
Abstract
Objective:
This formative study aimed to explore socio-ecological and structural determinants that influence substance use disorders (SUD) among Black men in rural areas of South Carolina (USA) and inform the design of culturally relevant community-based interventions.
Methods:
Black adult men (N = 15; ages 33-66 years) with known SUD were recruited from outpatient treatment centers, homeless shelters, and via community outreach initiatives within rural areas of South Carolina. Written informed consent was obtained, and interviews were conducted using a structured interview guide. Interview data was audio-recorded, coded and analyzed until consensus was reached on emergent themes. Data were collected between June 2023 and May 2024.
Results:
Five primary themes emerged: perceptions and experiences with substance use, contributing factors to substance use, determinants of treatment acceptance, and relapse triggers. Findings from this work highlight barriers such as financial constraints, peer influence, social dynamics, and systemic inequalities that hinder SUD treatment engagement for Black men in the rural South. Facilitators such as community and familial support, cultural considerations, and self-awareness were identified as critically important for encouraging treatment acceptance.
Conclusion:
This exploratory study provides insight into the socio-cultural and structural complexities faced by Black men in rural South Carolina (USA) regarding SUD treatment and relapse prevention. Our findings support the call for culturally sensitive, community-driven research and interventions that address both personal and systemic challenges. Larger and interdisciplinary studies are needed to address urgent prevention and treatment gaps, and pervasive disparities in SUD treatment outcomes for Black men in medically underserved rural communities.
Keywords
Introduction
Substance use disorders (SUDs) pose pervasive and significant challenges to global public health,1,2 particularly in rural and underserved populations. 3 In the United States (US), Black/African American men are disproportionately affected by substance use disorders (SUD) and face significant social, legal, and interpersonal consequences. 4 They are 3 times more likely than their White counterparts to experience negative outcomes related to substance use and 5 times more likely to report dependency. 5 The challenges faced by Black men with SUD in the US are also exacerbated in rural areas, where limited economic opportunities, labor-intensive jobs, and restricted healthcare access prevail. 6 In the rural South, Black communities experience persistent poverty, unemployment, community crimes and incarcerations, 7 and race-related stressors such as discrimination, economic distress, and historical trauma.8,9 This combination of socioeconomic and racial stress and other structural drivers of poor health often drives substance use as a coping mechanism for these compounded hardships. 10
Among Black Southern rural men in the US, the challenges associated with SUD treatment acceptance and relapse prevention are shaped by a complex interplay of ecological and structural factors. 11 These factors include limited healthcare access, socioeconomic hardships, cultural stigmas, 12 and historical mistrust of the medical system.13,14 As a result, this population faces a unique set of barriers to seeking and sustaining SUD treatment, leading to higher relapse rates 15 and poorer health outcomes. 2 Ecological factors, such as community dynamics, family structures, and social networks, play a critical role in shaping treatment decisions. 11 The social environment, including peer influences and family support, can either facilitate, or hinder treatment acceptance.16,17 Structural factors, including healthcare access, economic instability, 18 and systemic racism19,20 further compound these challenges, making it difficult for individuals to engage in sustained recovery efforts.
Despite these known barriers, there is limited research that focuses on how ecological and structural factors intersect to influence treatment acceptance and relapse prevention among Black men in the rural South. 3 There are notable disparities in the perceived need for SUD treatment across both geographic and gender lines. 21 Urban residents tend to report a greater perceived need for treatment compared to their rural counterparts. Additionally, predisposing factors such as age, and a history of prior drug treatment are more commonly observed in male substance users than in female users. 22 Research has shown that a higher perceived need for treatment is closely associated with increased acceptance of treatment, lower rates of relapse, and more positive treatment outcomes.23,24 A recent study conducted among rural residents admitted into a SUD treatment program indicated that Blacks were 2 times more likely to relapse into using drugs compared to their White counterparts 25 ; however, there is limited understanding in the literature as to the reasons behind this finding.
Guided by Bronfenbrenner’s Social Ecological Model (SEM), 26 this formative study sought to explore the ecological and structural factors that impact treatment acceptance and relapse potential for SUDs among Black men residing in the rural South. By examining personal narratives and community-based experiences, this research aimed to explore the perceived underlying barriers and facilitators that influence treatment decisions at the individual, interpersonal, organizational, and societal levels. The results can help inform the design of culturally relevant and ecologically grounded SUD interventions to improve the observed treatment engagement and reducing relapse rates among this population.
Methods
Setting and Study Design
This study was conducted among Black men residing in rural areas of South Carolina (SC), USA. Located on the southeastern seaboard, SC has a land area of 30 054 mi2 and an estimated population density of 170.3 people per square mile. According to the US 2020 Census Survey, approximately 729 735 (13.5%) of South Carolinians live in rural areas where the poverty rate is 20.4% compared with 13.6% in urban areas; 15.4% of the rural population has not completed high school versus 9.9% of the urban population, and the unemployment rate is 4.0% in rural areas versus 3.1% in urban. South Carolina’s Black population is the 15th largest in the US. In national surveys, Black rural South Carolinians have higher rates of age adjusted mortality from all causes, including cancer, cardiovascular disease, and stroke compared to their urban counterparts. 27 These rates are the highest among all racial and ethnic rural groups. Furthermore, Black rural South Carolinians report more social disadvantage, and more often rate their health status as “fair” or “poor,” and report delays in seeking medical care due to health care costs, as compared to other ethnic rural residents. 28 In 2021, it was reported that although Blacks comprised 25% of the SC population they represented 58% of the prison population, whereas Whites represented 63% of the state population and 39% of the prison population. 29
Sample
Participants (N = 15) were recruited through targeted study advertising using IRB approved materials and “snowball sampling” among SUD outpatient treatment centers, homeless shelters, and community outreach initiatives conducted within rural areas of South Carolina. Individuals interested in study participation were screened by the researchers using an eligibility checklist per the study’s inclusion/exclusion criteria. Interested individuals that screened eligible were consented and/or scheduled for consent and interview by the researchers. Participant eligibility criteria included being a Black/African American male, adult aged 18 and older, English speaking, residing in a rural area of SC State for at least 1 year, and a history of SUD. Individuals that appeared to be actively under the influence of drugs and/or upon asking failed to comprehend the informed consent, as demonstrated by a lack of understanding of the study procedures and/or their expectancies as a research participant, were excluded. For this study, rurality was determined using the county-based Rural-Urban Continuum Codes (RUCC) 30 and/or US Census Bureau maps of census tracts, 31 as applicable.
