
Abstract
Objective:
In 2020, approximately 1.7 million people were incarcerated in the United States, with nearly half of the general population being related to, or romantically involved with, an incarcerated individual. Over 70% of these incarcerated individuals met the criteria for a co-occurring mental health and substance use diagnoses. Individuals with co-occurring disorders often experience high rates of recidivism, which negatively impacts their non-incarcerated partners. This study aimed to examine the impact of incarcerated individuals with co-occurring ADHD and depression on their relationship quality, focusing on the roles of substance use, substance use treatment, and self-efficacy.
Methods:
The study analyzed the effects of substance use, substance use treatment, and self-efficacy on the relationship quality of couples where one partner was incarcerated and diagnosed with co-occurring ADHD and depression. The direct and indirect influences of these factors on relationship quality were assessed.
Results:
The findings indicated that higher levels of substance use and depressive symptoms, along with lower levels of self-efficacy and substance use treatment, were associated with lower relationship quality. ADHD indirectly affected relationship quality via substance use (β = −.015, 95% CI [−0.023, −0.008]) and self-efficacy (β = −.027, 95% CI [−0.039, −0.016]). Depression had both direct effects on relationship quality (β = −.180, 95% CI [−0.224, −0.138]) and indirect effects via substance use (β = −.023, 95% CI [−0.033, −0.015]), self-efficacy (β = −.040, 95% CI [−0.056, −0.025]), and through substance use and substance treatment (β = −.002, 95% CI [0.001, 0.005]).
Conclusion:
These findings highlight the need for further research to explore combined substance use and mental health treatment programs. Such interventions could potentially reduce recidivism rates, and promote the quality and maintenance of relationships among incarcerated individuals and their partners.
Introduction
The impact of co-occurring ADHD and depression on incarcerated men’s relationship quality: Mediating roles of substance use, self-efficacy, and substance treatment
Mass incarceration is a complex and systemic issue that has detrimental impacts on the incarcerated individual, their children, 1 siblings, 2 coparenting partners,3,4 and romantic partners.5 -8 To further compound the challenges with family dynamics, approximately 60% of individuals incarcerated are diagnosed with a mental health disorder, and roughly 50% of that same population have lived experience with substance use. 9 However, programs for federally incarcerated individuals, including drug education, non-residential programs, residential programs, and community transitional drug treatment, have decreased since 2019; 10 which has also been seen with state prisons. 11 Additionally, mental health programs are limited within prison contexts, which can further impact systemic areas outside of incarceration including employment, community, and parenting and relationship concerns.12,13 This study used a serial mediation analysis to examine the direct and indirect effects of ADHD and depression on incarcerated men’s relationship quality, and the impact on alcohol and drug related problems, self-efficacy, and substance use treatment.
Substance use and incarceration
Substance abuse is defined as the excessive misuse of psychoactive substances that creates social impairment, including failure to adhere to family or work commitments, and even the development of interpersonal frictions or legal predicaments. 14 Further, alcohol and drug (AOD) use is the pattern of drinking alcohol and using illegal substances, often resulting in physical, mental health, and social consequences. 15 Substance use is associated with various adverse outcomes, including substance relapse, violence, recidivism, and higher risk of mistreated co-occurring mental health and substance use disorders.9,16,17 Substance dependence is characterized by addiction’s behavioral and physiological symptoms, including the necessity for growing amounts of the substance to sustain craved effects, withdrawal from discontinued use, and dedicating large portions of time to obtaining or using substances.9,14
Individuals who experience incarceration are often engaged in high-risk behaviors and illegal activity that can be escalated with substance use.17,18 Approximately two-thirds of incarcerated populations qualify for a diagnosis of a substance use disorder, which is twelve times higher than the general population. 19 In fact, many formerly incarcerated individuals resume high levels of substance use post-incarceration, resulting in an increased chance of overdosing; which is roughly 17 times higher than the general population. 20 This may in part be due to decreased drug tolerance while incarcerated, and a lack of access to adequate substance use treatment upon release from prison. 12,13 Thus, suggesting the need for further examination of treatment of substance use disorder both during and post-incarceration, and the residual impacts it has on mental health outcomes and relationship quality.
