
Abstract
Objective:
Adults receiving residential treatment for substance use disorders (SUDs) who have comorbid psychopathology face unique challenges, including an increased risk of substance use craving and treatment dropout against medical advice (AMA). Prior studies have investigated associations between specific forms of psychopathology and these outcomes. However, psychological disorders often co-occur and may cluster together to amplify risk for craving and treatment dropout AMA.
Methods:
This study used latent class analysis to identify patterns of psychopathology in 1046 adult patients receiving residential treatment for SUDs (73.7% men; Mage = 42.31, SD = 12.13). We tested whether psychopathology classes differed in alcohol and drug cravings and treatment dropout AMA. We identified 4 latent classes: (1) high psychopathology, (2) moderate anxiety/depression, (3) illness anxiety/somatic problems, (4) low psychopathology.
Results:
The high psychopathology class reported significantly more alcohol and drug cravings than all other classes. The moderate anxiety/depression class also reported more alcohol cravings than the low psychopathology class. Additionally, the high psychopathology, illness anxiety/somatic problems, and moderate anxiety/depression classes had higher proportions of patients who dropped out of treatment AMA compared to the low psychopathology class.
Conclusion:
These findings suggest that comorbid psychopathology significantly impacts treatment outcomes in residential SUD treatment programs. Targeted interventions that address comorbid psychopathology may help reduce craving and improve treatment retention.
Introduction
National data show that 37.9% of people with substance use disorders (SUDs) report comorbid psychopathology, and rates of comorbidity are even higher among those who seek residential treatment for substance use.1,2 However, some residential treatment programs target substance use in isolation without adequately addressing the potential underlying impact of comorbid psychopathology on substance use. 3 Such approaches can hinder treatment outcomes for patients with comorbid psychopathology—often referred to as patients with dual diagnosis—as they face unique challenges in residential treatment. Patients with dual diagnosis may use substances to cope with psychological distress. 4 Without adaptive coping skills, they may experience elevated anxiety and depression in treatment, which is linked to increased distress and substance use craving. 5 Higher craving during treatment is associated with a greater likelihood of dropping out against medical advice (AMA) and poorer treatment outcomes.6,7 Understanding which constellations of psychopathology are related to increased craving and treatment dropout could improve the identification of SUD patients who may benefit from tailored, evidence-based interventions. This study used latent class analysis to examine associations between patterns of psychopathology, craving, and treatment dropout.
Comorbid Psychopathology and Craving
In accordance with conceptual models that explain the role of craving in SUDs, negative affect may be an especially salient predictor of craving for alcohol or drugs, particularly during the early phases of substance use treatment when the effects of withdrawal may be higher. 8 People with mood or anxiety disorders may be especially prone to experiencing negative affect during treatment, particularly when substance use was their primary emotion regulation strategy. Among those who used alcohol, people who experienced craving were more likely to have a mood, anxiety, or personality disorder relative to people who did not experience craving. 9 In fact, individuals in SUD treatment with mood or anxiety disorders had more craving intensity and more substance use relative to those without comorbid mood or anxiety disorders. 10 There may also be important differentiation within anxiety disorders. Individuals who experience somatic symptoms related to their anxiety may be particularly vulnerable to craving, as they may use substances to alleviate their physical discomfort. 11 These somatic symptoms may also explain the association between anxiety disorders and relapse after SUD treatment. 12 Moreover, anxiety symptoms have been linked to early treatment dropout AMA. 13 Investigating the specific patterns of psychopathology associated with craving is essential to improving treatment retention and outcomes.
