
Abstract
Background:
The quality of methadone treatment for opioid use disorder varies across the U.S., affecting patient retention and overdose. Staff stress, trauma exposure, vicarious trauma (VT), burnout, and empowerment are important yet understudied factors that influence workforce well-being and performance.
Objectives:
This study aimed to characterize trauma-related well-being among staff in a national sample of opioid treatment programs (OTPs) and to explore potential correlates of resilience.
Design:
A cross-sectional survey was conducted from June to August 2024 with OTP staff from clinics participating in a parent national study.
Methods:
The survey combined validated instruments and tailored questions to assess work experience, lifetime trauma exposure, trauma and stress-related symptoms, VT, burnout, and multiple dimensions of empowerment. Exploratory factor analysis was used to identify domains of staff well-being.
Results:
The sample (N = 86) included medical staff, counselors, and non-medical/counseling staff from OTPs across 16 states. Thirteen percent of staff met preliminary criteria for posttraumatic stress disorder, 89.2% reported VT exposure at work, and 63.8% reported moderate to severe VT symptoms. Medical staff reported the highest VT and stress scores. Overall, 19.8% of staff met criteria for burnout, with counselors reporting the highest rates (30%). VT symptoms were positively correlated with burnout among counselors, medical, and other staff (r = 0.413-0.650, P < .05). Empowerment subscales were strongly correlated. Two distinct, uncorrelated domains of staff well-being emerged: VT resilience (low VT symptoms and burnout) and empowerment (high perceived control and influence), reflecting distinct aspects of trauma-related functioning. Despite high exposure to lifetime trauma and VT, staff demonstrated moderate resilience and moderate-to-high levels of empowerment.
Conclusion:
Staff of OTPs experience high levels of trauma exposure and symptomatology, VT, and burnout, with notable differences by clinic role. Resilience and empowerment domains suggest opportunities to improve staff wellness.
Keywords
Introduction
Methadone and buprenorphine are safe and effective medications for opioid use disorder (MOUD).1,2 Currently in the United States (U.S.), methadone is dispensed exclusively through federally certified and accredited 3 opioid treatment programs (OTP). 4 These facilities operate under strict federal regulations that require frequent in-person, monitored dosing and limit patient access to take-home (multi-day) doses. 5 As of April 2025, there were over 2100 OTPs in the U.S., 6 serving approximately 524 160 patients, with a median patient census of 260 and over 100 daily clinic visits for supervised methadone administration.6,7 A recent national survey found that over half of OTP patients were required to attend daily medication dosing despite federal policy allowing up to 28 days of take home doses. 8 Clinic practice eschewing current treatment recommendations may explain why methadone patient treatment retention in U.S. is as low as 30%.9,10
Clinic-level practices, like daily clinic dosing requirements, 11 have been explored as factors contributing to poor patient retention. However, a wider and more nuanced assessment is needed to support treatment quality and innovation in the methadone space. For example, less is known about how staff-level factors contribute to clinic practices and patient outcomes. Staff-level factors such as occupational stress, vicarious trauma (VT), burnout, and perceived control or empowerment may influence OTP practices by shaping provider–patient interactions and broader workplace dynamics.12-14 This study provides national-level evidence on trauma-related stress, burnout, and resilience among OTP staff, highlighting distinct domains that can guide strategies to strengthen workforce well-being.
Background
Occupational stress has been shown to reduce healthcare staff job satisfaction, motivation, and overall productivity, which in turn significantly impairs work performance.15,16 Stress is a primary driver of burnout and turnover intentions, particularly among addiction specialists, 17 a provider population including physicians, nurses, and counselors who work closely with patients facing complex biopsychosocial challenges. 18 The constant exposure to patients’ struggles places significant emotional demands on providers; requiring substantial personal and professional resources to maintain work engagement.14,17
Vicarious trauma (VT) is a form of serious occupational stress characterized by affective (eg, emotional responses) and cognitive (eg, altered views of themselves, others, or the world) changes in response to repeated engagement with the traumatic experiences of others.19,20 VT has deleterious impacts on personal well-being and professional functioning, 21 including diminished provider motivation, professional efficacy, psychological health, and emotion regulation.22,23 VT can also disrupt core aspects of a provider’s sense of self, trust, and safety.23-25 Providers in clinical and therapeutic settings are especially at risk of VT as they deeply empathize with the physical or emotional suffering of patients and colleagues. 24 It is well established that patients seeking methadone treatment report high trauma exposure and posttraumatic stress disorder (PTSD), 18 which further increase the risk of exposure to secondary trauma and VT reactions among addiction medicine providers and counselors. Moreover, providers who closely identify with patient experiences, such as having a shared history of substance use disorder (SUD) or trauma, 26 may be particularly vulnerable to VT.25,27,28 In addiction medicine specifically, the relationship between provider personal trauma history and VT remains elusive, with some studies finding that lifetime trauma exposure may support resilience to VT.28-30 Conversely, posttraumatic stress symptoms (PTSS) that are associated with lifetime trauma exposure place providers at risk of increased VT reactions. 12
Staff burnout is also an important factor that can mean the difference between standard-of-care and diminished treatment. Burnout is a progressive psychological response to chronic occupational stress 31 that is linked with provider VT.32,33 Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment. 34 These symptoms are common among healthcare and addiction treatment providers.35-37 Burnout is associated with negative health outcomes for both providers and their patients, 36 specifically among OTP counselors.28,37 Structural and systemic factors, such as limited resources, restrictive clinic policies, and the broader social determinants of health in SUD, contribute to staff VT and burnout and are not easily addressed in OTP settings. 34