Mental health disorders and incarceration
Individuals incarcerated in the U.S. are more likely to meet the criteria for the diagnosis of a mental health disorder, compared to the non-incarcerated general population.13,16 In fact, 64% of jail-incarcerated individuals in the United States reported having severe mental health disorders, including psychosis or major depression.9,20 Regarding mental health disorder diagnoses, about 21% of incarcerated individuals experience depression, while 10.5% experience attention-deficit hyperactivity disorder (ADHD). 21 Subsequently, several mental health disorders are correlated with substance use disorders, including attention deficits, traumatic stress, and depression; which may exacerbate symptomology due to the constant disruptions in the neurobiological circuits that regulate reward and distress, when using substances.16,17,20,22
Mental health disorders can be impacted by environmental and developmental factors.13,16,20 One risk factor worth noting is substance use among parents, where individuals may develop delinquent behaviors in childhood, which has been linked to incarcerated individuals’ history of substance exposure.9,14,16 Parental substance use can impact an individual’s development, environment, trauma development, socioeconomic status, and increase the likelihood of developing co-occurring disorders, which can be linked to later incarceration.16 -18,20,21 Experiencing trauma can impact an individual’s perception of their abilities to navigate and manage their responsese through self-regulation.13,22 These feelings of self-doubt perpetuate low self-efficacy, which can compound feelings of hopelessness, defeat, and lack of control, especially when coupled with the stress of incarceration. 23 Thus, when working with incarcerated populations, it is critical to be aware of the influence on co-occurring disorders and its subsequent impacts on self-efficacy.
Co-occurring disorders and incarceration
Approximately 72% of incarcerated populations have a co-occurring mental health and substance use diagnosis. 24 A report from the National Center on Addiction and Substance Abuse indicated that incarcerated individuals often experience drug-related charges, and the report highlighted substance use as being the most significant risk factor for severe mental illness.14,16 Conversely, about half of individuals with severe mental health disorders will likely develop a substance use disorder, which can lead to legal implications, including incarceration.13,14,17 Co-occurring disorders can increase the likelihood of violence and aggression with men, which can amplify rates of legal issues and incarceration. 25 One potential explanation for the severity of co-occurring disorders within the criminal justice system can be attributed to conditions of abuse, inadequate nourishment and activity, solitude, and overcrowding. 26 Thus, suggesting a vicious cycle of mental health disorders, substance use, and incarceration conditions
When looking at heterosexual couples, with incarcerated male patterns, women often experience significant impacts of co-occurring disorders and incarceration, especially if there is a history of abuse.9,16 Additionally, individuals who have experienced physical abuse, sexual assault, and other forms of domestic abuse, are at an increased risk of aggressive and suicidal behaviors.14,17 When examining the impacts of increased aggression with men experiencing co-occurring disorders and incarceration, 25 acknowledging the subsequent impacts on non-incarcerated female partners, such as through domestic violence, 17 can provide clarity on the needs of the relationship. Thus, this clarity enables establishment of appropriate and constructive support for couples that experience the triadic impacts of incarceration and co-occurring disorders.
Relationship quality in prison with co-occurring disorders
Relationship quality is described as how a couple perceives the overall state of their relationship, in regards to level of support, emotional and physical connections, and the ability to work together. 27 As previously noted, co-occurring disorders can increase the risk of aggressive behaviors, which can result in violent offenses among partners.17,28 In couples where there is a history of violence and controlling behaviors, there is an increased likelihood of intimate partner violence (IPV) for non-incarcerated female partners when their male partners are recently released from prison. 25 McKay et al further noted that couples who had stronger conflict management skills, in longer term relationships, and maintained healthy beliefs about relationship quality, had significantly lower rates of IPV. Therefore, the multifaceted legal, social, and personal issues that sprout from under-treated co-occurring disorders suggest the need for more effective research-based interventions in working with incarcerated populations, as well as stronger advocacy efforts to promote the implementation of more effective interventions.
Treatment outcomes
Incarcerated individuals with co-occurring mental health and substance use disorders often experience inadequate treatment outcomes, as the duality of substance use disorders and mental health disorders are treated separately.20,29 Further, there are also impacts of symptomatology on psychosocial physical functionality from co-occurring disorders that can increase the possibility of relapse.14,17,20 Additionally, incarcerated individuals with histories of substance use face several unique treatment barriers including limited treatment space, limited qualified professionals, and inadequate financial resources, that often create non-existent or ineffective treatment.13,16,28,30
As previously mentioned, treatment in the U.S. for co-occurring disorders often treats mental health and substance use disorders separately, with hopes of targeting the root problem to resolve the other disorder. 29 Since these disorders are often treated separately, treatment can be ineffective in addressing the entirety of the issue. According to Kubiak et al, 31 the best approach to treating both mental health disorders and substance use disorders is to treat them in tandem. Meaning, clinicians should be trained to work with both types of disorders to work with each psychological component of the individual.
However, many agencies and facilities, such as corrections, do not facilitate integrative treatment plans that address all aspects of concurrent disorders.9,18,31 When individuals with co-occurring disorders transition from a correctional facility to the community, they often experience inadequate treatment and limited skills to manage that transition, which can perpetuate risk of recidivism.9,13,28,32 Therefore, treatment approaches should aim to address all aspects of co-occurring disorders, while facilitating emotional and relational skills, to mitigate relationship distress during the transition from incarceration.
