
Abstract
Physician Orders for Life-Sustaining Treatment (POLST) arose in 1991 to improve end-of life-care for patients with advanced, chronic, and progressive illnesses whose death is imminent within a year. POLST attempted to address problems inherent in advance directives (e.g., poor completion rates, confusing form language, dismal communication with a surrogate). POLST exists in all U.S. states, although each is unique and uptake is inconsistent, particularly in rural areas. The purpose of this study was to investigate current practices and barriers around POLST in a rural area using an online survey and interviews with practitioners. A total of 101 people responded to the survey, and 20 participated in interviews. Findings included the need for consistent funding, clarification of goals, and greater and varied opportunities for staff training. Also important was establishing strong support for POLST within healthcare entities, physician and community support, identification of champions, and research evaluating processes and patient outcomes.
Keywords
Introduction
In the 1970s, the advance care planning movement came about as a reaction to improvements in medical technology that lengthened life for patients in life-limiting situations, unleashing a bevy of ethical questions. Aggressive treatments at the end of life, for all ages, but often for older adults, should both extend and improve quality of life (Motamedi et al., 2021). However, these outcomes may or may not be possible given conditions facing older people. Older adults value independence and autonomy (Gibson et al., 2024), values that can be comprised if patients are not well informed and supported in decision making about end-of-life circumstances (Sánchez-García et al., 2019). The use of multiple and intensive services at the end of life may have little clinical benefit and cause unnecessary pain rather than improve quality of care (Lo et al., 2022).
One response to improving quality of life and end-of-life care is Physician Orders for Life-Sustaining Treatment (POLST). POLST was developed in 1991 with the goal of improving end-of life-care for patients with advanced, chronic, progressive illnesses whose death was imminent within a year or who wished to further define preferences for treatment (Sabatino & Karp, 2011). The intention of POLST was to address problems inherent in advance directives—that most people fail to complete them, cannot understand the language of the forms, neglect to update directives, and rarely, if ever, review them with a surrogate (Hickman et al., 2008). POLST exists in some form in all states in the U.S, although implementation is uneven.
Unevenness is particularly apparent in parts of the country where there are few, if any large, coordinated medical systems from which to draw and sustain support for POLST. Rural areas are examples where uptake of POLST has been light. For example, in sharp contrast to the densely populated areas of northern Virginia, one such rural area is located in the southwest corner of the state. To understand why uptake has been poor, the purpose of this project was to investigate current practices and barriers to the use of POLST in healthcare settings in rural Southwest Virginia.
The POLST Paradigm
The potential offered by life-sustaining technologies at end of life impelled the medical profession to offer patient-driven care. The first advance directive document was the living will, and the durable power of attorney for healthcare (DPOAHC) emerged as a mechanism to allow capacitated individuals to appoint a legal surrogate for healthcare decisions. The living will and the DPOAHC became known as medical advance directives, making approaches to end-of-life healthcare decisions highly legalistic, raising the need of healthcare systems to avoid abuse, error, or litigation when carrying out patients’ wishes (Sabatino & Karp, 2011). The legalistic approach relied upon prescriptive language and highly specific medical terms. To counteract inadequacies of advance directives, a communications approach emerged, acknowledging that advance care planning was not a “one size fits all” process.
POLST was a way to implement the communications approach by honoring patients’ values, goals of care, and preferences. Because it relied on a physician’s order, POLST had “teeth” to direct care at end of life. The paradigm involves a document and a process including a discussion with a healthcare professional, incorporation of patient preferences into a physician order, and assurance that the form is portable. The POLST Paradigm proliferated nationally because of its simplicity and evidenced-based effectiveness (Fromme et al., 2012; Pedraza et al., 2017).
The Evidence Base for POLST
Research has informed the POLST policymaking process since its inception, with about half of studies concerning patients in Oregon (Hickman et al., 2015). Chart reviews and patient-level studies of POLST users reveal that typical patients are older white people nearing the end of their lives (Hickman et al., 2015; Schmidt et al., 2014). Although POLST forms can be created in any venue (e.g., hospital, nursing home, assisted living facility, private practice location), highest rates of completion are in hospice settings (Hickman et al., 2010). About a third of completers requested low levels of treatment (e.g., comfort care, no artificial nutrition; (Schmidt et al., 2014)). Completion of a POLST form appears to facilitate better communication between nursing home staff and hospital staff (Caprio et al., 2012).
Alternately, studies identified problems with the form, including difficulty in explaining it to a patient (Sugiyama et al., 2013) and obtaining a physician signature (Wenger et al., 2013). Additional issues include lack of form completion in emergency departments and a need to standardize the approach (Bomba & Orem, 2017; Clemency et al., 2017).
