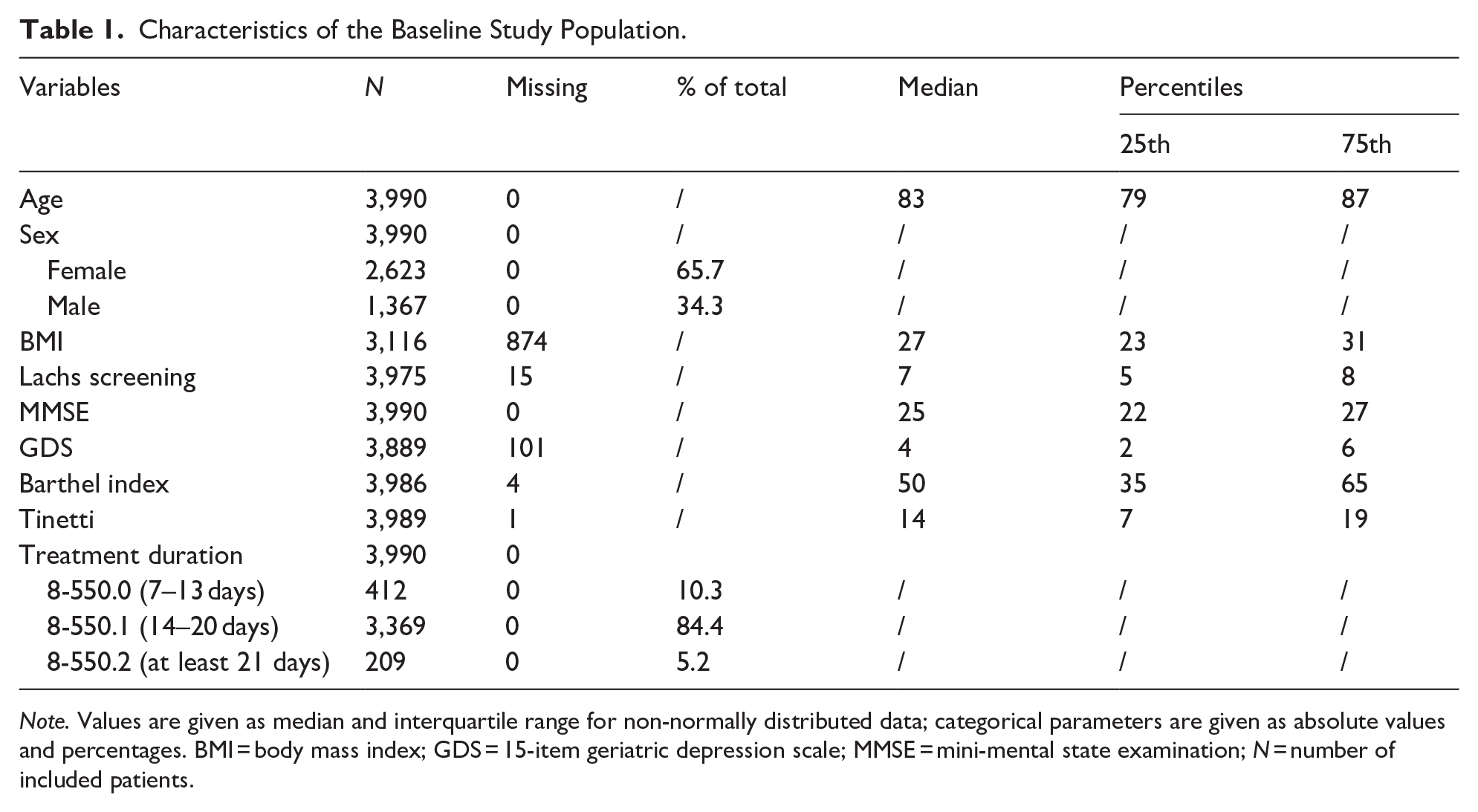
Note. Values are given as median and interquartile range for non-normally distributed data; categorical parameters are given as absolute values and percentages. BMI = body mass index; GDS = 15-item geriatric depression scale; MMSE = mini-mental state examination; N = number of included patients.
On admission to the CGC, female patients had older age (r = .130; p < .001), higher BMI (r = .061; p = .005), less mobility (r = .054; p = .005), and more functional disabilities according to Lachs (r = .057; p = .003) compared to male patients (see Supplemental S1 Table). However, the observed effect sizes were marginal (r < .1).