Psychopathology and Treatment Dropout
Numerous studies have investigated the associations between psychopathology and dropout from residential SUD treatment. Greater depressive symptom severity has been linked to increased rates of SUD treatment attrition, potentially due to hallmark features of depression such as low motivation and disinterest in completing treatment. 14 Further, anxiety symptoms, which underlie several psychological disorders, have also been associated with poor treatment retention. For example, one study found that generalized anxiety disorder (GAD) symptoms predicted leaving residential SUD treatment AMA, over and above the effects of depressive symptoms and SUD severity. 15 Social anxiety disorder (SAD) symptoms may also be particularly relevant in the context of SUD treatment programs that heavily rely on group psychotherapy. A prior study demonstrated that SAD symptoms were predictive of treatment dropout AMA, independent of depressive symptoms, posttraumatic stress disorder (PTSD) symptoms, GAD symptoms, and SUD severity. 13 PTSD, which frequently co-occur with SUDs, 16 has also been implicated as a potential predictor of treatment dropout AMA. Given the high comorbidity between these conditions, some SUD treatment centers integrate trauma-focused interventions into their programs. However, the association between PTSD symptom severity and treatment retention remains complex and inconsistent. Some studies showed that individuals with elevated PTSD symptoms were more likely to complete SUD treatment, particularly when trauma-focused interventions were provided.13,17 This suggests that addressing trauma-related symptoms could enhance treatment engagement and adherence. Conversely, receiving exposure-based PTSD interventions, which can exacerbate PTSD symptoms in the short-term, have been shown to increase dropout rates in cases where post-exposure distress and craving were heightened. 18 These mixed findings underscore the need for further research on the associations between PTSD symptoms, comorbid psychopathology, and treatment dropout.
Psychological disorders often co-occur and share transdiagnostic features, such as impulsivity, which is a feature of several psychological disorders, including SUDs, PTSD, personality disorders, and depressive disorders. 19 A recent study found that specific facets of impulsivity (ie, lack of perseverance and sensation seeking) were associated with greater odds of treatment dropout AMA among women in SUD treatment. 20 Given the overlap and shared features of psychopathology, examining clusters of psychopathology and their association with treatment dropout may be especially informative for interventions. For example, one study used latent profile analysis to identify subgroups of SUD and psychopathology severity among patients in SUD treatment. 21 They found that individuals with high drug use and severe psychopathology were at the greatest risk for early treatment dropout relative to other profiles. Similarly, another study employed latent class analysis to identify patterns of comorbid psychopathology and identified 3 distinct classes: a low-comorbidity class, a class with co-occurring major depressive disorder, and a class characterized by multiple forms of comorbid psychopathology. 22 However, no known studies to date have simultaneously identified patterns of psychopathology among SUD patients and examined which clusters are most strongly associated with craving and treatment dropout AMA.
Current Study
Prior studies examining associations between psychopathology, craving, and treatment dropout among adults in residential SUD treatment have primarily employed variable-centered approaches, focusing on the independent effects of specific psychopathology. This approach presents a critical limitation, as many forms of psychopathology often co-occur. To address this gap, further person-centered research is needed to identify constellations of psychopathology that associate with high risk for craving and treatment dropout. Such research could inform the development of targeted interventions to enhance treatment for these high-risk groups. This study aimed to address this gap by identifying patterns of psychopathology using latent class analysis (LCA) in a sample of adults in residential SUD treatment. Consistent with prior LCA studies of psychopathology, 22 we expected to find distinct classes characterized by multiple forms of comorbid psychopathology, few forms of comorbid psychopathology, and specific clusters of psychopathologies (eg, individuals with major depressive disorder). Further, we expected that classes with more comorbid psychopathology would report more craving and have higher rates of treatment dropout AMA relative to classes with less psychopathology.
