
Abstract
Background:
Peer recovery specialists (PRSs) are professionals with lived experience in substance use and recovery, playing an important and growing role in the substance use care workforce. However, there is limited guidance on best practices for integrating PRSs into health care settings and supporting their well-being and career development. This study explores the perspectives experienced PRSs across diverse clinical settings regarding training, support, and professional development.
Methods:
Between September 2021 and February 2022, we conducted semi-structured interviews with 15 PRSs from the Philadelphia area who participated in a virtual PRS support group. The interviews focused on barriers, facilitators, and unmet needs in their roles. Interviews were recorded, transcribed, and analyzed using thematic content analysis.
Results:
Most participants were female (53%) and white (93%) (Table 1), with 80% having 4 or more years of work experience. Participants worked in a variety of settings, including community-based programs (47%), outpatient specialty substance use disorder treatment (27%), and primary care (20%). Key interview themes included : (1) Motivation and satisfaction: Participants found meaning in client successes and peer support, emphasizing relationships and teamwork; (2) Burnout and role challenges: Many experienced high stress due to role ambiguity, excessive caseloads, and secondary trauma; (3) Supportive workplace factors: structured supervision, professional networks, and feeling valued within care teams were crucial supports; and (4) Professional development needs: Participants identified gaps in training, system navigation, and career advancement opportunities.
Conclusion:
PRSs are vital in substance use care but face significant challenges related to burnout, ambiguous role expectations, and inadequate job training. Establishing structured models for PRS training, supervision, and professional development may enhance their effectiveness within health systems.
Keywords
Highlights
Peer recovery specialists (PRSs) play a vital role in substance use care but face major challenges.
Burnout, role ambiguity, and high caseloads impact PRS effectiveness and job satisfaction.
Structured supervision, professional development, peer networks, and positive workplace culture enhance PRS well-being, job sustainability, and retention.
Clear career pathways and ongoing training can improve PRS integration in health care settings.
Introduction
The United States continues to face high overdose rates, largely driven by fentanyl, with 110 000 deaths reported annually as of August 2023. 1 Despite the availability of effective medications for opioid use disorder (MOUD), like methadone and buprenorphine, a minority of individuals receive treatment.2,3 Barriers to care include navigating a complex treatment system, limited psychosocial supports, stigma, and distrust in medical settings.4 -6
The integration of peer recovery specialists (PRSs) into substance use treatment has emerged as a promising strategy to address these challenges.7,8 PRSs are individuals with lived experience in substance use and recovery who are certified and trained to support people with substance use disorders (SUDs), including those seeking MOUD.9,10 Although training and certification vary by state, PRS roles generally align with core competencies established by the Substance Abuse and Mental Health Service Administration (SAMHSA). 11 PRSs bring firsthand knowledge of the systemic and personal barriers patients may face—including housing, transportation, and insurance—while their lived experience can foster trust and reduce power imbalances in clinical settings.10,12
A growing body of research highlights the benefits of incorporating PRSs into substance use care models across various settings, including inpatient hospitals, emergency departments, specialty substance use treatment, primary care, and harm reduction services.7,13 -16 Studies show that PRS integration may reduce substance use, improve treatment engagement, strengthen relationships with treatment providers, and enhance overall satisfaction with care.7,8,16 -18 Additionally, PRSs play key roles in promoting harm reduction principles and addressing the stigma often faced by individuals with SUD.1,19
Despite the growing integration of PRSs into substance use treatment settings, implementation has outpaced the development of best practices for integrating this professional role. While research highlights the positive impact of PRSs on patients with SUD seeking MOUD, it also underscores challenges in providing adequate support and supervision to PRSs across clinical settings.20 -22 Variability in training requirements, lack of role-specific preparation, and inconsistent expectations across care settings further complicate implementation.17,23 Additionally, PRSs frequently experience burnout, compassion fatigue, and concerns about adequate compensation. 7
Given the increasing adoption and demonstrated effectiveness of PRSs, it is essential to identify best practices for their implementation and support. This study explores the perspectives of experienced PRSs from diverse clinical settings in Philadelphia, focusing on their training, support, and professional development needs.
