
Abstract
Introduction:
Little is known about whether liking a person to reduce alcohol drinking (social pressure) might be related to mortality.
Objectives:
To analyze whether social pressure and an intention to reduce alcohol drinking may be related to time to death in an adult general population sample.
Methods:
Among the general population in northern Germany at age 18 to 64, a random sample had been drawn. Included in this study were persons who had consumed alcohol 3 or more times a week or drank 27 g pure alcohol per drinking day or had 1 or more alcohol dependence criteria or problems fulfilled. These persons provided data about social pressure and an intention to reduce alcohol drinking and were known to be alive or deceased 20 years later. Associations between social pressure and time to death were calculated.
Results:
Among the sample, 4075 (69.9%) residents participated at baseline, and 2060 fulfilled the inclusion criteria for this study. High social pressure to reduce alcohol drinking was related to a short time to death (hazard ratio 1.78; 95% confidence interval 1.17-2.73) after adjustment for the amount of alcohol drinking, an intention to reduce it, age, and sex.
Conclusion:
The finding suggests that social pressure to reduce alcohol drinking in addition to the amount of alcohol drinking is part of a trajectory of alcohol consumption leading to death in this general population sample.
Introduction
Support from partner, family or friends has been identified as 1 main factor that might add to change behavior among persons with alcohol problems. 1 Social support has been assessed as having persons who are expected to provide help if needed in a variety of daily problems. Compared to those with highest social support all other persons had increased odds ratios of an alcohol dependence or abuse. 2 The less support people perceived the more likely they were to have an alcohol use disorder. 3 It has been concluded that social support might be important for diminishing the risk of an alcohol use disorder. 3 Little is known about support that is more alcohol-specific, particularly motivating an alcohol consumer to drink less or to enter treatment of alcohol problems. Having close persons who may support has been shown to be associated with the confidence to reduce or stop alcohol consumption. 4 Being certain to receive support in the endeavor to reduce alcohol consumption has been revealed by data to be associated with better outcomes in terms of alcohol consumption than not having this belief.1,5 This was found for treatment-seeking alcohol drinkers1,5 and in the general population. 2
One kind of alcohol-specific social support is an effort to increase the intention to reduce or stop alcohol drinking. Liking an alcohol consumer to drink less has been expressed as social pressure to reduce alcohol drinking by the provision of feedbacks that are directed to reducing the alcohol drinking of a person. 6 The more alcohol is consumed the more likely is social pressure. This was found across nations. 7 Social pressure has been found to be a main factor of motivating a person to seek help for alcohol problems or to drink less. 8 Among men with an alcohol dependence in their history, the majority mentioned pressure from family or peers as a reason for their recovery. 9 In another study, persons who had remitted from their alcohol dependence without treatment did not differ in social pressure provided by their partner or relatives from alcohol dependent persons who were currently drinking alcohol. 10 Also, in a comparison of persons who remitted from alcohol dependence with or without treatment no statistically significant difference in social pressure to reduce drinking was found. 11 The data revealed a trend toward more social pressure from partner in the group who had utilized treatment.
Social pressure has been analyzed in samples of the general population. In the United States of America, 7.1% of an adult population sample disclosed social pressure to drink less alcohol. 12 Among study participants with social pressure, 44.9% confirmed alcohol-related harm. 13 The likelihood of having received social pressure to reduce alcohol drinking was the higher the more alcohol drinking had been disclosed. 12 Alcohol-related harm, being a man, and age younger than 50 years was associated with having received more social pressure compared to no alcohol-related harm, being a woman, and at age 50 or older. 13 Unfavorable characteristics such as drug in addition to alcohol use may increase the likelihood of having received social pressure. 14
Social pressure might increase or even be a main driver of the intention to reduce alcohol consumption. 6 It has been estimated to be low among people with problematic alcohol use in population samples.15,16 Intention to reduce alcohol drinking predicted treatment outcome 17 and moderation of drinking among excessive alcohol consumers. 18 Data of alcohol dependent persons revealed that the intention to reduce alcohol drinking was higher among patients in a general hospital than among the general population. 19 This finding speaks in favor of health disorders and intention to reduce alcohol drinking being associated with each other if alcohol drinking is perceived as a threat to survival. 6
Social pressure and intention to reduce drinking have been analyzed largely in the context of alcohol dependence. It is unclear whether it might exist among the entire population and across moderate to very high alcohol consumers. A broader spectrum of drinking behavior and problem severity than among treatment samples may be expected. Social pressure may be provided by relatives or friends in an effort to motivate an alcohol consumer to drink less. But also, relatives or friends might threaten the drinker to stop their help or terminate their relationship with the drinker. According to public health, the provision of social pressure and the support of an intention to reduce alcohol consumption could be understood as core steps in the curtailment of alcohol consumption, alcohol-related health disorders, and premature death.