A comprehensive examination of the functional disabilities documented by the Lachs screening revealed that polypharmacy was most frequently reported by female and male patients (83% and 86%, respectively), while lack of social support was least commonly reported (8 % and 7%, respectively). Significant group differences were observed, with female patients reporting more frequent impaired vision, arm function, leg function, urinary incontinence, and pain than male patients. In contrast, male patients reported impaired hearing, cognition (attention), and polypharmacy more frequently. Again, the effect sizes were marginal (see Supplemental S2 Table).
Functional Improvement
Over a period of 10 years, the Barthel Index at admission is largely evenly distributed with a median of 50 points (IQR 35–65; see Figure 1). From admission to discharge, the Barthel Index improved in N = 3,398 patients (85.2%). The median improvement was 20 points (IQR 10–30). A logistic regression analysis (χ2(6) = 181.32, p < .001, Nagelkerke’s R2 = 0.104) revealed that functional improvement was associated with female sex (OR = 1.352; 95% CI [1.085–1.685]; p = .007), less functional disabilities according to Lachs screening (OR = 0.905; 95% CI [0.856–0.957]; p < .001), better cognition (OR = 1.130; 95% CI [1.093–1.168]; p < .001), better mobility (OR = 1.114; 95% CI [1.090–1.138]; p < .001), and a worse Barthel Index at admission (OR = 0.964; 95% CI [0.957–0.972]; p < .001). Furthermore, a treatment duration of at least 14 days was associated with functional improvement (OR = 1.987; 95% CI [1.458–2.706]; p < .001). Thereby, group comparison revealed that patients, who were treated longer were older, had more functional disabilities, worse mobility, and a worse Barthel Index at admission (see Supplemental S3 Table). In general, no significant association regarding functional improvement was observed for age (p = .154), BMI (p = .161), or depressive symptoms (p = .977). For detailed information, steps 1 and 4 of the regression are presented in Table 2.
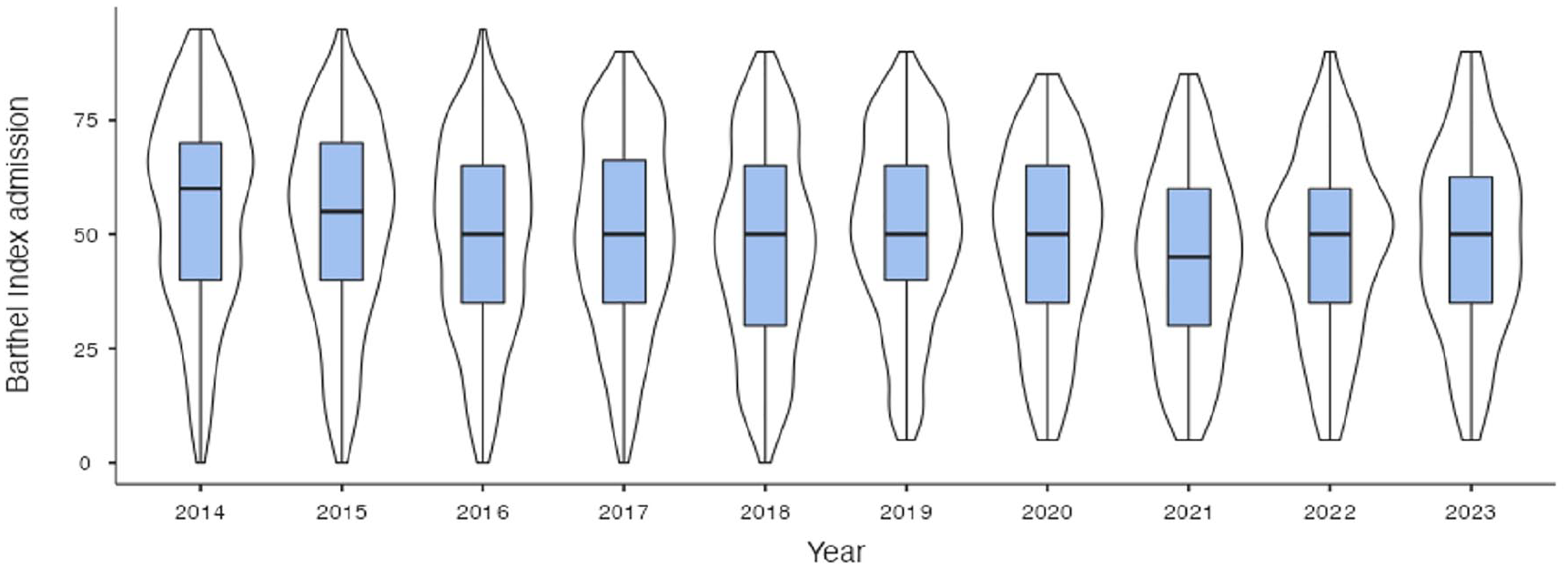
Yearly distribution of the Barthel Index at admission.