Method
Participants and Procedures
Study procedures were approved by the Institutional Review Board at the last author’s institution. Data were derived from medical records of patients in residential treatment for SUDs at a facility in the southeastern United States between December 2019 and October 2021. Participants were at least 18 years old and had been diagnosed with a SUD after consulting with a treatment team comprising a general physician, licensed social workers, and substance use peer counselors. As part of routine care following medical detoxification, participants completed a series of self-report measures. All participants signed an informed consent form for their deidentified medical records to be accessed for research purposes. Additionally, the Institutional Review Board at the University of Tennessee provided the researchers permission to review medical records at the affiliated residential substance use treatment center. Medical record data only contained participants’ scored self-report measures; therefore, we could not calculate Cronbach alphas for the measures as we did not have access to their individual responses to items. After medical detoxication, participants received treatment based on a traditional abstinence-based (ie, 12-Step) model. Participants also received individual psychotherapy, family psychotherapy, and group psychotherapy/psychoeducation that used evidence-based strategies, including cognitive behavioral therapy, dialectical behavior therapy, and schema-focused therapy. Some patients also receive medication-assisted treatment, as needed (eg, Suboxone for opioid use disorder). Notably, participants who had trauma-related distress might have also received both group and individual cognitive processing therapy. Participants typically were in treatment between 28- and 30-days after medical detoxification.
Participants (N = 1046; Mage = 42.31, SD = 12.13) were predominantly male (73.7%) and White (89.7%), followed by Black/African American (4.3%), Multi-Racial (1.00%), and other racial identities (eg, American Indian, Asian; 2.3%), whereas 3.1% preferred not to share their racial identity. Additionally, 3.1% of participants were Hispanic/Latinx. Most participants were diagnosed with an alcohol use disorder (85.1%), followed by cannabis use disorder (30.4%), opioid use disorder (23.9%), stimulant use disorder (23.7% total; cocaine [12.4%]; amphetamine [16.3%]), sedative use disorder (19.6%), hallucinogen-related disorders (4.2%), and inhalant use disorder (0.4%). Percentages for SUDs add up to more than 100% because 49% of participants had more than 1 SUD diagnosis. Participants, on average, spent 27.7 days (SD = 5.6) in treatment (range = 3-30 days). In regards to treatment dropout, 16.6% (n = 174; Mage = 39.68, SD = 12.89) dropped out of treatment AMA. Among those who dropped out of treatment AMA, most were women (64.9%) and White (92.0%), followed by Black/African American (4.0%), Asian (1.1%), or another racial identity (1.7%).
Measures
Demographics
We obtained participants’ demographics from their medical record at the residential substance use treatment center. Demographics and identities included age, sex assigned at birth, and race/ethnicity.
Treatment Completion
Treatment completion was coded as either “AMA” (0) or “completed” (1), with participants who left treatment before their discharge date against the advice of their treatment team being coded as AMA and those who remained in treatment until their discharge date being coded as completed. Participants who were transferred to a different level of care to better fit their needs were also coded as completed. Patients who withdrew from treatment for administration reasons (eg, a change in insurance) were excluded from analyses (n = 73). We also capped the maximum number of days in treatment completed to 30 days to reflect only the days participants spent in residential treatment. Moreover, we excluded the days from analyses that some patients spent in extended care (ie, additional time in treatment after the initial 28–30-days), as this is not part of the general residential treatment program.