It is unclear whether social pressure and intention to reduce alcohol drinking in addition to the amount of alcohol consumed are related to mortality. An expectation may be that social pressure adds to life expectancy. The reason is that the amount of drinking in lifetime could be curtailed by social pressure. It is largely unknown whether social pressure and the intention to diminish alcohol drinking is related to a gain in life expectancy. Also, a need of knowledge about the kind of social pressure was stated. 8 The aim of the present paper is to analyze time to death among persons with social pressure to reduce alcohol drinking using intention to decrease alcohol drinking, the amount of alcohol consumption and alcohol dependence as covariates in a general population sample. We hypothesized that the higher the social pressure is the higher is the probability of longer survival.
Methods
Sample
For this mortality cohort study, at baseline a random adult general population sample had been drawn from a total of 193 452 residents at age 18 to 64 in a northern German area using the data files of the residents’ registration offices of 47 communities.20,21 Exclusion criteria were: person unknown at the address which we had received, nationality other than German, had moved out of the sampling area or was institutionalized. From July 20, 1996, to March 18, 1997, standardized interviews were conducted face to face at home of or another place preferred by the study participant. For the inclusion in the present study 1 or more of 3 criteria had to be fulfilled: (1) having consumed alcohol 3 to 4 times a week or more frequently in the last 12 months or prior to this time with a duration of 6 or more months. (2) The respondent consumed more than 27 grams pure alcohol per drinking day in the last 12 months prior to the interview or with a duration of 6 or more months before the last 12 months. (3) The respondent confirmed 1 or more alcohol dependence criteria 22 or 1 or more problems associated with alcohol drinking: health disorders, problems in personal relationships, financial problems, having been exposed to the risk of injuring or having injured oneself under the influence of alcohol, problems with police, at work, school or home because of alcohol drinking. At mortality follow-up, vital status was ascertained from April 1, 2017, to April 30, 2018. For that purpose, the data files of the residents’ registration offices were screened. All persons who fulfilled the inclusion criteria for the present study and for whom vital status data were received are the final sample for the present data analysis.
Assessments
At baseline, all assessments were part of or embedded in the internationally standardized Munich-Composite International Diagnostic Interview.20,23 The questions were asked face to face or by questionnaire to be answered in 1 session. Social pressure to reduce alcohol drinking was assessed by the German language Social Pressure Scale, 6 a standardized questionnaire. We used the 8 questions that refer to specific persons in lifetime before baseline. They were introduced by “It may happen that people are confronted by others in their environment with the alcohol drinking or that the alcohol consumption may elicit certain situations. The following questions refer to such occurrences or situations.” “Did your spouse or partner ask you to drink less alcohol or to behave in another way when you have drunk alcohol? If yes: Did that result in a threat to your relationship or the termination of the contact?” Equivalent questions were presented according to further 7 persons: mother, father, other relative, close friend, another friend, another person the respondent lives together with, anybody else. The value range for each question was 0 to 2 for not having been asked (0) over having been asked and this had not resulted in a threat of the relationship or the termination of the contact (1) to having been asked and this had resulted in a risk of the relationship or the termination of the contact (2). We added the values up to a sum score of social pressure to reduce alcohol drinking with a range of 0 to 16. The German language Social Pressure Scale has been revealed by data of a general population sample to be internally consistent with a Cronbach’s Alpha of .85 among persons who consumed alcohol in high amounts. 24 The time frame of the questions was the lifetime before baseline.