Regression Analysis, Variables in the Equation.

Note. Values were obtained using binomial logistic regression analysis with backward selection (likelihood ratio) to identify predictors of functional improvement. Number of patients included in the regression analysis, N = 3,018 (75.6%). B = unstandardized regression coefficient; CI lb = lower bound of the 95% confidence interval; CI ub = upper bound of the 95% confidence interval; OR = odds ratio; BMI = body mass index; GDS = 15-item Geriatric Depression Scale; MMSE = mini-mental state examination.
Sex-Specific Analyses of Functional Improvement
From the time of admission to the time of discharge there was an improvement of the Barthel Index in a total of N = 2,255 female patients (86.3%) and N = 1,143 male patients (84.0%). The median improvement of the Barthel Index for female and male patients was 20 points (IQR 10–30) without significant group differences (p = .242). Logistic regression analyses were performed for female (χ2(5) = 127.59, p < .001, Nagelkerke’s R2 = 0.114) and male patients (χ2(4) = 52.27, p < .001, Nagelkerke’s R2 = 0.084) to uncover sex-specific differences in the predictors. No significant associations were seen for age, BMI, and depressive symptoms in female and male patients. In contrast, cognition, mobility, Barthel Index at admission, treatment duration, and functional disabilities according to Lachs screening were significantly associated with functional improvement (see S4 and S5 Tables).
Cognition
Functional improvement was associated with better cognition in female (OR = 1.140; 95% CI[1.093–1.189]; p < .001) and male patients (OR = 1.123; 95% CI [1.063–1.185]; p < .001).
Mobility
Both in female (OR = 1.123; 95% CI [1.092–1.155]; p < .001) and male patients (OR = 1.102; 95% CI [1.065–1.140]; p < .001), functional improvement was associated with better mobility.
Barthel Index at Admission
A lower Barthel Index at admission was associated with functional improvement in female (OR = 0.965; 95% CI [0.955–0.974]; p < .001) and male patients (OR = 0.966; 95% CI [0.955–0.978]; p < .001).
Treatment Duration
Functional improvement was associated with a longer treatment duration of at least 14 days in female (OR = 2.086; 95% CI [1.394–3.122]; p < .001) and male patients (OR = 1.798; 95% CI [1.108–2.916]; p < .001).
Geriatric Screening According to Lachs
In female patients, less functional disabilities according to Lachs screening were associated with functional improvement (OR = 0.891; 95% CI [0.831–0.955]; p = .001), whereas no association was seen for male patients (p = .060).
Discussion
In Germany, CGC according to OPS 8-550 is increasingly performed and has accordingly become a highly relevant treatment approach in the German healthcare system (Statistisches Bundesamt (Destatis), 2023). Here, we sought to describe changes in the Barthel Index within CGC from admission to discharge to identify factors associated with functional improvement and to explore sex-specific differences. Knowledge of these factors is important to optimize treatment and to develop tailored geriatric care for acute conditions.
The results of our analysis of 3,990 patients demonstrated that functional improvement according to a positive change in the Barthel index was achieved in over 85% of cases. Thus, the vast majority of individuals showed improvement during CGC, which supports existing evidence on the effectiveness of specialized geriatric care for acutely ill patients (Baztán et al., 2009; Fox et al., 2012; O’Shaughnessy et al., 2022). During the course of the CGC, there was an improvement of approximately 20 points on the Barthel Index scale. Taking into account the specifications of the OPS 8-550, these results are consistent with previous studies in Germany showing an improvement in the Barthel Index (Kwetkat et al., 2014; Niemöller, Arnold, Stein, Juenemann, Farzat, et al., 2023; Palzer et al., 2021).