Psychiatric Diagnostic Screening Questionnaire
Participants completed the Psychiatric Diagnostic Screening Questionnaire (PDSQ). 23 The PDSQ is used in clinical settings to screen for common DSM-IV Axis I disorders to facilitate diagnostic evaluations. 23 For each item, participants rated whether it applied to them (1 = yes, 0 = no). We then summed responses to create a total score for each subscale. Higher scores on each subscale indicated more symptoms of the associated psychological disorder. The PDSQ includes subscales that correspond with diagnostic criteria for major depressive disorder, bulimia nervosa, posttraumatic stress disorder, panic disorder, agoraphobia, social anxiety disorder, generalized anxiety disorder, obsessive-compulsive disorder, alcohol use disorder, drug use disorder, somatic symptom disorder, illness anxiety disorder, and psychotic disorders. Given the low rates of clinically significant symptoms of bulimia nervosa and psychosis in this sample, we excluded these subscales from analysis. We also excluded the alcohol use disorder and drug use disorder subscales considering that most participants in this sample met criteria for both SUDs. Previous research in clinical settings demonstrated that the PDSQ subscales have strong internal consistency and can predict diagnoses of psychological disorders.23,24
Penn Alcohol Craving Scale
We measured alcohol cravings using the Penn Alcohol Craving Scale (PACS). 25 The PACS is a 5-item measure of alcohol cravings that assesses the duration (eg, “How much time have you spent thinking about drinking or about how good a drink would make you feel during this period?”), frequency (eg, “How often have you thought about drinking or about how good a drink would make you feel during this period?”), and intensity (eg, “At its most severe point, how strong was your craving during this period?”) of alcohol cravings within the past week. We also administered a revised 5-item version of the PACS to also assess drug cravings, where we substituted “alcohol” in each item for “drugs.” All items were rated on a 6-point Likert scale, with the labels for each scale differing depending on the item. Responses to each item are summed to create a total alcohol or drug cravings score, with higher scores reflecting more intense, long-lasting, and frequent alcohol or drug cravings. Total scores range from 0 to 30, with studies suggesting that scores of 15 or higher may indicate clinically significant craving 26 ; however, a clinically significant cutoff has not yet been identified for the adapted drug craving version. The PACS has demonstrated strong psychometric properties in its initial validation. 25
Data Analytic Strategy
Three-step LCA was conducted in Mplus Version 8.10 with the maximum likelihood estimator, which categorized participants into subgroups with similar psychopathology. We started with a 6-class model and tested subsequent models by reducing the number of classes. We constructed LCA models using 9 dichotomous psychopathology indicators and we selected the best-fitting model by evaluating several fit indices, including the Aikaike information criteria (AIC), Bayesian information criteria (BIC), adjusted Bayesian information criteria (aBIC), and the adjusted Lo-Mendell-Rubin likelihood ratio test (LMR-LRT). For each fit index, lower values suggested better model fit. 27 The LMR-LRT assesses whether a k-class model fits significantly better than a k-1 class model. 27 When selecting the optimal latent class solution, we considered these fit indices, theoretical interpretability, and the size of the smallest class in each model. After we selected the model with the optimal number of classes, we used the Bolck, Croon, and Hadenaars (BCH) command in Mplus 28 to automatically assess differences in demographic variables as well as in levels of alcohol and drug cravings and treatment dropout AMA across latent classes using chi-square tests. 29
Results
Descriptive Statistics
For bivariate correlations between study variables as well as means and standard deviations for each variable, see Table 1.
Bivariate correlations, means, standard deviations of study variables.

Abbreviations: AMA, left treatment against medical advice (completed = 0, dropped out = 1); GAD, generalized anxiety disorder; MDD, major depressive disorder; OCD, obsessive-compulsive disorder; PTSD, posttraumatic stress disorder; SAD, social anxiety disorder.
Sex assigned at birth was coded dichotomously (men = 0, women = 1).
P < .01. *P < .05.
Latent Class Enumeration
Results suggested that a 4-class model was the best-fitting solution with good convergence (see Table 2). The 4-class had lower AIC and aBIC values than the 3-class model as well as lower BIC and aBIC values than the 5-class model. Further, the 4-class model had statistically significantly better fit relative to the 3-class model (LMR-LRT = 65.295, P = .002) and the 5-class model did not have statistically significantly improved fit (LMR-LRT = 31.23, P = .328). In the 4-class model, the smallest class size was 8.0% of the sample, whereas in the 5-class model, the smallest class size was 4.3% of the sample, suggesting that the 4-class model has more distinct, prevalent classes. Finally, the 4-class model was highly theoretically consistent and interpretable.
Model fit indices for latent class models specifying 1 to 6 classes (N = 1046).