Methods
Study Design
Semi-structured qualitative interviews were conducted with PRSs to explore their experiences, challenges and professional needs. This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines and was approved by the University of Pennsylvania Institutional Review Board. 24
Study Setting
This study was conducted in Philadelphia, a city with one of the highest overdose death rates among large US cities. 25 Participants were recruited from a virtual peer support group designed for PRSs working in various clinical and community settings.
In Pennsylvania, PRSs are credentialed as certified recovery specialists, requiring a minimum of 78 hours of standardized instruction, at least 18 months of continuous personal recovery, a statement of lived experience, and a passing grade on the state certification examination. To maintain certification, PRSs must complete 30 continuing education credits, including 6 in ethics and 3 in confidentiality.
The virtual peer support group met bimonthly, facilitated by an experienced PRS and member of the research team (N.O.). Meetings were largely unstructured, driven by attendees’ needs and interests, including career guidance, resource sharing, and emotional and recovery support. The group is part of a broader initiative by the City of Philadelphia, led by a member of the research team (N.O.), to develop and implement training and professional development for PRSs in medical settings in the Philadelphia area. Through this initiative, members of the research team were directly involved in supporting and coordinating the group, which facilitated the connection with potential interview participants.
Recruitment
Participants were recruited between September 2021 and February 2022 from the virtual peer support group. Eligibility included being an adult (≥18), working as a PRS in the Philadelphia area, speaking English, and the ability to participate in a virtual interview. State certification was not required. Recruitment was conducted via e-mail, and all invited individuals agreed to participate. Verbal informed consent was obtained, outlining the study purpose, protocol, and potential risks and benefits. Interviews were conducted via videoconferencing platform, and participants received a $50 incentive. Demographics were collected via self-report.
Interviews
The semi-structured interview guide explored PRS work environments, the nuances and diversity of PRS roles, and strategies to improve workplace support. The interview guide (Supplemental Material) was informed by existing literature and feedback from experienced PRSs. Major domains included barriers and facilitators to success in PRS works, gaps in institutional support and supervision, and methods to improve professional development.26,27
A trained research assistant (A.J.) with no prior relationships with participants conducted all 15 interviews virtually, each lasting approximately 30 minutes. The interviewer has a background in public health and prior experience conducting qualitative interviews on substance use-related topics, and they regularly debriefed with senior team members throughout data collection. All participants from the support group who were invited agreed to participate, and a total of 15 interviews were conducted. During the coding process, the research team determined that thematic saturation had been reached, with no new themes emerging in the later interviews, and therefore concluded that further recruitment was not necessary.
Data Analysis
Interviews were audio-recorded and transcribed by a professional transcription service. The research team developed an initial coding structure based on the interview guide and emergent themes. Coding was refined through discussion and consensus with the whole team, including N.O., an experienced PRS. Two trained research assistants (K.G. and A.J.) conducted thematic content analysis using NVivo 11 using a constant comparative approach to identify patterns and themes across transcripts. 28 Theme development involved iterative team meetings to group-related codes, resolve interpretive differences, and identify overarching patterns across the data. Twenty percent of transcripts were double-coded, and discrepancies were resolved through team discussion.
Results
Participant Characteristics
Most participants were female (53%) and white (93%) (Table 1). The majority (80%) had 4 or more years of work experience. Participants worked in a variety of settings, including community-based programs (47%), outpatient specialty SUD treatment (27%), and primary care (20%).
Participant Characteristics.