POLST in the Commonwealth of Virginia
In Virginia, POLST became a “standard of practice” rather than a law. In 2016, the Code of Virginia (12VAC5-66-10) was amended to include POLST, stating
Durable DNR Order shall also include a physician order for life-sustaining treatment (POLST) form. Durable DNR orders including POLST forms shall be completed and signed by a licensed practitioner and signed by the patient or patient’s authorized representative.
Presently, the Virginia POLST Collaborative is situated in a major palliative care organization and guided by an executive committee. The Collaborative tracks the issuance of each POLST form requested by a healthcare professional. Unfortunately, the Collaborative has failed to reach statewide coverage, particularly in rural areas such as Southwest Virginia (SWVA).
Rural Strengths and Challenges
Rural communities are integral to the American economy and culture and are situated in regions that provide natural, renewable, and reusable resources that contribute to the quality of life for all Americans. Definitions of rurality typically originate from the U.S. Census Bureau (2019) and the U.S. Department of Agriculture, Economic Research Service (2017) Heterogeneous traditions, customs, and social expectations shared by residents vary among communities and across locales. Understanding rural cultures and lifestyles is imperative to creating and implementing interventions (Afifi et al., 2022).
Across social determinants of health, rural populations do not fare as well as urban populations (National Academies of Sciences, Engineering, and Medicine, 2018). Rural areas are often characterized by poor economies and poverty, high numbers of older residents, limited access to goods and services, and isolation. These challenges, the direct result of remote geographic locations. have led rural residents to develop values that often include self-reliance, conservatism, a distrust of outsiders, religion, work orientation, emphasis on family, individualism, and fatalism (Flora, 2016). Research examining rural areas and palliative care is nascent; most studies involve small samples with findings difficult to generalize due to the uniqueness of the location under study (Lalani & Cai, 2022).
Although challenges exist, rural communities have numerous strengths. Characteristics of rural lifestyles can be powerful foundations for change (e.g., strong family ties, faith-based institutions, and connections to the land and community) (Jaffe, 2015). Strengths-based responses are frequently cited approaches for community-based interventions—they build upon existing resources rather than filling in gaps by bringing in outside resources. A strengths-based approach relies on the contributions of individuals, families, communities, and public infrastructure and explores how to connect and mobilize them for individual and community benefit (Becker, 2015).
In SWVA, a largely mountainous region of over 500,000 people, many counties are disproportionally impacted by chronic disease and chronic stress conditions (Khazan, 2015). Woolf et al. (2018) found that residents in SWVA had the highest mortality rates, the lowest median household income, and one of the highest unemployment rates in Virginia.
Methods
To understand the use of POLST in SWVA, our study involved a mixed methods approach, conducted in two phases. Phase I, an online survey, was developed based upon a review of the literature concerning use of POLST as well as suggestions from executive committee members of the Virginia POLST Collaborative. Several members also pilot-tested the survey. Once finalized, the protocols were submitted for IRB approval to Virginia Tech’s Institutional Review Board (protocol #21-187). Upon approval by the IRBs, the Virginia POLST Collaborative sent the survey to all members of Virginia POLST inviting them to participate in the study.
Survey (Phase I)
The online survey included questions concerning participants’ age, gender, primary occupation, and experience. Respondents were asked about the counties and care settings in which they practiced, organizations in which they practiced, and care they provided. Respondents were also asked about POLST: institutional awareness, nature and use by patient population, use of an electronic medical record system, institutional encouragement of the use of POLST, barriers to POLST use, and aids to encourage its use. At the conclusion of the survey was a question asking completers if they were willing to participate in a Zoom interview, and if so, to provide their contact information.
Interviews (Phase II)
As with the Phase I survey, the semi-structured interview questions were reviewed by members from the executive committee of the POLST Collaborative. Questions asked included how the forms had been used in SWVA, resources needed to implement and sustain POLST, and what stymied its establishment in rural SWVA. While the focus was placed on SWVA, health professionals from across the state representing both rural and urban areas were invited to participate.
Data Analysis
Frequencies and percentages were computed in Excel to summarize all categorical and continuous data from answers to the survey questions. Analysis of Phase II interview data occurred in three stages. The first stage took place during the interviews when responses to probe further (e.g., case examples) and to redirect (e.g., general commentary) presented themselves. The second stage included interviewer notes and observations of the information gleaned and the experiences participants shared. The third stage occurred upon completion of each interview when the audio-recorded session was transcribed. Transcripts were thematically coded separately by the authors with particular attention given to commonalities and differences among participants’ answers (Corbin & Strauss, 2014).
