
Abstract
Background:
Detoxification is often identified as treating drug withdrawal. All drug classes except hallucinogens and inhalants include withdrawal as diagnostic criteria for a substance use disorder diagnosis. This descriptive study provides an analysis of detoxification admissions for individuals with hallucinogens or inhalants as their primary substance.
Objectives:
This research aimed to explore the characteristics of these detoxification admissions, focusing on demographics, substance use patterns, and treatment characteristics.
Design:
This retrospective study used annual cross-sectional data.
Methods:
Using the Treatment Episode Dataset Admissions 2006 to 2022 file, data from 8919 detoxification admissions over a 17-year period from publicly funded treatment facilities in the United States were examined.
Results:
During the 17-year period, n = 6761 and n = 2158 detoxification treatment episode admissions had the primary substance hallucinogens and inhalants, respectively. Polysubstance use was prevalent among both samples, with 66% among the hallucinogen sample and 48% among the inhalant sample, with alcohol, cannabis, and cocaine/crack being the most commonly co-used substances. A total of 2872 cases were identified as only having hallucinogens and/or inhalants without other drug classes as reported substances during admission.
Conclusion:
These preliminary findings highlight detoxification admissions among individuals with primary substances that do not meet diagnostic criteria for withdrawal. More research is needed to better understand the context of detoxification among individuals with hallucinogens or inhalants as their primary substance.
Introduction
In the United States (U.S.), approximately 3% and 1% of the population used a hallucinogen or an inhalant, respectively, 1 with 0.2% of individuals having a hallucinogen use disorder and 0.1% having an inhalant use disorder in 2023. 2 Withdrawal is 1 of 11 symptoms used for a person to meet the criteria for a substance use disorder (SUD) according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. 3 Withdrawal diagnoses are present in drug classes such as alcohol and tobacco, but there are no such diagnostic criteria for an SUD with hallucinogens or inhalants. 3 While the International Classification of Diseases, 10th Revision, Clinical Modification has withdrawal codes for other drug classes (eg, F12.13 Cannabis abuse with withdrawal), no such codes exist for hallucinogens and inhalants. 4
This short report builds on previous studies that have described the experience of inhalant withdrawal,5-9 by focusing on the only 2 drug classes without a diagnostically defined withdrawal syndrome: hallucinogens and inhalants per the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. 3 Regarding hallucinogen withdrawal, Halpern & Corey stated, “Hallucinogen withdrawal is occasionally mentioned by those attempting to sell “detoxification” strategies or other interventions to an unwitting public, but because hallucinogens in general do not induce physiological dependence, there is no classic withdrawal syndrome.” 10 Detoxification is described as primarily managing withdrawal to reduce the effects of substances on an individual.11,12 Considering the absence of a diagnostically recognized withdrawal syndrome for hallucinogens or inhalants, and the role of clinical detoxification settings in managing withdrawal symptoms, this descriptive study explored detoxification admissions, with hallucinogens or inhalants as their primary substance (initial substance prompting admission) from 2006 to 2022. Prevalence, demographic characteristics, and polysubstance use were examined among these treatment episodes.
Materials and Methods
Data
This retrospective cross-sectional study using annual data, examined the Treatment Episode Dataset Admissions 2006 to 2022 file, which describes treatment episode admissions (not individual people) from SUD treatment facilities that receive public funds in the U.S. 12 The dataset contains 31 152 649 cases. After selecting only detoxification service/settings as indicated in the dataset which included [a] Detox, 24-hour, hospital inpatient (ie, hospital detoxification for severe medical-associated withdrawal), [b] Detox, 24-hour, free-standing residential (ie, non-hospital residential detoxification for withdrawal), and [c] Ambulatory, detoxification (ie, outpatient detoxification for withdrawal), 12 the sample size was reduced to 6 435 314. After selecting hallucinogens, inhalants, and phencyclidine (PCP) as the primary substance (see supplemental Table 1 for substances identified as hallucinogens and inhalants in the dataset) and removing cases from U.S. territories (<5 cases), the final sample size for the current study was N = 8919. This includes n = 6761 treatment episodes with hallucinogens and n = 2158 treatment episodes with inhalants as the primary substance.
Measures
Included variables are age, hallucinogens or inhalants only, mental health disorder, prior treatment episode, race and ethnicity, region, sex, treatment type, secondary substance, and tertiary substance. Age is a categorical variable including the following age groups 12 to 17 years, 18 to 20 years, 21 to 24 years, 25 to 29 years, 30 to 34 years, 35 to 39 years, 40 to 44 years, 45 to 49 years, 50 to 54 years, and 55 years and older. Hallucinogens or inhalants only describe cases that include the 2 drug classes as their primary, secondary, and tertiary substances. Cases were identified as hallucinogens and inhalants only if their secondary and tertiary substances were categorized as hallucinogens, inhalants, or none. Essentially, these are cases in which only hallucinogens or inhalants were documented, to the exclusion of all other drug classes. Mental health disorder described if the case had a co-occurring mental health disorder. Prior treatment episode described if the case had any prior substance use treatment. Race and ethnicity contain the following categories: American Indian or Alaska Native, Black or African American, Hispanic or Latino Any Race, White, and Another Race or Ethnicity. Region includes Midwest, Northeast, South, and West. Sex includes Female and Male as values. Treatment type includes Detox, 24-hour, hospital inpatient, Detox, 24-hour, free-standing residential, and Ambulatory, detoxification. Secondary and tertiary substances included substances such as alcohol, and cocaine/crack.