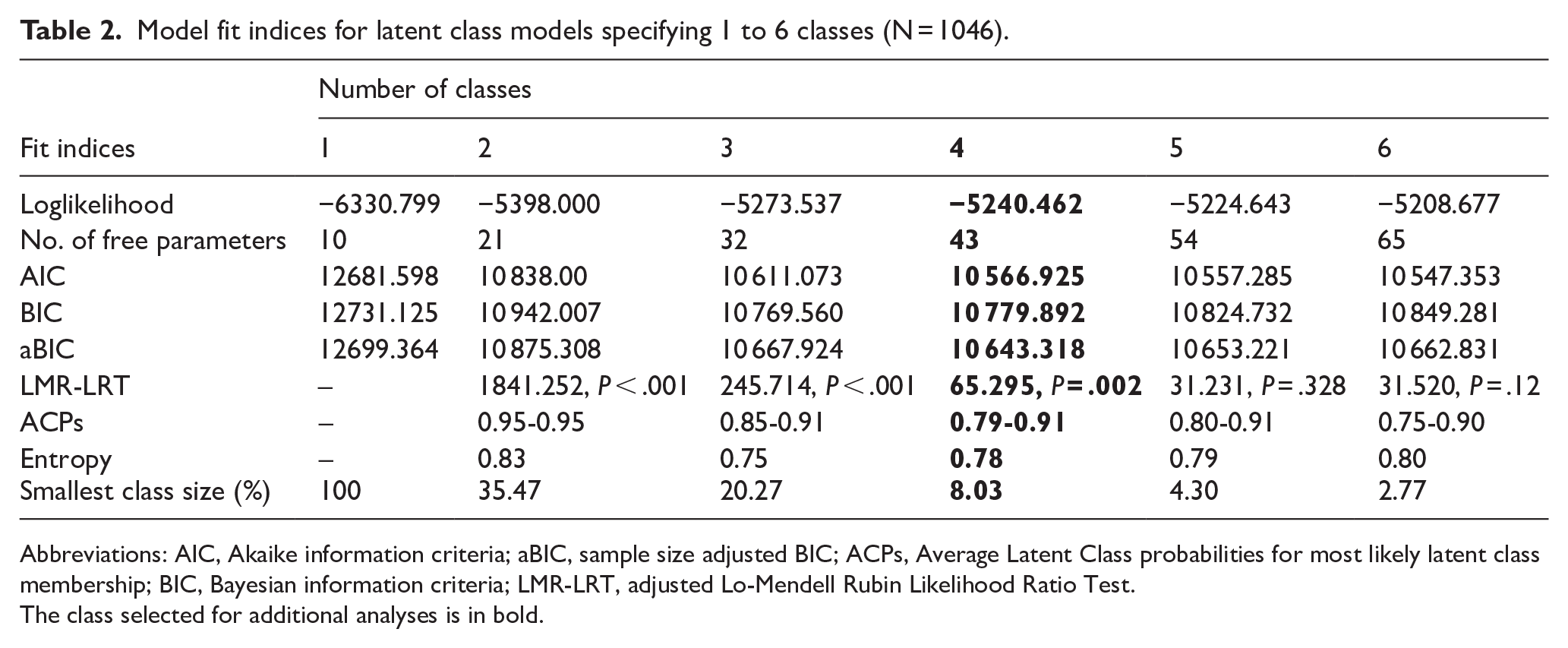
Abbreviations: AIC, Akaike information criteria; aBIC, sample size adjusted BIC; ACPs, Average Latent Class probabilities for most likely latent class membership; BIC, Bayesian information criteria; LMR-LRT, adjusted Lo-Mendell Rubin Likelihood Ratio Test.
The class selected for additional analyses is in bold.