The results of the regression analysis revealed that functional improvement was associated with a worse Barthel Index at admission, female sex, lower levels of functional disabilities according to Lachs screening, better cognition, better mobility, and a longer treatment duration of at least 14 days. This finding aligns with previous research indicating that patients with reduced functional capacity exhibit notable improvement (Kwetkat et al., 2014). However, the association between worse Barthel Index on admission and more functional improvement is intrinsic to the scale and depends on the primary outcome measure. An association between the Barthel Index and other mobility outcomes has not yet been demonstrated (Werner et al., 2024). Of note, we observed a beneficial association of female sex on functional improvement. It is already known that there are considerable differences in the health status of men and women, which can be attributed to a number of factors, including the prevalence of disease, the focus on disease prevention, and the way in which health is reported (Verbrugge, 1982). These differences occur in all age groups, culminating in elevated rates of hospitalization or emergency department visits among male nursing home residents compared to female residents (Brucksch et al., 2018; Hoffmann & Allers, 2016). Nevertheless, the underlying causes remain poorly understood. Our results showed only marginal differences in age, BMI, mobility, and functional disabilities between male and female patients in the CGC. Nevertheless, the sum of functional disabilities according to the Lachs screening is associated with functional improvement after CGC in female geriatric patients, but not in male patients. However, the results of the subgroup analyses also indicated only marginal effect sizes for the observed group differences. Accordingly, the relationship between sex differences, functional disabilities, and functional improvement needs further investigation.
An association was observed between enhanced cognitive function and functional improvement. This is consistent with previous studies indicating that cognitive impairment, in addition to physical frailty, is detrimental to health, and functional independence (Aliberti et al., 2019; Sugimoto et al., 2022). Thereby, the beneficial effects of physical activity on cognitive function and activities of daily living are well-documented and widely accepted (Lam et al., 2018; Li et al., 2023; Zhou et al., 2022). However, due to the exclusion criteria of our study, patients with severe cognitive impairment were excluded in order to ensure the validity of the results. Screening for depressive symptoms in severely cognitively impaired patients with the widely used GDS would result in less valid responses. Given these limitations, our results cannot be generalized and do not allow a causal statement about whether CGC is less effective in patients with severe cognitive impairment.
However, these variables explained only 10% of the variance of functional improvement (Nagelkerke’s R2 = 0.104). Accordingly, it can be posited that additional biopsychosocial factors may account for the majority of the variance and thus require further investigation. In this regard, we suggest elaborating on the types of biopsychosocial variables that may improve the predictive value of the model. Previous evidence has shown that frailty is associated with adverse outcomes after treatment on an acute geriatric rehabilitation ward (Singh et al., 2012). And this association is in turn influenced by psychosocial factors (Dent & Hoogendijk, 2014). Including anxiety, social activities, home, and neighborhood satisfaction, as well as premorbid functional independence and a tendency to fall in future prospective studies could lead to more holistic predictive models (Dent & Hoogendijk, 2014; Wu et al., 2006).
In contrast to the aforementioned predictors, no significant association was seen for age, BMI, and depressive symptoms regarding functional improvement. Besides the inherit risk of mortality, a higher chronological age is a known risk factor for frailty (X. Wang et al., 2022), and accordingly, functional dependence. However, our results suggest that CGC according to OPS 8-550 is also an effective treatment approach in older geriatric patients, which corresponds to the literature (Kwetkat et al., 2014). Likewise, age has not been shown to influence mobility outcomes within the CGC (Werner et al., 2024). However, it should be noted that the majority of patients were over 80 years of age and the age range considered is correspondingly small, which limits the generalizability of the association.