Analysis
The University of North Carolina at Chapel Hill Institutional Review Board considered study procedures not human subjects research because de-identified publicly available data were used. The package ggplot2 13 in R Version 4.3.3 14 and SPSS Version 29 15 were used. Focusing on descriptive statistics,16,17 this study examined the counts and percentages of study variables.
Results
Considering the total of 6 435 314 detoxification cases in the dataset before the sample selection criteria, hallucinogens as the primary substance accounted for 0.1% of cases annually (2006-2022). Similarly, inhalants, as the primary substance, accounted for 0.0% of cases annually (2006-2022), except in 2010 and 2016, when they accounted for 0.1%. Descriptive statistics of both study samples may be found in Table 1.
Sample Characteristics.

Hallucinogens or Inhalants only: Hallucinogens, inhalants, or none were selected as the secondary and tertiary substances.
Hallucinogens as Primary Substance
Among the sample with hallucinogens as their primary substance (n = 6761), the most reported secondary substances included cannabis (n = 1462; 21.6%), alcohol (n = 1184; 17.5%), and cocaine/crack (n = 732; 10.8%). The most reported tertiary substances in this sample include alcohol (n = 639; 9.5%), cannabis (n = 524; 7.8%), and cocaine/crack (n = 318; 4.7%). Considering the presence of a secondary substance, polysubstance use was reported among 66% of this sample (n = 4467). Regarding the primary substance, 55.5% (n = 3755) of the sample had PCP listed, whereas 44.5% (n = 3006) of the sample had hallucinogens listed. Non-Hispanic Black or African Americans were the most prevalent racial/ethnic group at 41.9%, PCP primarily drove this as PCP was the primary substance among n = 2346 treatment episodes involving non-Hispanic Black or African Americans. Figure 1 shows the annual counts of cases with hallucinogens as their primary substance.
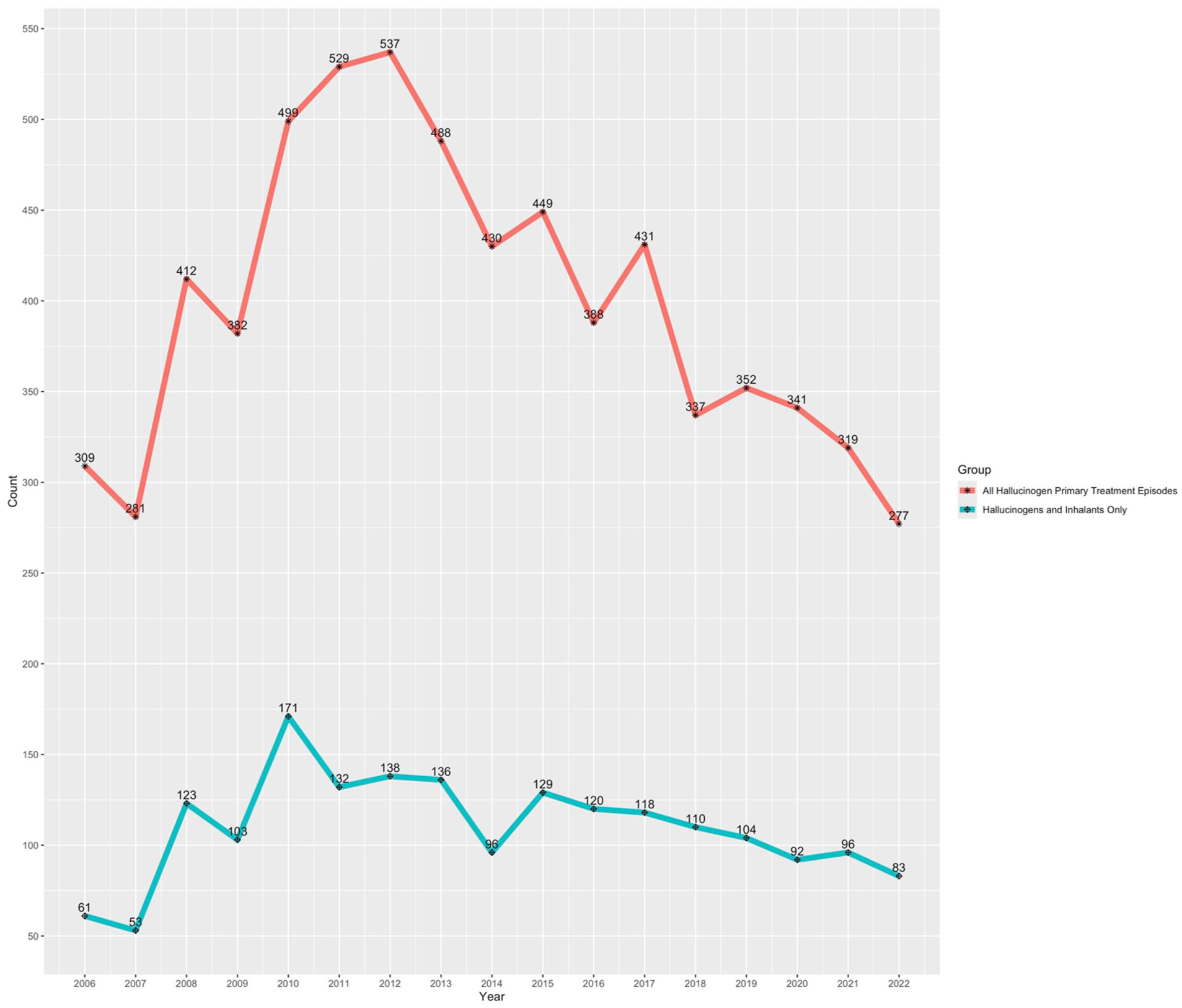
Annual counts of treatment episodes in detoxification with hallucinogens as the primary substance: 2006 to 2022.