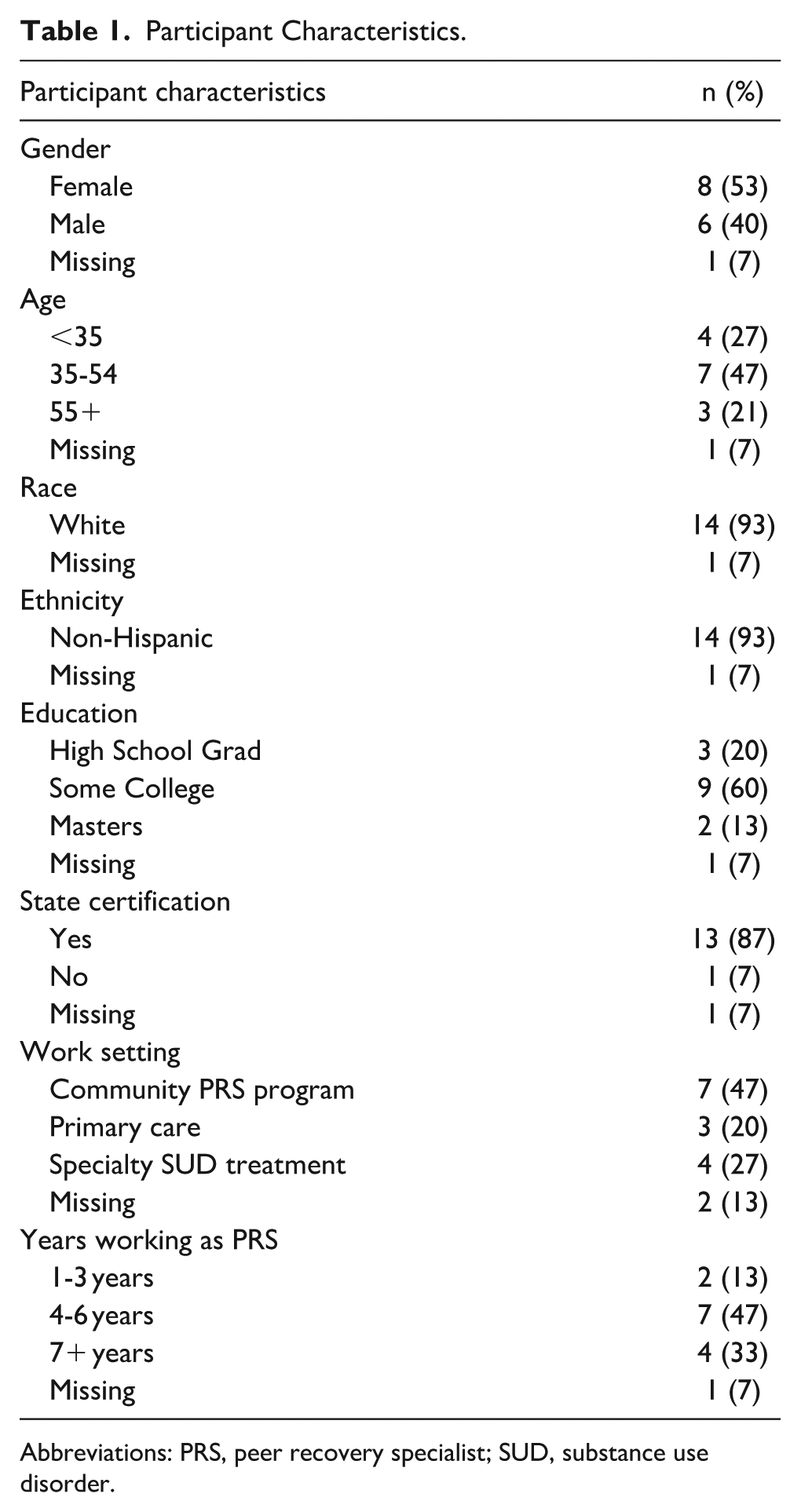
Abbreviations: PRS, peer recovery specialist; SUD, substance use disorder.
The following sections present 4 key themes that emerged from interviews: motivation and professional satisfaction, sources of burnout, supportive workplace factors, and professional development needs. Additionally, a thematic summary table (Table 2) presents an overview of the 4 major themes, including representative subthemes and illustrative quotes. This table is intended to provide a concise visual reference for the main findings described in the narrative text below.
Thematic Summary.
