
Abstract
Background:
Designing effective health campaigns requires a thorough understanding of the intended audience. For stigmatized health issues like substance use disorder and mental health disorders, campaigns must be strategic, culturally competent, and evidence based. This manuscript details the process of creating a comprehensive statewide health campaign focused on mental health awareness and substance use prevention in Texas.
Methods:
This study employs a multifaceted data collection approach. It includes a review of relevant health communication literature and an environmental scan to evaluate existing substance use and mental health campaigns. Two statewide online surveys were conducted with representative samples of Texans (N = 1028; N = 2033) to gauge views on substance use, mental health, risk perceptions, stigma, social connectedness, and prevention and treatment strategies. Additionally, 35 in-depth interviews were conducted with community leaders across Texas (eg, coalition managers, non-profit leaders, healthcare professionals), who then participated in 2 rounds of focus groups to provide feedback on research results.
Results:
This paper demonstrates how a focus on evidence-based health communication can support a statewide public health campaign. Key insights from multiple rounds of formative research include, but are not limited to, the rise of substance use and mental health issues across Texas following COVID-19, the positive impact of social connection, and the need for substance use and mental health education. The interviews and focus groups with community leaders revealed valuable feedback on proposed campaign messages and their potential impact, leading to refinements based on their input.
Conclusion:
The findings outline a multi-step, multi-method approach centered on the key elements of health campaign design—an environmental scan, extensive literature reviews, 2 statewide surveys, and interviews and focus groups with community leaders. This process culminates in a creative brief and comprehensive campaign, providing a framework for future researchers to design evidence-based health campaigns.
Highlights
Substance use disorder (SUD) and mental distress surged among Texans and the broader population, highlighting the urgent need for effective health communication interventions to promote individuals’ well-being.
This project bridges the gap between existing literature on mental health and SUD with its practical application in public health, thereby offering a novel perspective for addressing these critical issues.
This project uses a comprehensive data collection strategy, incorporating an academic literature review, environmental scan, 2 statewide online surveys, in-depth interviews, and focus groups across the state of Texas to develop a health communication campaign addressing the mental health and substance use impacts of the COVID-19 pandemic.
This research offers valuable insights into the development and design of a comprehensive public health campaign, providing a blueprint for future researchers to create evidence-based campaigns.
Introduction
Substance use disorder (SUD) remains a critical public health issue, affecting an estimated 40.3 million people aged 12 or older in the US in 2020. 1 The COVID-19 pandemic exacerbated this crisis, contributing to a record-breaking 107 622 overdose deaths in 2021, a record high and nearly 15% increase over the prior year. 2 Evidence from a systematic review indicated that COVID-19 lockdowns corresponded with a 23% increase in alcohol misuse and 31% increase in recreational drug use. 3
This surge coincided with a global decline in mental health, with depression and anxiety increasing by 25% between April 2020-February 2021. 4 Pandemic-related stressors, including social isolation, financial insecurity, disrupted routines, and reduced healthcare access intensified mental health burdens and compounded the SUD crisis. 5 National data indicate that approximately 13% to 18.2% of adults reported initiating or increasing substance use to cope with stress during the pandemic.1,6
These alarming patterns have disproportionately affected certain populations, including racial and ethnic minority groups, young adults (ages 18 to up to 35 years), essential workers, and individuals with preexisting chronic conditions.5-7 Black and Hispanic adults in particular experienced significantly higher rates of depression and anxiety than White adults, 7 driven by greater exposure to pandemic-related stressors such as higher COVID-19 infection rates, food and housing insecurity, and job loss.6,8 As mental health demands increased, longstanding gaps in behavioral health care became more pronounced. Factors such as medical distrust, discrimination, and declining confidence in public health guidance hindered access to and utilization of both mental health and SUD services, leaving many people at heightened risk.9,10 A 2020 survey of US adults found that 10.7% had seriously considered suicide in the previous 30 days, with rates significantly higher among Latinx adults (18.6%), unpaid caregivers (30.7%), and essential workers (21.7%). 5 Additionally, 13.3% of respondents reported starting or increasing substance use to cope with pandemic-related stress, with the highest rates among young adults, racial/ethnic minorities, and essential workers. 5 Although the national public health emergency has ended, the mental health and substance use challenges it intensified continue to persist, warranting sustained, integrated responses that address both issues concurrently. 7
Various approaches—harm reduction, overdose prevention, community-based programs—have been implemented nationwide to address SUD, but important gaps remain. A 2025 World Health Organization call-to-action urges public health campaigns to prioritize upstream approaches, including efforts to strengthen social connections, and highlights the need for stronger evidence-based strategies to advance population well-being. 11 Distrust of state and public health information, particularly amid growing skepticism towards medical systems, however, continues to limit the reach of interventions.9,10 Nonetheless, health communication can still make a meaningful impact. The aftermath of COVID-19 offers a unique opportunity to rebuild trust in health information and strengthen connections for vulnerable populations to mitigate daily stress that often leads to SUD—a primary goal of this campaign. Accordingly, the purpose of this paper is to describe the development of an evidence-based, statewide behavioral health communication campaign, Turn To, led by the Center for Health Communication (CHC) at the University of Texas at Austin and funded by the Texas Health and Human Services Commission (HHSC). The campaign aimed to reduce rising SUD rates by promoting connection and adaptive coping, with outreach strategically concentrated in counties and communities most affected by the pandemic, as prioritized by the HHSC.
