
Abstract
Background:
Substance use disorder (SUD) is a chronic and recurrent condition posing a significant health burden. The integration of out-on-pass (OOP) or day leave privileges during inpatient rehabilitation has been theorized to support recovery by enhancing social reintegration and preparing patients for discharge. However, evidence on the impact of inpatient OOP on post-discharge relapse rates is scant. This study investigates the effect of OOP during inpatient treatment and relapse outcomes.
Methods:
A retrospective cohort design was used to analyze data from 72 patients discharged from the Umm Salal Treatment and Rehabilitation Center in 2023, focusing on OOP during rehabilitation and urine drug test results during aftercare. Key variables included OOP frequency, comorbid personality disorders, forensic history, and relapse indicators. Statistical evaluation utilized logistic regression, chi-squared tests (Fisher’s exact test where appropriate), and survival analysis to identify predictors of relapse, adjusted for potential confounders.
Results:
Of the participants, 28 (38.9%) were granted OOP during inpatient treatment, while 44 (61.1%) were not. Relapse, defined by a positive urine drug screening post-discharge, occurred in 29 patients (40.3%). The median time-to-relapse was 28 days, with a longer duration observed among those granted OOP. Specifically, during the 26-week study period, 25% of patients with OOP relapsed compared to 50% of those without OOP (statistically significant difference; P = .04892). Survival analysis revealed that time-to-relapse was substantially longer for patients who were granted OOP compared to those who were not (P = .034). Furthermore, the granting of OOP during inpatient treatment of SUD was associated with a 73.2% reduction in relapse hazards ratio (P = .00876).
Conclusion:
This study highlights the potential of OOP as a therapeutic strategy and tool to support sustained recovery in patients with SUD. While relapse remains a significant challenge, OOP may contribute to extended abstinence periods and reduced relapse rates.
Highlights
This paper reveals that relapse into substance use remains a significant challenge post-discharge, but granting out-on-pass (OOP) showed a slower time-to-relapse compared to those without OOP, emphasizing the therapeutic potential of these privileges in reducing relapse rates.
The survival analysis demonstrated that patients granted OOP privileges exhibited a longer time-to-relapse and a lower relapse rate compared to those not granted OOP, reinforcing the value of structured OOP as part of rehabilitation treatment.
Introduction
Substance use disorder (SUD) is a complex, multifactorial chronic condition characterized by cycles of relapse and remission, imposing significant individual and societal burdens. Its global prevalence is rising, notably in regions like the Middle East and North Africa, including Qatar, presenting major public health and economic challenges.1,2 The cyclical nature of SUD results in a high disease burden, exacerbated by psychiatric comorbidities3-5 and an alarming trend of rising substance use rates linked to increased mental health problems, self-harm, and behavioral issues.6-8 This complex interplay is influenced by demographic, environmental, psychological, and therapeutic factors. 9
High relapse rates persist among individuals with SUD despite patient motivation and treatment team support.10-12 These rates remain poorly understood and understudied, largely due to the recent development of services and limited localized data.13-16
Qatar-specific data on relapse rates and substance use disorders remain limited; however, emerging regional evidence indicates significant challenges. The United Nations Office on Drugs and Crime (UNODC) World Drug Report 2024 highlights rising synthetic drug and prescription opioid use, particularly tramadol, across the Gulf Cooperation Council (GCC) region. 1 While overall drug use prevalence in the GCC remains lower than the global average, newer psychoactive substances and non-medical prescription drug misuse pose growing threats, with these trends linked to regional sociocultural and economic factors. 17 Retrospective studies in neighboring countries underscore rehabilitation challenges, such as a 30.17% one-year readmission rate at Saudi Arabia’s Al-Amal Hospital, where amphetamine use disorder significantly predicted relapse. 18 These patterns coexist with nationally reported lifetime SUD prevalence of 4.03%, 19 illustrating regional heterogeneity in SUD profiles. Globally, relapse rates of 40% to 60% mirror trends observed in GCC states,1,17 further emphasizing the urgent need for localized research in Qatar to clarify SUD epidemiology and optimize rehabilitation outcomes.
In addition, individuals recovering from SUD often face challenges in reintegrating into their families and communities, compounded by a lack of protective factors such as stable employment and supportive social relationships. Many also experience difficulties in building the necessary social capital for sustained recovery, demonstrating the importance of more frequent post-discharge evaluations to identify those at elevated relapse risk.20-23
In line with the World Health Organization’s recommendations, many countries, including Qatar, are gradually moving from punitive incarceration to voluntary healthcare models for SUD.24-26 This transition exposed a service gap, particularly for patients with SUD who opt against voluntary treatment, leading to the policies that incorporate court-mandated SUD treatment. 27
To address SUD challenges in Qatar, the Umm Salal Treatment and Rehabilitation Center (USTRC) was established by the Ministry of Interior and the Ministry of Public Health. It offers a mandated biopsychosocial residential rehabilitation program, incorporating non-monetary contingency management to enhance therapeutic engagement. 28 Patients in later rehabilitation stages can earn progressive, structured out-on-pass (OOP) leave privileges, facilitating reconnections with family therapy sessions and supportive social networks in the community.