Although larger sample sizes are more often used in exploratory studies of this nature, a prior review of the literature justified the selection of our sample size in showing that data saturation can be achieved with small, focused samples, particularly in homogeneous groups and narrowly scoped studies.32,33
Procedures
In-person interviews averaging 35 minutes were conducted in a private conference room at the treatment center or homeless shelter where the participant was recruited, or at the participant’s home. All interviews were conducted by the Principal Investigator (PI) using a developed interview guide (see Supplemental Materials). Prior to beginning each interview, the purpose and aims of the study were explained to participants and all questions were answered. Participant demographics were then collected, followed by the interview. Interviews were audio recorded with a portable audio-recorder and later transcribed verbatim to preserve the contextual meaning of the participant’s response. All participants were assigned a code number to preserve their privacy and anonymity, and all personal identifiers were removed from transcriptions. Recordings were uploaded to a secure server for data preservation purposes and deleted from the portable recording device. Participants received a $25 (USD) gift card as study compensation for their time.
Interview Guide
The interview guide was based on the researcher’s prior work and informed by the literature.3,34 -36 It was developed by the research team under the guidance of a senior methodologist (CP) with extensive expertise in leading qualitative research to inform community-based interventions. The guide was designed to explore the perception, experience and contributing factors associated with SUD among Black Southern rural men; to determine the factors associated with treatment acceptance decision making from those perspectives and to examine factors associated with substance use relapse. To assure that the study’s aims were covered, 4 open-ended questions were selected for the interview, with relevant follow-up prompts. The guide was pilot tested for clarity of understanding and relevancy with 3 individuals that met the inclusion/exclusion criteria, who were excluded from the main study. The guide is provided in the Supplemental Materials.
Data Analysis
Interview transcripts were thematically coded and then analyzed using a combined inductive and deductive approach 37 and ATLAS.ti software. The deductive component utilized the Socio-Ecological Model (SEM), 26 while drawing on existing research3,5,34 to test the model. In contrast, the inductive approach explored interview data to identify emergent themes, while allowing for generalizations to be made by the researchers. The integration of this combined approach was employed to develop a codebook that the PI and the senior researcher independently used to code interview transcripts.
A subset of the independently coded transcripts was compared to assess inter-coder reliability. Discrepancies were resolved through consensus, leading to iterative refinements of the codebook to ensure clarity and consistency across the dataset. Data saturation was reached after 10 transcriptions. Saturation was defined as the point at which no new themes or insights emerged, indicating sufficient depth to address the study’s aims.
To promote scientific rigor and increase the generalizability of our findings, we applied several strategies to ensure dependability, confirmability, and transferability. Dependability was addressed by maintaining a detailed written audit trail that documented the research process, including methodological decisions, coding procedures, and analytical steps; enabling others the ability to trace how data were collected and interpreted. Confirmability was addressed by employing reflexive journaling throughout the research process; a critical aspect of our data analysis included the consideration of personal bias and cultural context from the PI’s interview notes, as the PI is a Black African male that had been embedded in an exclusively Black neighborhood for 1 year. Recognizing that this positionality had the potential for interpretive bias and/or assumptions rooted in a sense of shared experience, the PI engaged in regular debriefings with the co-investigators (all white females) to review and examine both interview notes and emerging themes. This reflexive approach aimed to balance the advantages of cultural familiarity with methodological transparency. Transferability was addressed by collecting rich interview data, and providing detailed descriptions of the study setting, design, participant characteristics, and key findings; allowing others the ability to assess the extent to which the results may apply to similar populations or settings. Identified themes were shared with local community leaders and healthcare stakeholders, who provided confirmatory validity to support the findings by affirming that they were consistent with their experiences and perceptions of SUD in their communities.
Ethical Considerations
The study protocol underwent review and approval by the University of South Carolina Institutional Review Board (IORG0000142). The study was conducted by the researchers in compliance with Good Clinical Practices (GCP) of the International Conference of Harmonization (ICH) and accordance with the Declaration of Helsinki as revised in 2013. 38 Written informed consent was obtained from all participants prior to the conduct of research activities.