An intention to reduce alcohol drinking was assessed by questions about contemplation and action to reduce alcohol drinking from the German language Readiness to Change Questionnaire. 25 The Readiness to Change Questionnaire 25 is an instrument to assess an intention to reduce alcohol consumption by the allocation to the stages of change according to the Transtheoretical Model of Behavior Change. 26 The items mainly refer to the present, no specific time frame is given. The questionnaire has sufficient psychometric properties according to an analysis of a general population sample including high or very high alcohol drinkers. 26 Four questions represented contemplation and 4 questions represented action based on the Transtheoretical Model of Behavior Change. 27 An example for contemplation was “My drinking sometimes is a problem.,” for action “I do change my drinking habits right now.” The answers were ordered in 5 ranks from 1 (“Do not agree at all”) to 5 (“Agree very much”). We added the values of the 8 questions up to a sum score of an intention to reduce alcohol drinking with a range of 8 to 40.
The amount of alcohol consumption and alcohol dependence had been assessed as part of the interview. The study participant was asked whether s/he had consumed alcohol 12 or more times in life before. If this was the case the respondent was asked how often s/he had consumed 1 or more drinks per drinking day in the last 12 months prior to the interview or in a former time period (almost every day, 3-4 times a week, 1-2 times a week, 1-3 times a month, less often than once a month). Then the person was asked how many drinks s/he consumed usually per drinking day. For estimating the quantity of alcohol consumption, single glasses and bottles of beer, wine, long drinks, liquors, and spirits representing a variety of quantities were presented on a card, and the respondent specified the number of glasses or bottles consumed. As part of the Munich-Composite International Diagnostic Interview, alcohol dependence at any time in life before baseline was diagnosed according to the criteria of the Diagnostic and Statistical Manual of the American Psychiatric Association.20,22
For mortality follow-up, vital status data were retrieved from local residents’ registration offices and a national address data base of Germany. The data included whether the study participant was alive or deceased and if so at what date. The date had been provided by the physician in the death certificate. This has to be transferred to the registry office within 3 days by law. The date of death is then included in the data files of the residents’ registration office of the last place of residence of a person. Address changes have to be reported to the residents’ registration office by the resident, and the offices certify the new address as the current place of residence.
Data Analysis
The data analysis was performed using proportions, the Pearson chi 2 test, and Cox proportional hazards regression analysis with time to death as the dependent variable. The social pressure sum score was collapsed to no (value 0), medium (value range 1-3), and high social pressure (value range 4-16). We built these 3 categories according to 3 criteria. The Cox proportional hazards assumption had to be fulfilled. The number of death cases per category had to be 5 or higher. 28 If the collapsing of categories with similar hazard ratios led to significant results the categories were collapsed. In an equivalent approach the intention to reduce alcohol drinking sum score was collapsed to no (value range 8-14) or yes (value range 15-40).
The number of alcoholic drinks that had been consumed was calculated in grams pure alcohol in the understanding that 1 drink equals 9 g pure alcohol. The amount of alcohol drinking was divided into moderate, high, and very high. Moderate drinkers were study participants who had never fulfilled the criteria for high or very high alcohol drinking in life. A high drinking amount was assumed if women had consumed 20 to less than 40 g/day for 6 or more months in their life before or 65 or more grams once a month or more often and men 40 to less than 60 g/day for 6 or more months in their life before or 100 or more grams once a month or more often. Grams pure alcohol per day of a month had been calculated by the product of number of drinking days per month and the grams pure alcohol per drinking day. Very high alcohol consumption was assumed if women had drunk 40 or more and men 60 or more grams pure alcohol per day. All drinking amounts must have been valid for the last 12 months prior to the interview or for any time period of 6 or more months before the last 12 months.