We identified a 4-class solution (see Figure 1). Participants in the high psychopathology class (n = 212) had high item-response probabilities on major depressive disorder (.86), posttraumatic stress disorder (.77), panic disorder (.88), agoraphobia (.75), social anxiety disorder (.89), generalized anxiety disorder (.92), and obsessive-compulsive disorder (.74). Further, individuals in the high psychopathology class had moderate item-response probabilities on somatic symptom disorder (.68) and illness anxiety disorder (.59). Those who were in the moderate anxiety/depression class (n = 340) had moderate item-response probabilities on major depressive disorder (.58), posttraumatic stress disorder (.46), social anxiety disorder (.50), and generalized anxiety disorder (.42). Individuals in the illness anxiety/somatic problems class (n = 84) had high item-response probabilities on somatic symptom disorder (.80) and illness anxiety disorder (1.00), as well as moderate item-response probabilities on major depressive disorder (.47) and obsessive-compulsive disorder (.57). Finally, participants in the low psychopathology class (n = 409) had generally low item-response probabilities on all latent class indicators (.01-.11).

Item probabilities of endorsing clinically significant psychopathology for each latent class.
Differences in Outcome Variables
Chi-square tests revealed significant differences across the 4 classes in age, sex assigned at birth, treatment dropout AMA, alcohol cravings, and drug cravings (see Figure 2).

Alcohol and drug craving means across each latent class.
The low psychopathology class was older (M = 45.60, SE = .65) than the high psychopathology (M = 39.53, SE = .87) and moderate anxiety/depression classes (M = 39.38, SE = .82), χ2 (1) = 29.14-23.02, P < .001. The illness anxiety/somatic problems class was also older (M = 45.24, SE = 1.68) than the high psychopathology and moderate anxiety/depression classes, χ2 (1) = 8.60-9.15, P < .001 to P = .003. The high psychopathology class had more women relative to the illness anxiety/somatic problems, low psychopathology, and moderate anxiety/depression classes, χ2 (1) = 5.37-34.93, P < .02. The moderate anxiety/depression class contained more women than the low psychopathology class, χ2 (1) = 11.84, P = .001.
The high psychopathology class had more alcohol cravings (M = 11.28, SE = .76) than the illness anxiety/somatic problems (M = 8.19, SE = 1.13), moderate anxiety/depression (M = 8.43, SE = .56), and low psychopathology (M = 6.04, SE = .41) classes, χ2 (1) = 4.85-37.99, P < .001 to P < .028. Further, the moderate anxiety/depression class had more alcohol cravings than the low psychopathology class, χ2 (1) = 10.01, P = .002. The high psychopathology class also had more drug cravings (M = 8.74, SE = .69) than the illness anxiety/somatic problems (M = 5.63, SE = 1.08), moderate anxiety/depression (M = 6.80, SE = .55), and low psychopathology (M = 2.57, SE = .33) classes, χ2 (1) = 4.25-66.00, P < .001 to P = .039. Additionally, both the illness anxiety/somatic problems and moderate anxiety/depression classes had more drug cravings than the low psychopathology class, χ2 (1) = 7.34-35.88, P < .001 to P = .007. The high psychopathology, illness anxiety/somatic problems, and moderate anxiety/depression classes were all more likely to drop out of treatment AMA relative to the low psychopathology class, χ2 (1) = 5.38-11.30, P = .001-.02 (see Figure 3). No other classes differed significantly in distal outcome variables.

Treatment dropout AMA means across each latent class.
Discussion
These findings highlight distinct patterns of psychopathology among individuals in residential SUD treatment. Somewhat consistent with prior findings, 22 we identified a class characterized by multiple forms of psychopathology, a class characterized by minimal psychopathology, and another class with moderate elevations in major depressive disorder and anxiety disorders. We also identified an additional fourth class containing individuals who reported elevations in somatic symptom disorder and illness anxiety disorder, which may reflect related disorders characterized by heightened focus on and distress about physical symptoms and health concerns.30,31 Overall, these findings replicate prior LCA findings and advance these findings by testing which classes differ in outcomes relevant to SUD treatment retention.