Despite substantial wellness challenges facing the SUD workforce, there is reason for optimism. Many addiction medicine providers report high levels of compassion satisfaction and fulfillment from their work, suggesting pathways to resilience even in settings with high VT exposure.28,38 Resilience is a multidimensional construct connoting normative or positive functioning in contexts of significant adversity.39,40 In settings with high VT exposure, resilience can be conceptualized as resistance to negative stress effects, including the capacity to maintain psychological well-being and work engagement while being exposed to secondary trauma.41,42 Studies suggest that sense of control and empowerment are important constructs linked with provider resilience in stressful work contexts.43,44 Workplace empowerment has been found to increase positive occupational mental health and job performance.45,46 Perceived control, reflecting the degree to which individual employees feel they can influence their work environment and interactions with superiors, 47 also has a meaningful impact on work outcomes. 48 For example, beliefs about the level of control and agency in the workplace are related to active engagement and lower burnout.49,50
Existing Evidence on OTP Staff
Few studies have examined the prevalence and impact of stress and trauma in OTP staff. A 2023 study conducted by this team with staff from 3 Arizona OTPs 28 found that 63% of staff reported PTSS at levels indicating trauma treatment need. In this sample, VT levels were in the moderate to high range for over 70% of staff. Notably, while staff trauma history was significantly associated with PTSS, lifetime trauma exposure did not predict VT reactions. Instead, lifetime trauma exposure was associated with higher compassion satisfaction (ie, sense of fulfillment derived from helping others) and increased perceptions of psychological and physical safety at work (ie, resilience to VT).
A second study by this team 11 identified relationships between VT, PTSS, OTP staff beliefs, and personal and professional characteristics including clinic role. Greater VT exposure among OTP staff was associated with higher PTSS, lower perceived ability to provide care, and varied by clinic role and personal characteristics, with counseling staff, younger individuals, and those with less experience reporting greater vulnerability. Clinic-level factors, such as high staff turnover, poor staff-to-patient ratios, and role cycling within a patient-to-provider pipeline appeared to influence both staff well-being and perception of overall clinic culture of patient centeredness. These findings highlight how both individual and organizational factors interact to shape professional well-being, attitudes toward trauma-informed care, and the delivery of person-centered services in OTP settings. They set the stage for national studies involving diverse clinics and larger staff samples.
Study Purpose
The purpose of the current study was to characterize staff trauma-related symptoms and well-being within a national sample of OTPs and to explore potential indicators of resilience. To do so, we conducted a national survey to: (1) describe the prevalence and patterns of lifetime trauma exposure, PTSS, VT, burnout, and empowerment among OTP medical providers, counselors, and other staff; (2) identify key drivers of staff trauma-related well-being; and (3) test whether these factors cluster into distinct domains related to resilience. This work has the potential to inform the development of future workforce interventions to improve OTP staff wellness.
Based on prior evidence with this population, we anticipated that OTP staff would report high levels of trauma, PTSS, and VT, and that these variables may differ by staff role or geographic region. Regional differences were anticipated for 2 reasons. First, it is well known that there are geographic disparities with methadone treatment access.51-53 Second, in our data we observed regional differences in treatment accommodations, staff burnout estimates and patient-centered treatment accommodations. 8 Among all staff, we expected that PTSS, VT, burnout, and perceived control and empowerment would be significant indicators staff trauma-related well-being.
Methods
Data were collected from a cross-sectional national survey of OTP staff working in clinics that were part of a study of OTP clinic administrators conducted between June and August 2024 and described elsewhere.8,54 We recruited staff from among responding OTP clinics to complete an online survey measuring staff experiences of empowerment (ie, perceived control, empowerment to shape treatment, and empowerment to advocate for clinic change), stress, VT, and burnout. Clinic administrators who completed the parent study were asked to post a survey recruitment flyer in staff-only areas of their clinic. The flyer contained a QR (Quick Response) code and a URL leading to a landing page with study information and an opportunity to provide consent for study participation. Consent was given online and recorded as part of the anonymous data set. The selection options following review of study information online were: “yes, I agree to participate in the study” and “no, I would not like to participate.” Those selecting “yes” were led to the survey. Those selecting “no” were led to a message of thanks and were asked to close their browser. Staff completing the survey were offered a $40 electronic gift card. The study was approved by the University of Arizona Human Subjects Protection Program (ID: STUDY00003631).
Eligibility Criteria
To participate in the study, staff had to be at least 18 years of age, working at one of the responding OTP clinics included in the national survey of OTP administrators, and in one of the following roles at OTPs: medical (physician, physician assistant, nurse), counseling (counselor or clinical supervisor), or other staff in a non-medical/non-counseling role including peer staff, front desk, administration, case management, patient navigators, or outreach. Exclusion criteria included not being a full time staff member at a responding clinic, and having a staff role that was not medical, counseling, or among the other roles noted above.