Missing values were found in the data about social pressure, an intention to reduce drinking, alcohol consumption, and living alone. They were replaced by the mean using 10-year age groups and sex. All data analysis was performed using the Stata 18 software. 29 We present proportions, the Pearson chi 2 with a significance level P < .05 and the hazard ratio (HR) with 95% confidence interval (CI) according to Cox proportional hazards analysis. A hazard ratio is interpreted as significantly increased if both boundaries of the CI are 1.00 or higher. Analysis time was the time from baseline to mortality follow-up or death if before mortality follow-up. It was safeguarded that the Cox proportional hazards assumption was fulfilled using Schoenfeld residuals. The tests of the Cox proportional hazards assumption were performed for each model separately. All tests revealed that the Cox proportional hazards assumption was fulfilled. Relations of social pressure, intention to reduce alcohol consumption, and the amount of alcohol drinking with time to death were analyzed in 4 models. In model 1 four variables were tested, each in a separate analysis and adjusted for age and sex: social pressure, intention to reduce alcohol consumption, amount of alcohol consumption, and alcohol dependence. Model 2 included social pressure and the intention to reduce alcohol drinking adjusted for age and sex. In model 3 the amount of alcohol consumption was added to model 2. In model 4, alcohol dependence was added to model 3. We calculated cumulative hazards of the amount of alcohol consumption and social pressure adjusted for age, sex, and an intention to reduce alcohol drinking. This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 30 (Supplemental File 1).
Results
Study Participants
At baseline, among the sample of 6447 residents, 618 (9.6%) fulfilled the exclusion criteria. Among the remaining 5829 persons, the interview could not be realized for 1754 persons due to refusal, no contact realized, severe disease, interview incomplete or not face to face or other reasons. Interview data were provided by 4075 (69.9% of the included persons). 21 Of these, at mortality-follow-up vital status could not be verified for 47 persons (1.2%). Reasons include special data protection for single persons or having moved to an unknown address. For 4028 (98.8%) vital status data were received. Among them, 2060 fulfilled 1 or more of 3 criteria for the inclusion in the present study. The median time from baseline to mortality follow-up was 20.6 years. 31
The variables of social pressure among the 2060 study participants included a mean proportion of 1.99% missing values (range: 1.84%-2.67%). The variables of the intention to reduce drinking included a mean of 1.95% of the values of the 2060 study participants missing (range 1.84%-2.18%). The questions about alcohol consumption included 9, the question about living alone 2 missing values.
In the total sample with vital status data, among women 38.68%, among men 63.50% fulfilled the inclusion criteria for the present study (Table 1). Among persons who lived together with others in 1 household, 50.94% were included in the study. Of those with a very high drinking amount, 20.31%, of those with moderate drinking, 1.28% received high social pressure (Table 2).
Sex, Age, Living Alone of Study Participants in the Sample at Baseline.

Abbreviations: df, degrees of freedom; ns, not significant: P, probability of error.
Sex, Age, Living Alone, Amount of Alcohol Drinking and Alcohol Dependence by Social Pressure and Intention to Reduce Alcohol Drinking at Baseline.

Abbreviations: df, degrees of freedom; n, number of persons; ns, not significant; P, probability of error.
% Total may include rounding errors. Proportions may include rounding errors.