Literature-based conceptual integration
Attention Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder that progresses into adulthood, 33 and is characterized by inattention, hyperactivity, and/or impulsivity. 34 Approximately 2.5% of adults in the United States are diagnosed with ADHD.35,36 Adults with ADHD are at risk for comorbidity of mood disorders, depressive and anxiety disorders, and substance use disorders.35 -37 In fact, Lindquist et al (2018) Depressive Disorder (MDD) has a strong comorbidity rate with ADHD, which may be attributed to genetic and neurological factors, bullying, and challenges with executive functioning. 38 Further, individuals with ADHD may also experience low self-efficacy and self-esteem.33,37 This may be due to impairments with executive functioning tasks, 33 or even negative beliefs about one’s own competencies, based on past disappointments that reinforce these cognitive distortions. 37
In addition to comorbidities of depression and lowered self-efficacy, individuals with ADHD may experience issues with romantic relationships, and incarceration, due to challenges with impulsivity and poorer social functioning.36,39,40 In fact, individuals who have a significant other with ADHD perceive their partner less favorably, and report lower relationship quality overall. 40 This may be in part due to symptomology of inattention, impulsivity, sensitivity, reactivity, distraction, and forgetfulness that can lead to arguments, feelings of invalidation, and lack of balance of relational tasks. 39 Further, relational issues can be impacted by the incarceration of one’s significant other.17,25,27,28 Approximately, 26% to 30% of the adult prison populations meet the criteria for a diagnosis of ADHD, 36 suggesting the relevance and importance of examining the impacts of ADHD on incarcerated populations and their non-incarcerated romantic partners.
Current study
Previous studies showed a complex picture of substance use that requires further investigations into the tangible association of that factor and concurrent disorders, treatments, and health outcomes, such as relationship quality for incarcerated men having been in a romantic relationship. Therefore, in this study, we aimed to answer the research question: How are ADHD and depression in incarcerated men associated with their relationship quality directly and indirectly via their self-efficacy, substance/alcohol use, and treatment? Multiple parallel and serial mediation analyses were conducted to investigate the question (for conceptual and operative issues of mediation and serial mediation analyses, see Lemardelet and Caron42; MacKinnon et al. 42 ; Preacher and Hayes 43 ). Specifically, we hypothesized that ADHD and depression would show significant direct effects on relationship quality. Furthermore, we proposed that they would also significantly and indirectly influence the outcome via 3 mediators of AOD problems, self-efficacy, and AOD service (or treatment). In particular, we further examined 4 serial mediation models (ADHD → AOD problem → AOD service → relationship quality; ADHD → self-efficacy → AOD service → relationship quality; depression → AOD problem → AOD service → relationship quality; and depression → self-efficacy → AOD service → relationship quality). Please see Figure 1.