Measures
To assess trauma-related well-being among OTP staff, this study used a combination of validated instruments and tailored questions to capture participants’ work experience, lifetime trauma exposure, trauma and stress-related symptoms, VT, burnout, and multiple dimensions of empowerment. Work experience was assessed by asking participants to report their years of experience working in SUD treatment, methadone treatment, and at their current clinic. Participants also identified their current role as well as any previous roles they had held at that specific clinic. Additionally, participant demographic characteristics were captured, including age, race, ethnicity, gender identity, and U.S. geographic region.
Lifetime trauma exposure was assessed using the 17-item Life Events Checklist (LEC-5) for DSM-5. 55 The LEC-5 demonstrates strong validity and reliability across diverse samples. 56 PTSS were measured using a companion measure to the LEC-5, the 8-item PTSD Checklist for DSM-5 Short Form (PCL-5 SF). 57 The PCL-5 SF (PTSS scores) provides a provisional diagnosis of PTSD and demonstrates strong psychometric properties in previous studies (α = .95)28,58 and the current sample (α = .90).
Vicarious trauma was measured by the 8-item Vicarious Trauma Scale (VTS) assessing exposure to VT and subjective distress associated with working with clients with trauma histories. Items were rated on a seven-point Likert scale (1 = Strongly Disagree to 7 = Strongly Agree). The first 2 items assessed VT exposure at work, while the remaining items measured the severity of symptoms on 2 subscales: affective impacts and cognitive impacts. 59 The VTS demonstrates reliable and valid psychometric properties in prior studies (α = .78)59,60 and in the current sample (α = .80).
Burnout was assessed with a validated single-item self-defined burnout measure 61 in response to the following prompt: “Job burnout is a type of stress linked to work. It includes feeling worn out physically or emotionally and may also involve feeling ineffective or powerless. Overall, based on your definition of burnout, how would you rate your level of burnout?” Participants selected 1 of 5 response options for burnout, and a score of 3 or above was used as the cutoff for classifying burnout. The first 2 indicate the absence of burnout: “(1) I enjoy my work. I have no symptoms of burnout”; and “(2) Occasionally I am under stress, and I don’t always have as much energy as I once did, but I don’t feel burned out.” The remaining 3 reflect varying levels of burnout: “(3) I am definitely burning out and have 1 or more symptoms of burnout, such as physical and emotional exhaustion”; “(4) The symptoms of burnout that I’m experiencing won’t go away. I think about frustrations at work a lot”; and “(5) I feel completely burned out and often wonder if I can go on. I am at the point where I may need some changes or may need to seek some sort of help.” This measure has demonstrated convergent validity with other stand-alone burnout items 62 and longer validated measures of burnout 63 in prior studies.
Perceived control over professional activities was assessed using a 3-item subscale from the Menon Empowerment Scale, 64 which has demonstrated strong psychometric properties in prior studies (α = .87) 65 and the current sample (α = .79). Items included: “I can influence the way work is done in my clinic,” “I can influence decisions in my clinic,” “I have the authority to make decisions at work.” In addition, 2 customized items were included to capture staff empowerment to shape treatment (“I feel empowered to make changes in the way I work with patients”) and empowerment to advocate for clinic changes (“I feel empowered to advocate for specific changes at my clinic”). All items were rated on a five-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree), with higher scores indicating higher levels of perceived control and empowerment. While perceived control is a key domain within the broader construct of empowerment, the inclusion of additional items allowed us to examine empowerment more broadly, capturing both individual influence over professional decisions and perceived ability to shape treatment and clinic-level change.
Data Analysis
Trauma exposure, trauma symptoms, and indicators of trauma-related well-being were descriptively characterized. Continuous variables were examined prior to model testing to assess distributional properties. 66 When normality assumptions were not met, Spearman’s rho correlations were used instead of Pearson’s correlations to assess the strength and direction of associations among non-normally distributed variables. For group comparisons, ANOVA was used when assumptions were met; when they were not, chi-square tests were conducted to examine differences in categorical groupings across OTP staff roles (ie, medical providers, counselors, and other staff) and geographic regions (Northeast, Midwest, South, and West). Descriptive statistics and correlational analyses were stratified by staff role (medical, counselor, other).