Results
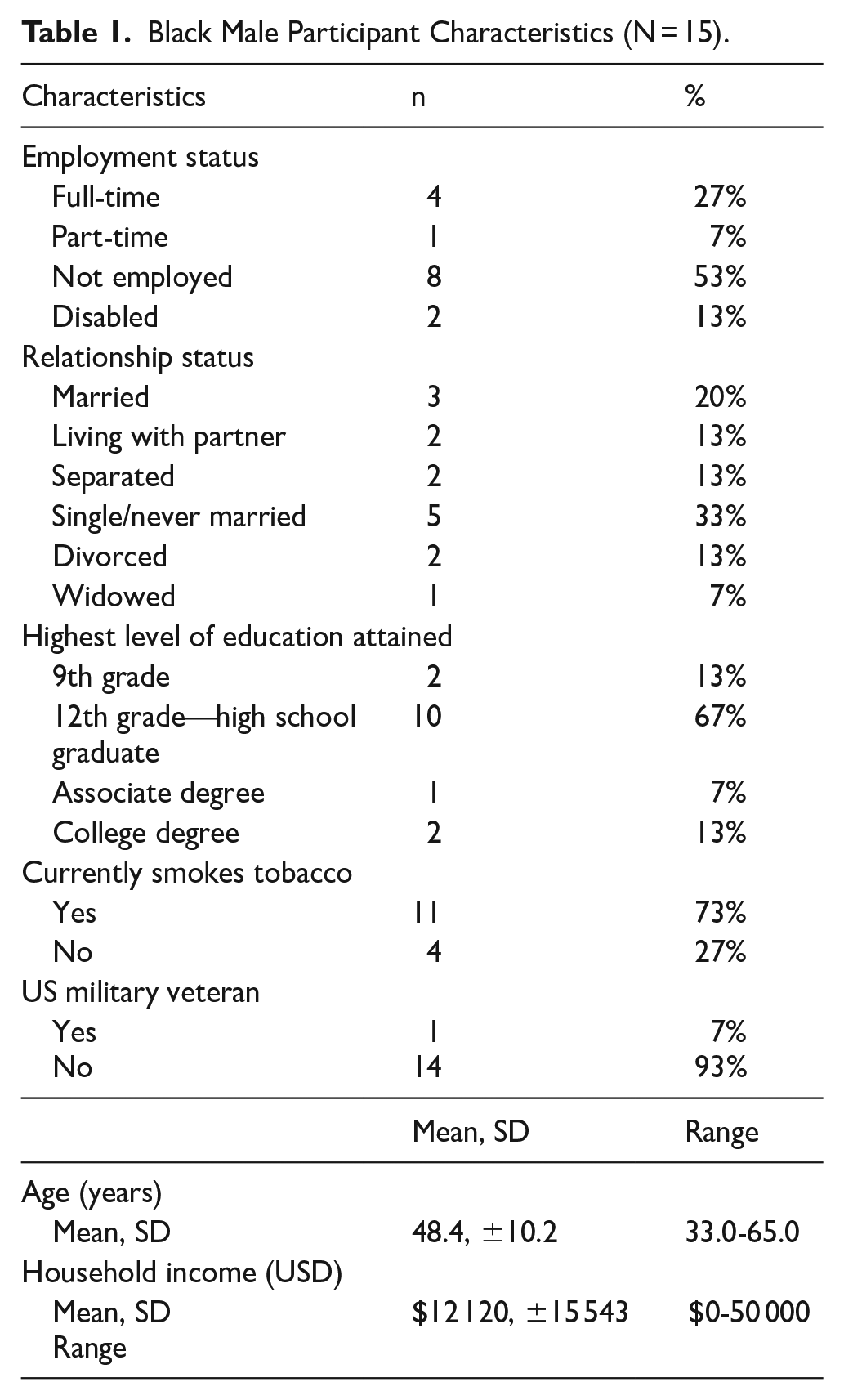
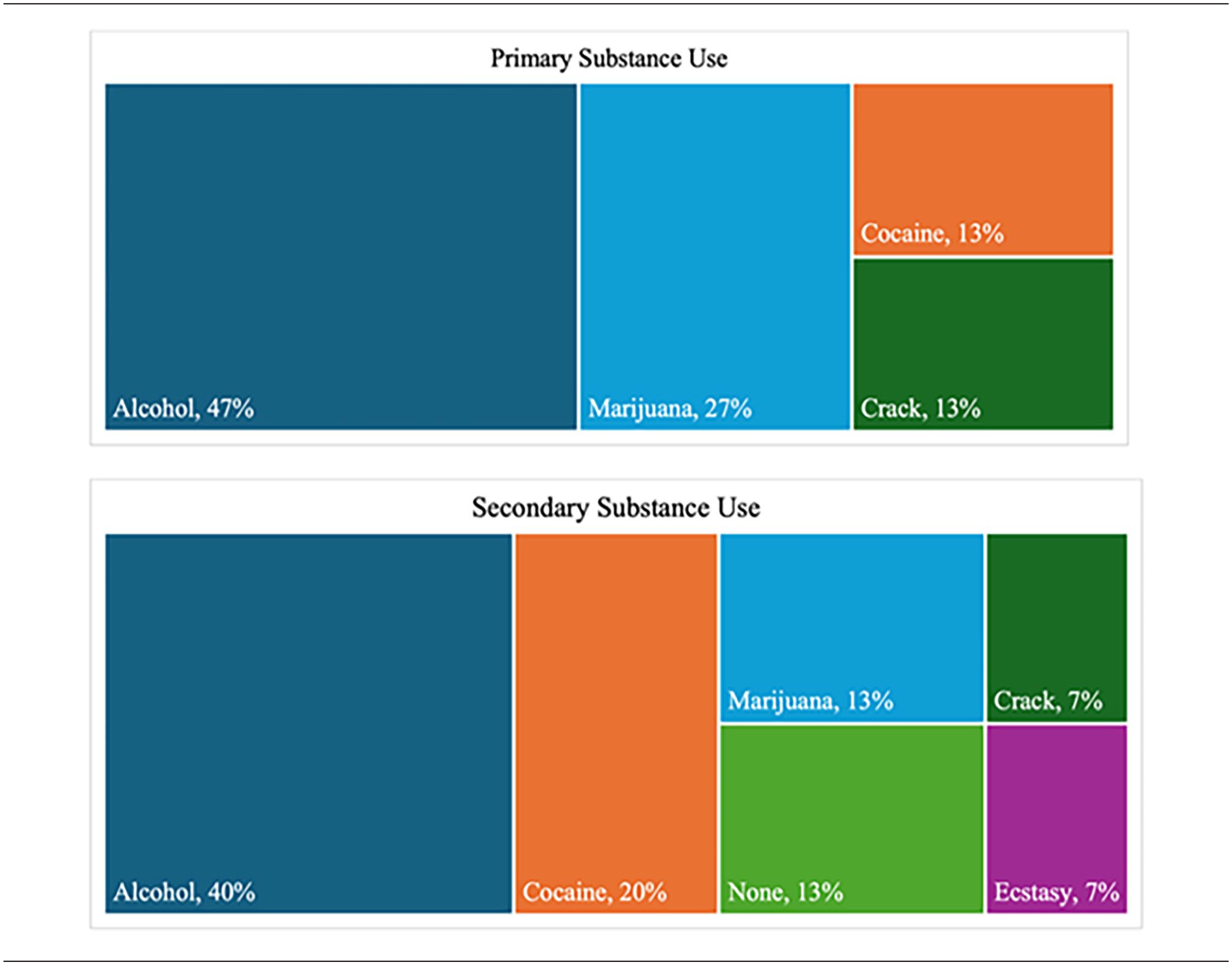
Participants (N = 15) were recruited from several sources, including an outpatient substance abuse treatment center (n = 4), a homeless shelter (n = 4), and through community outreach efforts (n = 7) in rural areas of SC. Participant characteristics are shown in Table 1. Participant ages ranged from 33 to 65 years, with a mean age of 48 years. Annual incomes varied from $0 to $50 000, with a mean income of $12 000. Twenty percent of the participants were married, while 53% were unemployed. The primary substances used were alcohol and cocaine. Seventy-three percent of participants identified as tobacco smokers (Table 1) and all participants reported using at least 2 substances (Table 2).
Black Male Participant Characteristics (N = 15).
Primary and Secondary Substance Use.

The study identified 5 major thematic areas: (1) perceptions of substance use among Black Southern rural men, (2) experiences with substance use, (3) contributing factors to substance use, (4) factors influencing the decision to accept treatment, and (5) factors associated with relapse. Each theme is explored in detail in the study’s subsequent sections. The overall grouping and organization of barriers and facilitators to SUD using the SEM is presented in Figure 1.

Socio-ecological model (SEM) of barriers and facilitators to substance use disorder acknowledgment, treatment, and relapse prevention among Black men residing in rural South Carolina, United States.
Perceptions With Substance Use
The majority of the participants understood substance use disorder as use of alcohol and drugs, as noted by 1 participant, “Substance abuse. . .substance disorder just mean, is a drug that you’re using that make you dysfunctional. . .but some of it be pills, cocaine, marijuana, liquor” (Transcript 220411-1410). However, some participants felt that substance use disorder did not stop at use of alcohol or drugs, rather that it extended beyond that to include misuse or abuse and other types of harm. This view was expressed by one of the participants, “Basically, mild habit of using mild substance abuse of overdosing with alcohol, it’s like . . .uhm. . .its always like you know overdosing it basically, you know like a eating disorder but mad as alcohol,” (Transcript 220330-1732). Another participant emphasized, “Its abusive. . .huh. . .may I say abusive I mean you do it too much and caused a scene. When the substance gets too much in your system and you can’t think, you over do it and then get in trouble, cause violenceand trouble it takes over” (Transcript 220411-1443).