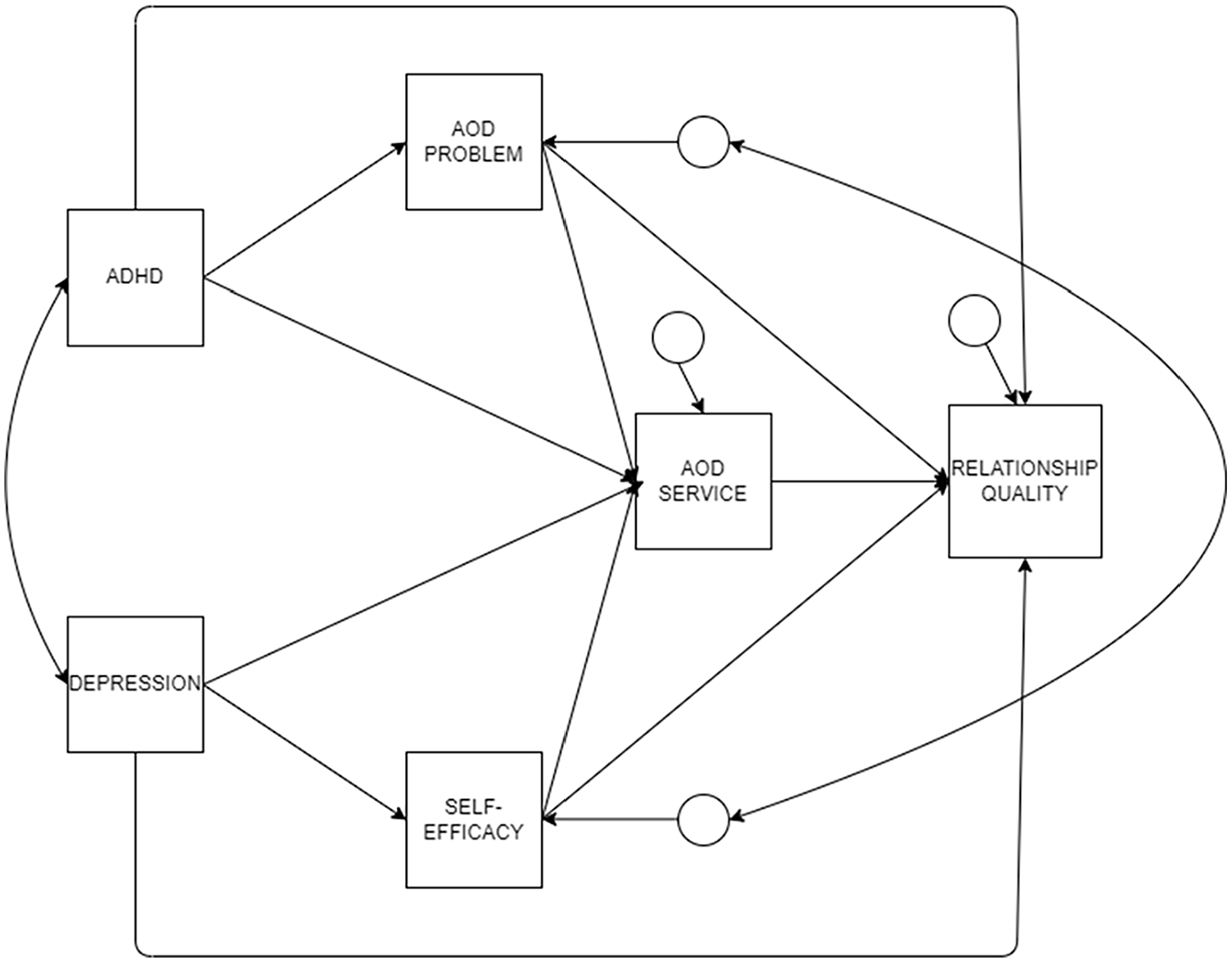
The hypothesized model.
Method
Data Source
The Multi-site Family Study on Incarceration, Parenting, and Partnering [MFS-IP] is a grant-funded dataset developed by the Office of Family Assistance within the U.S. Department of Health and Human Services, Administration for Children and Families. The MFS-IP is used to examine the validity of the program. The purpose of the program is to assist families in maintaining healthy relationships, while the father of the family is incarcerated. Criteria for this sample include all participants being age 18 or older and can speak English. The sample consists of women and their incarcerated coparenting counterparts from Indiana, Minnesota, Ohio, New Jersey, and New York. Same-sex dyads were not included in the original study and, thus, were not able to be included in this study. The incarcerated men from this sample were asked to identify their coparenting partner (who may also be, but do not have to be current romantic partners), as well as select their child who is closest to age 8 to be the “focal child” of the study. Only the men were incarcerated, and their coparenting female partners were not. The original researcher received informed consent and IRB approval. Many recent studies have explored incarcerated relationships with this dataset.3,4,6,8,25,44 -50
Interviews were conducted using audio computer-assisted self-interviews and computer-assisted personal interviews between December 2008 and August 2014. Several strategies were implemented to reduce common source bias, such as making clear interview instructions and using both positive and negative wording to prevent biases. Scales and items were organized in various forms to mask implied relationships between independent and dependent variables from respondents’ impressions. 51
Our study utilized this secondary dataset, the exemption received Institutional Review Board approval (IRB-FY2021-17). We estimated a necessary sample size using web-embedded software called “semPower 2,” found at https://sempower.shinyapps.io/sempower/. 52 In order to achieve a power of 95% to detect model misspecifications with 6 manifest variables, RMSEA = 0.05, α = .05, effect size = 0.05, and df = 4, a minimum sample size of 1859 participants is required. Our sample size satisfied the requirement as it yielded 1991 respondents. Demographic information of participants in this study is presented in Table 1.
Demographic characteristics (N = 1991 participants).

Measures
ADHD
A modified version of the Copeland Symptom Checklist for Attention Deficit Disorders was administered. 53 Participants were asked to use a 4-point Likert scale to respond to 3 statements reflecting distractibility and impulsivity (“You are easily distracted,” “You get frustrated easily,” and “You do not think before acting”) during the past month. Options range from 1-strongly agree to 4-strongly disagree. Items are re-coded to create a meaningful zero, and then scores are reversed before being summed to create a scale, where higher values imply greater distractibility and impulsivity. The checklist has been widely used in clinical settings to assess ADHD but has not been empirically validated. 54 Cronbach’s Alpha score is sufficient (α = .718).