Exploratory factor analysis (EFA) using the full sample, with cross-validation, was used to determine whether correlations among observed variables could be explained by 1 or more latent factors characterizing staff well-being. Models were fit using the lavaan package in R (R version 4.2.3 67 ). Seven theoretically specified indicators of trauma-related well-being were included in EFA models: PTSS, VT cognitive impacts, VT affective impacts, burnout, perceived control, empowerment to shape treatment, and empowerment to advocate for clinic change. EFA models specifying 1 to 3 factors were estimated using maximum likelihood extraction to identify the most parsimonious and interpretable factor solution. Based on existing literature, we anticipated a single factor solution or correlated multiple factors; therefore, Geomin oblique rotation was used to allow correlated factors and model the covariance among latent constructs. 68 Model selection was guided by multiple criteria including fit indices, the Kaiser Criterion (ie, eigenvalues > 1.0), factor loadings, and assessment of cross loadings.69,70
As study participants were drawn from a sample of OTP clinics responding to a national survey, tests of non-independence were run to assess the effects of clustering at the clinic-level. Specifically, intraclass correlation (ICCs) estimated the proportion of variance explained by clustering in VT symptoms (ICC = .040), burnout (ICC = .075), and empowerment measures (ICC = .099), and indicated minimal to moderate effects, with all values falling below the standard cutoff of .10. Corresponding design effects (DEFFs = 1.079-1.194) estimated how much data clustering inflated the variance of estimates compared with a random sample of the same size with no clustered data and suggested only modest inflation of standard errors (8%-19%). In sensitivity analyses, a confirmatory factor analysis (CFA) with cluster-robust standard errors was fit to provide model estimates that account for the effect of any clustering. Patterns and significance levels of factor loadings from the retained EFA model replicated in the CFA with cluster-robust standard errors.
Finally, to test the stability and generalizability of the EFA latent structure, we implemented a Monte Carlo twofold cross-validation procedure with 100 resamples.71,72 The repeated twofold cross-validation approach is a robust method for evaluating the replicability of an EFA factor structure under realistic sampling variability, particularly in small samples where traditional single-split validation may be unstable. 73 The dataset was randomly split into 2 equal halves (training and test sets), and this split-resample procedure was repeated 100 times. For each iteration, a CFA model based on the retained EFA factor structure was estimated in the training dataset and evaluated on the held-out testing dataset. Standard model fit indices were evaluated in training and testing subsets using conventional thresholds for acceptable fit [ie, Comparative Fit Index (CFI) ⩾ 0.95, Root Mean Square Error of Approximation (RMSEA) ⩽ 0.06, and Standardized Root Mean Square Residual (SRMR) ⩽ 0.08].70,74 Density plots and boxplots were visualized for each fit index to assess model performance across repetitions with graphs comparing fit in training and testing subsets. Threshold lines for acceptable fit were overlaid to facilitate interpretation. The survey instrument, data and data dictionary will be shared via the National Addiction & HIV Data Archive Program (NAHDAP) through Inter-University Consortium for Political and Social Research (NAHDAP-228330) per the HEAL data ecosystem data sharing requirements.
Results
Sample Characteristics and Bivariate Correlations
Among 86 OTP staff members completing the survey, 83 completed all survey items and were included in analyses (Table 1). These staff were from 25 of 44 clinics completing the national clinic survey. The sample was distributed across 3 staff groups (24 medical, 30 counselors, and 29 other staff (ie, non-medical, non-counseling) and 4 U.S. regions (Northeast, Midwest, South, and West) comprised of 16 states. The average age was 44.3 years (range 19-69), average years working in SUD treatment was 7 (range 0-20), and the majority of participants (84%) identified as female. The most common role among medical staff was dosing nurse (50%). Medical staff reported the most experience in methadone treatment settings, averaging 5.13 years. Counselors, the largest staff group (36%), had the most experience in broader, nonspecific SUD treatment settings, averaging 8.17 years.
OTP Staff Demographics Among National Sample Examining Wellness, 2024 (N=83).

The prevalence of staff lifetime trauma exposure and posttraumatic stress symptoms (PTSS) across staff roles is shown in Table 2. Participants reported a mean of 3.9 (SD 2.9; range 1-12) traumatic event types, 88% of respondents endorsed personally experiencing at least 1 significant traumatic event, and 54% reported personally experiencing ⩾ 4 traumatic event types. Lifetime trauma exposure was similar across clinic roles, F(2, 80) = 1.28, P = .28. Approximately 13.3% of staff scored in the clinical range for PTSS, indicating a provisional PTSD diagnosis. PTSS varied across roles, with medical providers reporting greater PTSS than counselors and other staff, F(2, 80) = 7.25, P = .001. Specifically, medical staff had the highest mean PTSS scores at 9.79 (SD = 6.95), whereas counselors and other staff reported lower scores at 4.83 (SD = 4.79) and 4.55 (SD = 4.91), respectively. Lifetime trauma exposure was positively correlated with PTSS in all staff groups (r = 0.53-0.63, P < .01).
OTP Staff Well-Being Outcomes in a National Sample, 2024 (N=83).

Values are Spearman’s rho correlation coefficients.
P < .05. **P < .01 (two-tailed).
About half (51.8%) of participants reported that their job involved exposure to distressing materials and experiences, and the vast majority (86.7%) reported their job required exposure to traumatized or distressed clients. Despite high prevalence of VT exposure, not all staff experienced affective and cognitive symptoms of VT. Across roles, 36.1% of staff reported low or no VT symptomatology, 56.6% endorsed moderate symptoms, and 7.2% endorsed high symptoms. Further, while VT exposure was similar across staff roles, χ²(2) = 0.87, P = .653, VT symptom severity varied by role, F(2, 80) = 3.23, P = .045. Medical staff reported the highest levels of VT symptoms with a mean score of 25.71 (SD = 6.89), compared to counselors (21.70, SD = 8.69) and other staff (20.45, SD = 8.12).