Social Pressure and Intention to Reduce Alcohol Drinking at Baseline
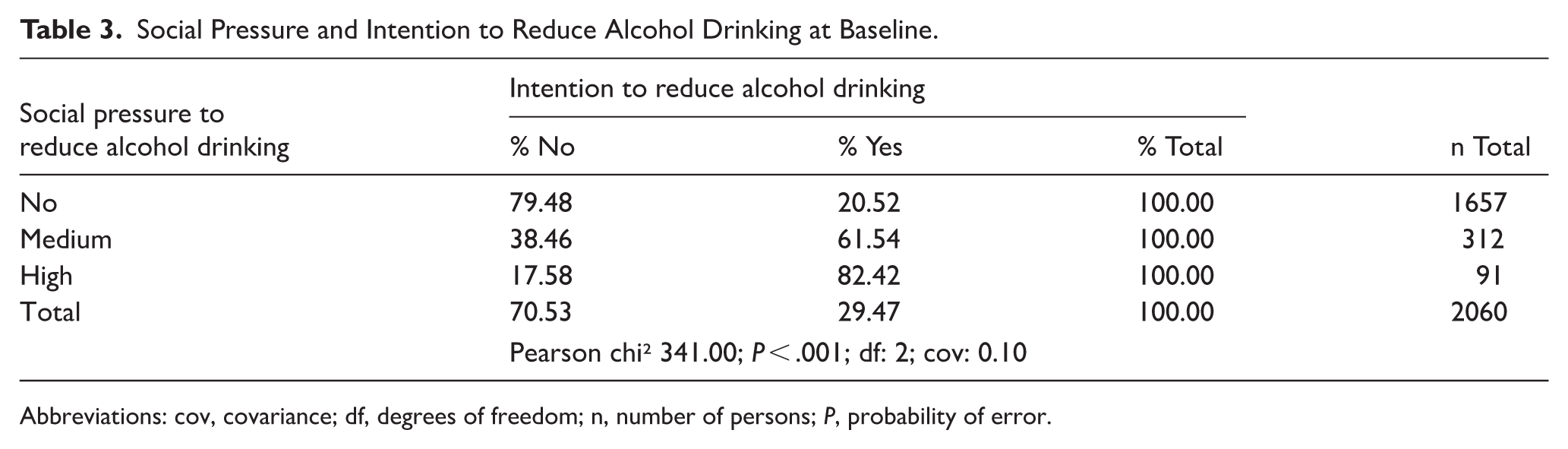
Both social pressure and an intention to reduce drinking were rather evenly distributed across 3 age groups (age at baseline: 18-33; 34-49; 50-64): 19.02% to 20.15% disclosed any social pressure and 29.11% to 29.67% an intention to reduce drinking (Table 2). Greater alcohol use was associated with higher social pressure and with a higher likelihood of an intention to reduce alcohol drinking. Among the 2060 study participants, 19.57% declared that they had perceived medium or high social pressure to reduce alcohol drinking. Among the study participants with moderate drinking in their lifetime before baseline, 12.36% had perceived medium or high social pressure to reduce alcohol drinking. Among all study participants who drank alcohol at very high amounts in their lifetime until baseline, 50.20% declared medium or high social pressure. Among the alcohol dependent persons, 82.37% had disclosed social pressure. An intention to reduce alcohol consumption was present for 22.50% of the study participants with moderate and for 58.62% of the study participants with very high drinking amounts. Social pressure and the intention to reduce alcohol consumption were associated with each other (Table 3). Among study participants with high social pressure, 82.42% intended to reduce alcohol consumption.
Social Pressure and Intention to Reduce Alcohol Drinking at Baseline.
Abbreviations: cov, covariance; df, degrees of freedom; n, number of persons; P, probability of error.
Time to Death
The proportion of deceased persons was 32.97% of the study participants with high social pressure and 14.97% of those without social pressure (Table 4). Persons with high social pressure had a hazard ratio 2.78 (95% CI: 1.89-4.07) to die early compared to those without social pressure after adjustment for age and sex (Table 5; model 1). Time to death turned out to be the shorter the higher the social pressure was after adjustment for age, sex, and an intention to reduce alcohol drinking (model 2). High social pressure was related to early death also after additional adjustment for the amount of alcohol drinking (model 3), not however after inclusion of alcohol dependence in the model (model 4). We alternatively also adjusted for the number of alcohol dependence criteria (HR 1.13, 95% CI: 1.03-1.23) in addition to an intention to reduce alcohol drinking, amount of alcohol consumed, age, and sex. Social pressure was not significantly increased.
Social Pressure and Intention to Reduce Alcohol Drinking, Amount of Alcohol Drinking, Alcohol Dependence at Baseline and Deceased Study Participants 20 Years Later.

Abbreviations: df, degrees of freedom; N, number of persons in the analysis; n, number of deceased persons; P, probability of error.
Social Pressure and Intention to Reduce Alcohol Drinking, Amount of Alcohol Drinking, Alcohol Dependence at Baseline and Time to Death 20 Years Later.

Abbreviations: CI, 95% confidence interval; HR, hazard ratio; nim, not included in the model; ref, reference group.
Cox proportional hazards regression analysis. Model 1: Each single HR in a separate model adjusted for age and sex. Models 2 to 4: HR in the column in 1 model adjusted for age and sex. All models fulfilled the Cox proportional hazards assumption.