Texas is a well-suited site for this campaign. As the second most populous and 1 of the most racially and ethnically diverse states in the US, it reflects national behavioral health challenges while introducing distinct local complexities. Between 2020 and 2021, drug overdose deaths in Texas rose by 37%, with opioids responsible for more than half. In 2022, 34.2% of Texas adults reported symptoms of anxiety or depression—surpassing the national average of 31.6%—yet only 30% received counseling or therapy. 12
Principles of Health Communication Campaign Design
The process for designing and executing a health communication campaign, as outlined in the National Cancer Institute’s (NCI) “Pink Book,” 13 involves several key stages: planning, designing and testing, implementation, and evaluation. In the planning stage, developers define the problem, set objectives, understand the audience, consider dissemination methods, and create communication plans. Designing and testing include studying previous campaigns, testing ideas, selecting materials, and developing and testing messages. Implementation encompasses the campaign launch, media exposure, and ongoing monitoring and evaluation.
Mackert 14 introduced an adjacent process called account planning, which combines advertising concepts with evidence-based approaches. This process prioritizes the audience’s perspective by developing a creative brief (a summary of findings to guide the creative team’s work) based on research, audience insights, and a dynamic campaign strategy. Unlike the NCI process, account planning strongly emphasizes making the campaign approachable and enjoyable for the audience. It emphasizes the interconnectedness of research, audience engagement, input, design, and implementation, ensuring that these elements work together at every step to create a meaningful and effective campaign.
Center for Health Communication
The CHC is a joint academic center supported by Dell Medical School and Moody College of Communication at the University of Texas at Austin. It focuses on evidence-based health communication across research, education, and practice, advancing the evidence base of health communication and translating it into effective public health campaigns. The remainder of this paper details the elements and processes employed by the CHC to develop what is currently 1 of the most extensive behavioral health campaigns supported in Texas, focused on SUD prevention and mental health awareness. It describes the campaign’s development, key research findings, and lessons learned to inform and support the replication of similar behavioral health efforts in Texas and in other states.
Formative Research
A mixed-method formative research process was conducted between 2021 to 2022 to inform campaign goals, messaging, and creative design. Guided by best practices in health communication campaign design, we triangulated insights from qualitative and quantitative methods, including an academic literature review, environmental scan, 2 statewide online surveys, and interviews and focus groups with community leaders across Texas.15,16 Procedures were developed by a multidisciplinary team of health communication and health promotion scholars and practitioners, in consultation with HHSC and with the approval from the University of Texas at Austin’s Institutional Review Board (IRB). Figure 1 depicts an overview of the campaign development timeline.
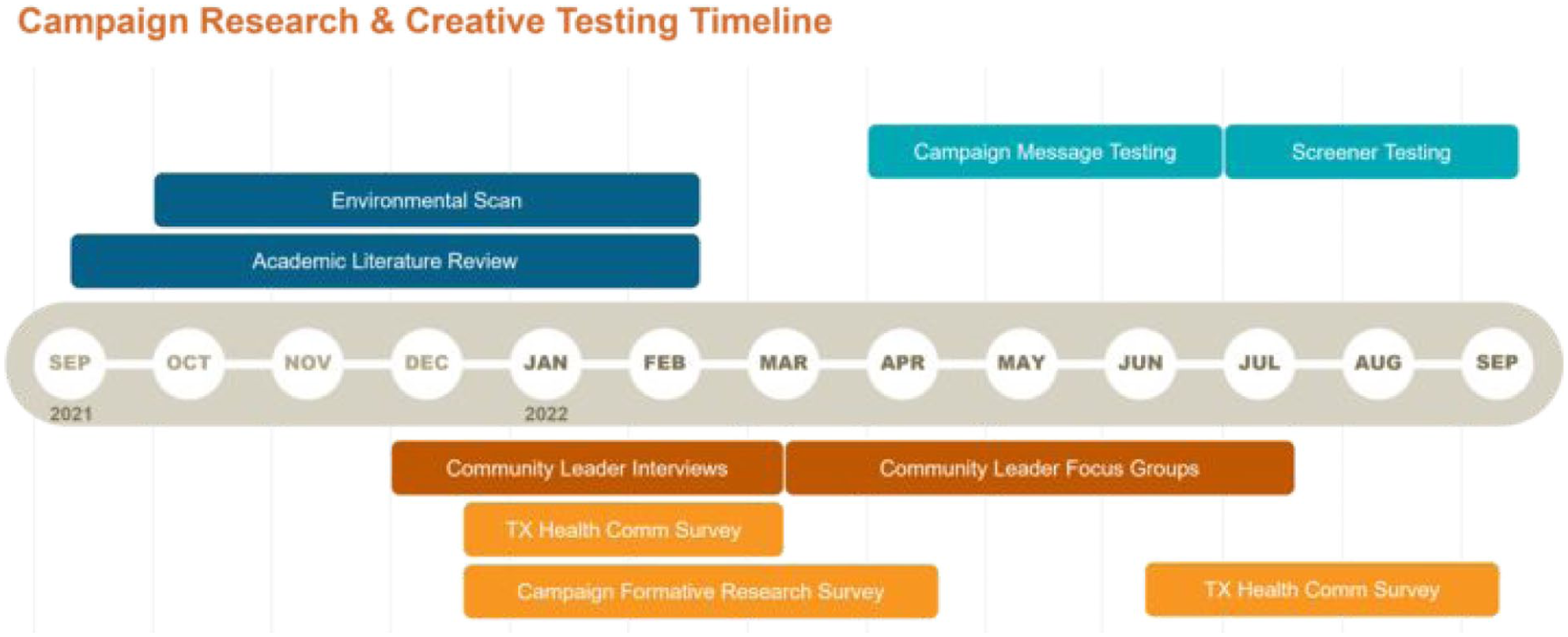
Campaign research & creative testing timeline.