They envisioned that substance use only crosses into abuse territory when it leads to dysfunctional behavior and suggested that consuming alcohol or drugs in moderation, without causing harm or dysfunction, does not constitute abuse as articulated by 1 participant, “If you drink alcohol, if you drink alcohol. . .you got meet up a person, not be able to control them but you like what they’re doing, you understand me? And you do it and if you, for instance go on my team, they’ll just want it” (Transcript 220411-1410). This view exemplifies a recognition that substance use becomes problematic when it impairs one’s ability to function effectively or leads to negative consequences. Therefore, while participants acknowledged the use of alcohol and drugs within their communities, they also held the importance of distinguishing between responsible consumption and abusive behavior.
Experience With Substance Use
Participants shared their diverse experiences with substance use within Black southern rural communities. Early and repeated exposure to substances in the community emerged as a recurrent theme, with all participants recounting encounters with various drugs throughout their lives and the effects. One participant vividly described “They have a lot of marijuana, they do crack-cocaine, they smoke pipe, they do everything, molly, everything they wanna do.” (Transcript 220316-1127). Another participant added “My friend. I’ve seen a lot, I’ve seen young ones, old ones, these days don’t be surprised what you see” (Transcript 220411-1410).
The negative impact of substance use on the broader community was also evident, with respondents directly attributing the prevalence of substance use as contributing factors to crime, death, and interpersonal conflicts. One of the participants explained, “I’ve seen people going to jail, marijuana cornered guys shot others a couple of weeks ago, you know all because of drugs, you know I can’t say I’ve been one of the people that shoot them, cause you know, I can’t. If you kill a Black, you know, you can’t want to kill a Black and then be on the side of Black too, you know one hand can’t watch while the other hand you know unless you straighten both hands out, yeah” (Transcript 220316-1155).