Overall, 17 (19.8%) participants scored above the cutoff for burnout. Counselors had the highest prevalence of burnout (30%), compared with medical staff (20.8%) and other staff (10.3%). Though group differences on burnout did not reach statistical significance, χ²(2) = 3.79, P = .15. Burnout scores were positively correlated with VT symptoms in all staff groups (r = 0.41-0.65, P < .05).
Regarding empowerment subscale items, participants reported moderate levels of perceived control (M = 10.40, SD = 1.96) and moderate to high empowerment to shape treatment and advocate for clinic change (mean of 4.00 and 3.87 on a 5-point scale, respectively). There were no statistically significant differences across staff groups on any of the empowerment subscales. Counselors showed moderate to strong correlations between perceived control and both shaping treatment (r = .434, P < .05) and advocacy (r = .506, P < .01). For medical staff, these links were even stronger (r > .86, P < .01). Other staff showed similar positive relationships. Burnout and trauma had minimal or negative associations with empowerment subscales (Table 2).
A statistically significant association was found between U.S. region and burnout status, χ²(3, N = 24) =9.21, P = .027, with Midwest staff reporting more burnout than expected (residual = 2.4). Analyses showed no significant regiosupplenal differences in lifetime trauma exposure, PTSS, VT, or empowerment subscales.
Exploratory Factor Analysis Findings
Table 3 displays outcomes from the exploratory factor analysis (EFA) clarifying the array of factors among the 7 indicators (PTSS, VT emotional/affective impact, VT cognitive impact, burnout, perceived control, empowerment to shape treatment, and empowerment to advocate for clinic change). A 2-factor solution provided the best fit to the data, χ²(8) = 4.30, P = .83, CFI = 1.00, RMSEA = 0.001 compared to the 1-factor model, (χ²(14) = 72.71, P < .001, CFI = 0.66, RMSEA = 0.23), and the 3-factor solution did not demonstrate improved fit over the 2-factor solution, χ²(3) = 2.237, P = .525, CFI = 1.000, RMSEA = 0.001. The 2-factor solution was supported by eigenvalue correlation (λ1 = 2.394, λ2 = 2.099, λ3 = .889, λ4 ⩽ .600).
Exploratory Factor Analysis Loadings, Communalities, and Variance Explained in the Retained 2-Factor Model in National Sample of OTP Staff (N=83), 2024.

Abbreviations: PTSS, posttraumatic stress symptoms; VT, vicarious trauma.
All factor loadings are significant at **P < .01 (two-tailed). No cross loadings. Communalities represent the proportion of each variable’s variance that is explained by the factors retained in the model.
The following latent constructs were identified in the 2-factor model: (1) VT Resilience, characterized by significant factor loadings for low cognitive (λ = 0.68, P < .01) and affective impacts of VT (λ = 0.84, P < .01), and low burnout (λ = 0.63, P < .01); and (2) Empowerment, indicated by significant factor loadings for perceived control (λ = 0.77, P < .01), empowerment to shape treatment (λ = 0.77, P < .01), and empowerment to advocate for clinic change (λ = 0.93, P < .01). The model had no significant cross-loadings. The indicator of PTSS did not load significantly on either factor in this solution, suggesting it may represent a distinct dimension requiring separate analysis. The 2 factors of VT resilience and empowerment were uncorrelated (r = .05), indicating relative independence between the latent constructs. Together, these factors explained approximately 53% of the total variance in the observed indicators.
A graphical representation of the retained 2-factor solution is presented in Figure 1 below. Manifest variables for VT cognitive and affective impacts, as well as burnout, are displayed in reverse score to indicate that lower levels of VT symptoms and burnout form the latent construct of VT resilience. Scaled factor scores were extracted from the model to characterize levels of VT resilience and empowerment among OTP staff (Table 4).

Model characterizing OTP staff trauma-related well-being in a national sample, 2024 (N = 83).
Descriptive Statistics for Scaled Latent Factor Scores in the Retained 2-Factor Model in national sample of OTP staff (N = 83), 2024.

Latent factors of VT resilience and empowerment among OTP staff were rescaled to a common 1 to 5 scale to facilitate interpretability.
VT resilience factor scores ranged from 1 to 5 (mean = 3.18, median = 3.09, SD = 0.94), indicating that, on average, staff displayed moderate resilience to the negative effects of VT. Empowerment factor scores also ranged from 1 to 5 (mean = 3.82, median = 3.94, SD = 0.86), reflecting moderate to high levels of empowerment with somewhat lower variability (Figure 2).