Academic Literature Review
The first step in the formative research process was to conduct an academic literature review to better understand the intended audience, inform data collection, and potential messaging strategies. The research team systematically searched databases (eg, PubMed) using relevant keywords such as “rural-urban health disparities,” “trauma-informed care,” “social connection and health outcomes,” “adaptive and maladaptive coping,” and “mental-behavioral health and COVID-19.” Articles were assessed for relevance, methodological rigor, and recency.
Several important findings emerged from the review. Pandemic-era research documented sharp declines in social connectedness and rising loneliness—both established risk factors for distress and substance misuse. 17 Extensive evidence links strong support from social networks to higher post-traumatic growth following highly stressful events, 18 more positive attitudes toward seeking help for mental health concerns, 19 and improved overall physical health.20,21 In risk and crisis communication research, strong connections with partners, family members, and friends are consistently shown to mitigate distress and enhance resilience. 22 These insights led our team to position social reintegration and connection as central themes in our campaign approach.
Our approach was further informed by the Transactional Model of Stress and Coping, 23 which posits that coping responses are shaped by individuals’ appraisal of stressors and their perceived availability of coping resources. For example, when stressors are appraised as uncontrollable and resources are perceived as limited, people are more likely to engage in emotion-focused coping strategies (eg, substance use). Social connectedness serves as a critical coping resource and well-established protective factor, facilitating more adaptive responses to stress.21,24 Therefore, the campaign strategy prioritized messaging that was authentic, accessible, and centered on support, with the aim of promoting healthier coping pathways and reducing SUD risk.
One-page briefs were developed for each topic of interest to translate key findings into clear, actionable takeaways for the research team, creatives, and media partners. These one-pagers help ensure that the campaign’s objectives are grounded in evidence-based, audience-relevant messaging.
Environmental Scan
Next, both the research and creative teams conducted an environmental scan of existing campaigns and web-based resources to identify trends, best practices, and gaps to inform new interventions. Findings were organized by focus areas such as SUD-focused campaigns, digital self-screening tools, and mental health promotion initiatives. We incorporated valuable strategies from these efforts, including interactive tools, nonjudgmental and accessible language, and resource-oriented messaging. Notable examples include the Centers for Disease Control and Prevention’s How Right Now, 25 which used culturally responsive design to promote emotional well-being by helping users identify their feelings and provided tailored resources through interactive tools; the Ad Council’s Seize the Awkward, 26 which encouraged young adults to recognize when a friend may be struggling and offered conversation starters to facilitate mental health conversations; and the Mental Health Test, 27 a brief online screening tool designed to connect users to appropriate care.
Notably, few campaigns explicitly addressed the intersection of stress, coping mechanisms, and substance use, which is an important gap our campaign sought to address. Leveraging these insights, the CHC aimed to develop a campaign that would tackle the multifaceted impacts of COVID-19 in a grounded manner, prioritize interactivity and personalization in the screener tool design and recognize the diversity of the Texas population.
Two Statewide Surveys
Two cross-sectional online surveys were conducted with representative samples of Texas residents to assess various domains related to SUD and mental health. Participants were eligible if they were 18 years or older and lived in Texas. All study procedures were approved by the authors’ university IRB.
Pilot Survey
A web-based pilot survey was administered through Qualtrics from January to February 2022 to gather baseline descriptive data and guide message development. A sample of Texas residents, intended to reflect U.S. Census Bureau data on age, gender, and race/ethnicity, was recruited and compensated through the Qualtrics panel, a widely used online recruitment tool with a diverse pool of registered participants. The survey, administered via Qualtrics took participants an average of 10 minutes to complete. In addition to demographics, the survey measured perceptions of social connection, trust in health information sources, and perceived reasons for substance use.
Qualtrics recorded 1046 responses, of which 18 responses were removed due to duplicate IP addresses or extreme survey duration. As a result, the final sample in this survey included 1028 Texans aged 18 to 92 (M = 45.2, Standard deviation [SD] = 17.7). Over half of the respondents were male (n = 520, 50.6%), and 501 (n = 48.7%) were female. Nearly 40% of participants reported Hispanic or Latin origins (n = 408, 39.7%). Among the non-Hispanic participants, the majority self-identified as White (n = 426, 41.4%), followed by African American or Black (n = 129, 12.5%), Asian (n = 25, 2.4%), and American Indian or Alaska Native (n = 11, 1.1%). Over a quarter of the participants received a Bachelor’s degree or higher (n = 286, 27.8%).
Findings from the pilot survey indicated that: (1) across all health topics (eg, SUD, COVID-19, mental health), doctors or healthcare providers were the most trusted information source, followed by the Texas Department of State Health Services; (2) participants reported being somewhat lonely since the pandemic, and believed they had social support to some extent; and (3) on average, they perceived that others consume alcohol primarily to feel good, relax, and to forget worries, while using substances to reduce medication side effects was rated lowest. Baseline data showing changes in social connection alongside alcohol use to cope with stress justified proceeding with a more comprehensive survey to advance the campaign’s goals of promoting healthy coping and connection.
Formative Survey
The second, more comprehensive online survey was conducted from February to March 2022. The survey research firm, Centiment, managed the survey administration and recruited a sample of adult Texans; age, gender, and race/ethnicity were representative of demographic strata according to U.S. Census Bureau data. Those who reported a non-Texas zip code, failed an attention check, or were identified as potential bots were excluded. The survey took approximately 20 to 25 minutes for participants to complete.