Factors Contributing to Substance Use
Participants in the study highlighted various factors contributing to substance use among Black rural southern communities. Ready availability to substances in the community emerged as a key factor, with majority noting the ease of access to drugs and alcohol in their surroundings. One participant remarked, “It’s basically all they sell us around here. Like more than half of guys ain’t finish school. Yeah, they are out by fourteen or fifteen and that’s all you know, no training, no parents, parents and drugs won’t do,” (Transcript 220330-1352), indicating the widespread presence of substances within these communities, especially with effects on young people.
Financial gains were identified as another significant driver of substance use, with participants describing how economic struggles and the attraction to quick money often led individuals to engage in substance-related activities. As 1 participant explained, “Wrong move, somebody gets addicted to it so they start saying hey he’s made the money and the first thing they say let’s explore. . . .and they knew that somebody else would need this because they see that he did it. So, it’s like a disease. . . .it starts spraying like a disease and that’s how drugs, alcohol abuse it begins to spray because it starts making money, starts being used, people start losing houses and cars and many get depressed if they fail to return their cars and drugs,” (Transcript 220411-1443).
Furthermore, the influence of boredom and peer pressure emerged as influential factors contributing to SUD. Participants described how idle time and social dynamics within their communities shape individual behaviors and decision-making to engage in drugs and alcohol. One participant reflected, “Well, I mean once. . . I mean if had nothing to do and you be around a certain crowd of people, eventually you start doing it and you might start trying this and that and then you might be here and it’s here and there and that will keep going on. And once you try it the first time, you know it’s like good taste, just like you try to take it the first time and continue trying it, you know,” (Transcript 220316-1308).
Personal challenges, including depression, financial strains, and going through hard times, were also identified as contributing factors. Participants frequently shared personal experiences of using substances as a means of coping with difficult circumstances or emotional distress. One participant explains, “Yeah, all the time, honestly, I thought about it before I went to jail and I had to turn myself in because something wrong was going on with me, see I missed a court hearing so I had to turn myself in but my friends were telling me they had never seen me drink like that before. But that was right after my wife had passed and I was just like. Like really yeah, seems I need help. That was the first time my friends ever talked to me like that” (Transcript 220330-1503).
Similarly, participants discussed how individuals often justified their substance use to manage stress or seek relaxation amidst life’s pressures, highlighting the strong relationship between substance use and stress coping mechanisms within these communities. One participant articulated, “What is it! It’s some-you know probably something to do, probably you know, chill out, sit back and relax and make you feel like you’ve had a good damn day working” (Transcript 220316-1155).
Factors Associated With Treatment Acceptance Decision Making
The analysis revealed a multitude of factors that influence individuals’ willingness to seek and engage in treatment for substance use disorders. Financial barriers emerged as a prominent deterrent to treatment acceptance, with participants citing lack of health insurance as a significant obstacle. One participant highlighted, “When Black people don’t have insurance to be honest, they won’t put too much care about us cause like we gonna be at -I mean I’ve seen this with my grandmother, it’s like when we don’t have insurance and happen to be a Black, it’s like you won’t be able to afford the medicine-the price they’ll charge you-more so if you had insurance. If you don’t have insurance, life is really hard, insurance now days is really hard, you know,” (Transcript 220316-1410). Reluctance to engage in treatment due to perceived financial or income loss was identified as another significant barrier. Participants expressed concerns about potential financial implications associated with seeking treatment, such as loss of income or employment opportunities. This fear of economic instability could deter individuals from pursuing treatment, as 1 participant mentioned, “Damn real, in fact everybody, drugs, drugs, drugs-look at- we’re constantly right here, you know I see it, we’re making a whole damn money, we’re making our money-. . .(laughs) Damn, open your eyes a little man, open your eyes a little. You don’t see it? (laughs) you know this shit damn well as I do. . .You see I can’t explain that what’s going on, you know it’s happening. I can’t, I can’t avoid it, I can’t help it, all I do is deal with it” (Transcript 220316-115).
Additionally, the influence of peer pressure and social circles was identified as another barrier to treatment acceptance. Participants described how social dynamics within their communities could deter individuals from seeking treatment, as 1 participant remarked, “Yeah, you’re around it, you’re around it but then you’re around it and you want out but can’t help it cause you’re surrounded and you’re like I can’t get myself out of this, you know, look at my surrounding I can’t do no that, you going nowhere, there no way,” (Transcript 220330-1421).
Non-recognition of the need for treatment emerged as a key barrier, with some participants underestimating the severity of their substance use or denying that their behavior warranted intervention. This self-denial often manifested as a reluctance to acknowledge personal vulnerability or the need for formal treatment. One participant expressed this sentiment directly: “No, I don’t need no help for it, because uhm. . .listen, maleor female, you got to understand what you want and what you’re doing. If you don’t want it, you don’t want it” (Transcript 220411-1443). Another participant elaborated on this mindset, explaining, “The key to ending things that you’re doing and success in life, is admit what you’re doing. . . if you don’t, trouble is gonna find you” (Transcript 220411-1443). The interplay between self-denial and non-recognition serves to illustrate how internal perceptions of readiness and problem acknowledgment critically shape individual treatment acceptance decisions. In parallel, skepticism toward the effectiveness and intent of drug policies and programs was also identified as a deterrent to seeking treatment. Some participants viewed these initiatives with suspicion, perceiving them as driven by political or economic agendas rather than genuine concern for community well-being. As 1 participant remarked, “You know, look at, all politician or everybody, look at them, any of them, Harvard whatever, they find a way to get away because you got an economy that makes this world revolve” (Transcript 220316-1155)
Participants did, however, identify potential facilitators to treatment acceptance. The majority of participants recognized SUD as a pressing issue that requires individual awareness to seek treatment. One participant asserted, “The key to ending things that you’re doing and success in life, is admit what you’re doing. . .if you don’t, trouble is gonna find you” (Transcript 220411-1443). Participants expressed the value of community-based awareness campaigns and educational programs in fostering treatment acceptance. Listening to 1 participant, “Well basically, you talk, go out make speeches around the community, you know like, uh, get a little microphone and tell them where you’ll be having a meeting in certain place where you’ll all be meeting at a certain time. Some will show up, some won” (Transcript 220316-1245).