For alcohol craving, participants in the high psychopathology class reported the highest levels relative to all other classes. Moreover, those in the moderate anxiety/depression class reported greater alcohol cravings compared to the low psychopathology class but did not differ from the illness anxiety/somatic problems class. Similarly, for drug craving, participants in the high psychopathology class again reported the highest levels relative to all other classes. Additionally, both the illness anxiety/somatic problems class and the moderate anxiety/depression class exhibited greater drug cravings compared to the low psychopathology class, though these 2 classes did not differ significantly from each other in drug cravings. These findings suggest that, as individuals experience more comorbid psychopathology, their risk for alcohol and drug craving increases. As such, the type of psychopathology may be less relevant to craving risk, except for alcohol craving, where individuals in the moderate anxiety/depression class reported significantly higher alcohol craving than those in the low psychopathology class, while the illness anxiety/somatic problems class did not significantly differ from the low psychopathology class. However, this finding should be interpreted cautiously, as the moderate anxiety/depression and illness anxiety/somatic problems classes did not significantly differ in their levels of alcohol craving.
Regarding treatment dropout AMA, individuals in the high psychopathology, illness anxiety/somatic problems, and moderate anxiety/depression classes were more likely to leave treatment AMA compared to those in the low psychopathology class. However, these 3 classes did not differ significantly in treatment dropout AMA from each other. This may reflect a potential threshold effect, such that individuals with moderate-to-high levels of comorbid psychopathology are at similarly elevated risk for treatment dropout AMA. Thus, the presence of comorbid psychopathology, regardless of the specific type or the amount, appears to contribute to challenges in treatment retention relative to those with minimal comorbid psychopathology. These findings align with prior research indicating that patients with dual diagnosis are generally at greater risk for treatment dropout. 32 Taken together with the findings on craving, these results suggest that, although craving severity may increase as the level of comorbid psychopathology increases, the risk for treatment dropout AMA remains comparable across all psychopathology classes. This finding underscores the potential importance of addressing any comorbid psychopathology in SUD treatment to improve treatment retention.
Clinical Implications
This study found that craving may be particularly prevalent among patients in residential SUD treatment who have multiple forms of psychopathology, highlighting the potential importance of incorporating mental health interventions into SUD treatment. Comorbid psychopathology may be directly related to substance use, as individuals may use substances to cope with psychological distress, 4 and substance use can exacerbate and maintain psychopathology over time. 33 Individuals who use substances to cope may lack adequate adaptive coping skills to manage distress and therefore may benefit from interventions that improve their emotion regulation and distress tolerance abilities. Further, treatment that directly targets craving during treatment may lead to reduction in substance use following treatment. 34 In accordance with study findings, individuals with more psychopathology may be particularly well-suited for interventions focused on reducing craving. Interventions historically effective in reducing cravings may include cognitive behavioral therapy, mindfulness-based approaches, and psychotropic medications tailored to the specific presenting concern (eg, brexpiprazole or lurasidone for schizophrenia).35 -37 Using a comprehensive, multi-method approach to treating comorbid mental health conditions may, in turn, enhance retention in residential SUD treatment.
Findings also highlight the potential need for psychopathology screening in residential SUD treatment settings to inform individualized treatment plans and improve retention. Standardized, one-size-fits-all interventions that focus primarily or solely on substance use reduction may not adequately address the needs of patients with comorbid psychopathology, which might contribute to elevated treatment dropout rates. Screening for psychopathology could help identify at-risk individuals and link them to tailored interventions that address the potential ways psychopathology contributes to their substance use. Early identification of at-risk individuals and the integration of transdiagnostic treatment approaches that target common features of psychopathology could enhance retention and outcomes for individuals with comorbid psychopathology, regardless of the specific form of psychopathology.