The final sample included N = 2033 respondents ranging in age from 18 to 90 years old (M = 42.8, SD = 17.7). Over half of the respondents were female (n = 1027; 50.5%). About one-third self-identified as non-Hispanic White (n = 675; 33.2%), 14.9% as non-Hispanic Black (n = 303), and 46.6% as Hispanic/Latino (n = 947). A detailed summary of participant demographics for the formative survey is presented in Table 1.
Formative Survey Sample Demographics.
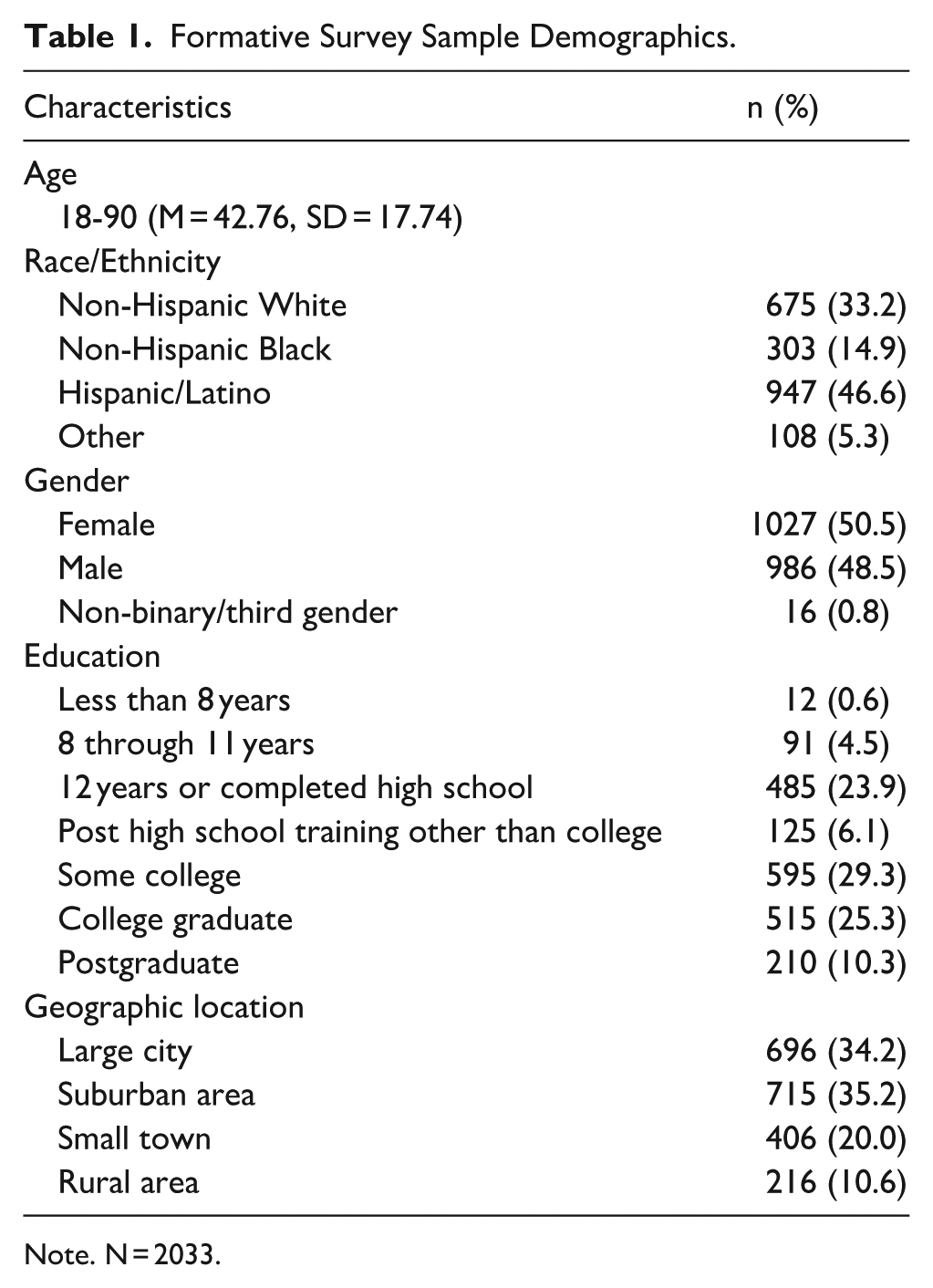
Note. N = 2033.
The survey assessed participants’ knowledge, attitudes, and beliefs related to substance use, mental health, and potential prevention strategies. Key domains included stigma, self-reported mental health, perceived risk, social connectedness, coping beliefs, and help-seeking behaviors. Additional measures included reasoned action variables related 4 target behaviors related to seeking or initiating conversations about mental health and substance use. Respondents also rated the persuasiveness of potential campaign messages. Table 2 presents descriptive statistics for selected questionnaire items, while bivariate correlations among selected variables are displayed in Table 3. Additional example items and results are available in previously published articles,28,29 and the full questionnaire is available from the authors upon request.
Means and Standard Deviations for Key Variable Items.