Results
Phase I Survey
Surveys took between 10 and 15 min to complete. Out of 101 survey respondents, 75 were women and 25 men; one person preferred not to disclose. About a third of respondents were social workers working in hospice settings, followed by registered nurses, physicians, nurse practitioners, and other healthcare professionals (e.g., ethicist, respiratory therapist, community healthcare worker). Respondents had a range of work experience–between 0 to 45+ years in practice. More than half (52%) had 20 or more years of experience. Few respondents (5%) conducted their work solely in rural areas. Figure 1 shows organizations in which respondents practice, with hospital-based clinics (29%) as the most common setting.

Organizations in which respondents practice.
Familiarity With POLST
The majority of respondents, or 93% (n = 94), had heard of POLST. Figure 2 demonstrates the degree of uptake and familiarity. Notable areas of opportunity include referring patients to a POLST facilitator (37.5% are not referred) and providing educational materials (66% do not provide materials to patients).
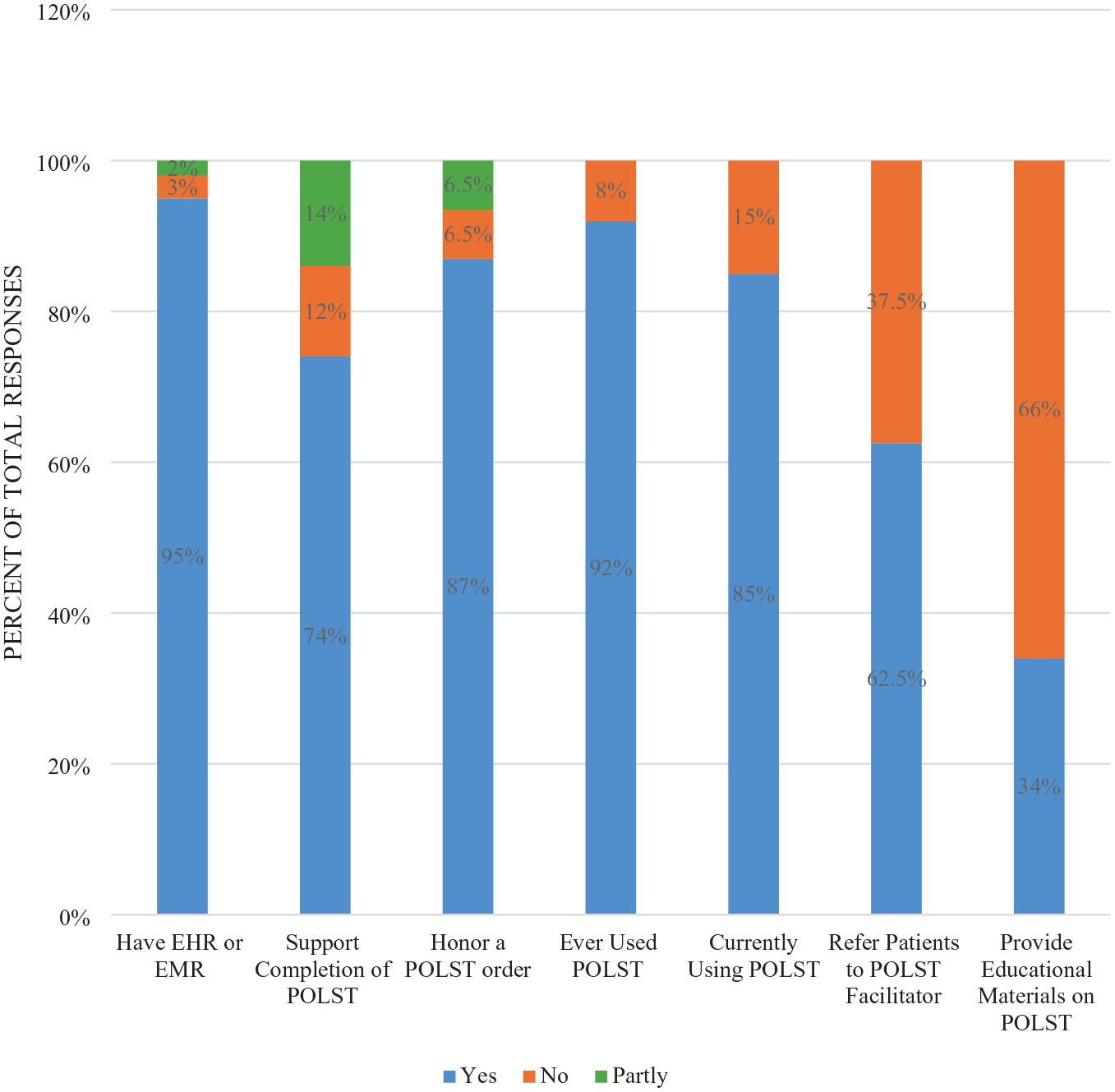
Organizations’ use of POLST.