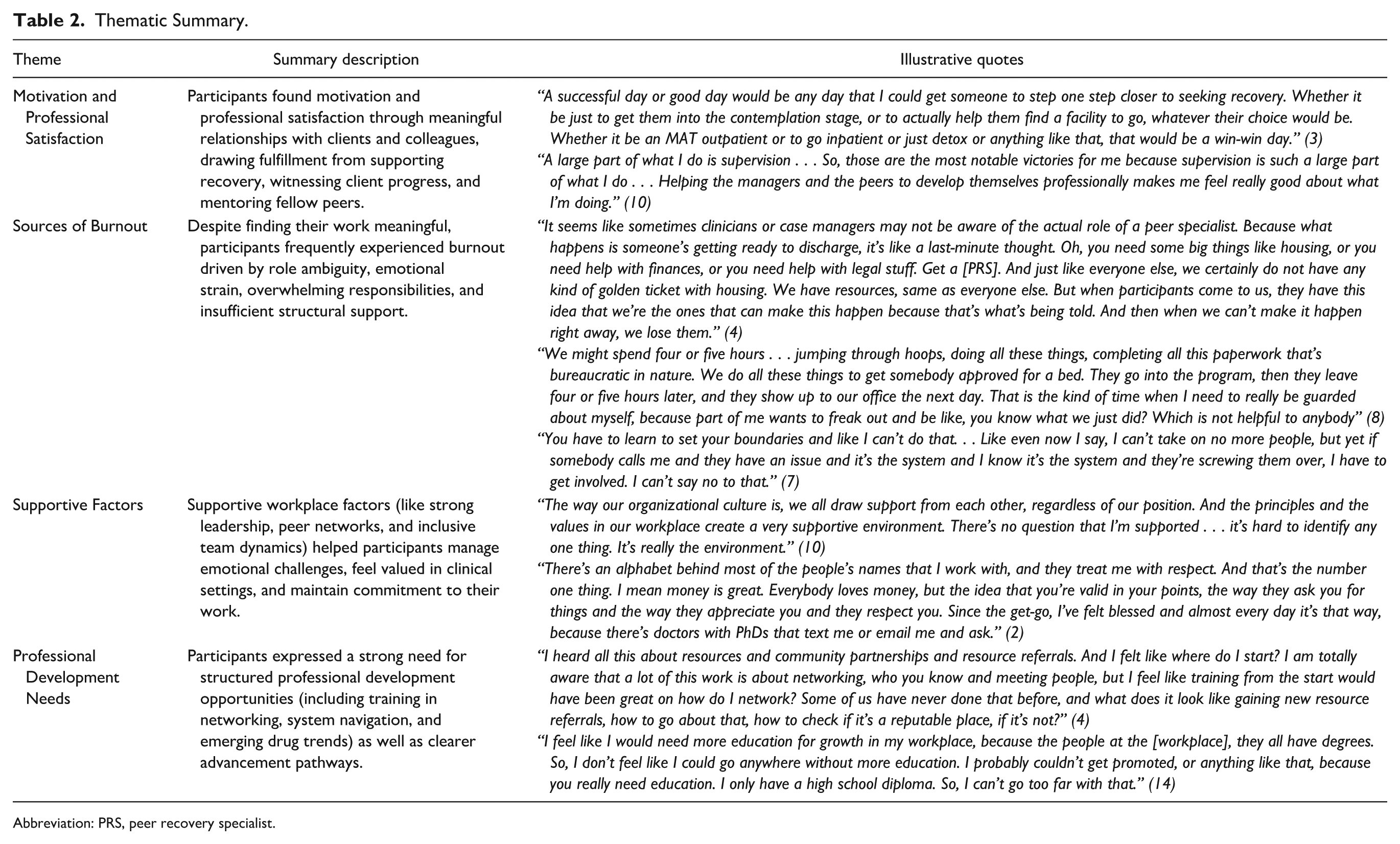
Abbreviation: PRS, peer recovery specialist.