Inhalants as Primary Substance
Among the sample with inhalants as their primary substance (n = 2158), the most prevalent secondary substances included alcohol (n = 360; 16.7%), cannabis (n = 259; 12.0%), and cocaine/crack (n = 117; 5.4%). The most prevalent tertiary substances included cannabis (n = 124; 5.7%), alcohol (n = 104; 4.8%), and cocaine/crack (n = 45; 2.1%). Polysubstance use was reported in 48% of this sample (n = 1045). Figure 2 shows the annual counts of cases with inhalants as their primary substance.

Annual counts of treatment episodes in detoxification with inhalants as the primary substance: 2006 to 2022.
Discussion
Building on prior research describing the experience of inhalant withdrawal,5-9 this study examined detoxification admissions among the only 2 drug classes without a diagnostically defined withdrawal syndrome: hallucinogens and inhalants, based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision criteria. 3 The number of individuals with hallucinogens or inhalants as their primary substance in detoxification accounted for approximately 0.1% (n = 8919), of all detoxification admission treatment episodes in the dataset. An even smaller number of individuals only had hallucinogens or inhalants as the substance(s) (n = 2872) during admission. In the sample with hallucinogens as their primary substance, non-Hispanic Black or African Americans were the most prevalent racial/ethnic group, which was primarily driven by PCP. A study from 1998 identified the duration and peak period of withdrawal related to PCP or psychedelics as days to weeks.18,19
The breadth of diverse hallucinogenic chemical derivatives and inhalant-viable substances enables greater difficulty in capturing the full range of withdrawal symptoms. These classes of substances also fall into contrasting regulatory spectrums. On one end, some hallucinogens are federally classed as Schedule I drugs under the Controlled Substances Act, while others are not. Inhalants can be modified from everyday items found in households. It is also worth noting that some commercially available items can also create a hallucinogenic response, such as the presence of lysergic acid amide. 20 Study limitations must be considered alongside these findings, such as the dataset only capturing treatment in facilities that receive public funds. Another limitation is that treatment episodes are the unit of analysis. Other future studies may examine these substances being co-used with other primary substances among individuals entering detoxification services. Overall, these preliminary findings highlight detoxification admissions among individuals with primary substances that do not meet diagnostic criteria for withdrawal. More research is needed to understand the contextual factors that influence detoxification admissions among persons primarily using hallucinogens and inhalants.
Supplemental Material
sj-docx-1-sat-10.1177_29768357251393025 – Supplemental material for A Descriptive Study of Hallucinogen and Inhalant Detoxification Admissions From 2006 to 2022
Supplemental material, sj-docx-1-sat-10.1177_29768357251393025 for A Descriptive Study of Hallucinogen and Inhalant Detoxification Admissions From 2006 to 2022 by G. Rose Geiger and Orrin D. Ware in Substance Use: Research and Treatment
Footnotes
Ethical Considerations
The University of North Carolina at Chapel Hill Institutional Review Board considered study procedures not human subjects research because de-identified publicly available data were used.
Consent to Participate
Informed consent is not applicable as publicly available de-identified data were used.
Author Contributions
GRG: Conceptualization, Writing – original draft, Writing – review & editing. ODW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: O.D.W. received a scholarship from the Joe & Sandy Samberg Foundation to receive Immersive Psychedelic Education from the Usona Institute. O.D.W. is a Faculty Fellow in the University Psychedelic Education Program (U-PEP) which was made possible by the Steven & Alexandra Cohen Foundation and the Joe & Sandy Samberg Foundation in partnership with the 1440 Foundation, Usona Institute, other collaborators, and other funders.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.