Barriers to and Supports for Using POLST
The perception that a Durable Do Not Resuscitate order (DDNR) was redundant to POLST was the most frequently cited barrier (22%). Lack of awareness and education was the second most cited barrier (14%). Supports most often identified were readily available online facilitator training (18%), support from organizational administration (16%), receipt of continuing education credit for training (15%), and support from the Virginia POLST Collaborative (14%).
Participant Interviews
Education Uptake
Twenty people were interviewed for 20 to 40 min. The most consistent theme sounded by participants was the importance of education. Educational opportunities not only needed to be conducted for the first time in some areas, but also areas needed to have continuous, consistent, and convenient updates to education, as emphasized by John, a physician.
And I just think that the education and access are the two keys to increasing the use of the POLST form in Southwest Virginia.
Doris, a nurse, stressed that conducting in-person training in rural SWVA presented a unique challenge because of its remoteness from the rest of Virginia.
I just wish there were more facilitator trainers in like the Southwest region or in some of these more remote areas, because I have a full-time job. . ., there were physicians that didn’t understand the form, and they were outside of the [organization] health care system, but they wanted them, but they were in rural areas and they wanted me to travel down there to do the one-on-one education with the physicians.
Jeremy, a physician, emphasized the need for constant training and availability.
. . .training has got to happen frequently. And it’s not a one and done because too many people rotate out of the system. . . .there’s too much transiency in the people.
Related to the need for training was that, without healthcare systems that strongly encourage POLST use and pay for staff training, training would be rendered ineffective for healthcare providers. While systems pay for training of staff and may strongly encourage use of POLST, it is entirely voluntary. A number of participants thought that true uptake would only occur if a healthcare organization required that POLST be used. According to Cassandra, a nurse, You have to start at the top, and then it has to be with the administration, it has to be a policy. In other words, it has to be a policy instituted that we are going to use POLST and then it has to be trained. Every time you have somebody new come in, it has to be part of the onboarding training.
Encouraging Establishment of POLST
According to Elaine, a social worker, changing organizational culture to include the use of POLST takes time.
Getting any medical system to consistently use something new is a challenge. I think that even when they changed the color of a DNR from yellow to white, it was like the shot heard around the world that they just didn’t like it. They would not embrace that.
Robert, an EMT, emphasized the role of EMT education coordinators to help EMTs understand POLST.
So whether you’re at an EMT class at the local Rescue Squad. . .or, if you’re enrolled in a college EMS program, that program director has to be an education coordinator. So, we first have to educate the ones providing the education so that we can start training the folks that are in school now going forward about what a POLST form is and just using that term in exchange for DNR and then we could do a requirement that all EMS providers are required to maintain continuing education hours every two years to maintain their certification.
Challenges for Establishment in Rural Areas
Rural areas pose special challenges because of fewer healthcare providers and specialists overall. Patients may have to travel several hours to see a medical provider, and many patients, particularly older people, may have little to no access or ability to use telehealth services. Elaine, a social worker, observed how rural residents access care, . . . rural areas lack the primary care at home services where if you have these homebound people who are getting to physician offices face-to-face and they also don’t have primary care at home, then they’re basically probably using an ER for their health care needs.
Another nurse, David, who used telemedicine to have end-of-life conversations, stated.
. . .for the most part, my patients are 65 plus, 85 plus. . . I have a fair amount of patients, a good amount of patients that are, you know, of very low socioeconomic status. So, and I have patients that are very high socioeconomic status. So, you know, their understanding of the internet is the same in how to fill out forms.
Discussion and Conclusions
Obvious from the interviews, each healthcare professional was passionate about advance care planning and convinced of the worth of POLST. Most stated their belief during the interview (i.e., “I am talking to you because I am passionate about this”). Moreover, respondents stressed that although systems and some professionals within them may have difficulty with POLST, the POLST conversation and form is typically welcomed by their patients. Healthcare professionals have an opportunity to respect their patients and their preferences using POLST (Tolle, 2021).