Persons with an intention to reduce alcohol consumption were more likely to die early than those without after adjustment for age and sex (model 2). The data analysis revealed a hazard ratio 1.47 (95% CI: 1.15-1.89). An intention to reduce alcohol consumption was also related to time to death after adjustment for the amount of alcohol drinking and alcohol dependence in addition to social pressure, age, and sex (model 4; HR 1.36; 95% CI: 1.06-1.75). We analyzed interaction between social pressure and an intention to reduce alcohol consumption. We added the product of these 2 variables in models 2 to 4. The data revealed that there was no interaction present, neither using the variables without the single categories nor with them.
Higher amounts of alcohol use were associated with earlier death. For persons who had drunk alcohol at high or very high amounts in their life before baseline, increased hazard ratios for early death were found. The data revealed increased hazard ratios for time to death in addition to high social pressure and an intention to reduce alcohol drinking in 1 model (model 3). The cumulative hazards data of the amount of alcohol consumption and of social pressure revealed the highest hazards for the persons with very high alcohol consumption and high social pressure and the lowest cumulative hazards for those persons who had drunk alcohol in moderate amounts and who had not experienced social pressure. Compared to these, persons with moderate alcohol consumption who had reported medium or high social pressure had higher cumulative hazards (Figure 1).

Alcohol drinking and social pressure. Cox proportional hazards regression adjusted for age, sex, intention to reduce alcohol drinking.
Discussion
This study has 4 main results. First, social pressure and the intention to reduce were found across all amounts of alcohol consumption including moderate drinking. Second, higher social pressure to reduce alcohol drinking was associated with higher amounts of alcohol drinking. Third, social pressure and the intention to reduce alcohol consumption were associated with each other. Fourth, high social pressure was related to short time to death after adjustment for an intention to reduce alcohol drinking and for its amount.
First, the data revealed that social pressure seems to exist across populations with moderate up to those with very high alcohol drinking. This result speaks in favor of social pressure not being limited to alcohol dependent persons. The finding adds to the evidence that a variety of alcohol consumers among the general population may perceive social pressure to reduce alcohol drinking beyond those who need help for alcohol problems.1,6,9 -13 Similar to social pressure, an intention to reduce was found across different amounts of alcohol drinking. Among the moderate alcohol consumers, 22.50% intended to reduce their alcohol consumption. However, no interaction effect between social pressure and an intention to reduce alcohol consumption was found.
Second, our data revealed that higher alcohol consumption was associated with a higher proportion among the study participants who had perceived social pressure from persons of their social network. Among those with moderate alcohol drinking, 12%, among those with very high drinking amount 50% received social pressure. This confirms data from other general population samples according to which persons with higher drinking amounts included more persons with social pressure than study participants with low drinking amounts12,13 One potential reason might be that families and friends of alcohol consumers could hesitate with a feedback until problems around alcohol become particularly evident in the life course. We analyzed both alcohol drinking amount and alcohol dependence because the amount of alcohol that has been consumed is likely to determine the health disorders that might contribute to the trajectory to death. Alcohol dependence may be associated with a variety of specific problems and conflicts in a social network. Problems or conflicts from for example, alcohol withdrawal, urge to drink or denial of problems might stimulate family, friends, or other to exert social pressure. This finding is plausible considering that among alcohol dependent persons the highest proportion of study participants, more than 80% perceived social pressure. This corresponds to evidence before according to which the majority of alcohol dependent men mentioned social pressure. 9 On the other hand, social pressure has also been present among those who had consumed alcohol in a moderate amount.
Third, social pressure was associated with an intention to reduce alcohol consumption. More than 80% of the study participants who had disclosed high social pressure also confirmed an intention to reduce alcohol consumption. This corresponds to evidence before.6,18 The respondents were open to refuse answers at any time, and no conditions were attached to the provision of the answers in the interview. We assume that the responses are valid. The findings might speak in favor of social pressure to be a suited approach to increase an intention to reduce alcohol drinking.