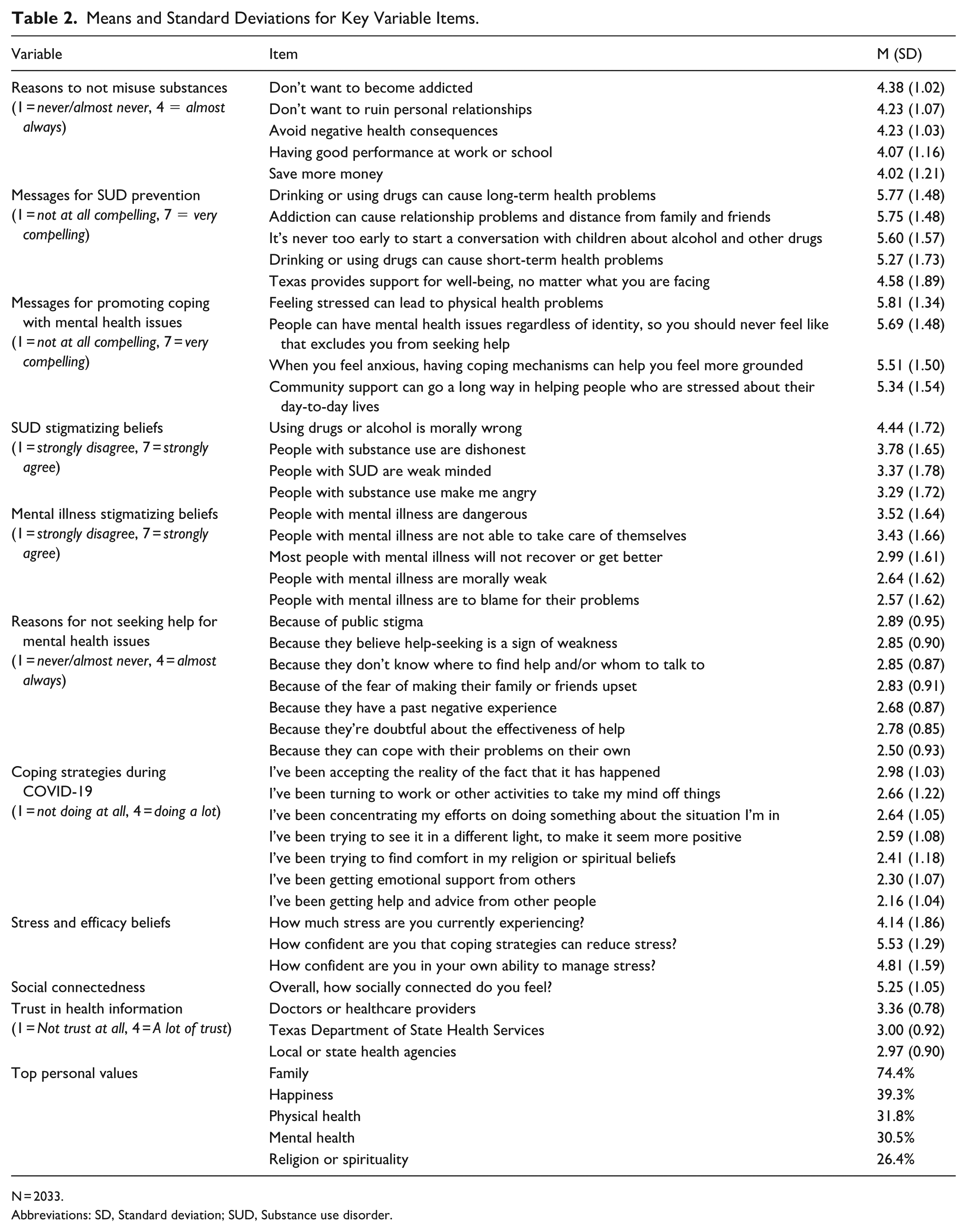
N = 2033.
Abbreviations: SD, Standard deviation; SUD, Substance use disorder.
Bivariate Correlations (Pearson’s r) Among Selected Variables.
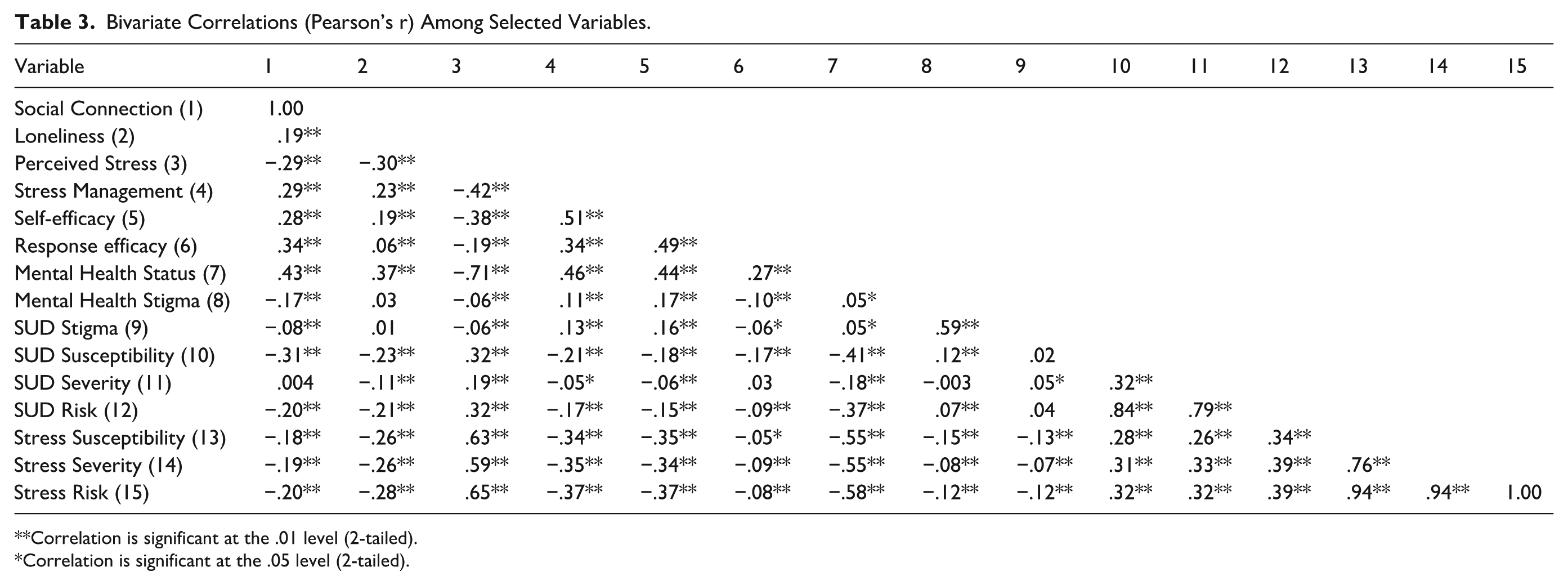
Correlation is significant at the .01 level (2-tailed).