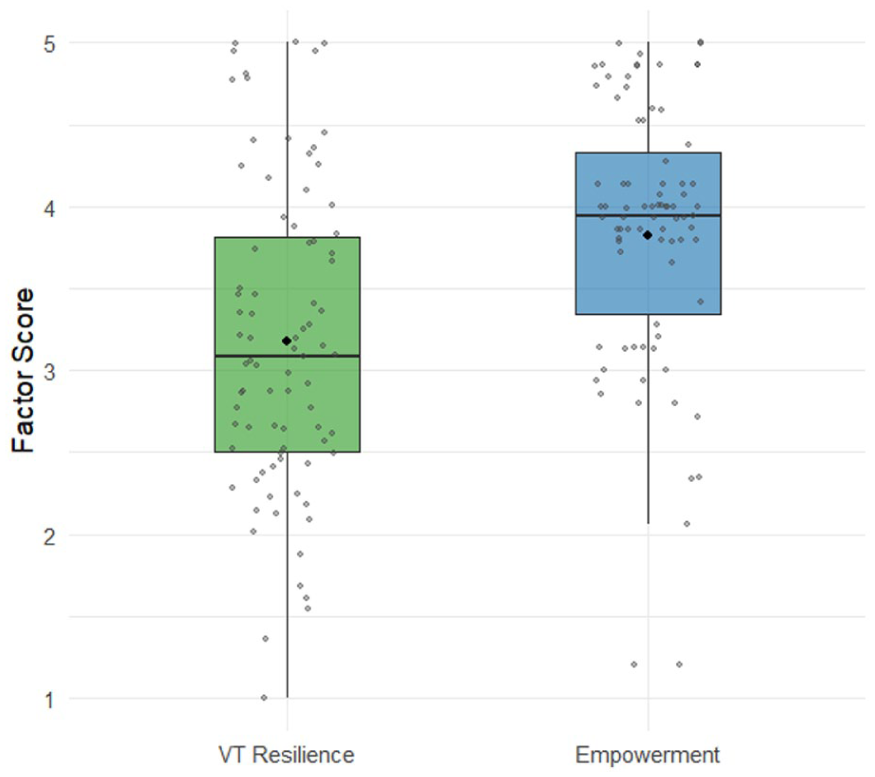
Scaled factor scores for latent constructs of VT resilience and empowerment in a national sample of OTP staff, 2024 (N = 83).
Confirmatory Factor Analysis Findings: Twofold Monte Carlo Cross-Validation
We conducted a repeated twofold Monte Carlo cross-validation with 100 resamples to evaluate the stability and generalizability of the 2-factor measurement model (Supplemental Table 1). In each iteration, the dataset was randomly split into equal training and testing subsets and a confirmatory factor analysis (CFA) model was fit separately to each subset. Results demonstrated a consistent strong fit with nearly identical performance across the training and testing datasets (average CFI = 0.99, RMSEA = 0.06, SRMR = 0.03), indicating good replicability and a close fit between the model and the observed data across repeated resamples. Further, density and boxplot visualizations of cross-validation fit indices revealed tight distributions with few outliers and minimal differences between training and testing sets (Supplemental Figure 1). Most resamples met or exceeded conventional standards for good model fit as shown by overlaid threshold lines (ie, CFI > 0.95, RMSEA < 0.06, SRMR < 0.80). In sum, the 2-factor structure provided the best fit to the data and appeared reliable across multiple random partitions, indicating that the identified latent constructs were stable representations of the underlying data structure. These findings provide preliminary evidence that this model is appropriate to retain based on repeated cross-validation.
Discussion
This exploratory study characterized trauma-related well-being outcomes among OTP staff, highlighting how trauma exposure, PTSS, VT, burnout, and empowerment intersect across different staff roles and regions. Consistent with prior regional studies, our findings demonstrate that OTP staff experience high levels of lifetime trauma and VT exposure and moderate VT symptoms, with notable differences by role. Importantly, we identified 2 distinct, uncorrelated domains—VT resilience and empowerment—that characterize staff well-being, suggesting that trauma-related risk and protective factors may operate independently but simultaneously within OTP settings.
Despite high rates of trauma and VT exposure, OTP staff in this national sample demonstrated moderate resilience to VT and moderate-to-high levels of perceived empowerment. Notably, not all staff experienced significant affective or cognitive VT symptoms, which suggests that individual or organizational factors may help buffer the negative effects of VT. These protective factors could be further strengthened through targeted interventions to support staff well-being and sustain treatment quality across roles. These insights extend the existing literature by showing that staff well-being and resilience are multidimensional and multiply-determined, reinforcing the need for tailored interventions to support the diverse roles within OTPs and ultimately strengthen workforce sustainability.
Four important observations emerged from this study. First, OTP medical staff may be uniquely vulnerable to trauma impacts. Their higher levels of VT and PTSS contrasted with those of counselors and other staff despite having similar lifetime trauma exposure. These findings build on prior research, 28 especially that medical staff VT symptom severity reflected known disproportionate trauma-related stress among healthcare workers.75,76 Reasons for this vulnerability are not known and should be explored. The level and depth of training in self-care and setting emotional boundaries may vary across staff roles and could influence prevalence of burnout. Unlike counselors, who are often trained and encouraged to build therapeutic alliances through empathetic engagement, medical providers may be expected to maintain greater emotional distance. While this boundary-setting may be protective in some clinical settings, it could limit opportunities for compassion satisfaction. Without the same access to emotionally rewarding patient interactions, medical providers may be more vulnerable to cumulative stress, especially when navigating complex care demands, regulatory pressures, and repeated exposure to patients’ trauma histories. Additionally, it is possible that OTP medical staff’s proximity to acute clinical scenarios (eg, overdoses, complex dosing decisions) and heightened sense of responsibility for patient survival may explain this outcome.