Importance of Stakeholders
Many respondents stressed that POLST uptake would occur across Virginia when important stakeholders were convinced of its worth and stressed that culture change had to occur in three areas. First, major healthcare organizations, both acute and long-term care, needed to make it a policy that its members were trained in how to use the form. Second, physicians must support POLST, particularly those in palliative care, internal medicine, oncology, geriatrics, and emergency medicine. A number of respondents mentioned that, in rural areas, primary care physicians need to be included because for they are the only physician that a patient might ever see. Finally, many respondents emphasized the importance of grassroots support.
Importance of the Virginia POLST Collaborative
The Virginia POLST Collaborative is critical to the success of POLST uptake. An important way for the Collaborative to be more efficacious is for it to have consistent state funding for education, administration, and evaluation. Stable financial support would enhance training and outreach efforts and increase dissemination of information to healthcare providers and the patients. The location of the headquarters of the Collaborative in Northern Virginia makes uptake in rural SWVA a challenge because of the distance required to travel from one end of the state to another for in-person training.
Costs of Training
In addition to the need for training, a need exists for funding and time to attend the training. Respondents emphasized that costs for training were prohibitive for some professionals and should be borne by their healthcare system, not by an individual. Employer payment for training would increase the likelihood that completion of POLST forms becomes a standard of practice.
Opportunity costs were another problem with training. Many respondents remarked that the training took too much time away from the work of busy healthcare professionals and that organizations could not spare the time away from the office.
Virtual Training for Healthcare Professionals
A solution to the opportunity cost of lost time due to traveling and lack of coverage is the use of technology. Most healthcare systems in SWVA have the bandwidth to conduct on-line training. Although meeting in-person may be preferable, using a virtual platform such as Zoom or Teams presents a viable and efficient method to train people in hard-to-reach areas and to provide important networking opportunities.
Virtual POLST Conversations With Patients
Having a goals of care conversation took time that many healthcare professionals simply did not have. Conducting important and patient-centered goals of care conversations virtually has potential for some rural populations. An argument rebutting the time problem is that having goals of care conversations is reimbursed by Medicare. Although not all providers were aware of the reimbursement, many were aware and stressed that using reimbursement codes for the end-of-life goals of care conversations could facilitate POLST implementation.
Measuring POLST Goals
Stable funding for POLST is critical for sustainability. While research generally supports the use of POLST, no Virginia studies have been conducted. For long-term success that does not rest on the good will and passion of its advocates, outcomes should be clearly specified and measured. With data for credible outcome measures, the “policy community” can provide critical leverage for improving rural uptake of POLST.
Need for Consistent Champions
Many respondents identified the need for POLST champions and stressed that there should be several champions because healthcare professionals often move in and out of the area. It is especially important that champions of POLST are identified and nurtured in SWVA; POLST should become a routine component of onboarding for staff who may have the opportunity to use it. Mentioned earlier, promising avenues are through healthcare organizations, physicians, and grassroots efforts.
Limitations
These findings represent information from persons highly invested in POLST. It is unlikely that detractors either completed the survey or were interviewed. Thus, problems associated with POLST were not a part of these data. A remedy for the next study would be to conduct a survey and interviews drawn from the entire state and disseminated through a hospital or long-term care association rather than the POLST Collaborative.
Conclusion
In summary, it is important to increase the uptake of POLST in SWVA and other rural areas of the state. While voluntary, health care systems should institute policies that provide a clear message to primary care providers, staff in long-term care facilities, and regional hospitals and clinics, that their organization strongly encourages POLST conversations and form completion. Model policies that already exist, such as those used by health systems already supportive of POLST use, can serve as an excellent starting point for other healthcare systems.
Respondents indicated that, although presenting challenges, the pandemic created moments of illumination, such as the usefulness of a viable, virtual instructional environment as well as viable, virtual networking environments to engage in goals of care conversations. Despite challenges with rural broadband, online training related to POLST should proceed with dispatch.
In the future, it is critical to collect data on POLST. Abundant examples from the literature on POLST exist. Once conducted, findings can assist with the institution of POLST across the state. Data should be collected on the utility of online versus in-person training as well as on similarities and differences between POLST for younger people versus older people. Also, studies should examine similarities and differences between rural and urban areas.
Individuals who live in rural areas, like SWVA, are often disenfranchised due to their remote location. Ethically, a patient’s location should not determine their ability to direct care at the end of life. For rural people who are individualized, strong, and wise, it is time to devote attention, energy, and resources to the implementation of POLST. The work and will of the many people who responded to this survey and participated in the interviews present an opportunity to increase momentum to implement POLST in rural areas in Virginia.
Footnotes
Author Note
The research project was approved by Virginia Tech’s Institutional Review Board (protocol #21-187).
Consent to Participate
Written consent was obtained by participants who participated in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.