Enhancing access to SUD treatment centers in rural areas emerged as a key facilitator of treatment acceptance. “But, if you get a treatment center down here and 1 person goes in, one, two people go in, they start seeing people changing, it’s like a flower which is starting to blossom. . .uh blooming. You like oh yeah, this person is starting to change, this person is making progress. Let me see if I can do it. Everybody not gonna wanna do it, you gonna have certain people who are like am not doing it, they’re gonna be stuck in the old ways. But you will have people who will be like it’s time for me to change, it’s time for me to go back and give back what I need to give back. In life, that person got my life better, you know, once you get that” (Transcript 220316-1308).
Similarly, other support systems were mentioned, these included family support during the treatment journey, professional support, and support from community leaders. Participants said, “Having my family behind me makes a big difference” (Transcript 220330-1759), “Just in Columbia, and so I dealt with that and got out but it helped me a lot man, it helped me a lot and that was something I did, trying to get some help. But you can’t just stop if you let your body control you down, don’t let your body control you down” (Transcript 220316-1127), shared a participant, highlighting the beneficial role of professional guidance and assistance in the treatment process. “Because, if a stranger come out and say. . .and start telling you man. . . . you need treatment, I’ll say man you don’t know me. . .mind your own business, leave me the hell alone. But if you know me, you tell me bro let me talk to you, you just talk to that person from the beginning” (Transcript 220330-1759), noted a participant, showing the importance of involving a community leader or well-known person.
Recognition of personal need to change was also mentioned as key in initiating the treatment-seeking process. “I don’t need nothing cause it’s a mind thing to me. If you’re strong by average and you can’t feel a kicking or motivated a little, when you get older, think about it, you see like. . .why am I using these drugs? I don’t need all this staff to act satisfied, I don’t need this anymore, see” (Transcript 220330-1352), showing the importance of self-awareness and acknowledgment in overcoming barriers to treatment acceptance.
Factors Associated With Substance Use Relapse
Factors associated with the theme substance use relapse encompass a variety of influences that contribute to individuals returning to substance use following a period of abstinence or recovery. Participants identified easy access to substances as a significant environmental factor contributing to relapse. “They’re gona. . . . . .they gonna, they’re gonna relapse man. You see in this area, they aint gonna be able to give it up man because everywhere they go, payment there and there. Somebody will tell them oh come on here man, come on and do it with me and they’re like man, okay ama gonna try it last time and they keep on trying it,” expressed 1 participant from Transcript 220316-1127, showing the challenge of maintaining abstinence in environments where substances are readily available and socially acceptable.
Participants also talked about personal challenges in influencing relapse. Among these, participants mentioned the experience of depression which was recognized as a personal challenge that can contribute to relapse. “Because, in my situation, you know, am very smart in a lot of things but education don’t help, you know, and you need a good job but you can’t too, cause if you can’t get a job with a man as educated as I am, then the pressure man, it will lead you to sadness and you’ll want where you gona put it. Then you gona start to join masses that make you wanna take a drink or smoke a cigarette or something but am stuck again, am too old man for this. But then, a lot of people, am talking about citizens, a lot of people is sad, slow or need help, they got a problem or many problems,” shared a participant from Transcript 220330-1421, indicating the role of societal pressures related to socioeconomic status/educational achievement and depressive symptoms in triggering substance use as a coping mechanism.
Financial difficulties were cited as another personal challenge that can increase the risk of relapse. “Oh yeah, definitely because if you. . .if you know you can’t pay the rent or you can’t pay your light that might be you know, you’re going to take a drink and try to figure out man, I can’t deal with this, how am I gonna deal with this? How am I gonna pay this rent? How am I gonna pay this lighting bill? How am I gonna feed my child? And you know it could be pressure coming from inside out because I know. . .I got a lot who say, you need to do something, you need to do something about this and I guess as a Black man, you’re supposed to be the head of the family so there’s a lot of pressure with that. If you can’t live up to the expectations of the family that they want to, so that may lead to some use or relapse,” noted 1 participant from Transcript 220330-1732.
Participants also acknowledged that going through difficult life circumstances can heighten vulnerability to relapse. “Mo. . . . most times the cause of relapse, uhm. . .is something destined to happen and you can’t control your anger, somebody died, you just caught your spouseor somebody doing something behind your back. . . . you turn back to drinking or lose control, whatever, do something crazy cause you’re angry. Now, that sort of thing either sues you or make you do something crazy and you do it for whatever they’re gonna do, they give you that boost. Its that boost to either. . .say forget it or that boost to say whatever is on your mind that you’ve been holding all along for so long, therefore causing relapse. Somebody lose a loved one, somebody shoot your brother and then like that . . . . that’s cause of relapse,” expressed a participant from Transcript 220330-1759.
Social influences, particularly peer pressure and social circles, were identified as significant factors contributing to relapse. “When everyone around you is using, it’s hard to stay clean,” shared 1 participant from Transcript 220330-1759, highlighting the influence of social dynamics on substance use behaviors and the risk of relapse in peer-driven environments. These social dynamics were also emphasized by another participant, “Uhm. . .basically hanging around the same people that are doing what you’re trying to get away from and then you know, peer pressure. They you know, come on, you can drink one or you can smoke one, that’s the main reason why a lot of people relapse. You know, being around the same people, same circle of friends or whatever and then may be might have some life changing event that happen in your life and you just might say you know what, I lost my sonor daughter, I can’t take this, I gotta go take a drink or a smoke or lose your job or something like that,” (Transcript 220330-1732).