Fourth, higher social pressure to reduce alcohol drinking was associated with shorter time to death. This result remained after adjustment for intention to reduce alcohol drinking and for amount of alcohol drinking in addition to age and sex. If alcohol dependence was also considered social pressure was not significant any more. These findings suggest that alcohol dependence and alcohol consumption are the main factors of the association with diminished survival. The alcohol that has been consumed is one causal factor for the health disorders that are involved in the trajectory to death. The data do not provide any information about effects of social pressure. It might indicate a subpopulation of alcohol consumers with a partner, family, friends, or other persons who provide social pressure to reduce drinking. The data also speak in favor of severe alcohol-related problems in this subpopulation. The finding is opposite to what we hypothesized. It did not affirm that social pressure may add to longer survival. Although social pressure may have had beneficial effects the data did not reveal an expectancy of a long life for those study participants who had received social pressure. Permissive norms about drinking in the network of the alcohol consumer as well as in the nation may play a main role in that. Social pressure may have been provided too late in a life course of an alcohol consumer. The results speak in favor of motivating the social network to intervene early in an alcohol trajectory of a network member and in an effort to prevent alcohol consumers from early death.
The cumulative hazards of the amount of alcohol drinking and of social pressure are in a plausible order. In each of the person groups with medium, high, and very high alcohol consumption those without social pressure have the lowest and those with high social pressure the highest hazards of a short time to death. The cumulative hazards data revealed that even among moderate alcohol consumers social pressure appears to be an indicator of a short time to death. Reasons for these results among other may be denial of a higher alcohol drinking amount.
Social pressure to reduce alcohol drinking differs from social support in 2 aspects. Social pressure is alcohol-specific in that the alcohol consumer is requested to cut down on drinking. The relationship between the person who provides and the person who receives social pressure may change or the contact may be terminated. This could be one of the reasons for our finding that social pressure was more likely among study participants with high alcohol consumption or dependence than among those with moderate alcohol consumption or without alcohol dependence. This could also be an indicator of further alcohol consumption which might have added to a short time to death. It seems plausible that this is in contrast to findings according to which social support is associated with good alcohol-related outcomes among treatment samples1,5 and an alcohol use disorder being less likely among persons with the highest support in the population.2,3
Social pressure may be a problem in interpersonal relationships that include a heavy drinker. Requests from loved ones to drink less may motivate the drinker to reduce or stop alcohol consumption in a part of cases, among others not. After having given up a relationship the alcohol drinker may increase the consumption. One approach to diminish this problem might be to intervene early in the life course of an alcohol consumer and to support social norms of cutting down drinking or abstaining from alcohol.
The findings of this study have a variety of implications for efforts to reduce alcohol drinking in the general population. It must be considered that the intention to reduce alcohol consumption has been found to be low in populations.15,16 Motivating people to provide social pressure as early as possible in a drinking trajectory seems promising. The findings speak in favor of strengthening endeavors to provide social pressure in social networks of alcohol consumers whoever is involved. This may be the partner, family, friends, neighborhood, or workplace. Messages should include to care for drinking less among family or friends. The advantage is twofold. First, drinking less even among persons with low to moderate alcohol consumption probably adds to the reduction of alcohol consumption in the entire nation. Second, social pressure among any drinker irrespective of the drinking amount may contribute to decrease the incidence of alcohol dependence or other alcohol-related disorders. Third, people should not hesitate to use social pressure if the drinking amount is not high and harm not obvious. The findings suggest that in addition to addressing drinkers themselves it seems useful to motivate people to keep an eye on the alcohol consumption of loved ones or people in a less close relationship and to have the heart to provide social pressure. These conclusions are particularly justified by the finding of the relations between social pressure and the intention to reduce alcohol drinking. Further studies could explore kinds of social pressure and how to address persons who may provide it.