Second, burnout is prevalent yet regionally distinct. Staff in the Midwest region reported significantly higher rates than expected, and counselors had the highest group-specific rate of burnout (30%), though role-based differences did not reach statistical significance. These patterns may reflect geographic variability in staffing levels, patient volume, and access to support/referral services, as well as the emotionally taxing nature of counseling work. The emotionally taxing nature of counseling work stems from the ongoing exposure to clients’ trauma, pain, and crises, requiring counselors to remain empathetic, attuned, and composed. This sustained emotional labor, combined with limited opportunities for recovery or support, can lead to emotional exhaustion, burnout, or VT.17,37 Over time, the cumulative demands may impact counselors’ mental health, well-being, and job satisfaction. 77
Rates of burnout among OTP staff in this study are consistent with those reported among nurses, social workers, therapists, and military behavioral health providers.78-80 Counselors working in addiction settings are especially vulnerable, given the emotional toll of supporting clients through relapse, trauma, and high-stakes recovery efforts. 35 In terms of regional differences, it is possible that clinic trauma-informed practices, such as regular assessment of staff trauma symptoms may explain regional differences. In the parent study, OTPs located in the west were more likely to be among the 22.7% of clinics that self-assess staff trauma symptoms. 8
Third, correlational analyses identified role-specific pathways to stress and burnout. For counselors and medical staff, VT was strongly associated with burnout, reinforcing the need for trauma-informed strategies tailored by role. Empowerment domains, including perceived control, influence over treatment decisions, and advocacy, were closely interrelated across all staff types, pointing to universal organizational levers that may enhance engagement and retention. These findings suggest that a one-size-fits-all approach to workforce support may be insufficient; instead, nuanced strategies tailored to the specific needs of individual roles and organizational environments are warranted.
Finally, trauma-related well-being in this sample appeared to operate through 2 uncorrelated latent constructs, VT resilience and empowerment. This suggests that emotional well-being and structural empowerment are distinct domains of OTP staff well-being and, thus, may have different antecedents and consequences that should be explored in future research. Staff in OTP settings may be psychologically resilient to the effects of VT yet feel disempowered to provide the care and treatment they desire for their patients. Similarly, staff who perceive that they are empowered to shape clinic practices and treatment may still experience trauma-related emotional exhaustion or cognitive distortions that negatively impact their treatment provision. Failure to support staff in 1 area alone may not be enough to affect improved patient outcomes. Future research should aim to measure VT resilience and empowerment in provider samples across OTP and other substance use treatment settings to evaluate whether these are core, generalizable dimensions of staff trauma-related well-being. These constructs have the potential to guide future research, workforce assessments, and program evaluations aimed at improving staff experiences and retention in and beyond OTP settings. It will be important for future research to identify the unique correlates of VT resilience and staff empowerment, in order to determine when and how these constructs influence provider functioning and patient treatment outcomes.
This study expands upon state-level findings, including prior research in Arizona, 11 by offering a broader national perspective on staff trauma-related well-being in OTPs. While local studies have identified important clinic-level practices (eg, collaborative decision-making, structured supervision), these dynamics remain underexplored at a national scale. Understanding the interplay between individual-level and organizational factors is essential for developing scalable interventions that promote retention and satisfaction. Although this study did not include direct measures of patient care quality, the observed associations among trauma exposure, burnout, and staff empowerment may have downstream implications for patient experience and methadone treatment quality. Future research should aim to empirically examine how workforce well-being is linked to specific patient outcomes (eg, treatment retention, satisfaction, and therapeutic alliance) to clarify these potential relationships and support evidence-based improvements in both staff and patient outcomes.
Clinical Implications
These findings highlight the distinct and often underrecognized stressors faced by OTPs. Repeated exposure to patients’ struggles, especially in cases of return to use despite best efforts, can erode providers’ emotional resilience and sense of efficacy, threatening both staff well-being and care quality. Notably, the emergence of 2 distinct, replicable constructs, VT resilience, and empowerment, underscores the importance of addressing both emotional and structural dimensions of staff well-being.
To mitigate these risks, OTPs should implement confidential screening and trauma-informed support services to enable early intervention. Access to targeted mental health resources such as peer support programs, trauma-informed counseling, and workplace wellness initiatives can help staff manage chronic stress and reduce burnout. 81 Fostering a workplace culture that values staff well-being, through training, structured clinical supervision, and reasonable workload distribution, is essential. Research indicates that these strategies can enhance provider resilience and job satisfaction, while also improving retention.82,83 Resilience, the capacity to preserve mental well-being and maintain positive functioning when faced with adversity, is closely linked with empowerment and burnout. 84 Strategies to promote resilience such as engaging in meaningful work and fostering positive team dynamics may reduce burnout and improve patient care and job satisfaction. 85
Furthermore, resilience is not solely an individual trait but a skill that can be cultivated through intentional organizational and leadership efforts. 85 Previous research also identified several system-level changes to mitigate burnout, such as fostering more frequent staff-wide interactions, improving communication, providing accessible paid time off, and enhancing clinical supervision. 37 OTP leadership plays a critical role in creating environments that support well-being by promoting open communication, allocating resources, and facilitating the integration of evidence-based practices. By investing in tailored, role-specific interventions that strengthen both individual resilience and organizational empowerment, OTPs can build a more sustainable workforce and may contribute to improvements for both staff and patient outcomes.