Socio-Ecological Model (SEM) of Barriers and Facilitators to SUD Acknowledgment, Treatment, and Relapse Prevention
Highlights the complexity of SUD among this population, Figure 1 presents a synthesized mapping of the study’s main findings within the SEM framework and provides a visual and narrative bridge between the lived experiences of Black men in rural South Carolina and the multi-layered factors shaping substance use disorder (SUD) trajectories. This representation contextualizes the pathways through which substance use is shaped and sustained at the personal, relational, community, and systemic level, and provides critical leverage points for the design of targeted, culturally responsive, and multi-level SUD interventions.
At the individual level, participants emphasized personal agency, mental health struggles, and treatment readiness as pivotal themes. One participant shared, “Yeah, all the time. . . that was right after my wife had passed. . . I was just like, really yeah, seems I need help” (Transcript 220330-1503), underscoring the critical role of emotional distress and grief in substance use decisions. Another participant described using substances as a form of stress relief: “Probably something to do, probably you know, chill out, sit back and relax and make you feel like you’ve had a good damn day working” (Transcript 220316-1155). Interpersonal factors centered around family dynamics, peer influence, and the importance of social support networks. For example, 1 participant highlighted the value of family backing: “Having my family behind me makes a big difference” (Transcript 220330-1759), while another emphasized the influence of peer circles on relapse risk: “You know, being around the same people, same circle of friends. . .you just might say. . . I lost my son or daughter, I can’t take this, I gotta go take a drink or a smoke” (Transcript 220330-1732). Community-level determinants included both structural facilitators and barriers such as access to services and trust in local systems. Participants noted pervasive substance availability: “It’s basically all they sell us around here. . . no training, no parents. . . and drugs won’t do” (Transcript 220330-1352), reflecting how environmental saturation of substances perpetuates risk. Trustworthiness of local interventions also emerged as a concern, with participants stating a preference for treatment led by familiar figures: “If a stranger comes out. . . you need treatment, I’ll say man you don’t know me. . . But if you know me, you tell me bro let me talk to you. . .” (Transcript 220330-1759). Finally, the structural and societal level encapsulated systemic barriers including transportation difficulties, healthcare access, and the enduring legacies of racial discrimination. Participants voiced the economic and social precarity they face, with 1 noting, “If you can’t get a job with a man as educated as I am, then the pressure. . . will lead you to sadness and you’ll want. . . to take a drink or smoke a cigarette” (Transcript 220330-1421), exemplifying how socioeconomic pressures intersect with SUD risk.
Discussion
This formative study sought to gain insights into the socio-ecological and structural factors that shape SUD among Black men in the rural US South. The findings from this research, capturing the lived experience of these men, highlight the complexity of substance use behaviors, as well as the multiple barriers, and facilitators influencing both treatment acceptance and relapse prevention. When viewed through the SEM framework, the study’s findings serve to illustrate the complex, multi-level nature of SUD experiences among Black men in rural South Carolina. At the individual level, participants highlighted the interplay between personal agency, emotional well-being, and treatment readiness, factors well-documented as critical to SUD intervention success.39,40 Interpersonal dynamics, particularly the supportive or detrimental roles of family and peers, emerged as pivotal influences on treatment engagement, and relapse, mirroring other researcher’s findings on the importance of social networks in recovery trajectories.41,42 Community-level insights revealed persistent mistrust of local service providers and the environmental saturation of substances, exemplifying the need for culturally competent, community-embedded interventions to rebuild trust and improve engagement.43,44 At the structural level, participants described systemic barriers, including transportation challenges, economic hardship, and racial discrimination, that compounded risk and impeded sustained recovery, reinforcing broader evidence on the influence of social determinants of health.45,46 Collectively, these findings emphasize that effective SUD interventions in this context must simultaneously operate across multiple ecological levels, addressing both individual behaviors and the broader relational, community, and systemic structures that shape substance use risk and recovery opportunities.