Depression
It is measured using a 9-item version of the Center for Epidemiologic Studies Depression Scale. 55 The original measure contains 20 items and is popularly used to detect depression symptoms in different populations. The shortened instrument has also been commonly used in studies with justice-involved families. Scores on the 9-item measure can range from 0 to 27. A higher score indicates the person is encountering more depressive symptoms. CES-D demonstrated robust internal consistency and adequate validity (criterion, convergent, and discriminant) in previous studies across various sociocultural groups.56 -58 CES-D showed a reliable Cronbach’s Alpha score in this study (α = .747).
AOD problem
The variable is investigated using 7 items of the CAGE Adapted to Included Drug Use 59 and 3 other items examining respondents’ anger problem, violence problem, and drinking severity. CAGE-AID items are dichotomous; examples are “Did you ever have a drink first thing in the morning to steady your nerves or get rid of a hangover ("eye-opener")?” and “Did you ever feel bad or guilty about your drug use?” The others are Likert scales, ranging from 1-often to 4-never and 5-no AOD use. They are initially dichotomized; 1 and 2 are recoded to 1-yes, and 3-5 are recoded to 0-no. Eventually, ten items are summed (possible scores range from 0 to 10), and higher scores indicate greater troublesome AOD problems. CAGE and CAGE-AID have been commonly used as a screening tool for alcohol and substance use in different settings and have been found to have sufficient internal consistency as well as validity (factorial, convergent, and discriminant).60 -62 Cronbach’s Alpha is adequate for this study (α = .757).
Self-efficacy
A modified version of a 7-item instrument of mastery was administered. 63 Participants are asked how they agree or disagree with 3 statements. An item example is “Sometimes you feel like you’re being pushed around in your life.” Options range from 1-strongly disagree to 4-strongly disagree. Scores were recoded to create a meaning zero value and then summed. Higher scores imply greater levels of perceived self-efficacy. This measure has not been validated in previous studies. In this study, Cronbach’s Alpha is low (α = .519).
AOD service
The variable is operated using a dichotomous item, asking respondents whether they have received any interventions, such as counseling, self-help groups, group sessions, or other treatments, to help them manage alcohol or substance use problems during their incarceration.
Relationship quality
The dependent variable is measured with an abbreviated 8-item version of the original 32-item Dyadic Adjustment Scale (DAS).64,65 The modified DAS version was first generated and used in the “Québec Longitudinal Study of Child Development (QLSCD 1998-2002)” study. 64 While it can detect marriage-related distress and satisfaction, its measurements are similar to the 32-item version. Still, its shorter form allows it to be conveniently immersed in longer questionnaires. Seven of them are 4-point Likert items, ranging from 1-often to 4-never. The other is a 10-point Likert item, asking respondents about their relationship happiness: “On a scale from 1 to 10 where 1 means not at all happy and 10 means perfectly happy, which number best describes your happiness with your relationship now?” The items are rescaled to create a meaningful zero score (eg, 1-4 to 0-3). The happiness item is further scaled to comprise 19% of the total score. Finally, they are summed, and a higher score reflects a greater level of relationship quality. Sufficient internal consistency and validity (factorial, convergent, and discriminant) for the scale were demonstrated.66,67 In this study, the measure displayed a robust Cronbach’s Alpha score (α = .825).
Analytic strategy
Preliminary statistics, such as descriptive statistics and bivariate correlations, are explored in SPSS version 25, using the mean-imputed dataset published by the original research team. If absolute skewness and kurtosis values are smaller than 2 and 7, respectively, a relatively normal distribution of data is considered. 68 Data are free of multicollinearity problems if bidirectional correlation coefficients among variables are lower than .800. 69
Subsequently, path analysis and indirect effects are administered using Mplus version 8.8. 70 Maximum likelihood (ML) estimation is used to account for data missingness and estimate model fitness of the hypothesized model. 71 A combination of 5 fit indices is chosen to test model fitness to the observed data: a nonsignificant standard chi-square index (χ2), root mean square errors of approximation (RMSEA) < .06 with 90% confidence intervals (CI), standardized root mean squared residual (SRMR) < .06, comparative fit index (CFI) > .95, and Tucker-Lewis Index (TLI) > 95.72,73
As the hypothesized model is saturated, a chi-square different test is implemented to find a more parsimonious model that still fits the observed data. 74 In particular, nonsignificant parameters are sequentially fixed to 0, starting from the one having the smallest b value. If the chi-square values of nested models are smaller than the cut-off chi-square values at their degree of freedom and P-value of .05, those models are considered significant and parsimonious. A model with better-fit indices and more degrees of freedom among the significant models will be considered the most parsimonious one.
Bias-corrected bootstrapping with 95% CI and 10 000 iterations is used to estimate more accurate indirect effects.42,43 If a confidence interval does not contain a zero score, it signals the significance of an indirect effect.