Limitations and Future Directions
The present study has several limitations that should be discussed. First, the use of dichotomous indicators to indicate whether an individual met the clinical threshold for a psychological disorder may overlook individuals who experience subthreshold symptoms that might still cause distress or functional impairment. Additionally, the study relied on the PDSQ, a measure based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria, which has since been updated in the DSM-5-TR. 38 The use of an outdated measure of psychopathology may limit the relevance and clinical applicability of the study’s findings. We attempted to remedy this by using modern names for a given psychological disorder; however, the PDSQ subscales may not directly map onto its modern conceptualization. Additionally, our measure of drug craving did not specify which drug(s) patients were craving, which is a significant limitation given that craving experiences likely vary by substance. Relatedly, we adapted the PACS measure to assess drug use craving in this study; however, this measure was not pilot tested prior to implementation. Future studies should conduct a psychometric investigation of this measure. Further, the sample was predominantly male and lacked sufficient representation of people with minoritized racial and ethnic identities, which likely limits the generalizability of the results to the broader population of individuals with SUDs.
The residential treatment center where this research was conducted is also unique in several ways, including its patient population consisting of largely professionals, its use of evidence-based interventions offered through both group and individual therapy, and its amenities such as access to a gym and chronic pain management. However, the incremental influence of these services and amenities on treatment retention is unclear. The typical treatment program typically lasts for approximately 30 days and adheres to a 12-Step, abstinence-based approach to SUD treatment. These characteristics may differ from those of many other residential treatment centers, which could also influence treatment retention and ultimately hinder the generalizability of the findings, especially to centers that follow a harm reduction model or those that have differing availability of resources and amenities. Additionally, because we used a convenience sample provided by the affiliated residential treatment center, our analyses were constrained. Consequently, we were unable to conduct an a priori power analysis to inform sample size determination, which could potentially limit the statistical power to detect certain effects. Finally, the latent class solutions in this study could have been influenced by reporting biases, such as overreporting distress or responding in socially desirable ways. For example, individuals in the high psychopathology class may be more likely to report cravings, while those in the low psychopathology class might underreport their cravings. Additional studies using similar methodologies are needed to confirm whether these latent classes replicate across samples and to explore how class membership relates to health and behavioral outcomes in this population. To enhance the applicability of these findings, future research should aim to replicate these findings using diverse, representative samples and updated, comprehensive measures of psychopathology in various treatment settings.
Conclusion
The present study identified latent classes of psychopathology among adults in residential SUD treatment and examined differences in craving and treatment dropout AMA across classes. We identified a 4-class solution and found that classes with more psychopathology reported more alcohol and drug cravings relative to classes with less psychopathology. Further, we found that rates of treatment dropout AMA were similar across all classes with psychopathology, regardless of the type or amount of psychopathology that comprised each class—all were at similarly higher risk of treatment dropout AMA relative to the class containing individuals with low psychopathology. Results highlight the potential importance of screening for psychopathology and linking patients with comorbid mental health problems to interventions, including psychotherapy and medication, to prevent craving and treatment dropout AMA. Future studies should examine the effects of screening and tailored interventions in residential SUD treatment centers on treatment retention and outcomes.
Footnotes
Author Contributions
Evan J. Basting led the project conceptualization, data analysis, and manuscript writing. He was responsible for formulating the primary research questions, conducting statistical analyses, and drafting and revising the manuscript.
Alyssa M. Medenblik, Alisa R. Garner, Samantha Schlachta, Ryan C. Shorey, and Gregory L. Stuart contributed to reviewing and editing the manuscript.
Gregory L. Stuart and Ryan C. Shorey also contributed to the conceptual development of the research questions.
Samantha Schlachta served as the clinical collaborator from the substance use treatment center where the study was conducted and provided critical support in facilitating the research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gregory Stuart conducts psychoeducational treatment groups for patients at Cornerstone of Recovery for a maximum of 3.5 hours per week. Dr. Stuart does not do any study recruitment, is not informed which patients do or do not participate in research, and does not mention anything about research to the patients attending groups. In addition, Gregory Stuart serves as the Editor in Chief of the journal.