Strengths and limitations
Strengths of the study include that a random adult general population sample was used among which 69.9% participated in the baseline data collection. Assessments included standardized instruments. Social pressure was measured by a standardized questionnaire for which data of reliability exist. Alcohol consumption had been assessed in detail, alcohol dependence according to diagnostic criteria. The mortality follow-up time was 20 years. At least 5 limitations of the study have to be considered. First, social pressure and alcohol consumption may have been under-, the intention to reduce alcohol consumption overreported. Several barriers to disclose social pressure may have existed. The alcohol consumer must recognize social pressure, must be willing to admit it to her-/himself, and must be willing to disclose it in the baseline questionnaire. These steps make selection bias likely. In addition, the perception of social pressure was assessed from self-statements of the alcohol consuming person only, not from members of the social network who tried to motivate the alcohol consumer to reduce drinking. Underreporting of alcohol consumption is likely because only self-report of alcohol consumption was used. Furthermore, memory deficits may have interfered with self-report. On the other hand side, participation in the survey was not attached to any conditions, and the respondent was free to terminate the interview or to refuse a response at any time. Second, social pressure was used with only 3, an intention to reduce alcohol drinking with only 2 categories. The limited number of deceased persons precluded a data analysis of all categories of social pressure and an intention to reduce alcohol drinking with respect to time to death. Third, no sample size calculation had been done for the study. Fourth, no conclusion may be drawn according to the Transtheoretical Model of Behavior Change or criticisms on it. 32 Fifth, according to the time period of 20 years that is spanned by the present cohort study, diagnostic classification systems used at baseline are outdated.
Conclusions
Data of this mortality cohort study revealed that pressure from partner, relatives, friends, or other persons to reduce drinking of an alcohol consumer existed across study participants with moderate up to very high drinking amounts. Higher alcohol consumption was associated with higher social pressure. The results speak in favor of social pressure not being limited to alcohol dependent persons. Social pressure might have increased an intention to reduce alcohol consumption. Social pressure in addition to the amount of alcohol consumption was related to early death. This finding suggests that social pressure may be part of trajectories of alcohol-related harm. The results support endeavors to provide social pressure earlier in these trajectories. The results speak in favor of efforts to encourage social pressure to reduce drinking in the entire general population. This might add to preventive efforts to reduce alcohol drinking and add to provide social pressure to drinkers as early as possible in trajectories of drinking and drinking-related harm. More efforts to develop effective kinds of social pressure and ways to deliver it should be explored in the future.
Supplemental Material
sj-doc-1-sat-10.1177_29768357251408951 – Supplemental material for Social Pressure to Reduce Alcohol Drinking and Mortality 20 years Later in a General Population Sample: A Cohort Study
Supplemental material, sj-doc-1-sat-10.1177_29768357251408951 for Social Pressure to Reduce Alcohol Drinking and Mortality 20 years Later in a General Population Sample: A Cohort Study by Ulrich John, Hans-Jürgen Rumpf, Monika Hanke and Christian Meyer in Substance Use: Research and Treatment
Footnotes
Acknowledgements
No.
Ethical Considerations
No approval of an institutional review board was needed in the years when the baseline part of the study had been conducted (1996-1997). The study protocol has been reviewed retrospectively by the Ethics Committee of the University Medicine of Greifswald and retrospective approval has been granted, approval number BB 044/13, August 16, 2016, and May 02, 2013. The mortality follow-up part of the study had been approved by the ethics committee of the University of Greifswald (approval number BB 044/13).
Consent to Participate
Informed consent for being included in the study was obtained from all study participants. All study participants had been informed that they were free to withdraw consent at any time. Informed consent was not written because at the time of baseline assessments this was not needed. This consent protocol was retrospectively reviewed by the Ethics Committee of the University Medicine of Greifswald (BB 044/13). The written study information and the written data safety statement that had been given to the study participants was part of the material based on which the ethics committee approved the study. Consent for publication was part of the informed consent. It was ensured that no individual study participant could be identified in published material. Consent was not required for mortality follow-up because it was based on publicly available data.
Author Contributions
Ulrich John, Hans-Jürgen Rumpf, and Christian Meyer were involved in the study design, funding, conceptualization of the data analysis, the data analysis, and the writing of the manuscript. Monika Hanke was involved in the data gathering, data analysis, and the writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by grants from the German Federal Ministry for Education and Research (grant number: 01 EB 9406) and the German Research Foundation (DFG; grant number: JO 150/11-1; ME 3180/4-1; RU 1570/3-1).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.