Results
Descriptive statistics of studied variables and their bivariate correlation coefficients are presented in Table 2. In particular, they are normally distributed, as no absolute skewness and kurtosis values are larger than the criteria. 68 All correlation coefficients are not beyond the cutoff of .800 to warn of multicollinearity. Therefore, conditions are justified to test the hypothesized model.
Mean, standard deviation, and correlations for study variables (N = 1991).

Abbreviations: M, mean; SD, standard deviation.
**P < .05.
The hypothesized model is saturated with zero degrees of freedom; thus, it yielded perfect model fit indices (χ2 (0) = .000 (P = .000), RMSEA = .000 90% CI (0.000, 0.000), SRMR = .000, CFI = 1.000, TLI = 1.000). Results show that ADHD is significantly and positively associated with depression among respondents (r = .498, P < .001). Among the studied variables, the path coefficients between ADHD and relationship quality, as well as ADHD, depression, and self-efficacy, respectively, and AOD service are insignificant. Therefore, they will be sequentially constrained to zero, starting from the smallest insignificant coefficient between self-efficacy and AOD service (b = .006, P = .801) to the highest insignificant one between ADHD and relationship quality (b = .041, P = .154). Please see Figure 2.

The saturated model.
A nested model in which all insignificant path coefficients are constrained to zero yielded 4 degrees of freedom and the best model fit, in comparison with other nested models. Its model fit is as follows: χ2 (4) = 7.463 (P = .113), RMSEA = .021 90% CI (0.000, 0.044), SRMR = 0.014, CFI = .997, TLI = .989. Results do not show considerable changes regarding path coefficients among the variables, except for a reduced (standardized) effect of AOD problems on AOD service compared to their value in the saturated model (β = .292, P < .001; reduced from β = .303, P < .001). The model significantly accounted for 10% of the variance in relationship quality, 9% of the variance in AOD service, 25% of the variance in self-efficacy, and 6% of the variance in AOD problem (P < .001).
Furthermore, relationship quality could be significantly predicted by depression, AOD problems, self-efficacy, and AOD service. However, it cannot be statistically significantly predicted by ADHD, as the p-value is high and the 95% CI contains zero value. When the mediators are placed into the model, ADHD’s total indirect effects and depression’s direct and total indirect effects on relationship quality are significant. In particular, it shows that all indirect pathways from ADHD to relationship quality, except for the one from ADHD → AOD problems → AOD service → relationship quality, are significant as their 95% CIs do not contain zero value. In other words, ADHD exaggerates AOD problems, while simultaneously reducing self-efficacy. Thus, increasing AOD problems and decreasing self-efficacy will weaken relationship quality.