Motivation and Professional Satisfaction
Participants consistently expressed that professional satisfaction came from meaningful interactions with both clients and colleagues. They found fulfillment in helping clients make any positive changes, whether by connecting them to resources or treatment, supporting harm reduction efforts, or providing encouragement. One participant described success as any progress toward recovery, sharing: A successful day or good day would be any day that I could get someone to step one step closer to seeking recovery. Whether it be just to get them into the contemplation stage, or to actually help them find a facility to go, whatever their choice would be. Whether it be an MAT outpatient or to go inpatient or just detox or anything like that, that would be a win-win day. (6)
Satisfaction also stemmed from witnessing a range of patient successes, including engagement with harm reduction resources, initial treatment engagement or long-term recovery milestones. One participant highlighted: One [source of satisfaction] could be if I’m trying to help somebody that’s newer and they wanted to get into treatment. Or were motivated to get better or using harm reduction skills. They just wanted to be motivated and they got into treatment or got onto medication or went and got Narcan and clean needles, and things like that, that would be a good day. Or the opposite of getting a phone call or knowing that this person I’ve been working with for a long time just got a job or got their kids back. So, it can be a range of things. (3)
Beyond patient interactions, participants also found professional fulfillment in supporting fellow PRSs. They valued opportunities to mentor peers, provide emotional support, and contribute to team problem-solving. One participant emphasized the importance of supervision and leadership: A large part of what I do is supervision . . . So, those are the most notable victories for me because supervision is such a large part of what I do . . . Helping the managers and the peers to develop themselves professionally makes me feel really good about what I’m doing. (10)
Overall, participants found value in fostering positive relationships, whether in the lives of their patients or within their professional networks, particularly when they could contribute to positive changes or team dynamics. The ability to build meaningful relationships was a key driver of motivation and fulfillment.
Sources of Burnout
While participants found their work fulfilling, they frequently reported experiencing high levels of burnout, limited professional support, and inadequate resources for clients and for their own professional development. Several key factors contributed to burnout, including unclear role expectations, overwhelming case management responsibilities, and a lack of defined boundaries across different work environments. Many participants described struggling with role ambiguity, particularly where their responsibilities overlapped with social work and clinical care, often leading to excessive workloads. One participant shared: It seems like sometimes clinicians or case managers may not be aware of the actual role of a peer specialist. Because what happens is someone’s getting ready to discharge, it’s like a last-minute thought. Oh, you need some big things like housing, or you need help with finances, or you need help with legal stuff. Get a [PRS]. And just like everyone else, we certainly do not have any kind of golden ticket with housing. We have resources, same as everyone else. But when participants come to us, they have this idea that we’re the ones that can make this happen because that’s what’s being told. And then when we can’t make it happen right away, we lose them. (4)
Many participants found it difficult to balance multiple job roles, from providing motivational support and leveraging lived experience to coordinating complex social services and treatment referrals.
The emotional toll of working with a high-needs population was another major challenge. Participants frequently supported people struggling with long-term housing instability, barriers to treatment, and systemic failures, making it difficult to witness repeated cycles of hardship. One participant described the emotional burden: My job is to try to help people, and I take it to heart, and that’s I think the reason a lot of us get burned out so bad, a lot of people, because of the fact that you don’t go to bed at night not thinking about the person that you’re trying to help if something bad happened to them. (2)
Participants also expressed frustration with navigating challenging bureaucratic systems that often hindered their ability to help patients. Despite investing significant time in securing housing or treatment placements, participants often observed that some patients faced difficulties remaining in programs or maintaining engagement with services. This experience could be challenging and emotionally taxing: We might spend four or five hours . . . jumping through hoops, doing all these things, completing all this paperwork that’s bureaucratic in nature. We do all these things to get somebody approved for a bed. They go into the program, then they leave four or five hours later, and they show up to our office the next day. That is the kind of time when I need to really be guarded about myself, because part of me wants to freak out and be like, you know what we just did? Which is not helpful to anybody. (8)
High caseloads and the on-call nature of PRS work also made difficult to achieve work-life balance. Many participants described feeling obligated to be available at all hours, often at the expense of their own well-being: You have to learn to set your boundaries and like I can’t do that. . . Like even now I say, I can’t take on no more people, but yet if somebody calls me and they have an issue and it’s the system and I know it’s the system and they’re screwing them over, I have to get involved. I can’t say no to that. (7)
In addition to emotional and logistical burdens, participants noted that administrative requirements—such as documentation—added another layer of stress, often feeling misaligned with the relational nature of their work. One participant described this challenge: If you want to talk about things that make you anxious, it’s all the documentation – documentation is very hard when you’re talking compassionately to people. Grabbing facts during compassion – that’s an art. (6)
Finally, participants identified secondary trauma as a major concern, particularly given that they were in recovery themselves. Supporting people who were actively using substances or struggling with relapse could be emotionally draining: If you’re fresh in recovery, that’s a lot. You’re like a sponge. You’re always sucking everybody’s stuff up. (2)
Overall, participants grappled with unrealistic expectations and systemic barriers while deeply investing in their patients’ well-being. Without clear job structures, strong professional support, and safeguards in place to address work-life balance, burnout remained a challenge.