The investigation of the 5 major themes—perceptions of substance use, personal experiences, contributing factors, decision-making for treatment acceptance, and relapse triggers, offers valuable insight into the lived experiences and realities of this underserved population. One of the key findings of this study relates to the varied perceptions of substance use, where participants emphasized that substance use only becomes problematic when it leads to dysfunction or harm. This commonly shared belief among participants suggests that SUD interventions should account for culturally specific understandings of “abuse” and “misuse” to be effective.47,48
The study also serves to illustrates how community dynamics, family structures, and social environments play a critical role in shaping substance use behaviors. The presence of substances within these communities, combined with financial hardships, peer pressure, and the normalization of substance use, exacerbates the risk of SUDs. Personal challenges such as depression 49 and coping with stress 50 further contribute to substance misuse, making it imperative that interventions also address mental health and socio-economic pressures.17,51
One significant barrier to treatment acceptance for Black males in the rural US South is the lack of access to healthcare services, compounded by systemic racism 52 and historical mistrust in medical institutions.13,53 The participants’ narratives highlighted not only financial challenges, such as lack of insurance, but also the powerful social influence of peer pressure 54 which often deters individuals from seeking treatment.16,55 These findings resonate with broader research showing that economic instability and systemic healthcare inequities create major obstacles for minority populations in rural areas. 19 Additionally, the reluctance to seek treatment due to the fear of income loss or the perceived futility of medical assistance reflects a deeper disillusionment with existing structures of support. 14 However, several facilitators were identified that could enhance treatment engagement. Community-based interventions, particularly those involving trusted local leaders or well-established figures, were seen as pivotal in raising awareness and reducing stigma. Participants expressed a desire for treatment centers within their communities, suggesting that proximity and visibility of recovery services may increase treatment acceptance. The importance of family support and self-awareness also emerged as critical factors that help sustain recovery and prevent relapse.32,56
Relapse, as discussed by participants, is often driven by personal and environmental factors. The easy availability of substances within the community, combined with personal struggles like financial hardship and depression, heightens the likelihood of relapse. 57 The study sheds light on the fact that sustained recovery is particularly challenging in environments where peer pressure is constant, and access to substances is ubiquitous.12,55 Additionally, life events—such as the death of a loved 1 or loss of a job—can act as triggers, leading individuals to return to substance use as a coping mechanism. These insights emphasize the need for comprehensive long-term support systems that address not only the individual’s recovery but also the broader social and environmental contexts that contribute to relapse58,59
In comparison to other investigations of this kind, our study reinforces the call for culturally tailored, community-driven interventions that address the specific socioecological and structural realities 48 faced by Black men in the rural US South. Our findings supports the need for targeted intervention strategies to address urgent treatment gaps that are also considered systemic barriers to healthcare, such as lack of insurance and mistrust in medical institutions, while promoting community involvement and peer-led recovery programs.59,60 Our study posits that addressing the root causes of substance use, including economic instability and social stigma, is essential for reducing both the incidence of SUDs and the high rates of relapse in these Black communities.
Limitations
This study has several known limitations that should be acknowledged. First, we employed the use of snowball sampling, a strategy that, while useful for accessing hard-to-reach populations, may introduce bias through the over-representation of certain social networks which can limit the diversity of perspectives captured. Second, although we achieved thematic saturation after 10 interviews, we recognize that some researchers recommend a larger sample size. Third, while participants varied in age, employment, and treatment history, we did not systematically assess or explore the influence of socioeconomic variation within our sample which may limit the transferability of findings to individuals from different socioeconomic backgrounds. Finally, although we did share identified themes with local community leaders and healthcare providers for confirmatory validation, we did not conduct member checking (ie, returning transcripts or findings to participants for their validation), which may reduce the confirmability of our findings.
Conclusion
This formative study aimed to explore socio-ecological and structural factors influencing substance use disorders (SUDs) among Black men in the rural US South. Through an examination of personal narratives and community experiences, it identifies critical barriers to treatment acceptance, including financial constraints, mistrust in healthcare systems, and social pressures. Furthermore, the research highlights factors that contribute to relapse, such as easy access to substances, depression, and peer influence. It also reveals potential facilitators for treatment acceptance, such as community-based interventions, family support, and self-awareness. Our findings support the importance of culturally sensitive and ecologically grounded approaches to addressing SUDs, with interventions that resonate with the lived experiences of this population. While this exploratory study offers valuable insights, further research is needed to inform broader intervention design for addressing SUDs and related health disparities in Black Southern US rural communities.
Supplemental Material
sj-docx-1-sat-10.1177_29768357251349918 – Supplemental material for Exploring Socio-Ecological and Structural Factors Among Black Men in Rural South Carolina to Inform Substance Use Disorder Interventions: A Qualitative Study
Supplemental material, sj-docx-1-sat-10.1177_29768357251349918 for Exploring Socio-Ecological and Structural Factors Among Black Men in Rural South Carolina to Inform Substance Use Disorder Interventions: A Qualitative Study by Serge R. Wandji, Jean E. Davis, Monica H. Swahn, Mohan Madisetti and Charlene Pope in Substance Use: Research and Treatment
Footnotes
Abbreviations
IRB: Institutional Review Board
PI: Principal Investigator
RUCC: Rural-Urban Continuum Code
SEM: Social Ecological Model
SC: South Carolina, USA
SUD: Substance use disorders
Ethical Considerations
The study protocol underwent review and approval by the University of South Carolina Institutional Review Board. The study was conducted in compliance with Good Clinical Practices (GCP) of the International Conference of Harmonization (ICH) and accordance with the Declaration of Helsinki as revised in 2013.
Consent to Participate
Written consent was obtained from all participants prior to the conduct of study procedures.
Consent for Publication
Participants provided consent for the data to be used for publication purposes without identifying information.
Author Contributions
The authors meet the International Committee of Medical Journal Editors (ICMJE) authorship Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals and have approved the final version of this manuscript. SRW: Conceptualization, Methodology, Funding acquisition, Project administration, Investigation, Data curation, Formal analysis, Writing—Original draft, Writing—Review and editing; JED: Supervision, Conceptualization, Methodology, Data curation, Formal analysis, Writing—Review and editing; MHS: Supervision, Formal analysis, Writing—Review and editing; MM: Writing—Review and editing, Visualization; and, CP: Supervision, Methodology, Formal analysis, Writing—Review and editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Serge Wandji was supported by the Substance Abuse and Mental Health Services Administration (SAMHSA; Grant# 5H79SM080386-05). The views expressed in written training materials or publications and speakers and moderators do not necessary reflect the official policies of the Department and Human Services nor does mention of trade names commercial practices, or organization imply endorsement by the U.S. Government.
This work was also supported by Global Health Equity Scholars (GHES) Program from the Fogarty International Center of the National Institutes of Health (Grant# D43TW010540). The content is solely the responsibility of the authors and does not necessarily represent the official views nor imply endorsement by the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets produced under this research study are available upon reasonable requests made to the corresponding author.
Generative AI and AI-Assisted Technologies
The authors declare that no generative AI or AI-assisted technologies were used in the creation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.