On the other hand, all indirect pathways from depression to relationship quality, including the serial indirect one from depression → AOD problems → AOD service → relationship quality, are significant. In other words, depression simultaneously impacts relationship quality directly and indirectly. The direct relationship is that depression reduces relationship quality. The indirect effect is that depression exasperates AOD problems and minimizes self-efficacy, thus depleting relationship quality.
Depression is significantly related to a higher score on AOD problems. Subsequently, AOD problems were positively associated with AOD service, and that is a significant predictor of higher relationship quality (see Table 3 and Figure 3). In other words, receiving AOD services can attenuate the negative indirect influence of depression on relationship quality via AOD problems.
Indirect effects of ADHD and depression on relationship quality through AOD problem, self-efficacy, and AOD service.
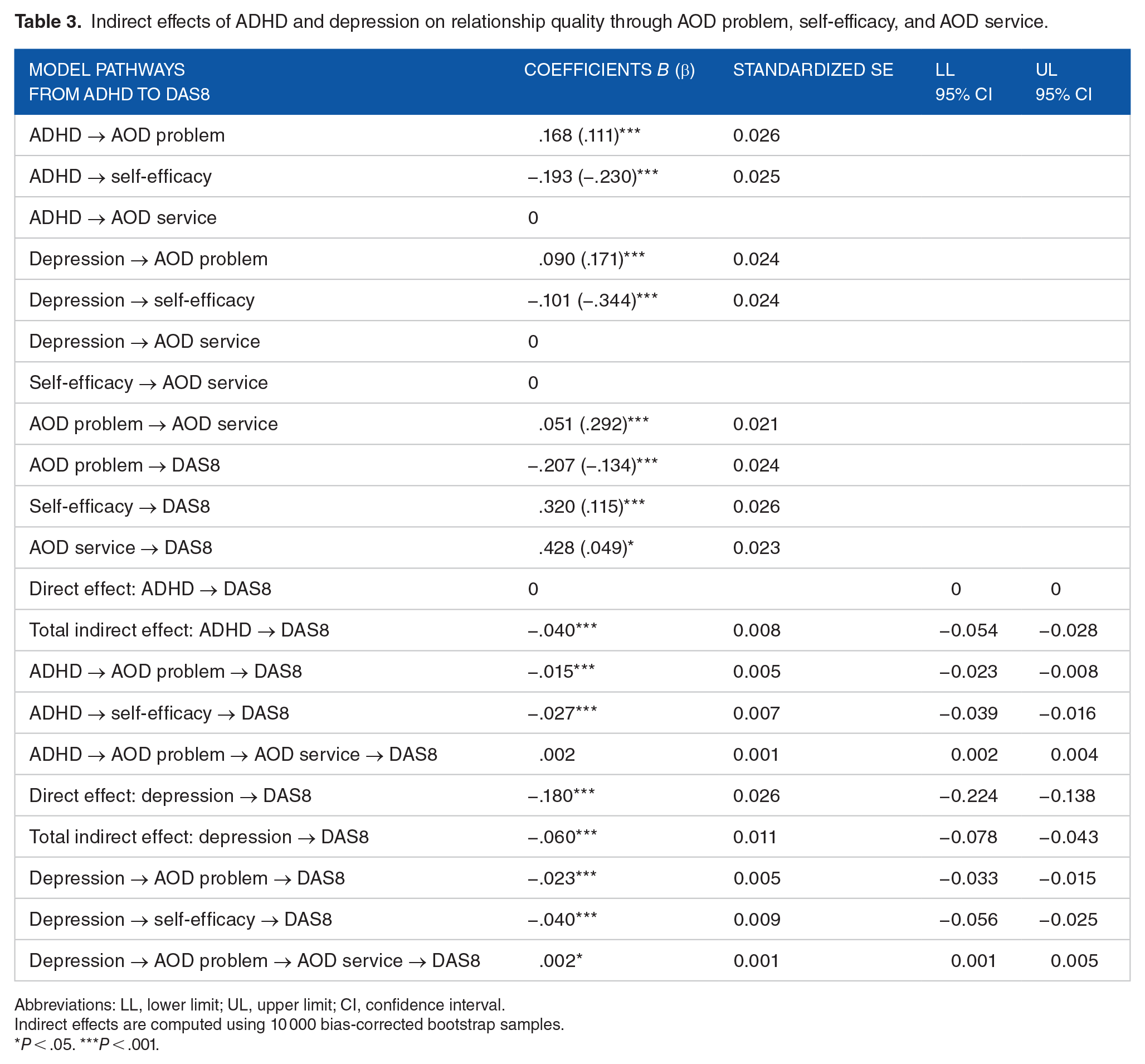
Abbreviations: LL, lower limit; UL, upper limit; CI, confidence interval.
Indirect effects are computed using 10 000 bias-corrected bootstrap samples.
P < .05. ***P < .001.

The final model.
Discussion
The current study examined the impacts of incarcerated individuals with co-occurring disorders on their treatment outcomes and couple relationship quality. The findings yielded various outcomes. Regarding pathways from ADHD to relationship quality, only certain indirect effects of ADHD on relationship are significant. In particular, when incarcerated men experienced higher rates of ADHD symptomatology, symptoms of substance use disorders also increased, while perceived self-efficacy decreased; an increase in substance/alcohol use and a reduction in self-efficacy then negatively relate to relationship quality. A serial pathway from ADHD to AOD use to AOD service to relationship quality, however, was not significant. There are several explanations for the above findings. ADHD is often treated with stimulants, but individuals may turn to nonmedical stimulants, such as methamphetamine, to manage their symptoms if they are unable to access prescriptions. 18 Thus, if incarcerated men in this study did not receive treatment for ADHD, that might exacerbate their substance and alcohol use.
In terms of pathways from depression to relationship quality, depression was directly and indirectly significantly associated with relationship quality. Among the indirect associations, similar to ADHD, depression exaggerated AOD problems while attenuating self-efficacy. An exaggeration of AOD problems and an attenuation of self-efficacy then led to a decrease in relationship quality. Unlike ADHD, the serial pathway from depression to AOD problems to AOD service to relationship quality was significant. In other words, the more severe the depression is, the mores severity of AOD problems. Subsequently, when AOD problems are heightened, the engagement in AOD service is also greater. That eventually leads to higher relationship quality.