Supportive Factors
Almost all participants identified aspects of their work environments that provided meaningful support. Material benefits, such as paid leave and competitive salaries, as well as positive workplace culture were valued. Supportive and respectful leadership, strong team relationships, and open communication were frequently cited as factors that enhanced their professional experience. One participant described the significance of their organization’s culture: The way our organizational culture is, we all draw support from each other, regardless of our position. And the principles and the values in our workplace create a very supportive environment. There’s no question that I’m supported . . . it’s hard to identify any one thing. It’s really the environment. (10)
Structured support systems, including supervision, mentorship, and professional development opportunities, were also seen as essential. Participants valued regular check-ins and spaces to discuss challenges, particularly when dealing with emotionally difficult situations. One participant emphasized the importance of supervision when facing secondary trauma: I’d never experienced [secondary trauma] before, and I was eager for my supervision, so I had somebody to talk to. My supervisor said, there’s gonna be days where you’re gonna want supervision because you have something to talk about, and that was one of those days that I was like, thank God I have somebody I can talk to about what’s going on. (9)
Feeling respected and valued within their teams was another critical source of support. While PRSs play an important and unique role in clinical environments, participants noted that hierarchical workplace structures sometimes left to them feeling less valued than traditional clinical staff. However, when PRSs were included as key members of the team, it strengthened their sense of belonging. One participant shared: There’s an alphabet behind most of the people’s names that I work with, and they treat me with respect. And that’s the number one thing. I mean money is great. Everybody loves money, but the idea that you’re valid in your points, the way they ask you for things and the way they appreciate you and they respect you. Since the get-go, I’ve felt blessed and almost every day it’s that way, because there’s doctors with PhDs that text me or email me and ask. (2)
Because PRSs have unique roles in clinical spaces, many participants stressed the importance of peer support and debriefing with other PRSs as a way to process their experiences. Peer spaces allowed them to feel understood and validated: Then when you go to any other kind of neutral support group meeting, it’s just like you think that everything in your head is crazy and then you say it out loud to a group of people and they don’t call you crazy, they’re like, oh, yeah, I’ve thought that, too. Just to not – the sense of community and just not feeling alone and like a lunatic all the time is a beautiful thing. (11)
Having professional support from other peers, whether in the workplace or in their personal lives, was an important buffer against burnout. Many participants emphasized that peer networks helped them navigate challenges while reinforcing their sense of purpose and commitment to their work.
Professional Development Needs
Opportunities for professional development varied based on participants’ work environments. Many participants emphasized the need to build networks to better locate and navigate patient resources, a skill they often developed informally rather than through structured training. One participant expressed the challenge of learning how to network effectively: I heard all this about resources and community partnerships and resource referrals. And I felt like where do I start? I am totally aware that a lot of this work is about networking, who you know and meeting people, but I feel like training from the start would have been great on how do I network? Some of us have never done that before, and what does it look like gaining new resource referrals, how to go about that, how to check if it’s a reputable place, if it’s not? (4)
Many participants also found navigating decentralized resources—such as housing, treatment programs, transportation, and insurance—difficult. When unfamiliar with specific resources, participants often relied on peer networks, including those outside of their local area, to connect patients to appropriate supports.