We did not observe an association between depressive symptoms and functional improvement. This finding is consistent with that of a previous study, that found no difference in the degree of improvement between geriatric patients undergoing CGC with and without relevant depressive symptoms (Niemöller, Arnold, Stein, Juenemann, Farzat, et al., 2023). Although the prevalence of depressive symptoms was higher in female patients in the aforementioned study, no differences in depressive symptoms were observed between male and female patients in our study. In addition to female sex, somatic illness, cognitive and functional impairment, and less social contacts are known predictors of depressive symptoms in older people (Djernes, 2006). Therefore, older people are particularly vulnerable to the onset of depression (Noel et al., 2004). Although our study did not find an association between depressive symptoms and functional improvement at the end of the CGC, it is reasonable to hypothesize that depressive symptoms have a significant influence on the subsequent course of treatment after hospital discharge. Accordingly, previous studies have shown that depressive symptoms (e.g., anhedonia) are associated with frailty and functional decline (Covinsky et al., 1997, 2014; Laura et al., 2022; Reichardt et al., 2020), and that somatic depressive symptoms in particular are associated with long-term mortality (Covinsky et al., 1999; Smolderen et al., 2009). However, the association between depressive symptoms and hospital readmission is inconsistent (Albrecht et al., 2014; Smolderen et al., 2009). Therefore, further studies are needed to determine whether depressive symptoms in general or specific subtypes have a long-term impact on other relevant patient-related outcomes in acute geriatric care, such as rehospitalization, institutionalization, and mortality. Moreover, further research is needed to determine the impact of different depressive symptoms on health outcomes in patients with severe cognitive impairment. While these patients were excluded from the current study due to the limited validity of the screening instrument used for depressive symptoms, further studies using validated screening instruments for people with severe dementia are needed. As depression is a crucial determinant of well-being in older adults (Cavdar et al., 2024; Tan et al., 2023), screening for depression and early interventions are of utmost importance and should remain an integral part of CGC. However, it should be pointed out that although the GDS-15 is an established screening instrument for depressive symptoms in older patients (Lesher & Berryhill, 1994; Yesavage et al., 1982), it cannot replace neuropsychological testing in individual cases.
Our study has certain limitations. First, as data is based on a retrospective analysis without a follow up or control group, the results of the available data only describe cross-sectional associations. In this regard, our data do not allow any causal statements whether the CGC leads to functional improvement. However, most patients experienced improvement during the course of CGC. Second, patients with severe cognitive impairment were excluded to ensure valid responses in the assessment of depressive symptoms. Exclusion of severely cognitively impaired patients limits generalizability to more affected patient groups. Third, due to the monocentric design, we only considered patients treated at one hospital, which limits is generalizability to other regions. However, the studied cohort is comparable to the cohort of Niemöller et al. (Niemöller, Arnold, Stein, Juenemann, Farzat, et al., 2023). Fourth, to the best of our knowledge, no previous study has examined the predictive value of standardized acute geriatric care according to the specifications of OPS 8-550 in Germany. This restricts the evaluation of whether the low level of explained variance is typical for the treatment or not. Finally, we used routine data that do not adequately cover the variety of biopsychosocial factors contributing to well-being in older adults.
Conclusion
Most patients experienced a functional improvement during CGC. Therefore, it can be considered an effective treatment approach for older patients. This improvement is associated with female sex, less functional disabilities in the Lachs screening, better cognition, better mobility, a worse Barthel Index at admission, and a longer treatment duration of at least 14 days. Nevertheless, the capacity of these frequently used variables to predict functional improvement is limited. Accordingly, due to the low predictive value, further research is needed to identify additional biopsychosocial factors that will allow better characterization of different patient subgroups, improved prediction of treatment outcomes, and enhanced individualized treatment strategies. Further research is required to elucidate the impact of depressive symptoms on the course of treatment after hospital discharge.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334251346941 – Supplemental material for Predictors of Functional Improvement During Comprehensive Geriatric Care in Germany: A 10-Year Monocentric Retrospective Analysis
Supplemental material, sj-docx-1-ggm-10.1177_30495334251346941 for Predictors of Functional Improvement During Comprehensive Geriatric Care in Germany: A 10-Year Monocentric Retrospective Analysis by Konstantin G. Heimrich, Aline Schönenberg, Sarah Mendorf, Thomas Lehmann and Tino Prell in Sage Open Aging
Footnotes
Acknowledgements
We thank Anja Kwetkat, the former Head of the Department of Geriatrics at Jena University Hospital, who directed the department with great dedication until 2022.
Ethical Considerations
The study was approved by the local ethics committee of the University Hospital Jena (registration number: 2024-3252-Daten) on February 20, 2024.
Informed Consent Statement
As this was a retrospective study with anonymous data, patient consent was waived by the ethics committee.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bundesministerium für Bildung und Forschung (BMBF, Federal Ministry of Education and Research) to TP (grant number 01GY2301), and by the Bundesministerium für Bildung und Forschung (BMBF, Federal Ministry of Education and Research) to SM (grant number 01GY1804).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.