Correlation is significant at the .05 level (2-tailed).
Formative Survey Results
Findings revealed that Texans highly value family, happiness, physical and mental health, and rated all proposed SUD prevention messages as compelling. The most persuasive messages emphasized consequences such as addiction, harm to relationships, and long-term health impacts. Participants also agreed substance use is often emotionally driven (eg, to relax or forget worries), suggesting effective when they acknowledge emotional motivations, promote healthier coping alternatives, and emphasize protecting relationships and health.
Although participants reported few personal stigmatizing beliefs toward people with mental illness and SUD, they identified public stigma as the most common barrier to seeking help. This distinction aligns with prior research showing that perceived public stigma (ie, concern about how others might judge or discriminate) can deter help-seeking even when individuals themselves hold accepting views. 30 Informed by these findings, campaign messages should normalize help-seeking by correcting misperceptions about public attitudes and emphasizing that acceptance may be more widespread than people assume.
Survey findings also indicated that participants favored coping strategies emphasizing personal control (eg, accepting the reality of the situation, turning to work or other activities) over seeking support or advice from others. Yet, consistent with research, social connection emerged as a potential critical protective factor,20-22 with higher connectedness associated with lower perceived stress and SUD risk, and greater self-efficacy and response efficacy for stress management. Messaging should therefore affirm personal agency while illustrating how social connection can enhance coping—offering clear yet flexible actions, such as small steps like checking in with a friend, presented in ways that support autonomy and feel adaptable to individual needs.
Despite recognizing the effectiveness of coping strategies for reducing stress (ie, higher response efficacy), participants expressed less confidence in their own ability to apply them (ie, lower self-efficacy). Since research has shown that adaptive coping is positively associated with self-efficacy, 24 campaign messages should highlight accessible coping strategies and normalize trial and error to help individuals build confidence in managing stress in healthier ways.
Lastly, subgroup analyses revealed notable disparities in social connectedness during COVID-19. Young adults were more likely to report decreased social connections compared to other age groups. Self-identified non-Hispanic Black respondents were more likely than the overall sample to report decreased connection (48% vs 44%) and cite prior negative healthcare experiences as barriers to seeking support. Increased loneliness was more commonly reported by individuals in urban, suburban, and small-town settings than in rural areas. This points to the importance of meeting people where they are and tailoring messaging to reflect diverse community needs and experiences.
Community Leader Interviews
To gain contextual insights beyond quantitative data, the CHC conducted 35 in-depth interviews with community leaders, including coalition managers, religious figures, non-profit leaders, healthcare professionals, and charitable organization directors from across Texas. As trusted messengers, community leaders play a critical role in connecting public health efforts to diverse populations by offering insights into local dynamics, resource gaps, and culturally relevant messaging strategies campaigns resonate locally.16,31 Interviews were conducted on Zoom by the first interviewer using a semi-structured guide that explored community leaders’ perspectives on the impact of COVID-19 on SUD, mental health, and community well-being. On average, interviews lasted 45 minutes and were audio/video recorded with the participant’s consent for transcription and analysis purposes. Each participant was compensated with a $50 gift card for their time.
Data Analysis
Transcripts were inductively coded by 4 experienced qualitative health researchers using Braun and Clarke’s reflexive thematic analysis (RTA), which emphasizes the researcher’s active role in interpreting the data to develop coherent patterns of meaning. 32 Coders first engaged in repeated transcript readings and reflexive memo writing to deepen familiarity with the data. Through iterative, line-by-line initial coding, they prioritized reflexivity over reliability, emphasizing researcher interpretation over consensus. The team met regularly to collaborate, discuss emergent patterns, and interpret and refine thematic insights. Consistent with RTA, rigor was established through transparency, ongoing reflexive dialogue, and rich engagement with the data rather than inter-rater reliability. 33
Several interconnected themes emerged, including pandemic-driven stress and coping, barriers to healthy coping and support, declining trust in health systems, and the need for community-centered communication strategies. Community leaders identified alcohol as the most pressing substance use issue, along with concerns about increases in underage and binge drinking, marijuana, methamphetamine, opioids, and vaping. Regarding mental health, participants also highlighted an alarming increase in adolescent and youth depression and suicidal ideation, attributed to increased feelings of isolation, boredom, stress, food insecurity, and drug use as coping mechanisms. Participants described how short-term coping often evolved into long-term patterns, due to these stressors as well as limited access to healthier alternatives. Many also expressed a growing mistrust of state and federal health departments since the pandemic among their communities, citing conflicting information as the primary cause. Finally, they noted that mental health was often discussed in indirect terms (eg, “a tough couple of months”) and emphasized the need for stigma-reducing messaging that reflects local language and resonates with how people actually talk about their experiences.