Participants described mixed experiences with workplace opportunities for growth and promotion. Some felt that leadership pathways were available and that their organizations encouraged professional development: In my workplace currently there’s a lot of opportunities for growth. They’re very open to my ideas, even though I’m really new with the organization. But they’re letting me put together a presentation on stigmatizing language that they’re gonna let me present to the other [peers] . . . They also provide money that you can get reimbursed, if you have to pay for trainings, every year. So, actually it’s really good opportunity, in those regards, with my company. (12)
However, these opportunities did not always come with formal promotions or titles. Others saw limited opportunities for career advancement, particularly those without advanced degrees. One shared concern about their ability to move up in their organization: I feel like I would need more education for growth in my workplace, because the people at the [workplace], they all have degrees. So, I don’t feel like I could go anywhere without more education. I probably couldn’t get promoted, or anything like that, because you really need education. I only have a high school diploma. So, I can’t go too far with that. (14)
Participants also identified a range of training needs, including workplace skills such as using e-mail and word-processing software. Others sought training on substance use trends, changes in the drug supply, and interactions with the criminal-legal system. Several participants mentioned interest in ongoing education on emerging best practices in substance use treatment and recovery support, including updates on policy changes and new care models. One noted: I feel like there could be one place that you could get a freaking newsletter every week, this is what’s up in the fucking substance user scene right now, this is the new thing that’s coming out, or this is less popular. (12)
Although continuing education is required for certification, most participants felt that existing programs did not adequately prepare them for the challenges of their roles. Instead, participants often relied on peer support networks and even their patients to stay informed: And actually, if we want to know something, all we have to do is ask our participants. They are the best. They know what’s out there, and they train us also. (15)
Overall, PRS participants expressed a desire for more structured opportunities to develop their skills, expand their knowledge, and advance in their careers.
Discussion
This study highlights the challenges faced by PRSs in their work and strategies to increase support and promote professional development. Across work environments, participants frequently reported burnout due to a combination of demanding, ill-defined roles, and a lack of work-life balance. Despite these challenges, participants remained committed to their work, finding fulfillment in supporting individuals with SUD. Many felt most effective when working in a supportive organizational culture with opportunities for professional growth.
These findings add to a growing body of literature on the role of PRSs in substance use care and factors that shape their experiences.29,30 PRSs hold a unique position in health care settings, combining professional training with lived experience to provide emotional, social, and practical support. 31 Emerging evidence suggests that PRSs may improve treatment access and retention while helping to mitigate stigma.32 -35 Additionally, PRSs are often described as “bridges” between individuals seeking services, the health care system and the wider community, helping to facilitate engagement and continuity of care. 36 These findings suggest that the bridge-role of PRSs—positioned between patients, health care systems, and community resources—can contribute to task ambiguity, difficulties setting boundaries, and burnout, particularly given the complex psychosocial needs of the patient population and inadequate systems for addressing these needs. These challenges align with prior research on peer workers in SUD and mental health treatment settings.27,37 -39
Unlike clinicians or social workers, PRSs rely on lived experience trust building to support patients, fostering a unique form of peer-based engagement. However, they may also face imposter syndrome and stigma within hierarchical clinical environments.30,40 -42 To optimize PRS effectiveness and job sustainability, further work is needed exploring strategies for managing large caseloads, clarifying PRS roles within clinical settings, and reducing stigma for both patients and peer workers.
This study is among the first to identify facilitators of effective PRS implementation across a variety of clinical settings. Supportive workplace environments played a critical role, including both formal structures and connections to peer recovery networks, an insight that, to our knowledge, has not been previously documented in the literature. Another major facilitator was being integrated and valued within interprofessional teams, aligning with prior research showing that workplace policies and practices impact PRS mental and emotional well-being. 29
These findings also highlight the importance of professional development opportunities. In addition to appropriate compensation and benefits, participants expressed a strong desire for leadership roles, mentorship opportunities, and peer collaboration. Many also sought opportunities to continue education on a broad range of topics within substance use treatment. This is particularly relevant given existing literature showing mixed attitudes among PRSs toward evidence-based treatment like MOUD. 43 Expanding continuing education and peer mentorship programs may be essential in strengthening PRS effectiveness and ensuring the dissemination of best practices in treatment. Existing literature has demonstrated the need for standardized training guidelines for PRSs, and this study adds important context by illustrating those needs from the perspective of the peers themselves. 44 Some participants noted that lacking a formal degree limited their ability to advance in their roles, despite extensive lived and professional experience. This underscores how credentialism may unintentionally restrict career progression for PRSs and contribute to inequities in workforce development. Future PRS programs should prioritize fostering a supportive work culture, expanding accessible educational opportunities, and creating clear pathways for professional development. Recognizing PRSs as integral members of health care teams will be essential to sustaining and improving peer recovery models.