Clinical implications
Incarcerated individuals in the U.S. with co-occurring issues of mental health issues and substance use disorder are typically underserved within the justice system. In fact, only 11% to 28% of incarcerated individuals receive sufficient substance use treatment.14,20 Incorporating mental health, substance abuse, or integrated treatment programs has been difficult to establish for transient jail populations due to their short length of stay. Thus, limiting the likelihood of incarcerated individuals participating in beneficial programs. Incarcerated individuals who do seek substance use services engage in self-help groups or peer counseling such as Narcotics Anonymous or Alcoholics Anonymous or through detoxification. 14
In terms of effective treatment approaches, it has been found that self-motivation has been classified as the most decisive factor in deterring recidivism, paired with family support as an origin of support. 75 In fact, when couples with an incarcerated partner are able to build their communication skills, relationship quality and maintenance increase, while simultaneously decreasing recidivism rates. 44 Further, motivational interviewing is highly effective and has shown reduced substance use, compared to those who did not receive this treatment, and when implemented early on in treatment.76,77
Limitations and future directions
There are several limitations of the current study. The data utilized in this study [MFS-IP] does not support generalization and does not represent the national population. Data does not include same-sex couples or incarcerated women who have a nonincarcerated partner as the data from the MFS-IP only addressed the relationships of incarcerated men and nonincarcerated women. Some measures were not piloted and did not show sufficient internal consistency (eg, self-efficacy), possibly indicating measurement errors in measure variance. 78 It might result from a low number of indicators, respondent inconsistency, poor test conditions, and a lack of measure one-dimensionality. Future investigators should look for more reliable inventories to assess self-efficacy. In addition, this study is exploratory in nature, so its; findings should be carefully interpreted. Nevertheless, precautions were taken to minimize type I and type II errors. In particular, an SEM power analysis was conducted, preceding the major statistical analysis. To prevent type I errors, the significance level was established at 95% (α = .05). The effect size in was also set at the medium level of .5 to reduce type II errors.
Other researchers can replicate the final path model in this study with other populations and different sociocultural contexts to verify its credibility and validation. Future research should look to bridge the gap in the literature regarding incarceration studies with a focus on female-incarcerated partners, exploration of LGBTQ+ dyads, and diverse family structures. With regard to substance use, future studies can explore the impact of supportive skills on recidivism and substance use rates. 44 Understanding the social connections of building supportive communication can be impactful in the treatment of co-occurring disorders while incarcerated. Additional research can also investigate the need for combined substance use and mental health treatment programs within the prison system to address the diverse needs of healthcare and post-incarceration maintenance. 20
Conclusion
This study investigated the simultaneous impacts of co-occurring ADHD and depression on relationship quality via multiple mediators of substance use, substance use treatment, and self-efficacy in a sample of incarcerated men. Preliminary findings indicated several different pathways through which ADHD and depression could impact the outcome. ADHD only showed negative impacts on relationship quality through increasing participants’ substance use and lowering their self-efficacy. Besides its direct effect, depression also deteriorated relationship quality in similar indirect ways to ADHD. A significant serial pathway was found when depression heightened the men’s use of substances, their engagement in substance use treatment increased, which eventually improved their relationship quality. Further investigations are required to explore effective programs to mitigate substance use and promote self-efficacy, as well as substance use treatment to promote relationship quality.
Supplemental Material
sj-doc-1-sat-10.1177_29768357241284097 – Supplemental material for The Impact of Relationship Quality on Couples With an Incarcerated Partner With Co-Occurring Mental Health and Substance Use Issues
Supplemental material, sj-doc-1-sat-10.1177_29768357241284097 for The Impact of Relationship Quality on Couples With an Incarcerated Partner With Co-Occurring Mental Health and Substance Use Issues by Eman Tadros, Anh-Khoi Nguyen Le and Alexis Gregorash in Substance Use: Research and Treatment
Supplemental Material
sj-docx-1-sat-10.1177_29768357241284097 – Supplemental material for The Impact of Relationship Quality on Couples With an Incarcerated Partner With Co-Occurring Mental Health and Substance Use Issues
Supplemental material, sj-docx-1-sat-10.1177_29768357241284097 for The Impact of Relationship Quality on Couples With an Incarcerated Partner With Co-Occurring Mental Health and Substance Use Issues by Eman Tadros, Anh-Khoi Nguyen Le and Alexis Gregorash in Substance Use: Research and Treatment
Footnotes
Acknowledgements
n/a
Author Contributions
Eman Tadros—The lead author on the paper. Conceptualization, oversaw the entire project and ensured completion. Participated in writing the initial draft, revisions, and final edits. Selected the data, formulated the research question, research design, and associated measures. Responsible for correspondence with the journal during submission and peer review.
Khoi Nguyen Anh Le—The second author. Participated in writing the initial draft, revisions, and final edits. Took the lead in data analysis and results, and created the tables and figures.
Alexis Gregorash—The third author. Participated in writing the initial draft, revisions, and final edits. Assisted with the literature review and implications.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
All ethical standards were followed and complied with. All ethical guidelines and procedures have been followed. This study was exempt by the Institutional Review Board for usage of secondary data.
Informed Consent/ Patient Consent
This study was exempt by the Institutional Review Board for usage of secondary data.
Grant Number
n/a
Trial Registration Number/Date
n/a
Data Availability Statement
The data is publicly available through ICPSR.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.