Regarding messaging, community leaders emphasized the need for SUD and mental health education for parents and youths. Empowerment emerged as a standard message strategy, as they stressed the importance of delivering health messages through trusted community organizations, healthcare providers, public health teams, or social media platforms (eg, Instagram, TikTok). They also recognized the influence of community activities and religious leaders, but noted limited collaboration between churches and governmental health entities.
Campaign Development
Creative Brief
A critical step in developing any health communication intervention is creating a creative brief that synthesizes formative research findings and provides strategic guidance for the creative team designing public messaging materials. 13 In our campaign, the creative brief was directly informed by formative research and structured around standard components; the contents of the creative brief are summarized in Table 4.
Creative Brief.
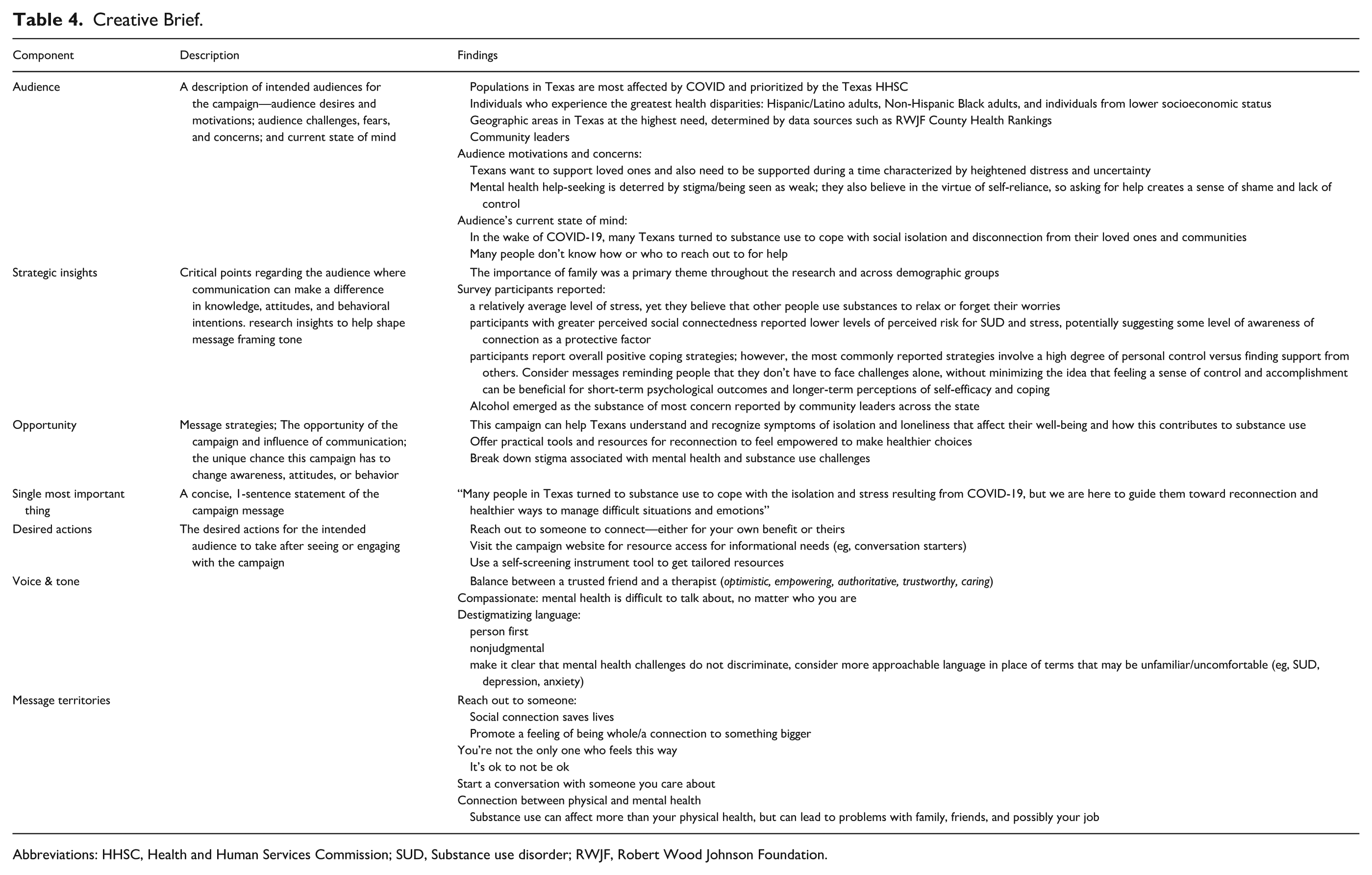
Abbreviations: HHSC, Health and Human Services Commission; SUD, Substance use disorder; RWJF, Robert Wood Johnson Foundation.
Community Leader Focus Groups: Disseminating Findings and Guiding Next Steps
A series of focus groups with community leaders who had previously participated in the formative interview phase was conducted to iteratively shape the campaign message strategies. The overall goal was to share research findings and elicit feedback on proposed campaign messages and their potential impact on their communities. Moderated by the first author, the 2 focus group sessions lasted about 60 minutes, were audio-recorded, transcribed, and analyzed thematically.
During the first round, participants reviewed findings from community leader interviews and statewide surveys and confirmed they aligned with their experiences. They also offered feedback on proposed ideas, leading to the refinement of messaging strategies. For example, the message “take back control,” was considered too absolute, especially in situations where support options are limited, and recommended a more inclusive and attainable alternative: “Any progress is good progress.” Participants stressed that messages should go beyond awareness by providing clear, actionable resources (eg, self-screening tools). Without these, they worried that messages could leave people unsure about what to do next. From the perspective of the Stages of Change model, this feedback highlights the importance of meeting individuals where they are and aligning messages with their current readiness to change to support progression from contemplation to action. 13 In reviewing potential messages, participants found vague collective language (eg, “we are all in this together”) unconvincing, especially in a polarized context where shared experience feels out of reach.