Additionally, the unique professional background and workplace environment of PRSs presents both challenges and opportunities. An important challenge is the issue of secondary trauma, a concern frequently identified by our participants and well documented in the literature.45 -48 PRSs working in SUD care often operate in high-risk, high-intensity environments shaped by overdose risk, an unstable drug supply, and fragmented service systems. These conditions demand real-time adaptation, nuanced harm reduction knowledge, and the ability to navigate complex psychosocial needs. These specific requirements are not consistently addressed by broader peer support models. Many participants emphasized that having peer networks and peer-based supervisory structures was essential for processing difficult patient experiences and mitigating the emotional toll of the work. At the same time, PRSs’ deep connection to patients’ lived experiences makes them a valuable source of insight. Participants highlighted that individuals with SUD, who have historically been marginalized, offer critical perspectives on their own needs and the systemic barriers they face. This study adds to the literature by documenting how PRSs not only draw from their own experiences but also rely on real-time knowledge sharing with patients to stay informed about emerging drug trends, underscoring both the strength of experiential expertise and the limitations of formal training in keeping pace with a rapidly evolving and unregulated drug supply. In this context, PRSs adapt in real time to meet patient needs, often filling critical knowledge gaps that formal education has not yet addressed. Ensuring that patient voices are incorporated into care models can improve service delivery and better address emerging challenges in substance use treatment. 49
One important limitation of this study is the homogeneity of participants, most of whom were white and female. Therefore, the findings do not fully capture the perspectives and experiences of PRSs from minoritized groups. There are limited demographic data on PRSs at the local or national level, and future research should examine how race, gender, sexuality, and other social identities influence PRS experience, their relationships with clients, and their role within interprofessional teams. Additionally, this study was conducted in a single geographic area and PRS certification was subject to Pennsylvania-specific regulations, which may limit the generalizability of our findings to other regions. Participants were experienced PRSs recruited from a voluntary peer support group, which may reflect a more engaged subset of the workforce with greater access to resources or opportunities for reflection. As such, their perspectives, particularly around support needs and burnout, may not fully represent the broader PRS workforce. Finally, this study did not include PRSs working in inpatient hospital settings or emergency departments, which are critical access sites for individuals with SUD. Future research should explore how PRSs operate in these high-acuity environments and the specific challenges they face in engaging patients during acute care encounters. Future research should also explore how clinicians perceive the integration of PRSs to inform effective role clarity and interprofessional collaboration.
In conclusion, as PRSs continue to be integrated into the substance use treatment workforce, these findings highlight key considerations for workforce development and professional satisfaction. PRSs play a critical role in addressing barriers to treatment access and retention, yet effective PRS implementation depends on supportive workplace environments, clear role definitions, and growth opportunities. Strengthening organizational support systems, fostering a culture that values and respects PRS expertise, and expanding professional development pathways will be essential for developing and sustaining peer recovery models.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251372319 – Supplemental material for Exploring the Perspectives of Peer Recovery Specialists: Needs for Training, Support, and Professional Development
Supplemental material, sj-docx-1-saj-10.1177_29767342251372319 for Exploring the Perspectives of Peer Recovery Specialists: Needs for Training, Support, and Professional Development by Margaret Lowenstein, Kathryn Gallagher, Nicole O’Donnell, Aminata Jalloh, Selena Suhail-Sindhu, M. Holliday Davis and Jeanmarie Perrone in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of our interview participants and thank them for generously sharing their insights. We respectfully acknowledge the lands of the Lenni-Lenape People of Lënapehòkink and the Poutaxat on whose territory the University of Pennsylvania stands and whose historical relationship with the land continue to this day.
Author Contributions
Conceptualization: ML, KG, NO. Formal analysis: KG, AJ. Writing—original draft: ML, KG. Writing—review and editing: NO, AJ, SSS, MHD, JP. Project administration: KG. Supervision: ML.
Data Availability Statement
Data not available. Due to the sensitive nature of the questions asked in this study, participants were assured raw data would remain confidential and would not be shared.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by funding from the City of Philadelphia Department of Public Health. Dr. Lowenstein is supported by the National Institute on Drug Abuse (K23DA055087).
Compliance,Ethical Standards,and Ethical Approval
This project received ethics approval from the University of Pennsylvania Institutional Review Board. Respondents gave verbal consent for participation and publication before starting interviews.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.