Limitations
This study is exploratory in nature due to its cross-sectional design and limited sample size. The sample for this study was drawn from a national survey that employed specific eligibility criteria, which may limit the generalizability of the findings. Additionally, no power analysis was conducted and the EFA was conducted with a relatively small sample size, which may limit the stability and generalizability of the factor structure; therefore, findings should be interpreted with caution and validated in larger samples. This study relied on retrospective self-reports of trauma histories, which may be subject to limitations such as recall bias, inaccurate reporting, or difficulty in accessing traumatic memories.86,87 As with all studies using self-reports of lifetime trauma, our data may include some false positives regarding traumatic events. However, longitudinal evidence indicates that individuals often underreport earlier trauma experiences, suggesting that self-report data may provide conservative estimates of actual exposure. 88
Other confounding variables may influence the relationship between staff trauma, stress, empowerment, burnout, and functioning at OTPs, which were not accounted for in this analysis. For example, there is currently no nationally accepted definition of a “counselor” in OTPs, and therefore functions and staff education (which may prepare them for stressful work) may also vary. Future research should explore potential confounders and moderators, including clinic-level factors such as access to training and supervision, case consultation to improve care, supervised urinalysis, the clinic’s commitment to abstinence, required counseling, and leadership style. A more comprehensive understanding of these influences can inform targeted interventions to support the well-being of OTP staff and optimize patient care. Finally, as this study identified indicators of well-being and explored associations between variables, it does not establish causal relationships regarding staff well-being.
Conclusion
Findings highlight distinct role- and region-specific patterns in OTP staff trauma-related well-being. A stable two-factor model, VT resilience and empowerment, emerged as a reliable framework to understand OTP staff trauma-related well-being. This model suggests that emotional distress and perceived influence over treatment and organizational processes operate independently. Together, these results highlight the importance of developing tailored, role-sensitive interventions that address both trauma exposure and structural empowerment to foster resilience, reduce burnout, and improve workforce sustainability across OTP settings.
Supplemental Material
sj-doc-2-sat-10.1177_29768357251383239 – Supplemental material for Trauma-Related Stress and Resilience in a Multistate Sample of Methadone Treatment Staff
Supplemental material, sj-doc-2-sat-10.1177_29768357251383239 for Trauma-Related Stress and Resilience in a Multistate Sample of Methadone Treatment Staff by Zhanette Coffee, Linnea Linde-Krieger, Gregory A. Carter, Benjamin R. Brady, Alissa Davis, Richard A. Crosby, David Frank, Arlene N. Mahoney, Sara M. Najar and Beth E. Meyerson in Substance Use: Research and Treatment
Supplemental Material
sj-docx-1-sat-10.1177_29768357251383239 – Supplemental material for Trauma-Related Stress and Resilience in a Multistate Sample of Methadone Treatment Staff
Supplemental material, sj-docx-1-sat-10.1177_29768357251383239 for Trauma-Related Stress and Resilience in a Multistate Sample of Methadone Treatment Staff by Zhanette Coffee, Linnea Linde-Krieger, Gregory A. Carter, Benjamin R. Brady, Alissa Davis, Richard A. Crosby, David Frank, Arlene N. Mahoney, Sara M. Najar and Beth E. Meyerson in Substance Use: Research and Treatment
Footnotes
Acknowledgements
We are grateful to the participants who generously shared their time and experiences for this study. We also extend our sincere thanks to the National Institutes of Health (NIH), and specifically the NIH HEAL Initiative® and the National Institute on Drug Abuse (NIDA), for their support of this research.
ORCID iDs
Author Contributions
Zhanette Coffee: Conceptualization; methodology; formal analysis; investigation; data curation; writing—original draft preparation; writing—review and editing; visualization; supervision.Linnea Linde-Krieger: Conceptualization; methodology; funding acquisition; data curation; formal analysis; writing—original draft preparation; writing—review and editing.Gregory A. Carter: Methodology; funding acquisition; investigation; writing—review and editing.Benjamin R. Brady: Methodology; funding acquisition; investigation; writing—review and editing.Alissa Davis: Methodology; writing—review and editing.Richard A. Crosby: Methodology; funding acquisition; investigation; writing—review and editing.David Frank: writing— Methodology; review and editing.Arlene N. Mahoney: writing— Methodology; and editing.Sara M. Najar: writing— Methodology; review and editing.Beth E. Meyerson: Conceptualization; funding acquisition; investigation; methodology; project administration; supervision; writing- original draft; writing-review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Helping to End Addiction Long-term® Initiative, or NIH HEAL Initiative® by the National Institute on Drug Abuse of the National Institutes of Health under Award Number R61DA059889. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.