In the second round, participants reviewed 2 campaign concepts: “Turn To,” with messages centered on turning to others for social support, and “On My Mind,” conveying messages about checking in on people who have been on someone’s mind, reflecting on one’s substance use and how to feel better. Feedback was helpful in refining messages and visual style, with participants emphasizing the need for an authentic tone. They noted that “Turn To” felt more uplifting, “On My Mind” more somber, and cautioned against superficial portrayals of healthier coping strategies.
Campaign Framework
The final step in the process was settling on a final campaign message framework that brought together key points from multiple rounds of formative research, relevant evidence from health communication theory and literature, and key considerations from the perspective of the state and its goals with this campaign. The final campaign framework guided the development of all campaign materials, such as an online interactive screener, conversation guides, video advertisements, out-of-home messaging, and digital media buys.
The final campaign was built around the idea of Turn To, given its flexibility—turn to others for social support, turn to someone you might be concerned about, turn to a variety of healthier coping strategies, etc. Given the importance of local community leaders to the development of the campaign and eventual dissemination, it was also essential to ensure the campaign would include key messages relevant to different kinds of community leaders to incorporate into their work so that it is ecologically valid. After approval by the state health department, this campaign framework would guide all work on the campaign, including the eventual public launch, ongoing implementation and refinement, and evaluation.
Discussion
Health communication is essential to public health efforts, shaping how people understand and respond to health information in ways that raise awareness, build knowledge, shift attitudes, and influence behavior.15,16,34 Theoretically grounded, data-driven campaigns have proven effective in promoting behavior change across a range of health issues including nutrition, 35 tobacco prevention, 36 and opioid use disorder. 31 That said, few health communication campaigns have leveraged social connection as an upstream strategy for broader SUD prevention efforts.11,15 This gap underscores the importance of centering social connection in our campaign approach. The purpose of this report was to illustrate how rigorous, evidence-based communication research informed the development of a statewide public health campaign aimed at strengthening social connection to reduce SUD risk and support mental well-being. As the most extensive public health campaign in Texas history, it offers a replicable framework and practical insights into integrating research across all stages of campaign design and implementation.
The work on this project reflects best practices in health communication campaign design, integrating formative research, message development, and concept testing.13,37 By combining quantitative and qualitative data across multiple stages, the campaign ensured ecological validity and cultural relevance, and theoretical alignment. Rather than broadly encouraging people to reconnect with others, the campaign emphasized the quality of social connections, not just the quantity, by modeling realistic and achievable coping behaviors. Research has shown that vague or overly broad behavioral recommendations are less effective, especially when they lack clear behavioral guidance or fail to address barriers like low confidence. 16
While it is an established best practice in health communication campaign design to review relevant literature and other comparable campaigns, it was helpful and productive at the launch of this project; traditional academic processes, such as human subjects approval, can take time—these kinds of reviews can make progress while pursuing other parts of the formative research approach. The campaign’s goals made the academic literature review particularly complex and expansive, covering multiple topic areas. Findings were translated into concise, actionable summaries for program and creative teams—a process that can benefit similar efforts regardless of their scope or resources. A key lesson from this work is the value of using complementary approaches to data collection over time to validate findings and sustain stakeholder engagement. Multiple surveys and rounds of qualitative data collection with community leaders ensured the research team could confirm data findings via alternative methods, refine messages over time in partnership with stakeholders, and develop an evidence-based messaging framework for the campaign.
Limitations
The research has limitations, many stemming from practical constraints of this kind of work. While parts of the formative research used representative samples (eg, online statewide surveys), others relied on convenience sampling (eg, community leader stakeholder interviews), which may limit generalizability, even within this state. Such limitations must be balanced against the potential for eventual campaign messages to be evaluated in more advanced ways—including actual changes in knowledge, attitudes, and behaviors via campaign exposure—and the model this work can offer for funding health communication research more broadly. Relying on funding for the practice of health communication has been a largely untapped approach for pursuing academic health communication research, and this project demonstrates how rigorous research can be conducted in the service of developing public health campaigns—simultaneously advancing the field and personal and public health.
Conclusion
This manuscript outlines the development of a comprehensive statewide health communication campaign in Texas, targeting mental health awareness and substance use prevention in response to the lasting consequences of the COVID-19 pandemic. Informed by evidence and stakeholder input through a multi-method formative research process, the campaign offers a replicable model for strategic, evidence-based health communication. Although the pandemic has ended, its impact on public mental health and substance use has revealed the importance of addressing these as interconnected challenges in future public health efforts.
Footnotes
Ethical Considerations
Institutional Review Board approval was not required.
Author Contributions
Mike Mackert: Conceived and designed the analysis, other contribution. Erin Donovan: Conceived and designed the analysis, other contribution. Karly Quaack: Conceived and designed the analysis, collected the data, wrote the paper, other contribution. Weijia Shi: Conceived and designed the analysis, performed the analysis, other contribution. Daniela De Luca: Conceived and designed the analysis, other contribution. Haley Nolan: Conceived and designed the analysis, collected the data, other contribution. Audrey Shaffer: Other contribution. Jiahua Yang: Conceived and designed the analysis, other contribution. Olubunmi Obayemi: Conceived and designed the analysis, performed the analysis. Tracy Arrington and all else: Conceived and designed the analysis, collected the data, contributed data or analysis tools, performed the analysis, wrote the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Texas Health and Human Services Commission (#HHS001042300001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.