Debate exists on mandated SUD treatment efficacy, with some studies questioning outcomes29-34 while others report comparability to voluntary programs.35-40 Sustained recovery often faces reintegration challenges, where family engagement is critical for relapse prevention.41,42 As substance misuse rises, providers must enhance effectiveness using treatment models reflecting international best practices tailored to local contexts, ultimately aiming for improved patient outcomes.43,44 This study evaluates factors influencing outcomes within Qatar’s rehabilitation model, particularly OOP utilization.
Our intention in the study is to examine the potential of therapeutic leave programs in the community in preparation before discharge from the hospital (OOP, therapeutic leave, or therapeutic passes, leave, community treatment order within psychiatry and SUD frameworks) to enhance relapse prevention strategies, strengthen social bonds, and facilitate reintegration into the community.45-50.
Observational studies and clinical experience suggest that OOP programs facilitate reintegration by promoting independence, social connections, and motivation, allowing patients to apply coping skills in real-world settings during a gradual transition that reinforces abstinence and behavioral change.51-54 However, concerns exist regarding OOP potentially increasing relapse risk due to exposure to environmental triggers, insufficient coping skills, vulnerability to social pressures, lack of preparedness, and overconfidence.53-56 Crucially, evidence on optimal therapeutic OOP duration for relapse reduction remains scarce.
Mitigating these risks requires a multidisciplinary team implementing OOP within a graded approach, incorporating family therapy and careful consideration of patient autonomy, outcomes, and risk management.48,57,58,59 Establishing healthy community social networks (family, friends, employment) is crucial.41,57,60,61 When carefully applied, OOP empowers patients and reduces relapse risk by enabling gradual reintegration, providing real-world practice, and offering emotional support.58,59 This balance of structured support and freedom fosters self-efficacy, strengthens social networks, and sustains treatment engagement, significantly contributing to recovery success.53,54,62
Empirical research on OOP effectiveness in SUD rehabilitation is scarce, relying primarily on observational studies, qualitative reports, and clinical experience with an absence of rigorous trials. This methodological gap introduces limitations like selection bias and reduced generalizability, though existing literature offers practical insights into implementation frameworks, supervision, and risk management.
Within the GCC region, research on SUD rehabilitation and OOP is particularly limited due to societal stigma, cultural-religious sensitivities favoring inpatient care, and emerging healthcare systems. 13 While regional services show a gradual shift toward adopting international best practices, step-down programs, and community-based recovery initiatives, there remains a critical lack of evidence evaluating OOP benefits in the region.63-65
Given this significant regional evidence gap and the potential of carefully managed OOP to enhance reintegration while mitigating relapse risks, we hypothesize that granting OOP privileges during rehabilitation reduces post-discharge relapse rates with longer cumulative durations yielding progressively stronger protective effects, indicating a dose-response relationship.
Therefore, the objective of this research is to examine the potential association between the granting of OOP privileges during inpatient rehabilitation and subsequent relapse rates following discharge. In addition, it aims to assess whether the duration and frequency of OOP privileges correlate with post-discharge drug screening outcomes, as well as to determine the extent to which such privileges influence the likelihood of relapse after leaving rehabilitation.
This study attempts to add to the body of evidence to inform regional and local policymakers and improve guidelines for service providers.
Methodology
Study Design
This study employed a retrospective medical record-based design to analyze the relationship between various clinical, demographic factors, and treatment outcomes among patients at the USTRC. We aimed at complete enumeration of patients we found without resorting to sampling. The sample size was incorporated in the choice of statistical testing and threshold for statistical significance throughout the analysis. For instance, we preferred using non-parametric tests such as Fisher’s exact and chi-squared tests to parametric alternatives.
Undoubtedly, it would have been far better to carry out a prospective cohort design with a larger sample of patients. However, we opted for a retrospective cohort design due to the severe restriction in terms of time, money, and personnel during the conduct of the current study. We received no financial support, and we hope that future research endeavors in this area will be well-funded to carry out a more comprehensive investigation. The OOP is granted primarily based on the achievement of a certain pre-determined balance of therapeutic engagement across the multidisciplinary plan. This indeed will favor high achievers and patients with better motivation. This constitutes potential selection bias that has to be acknowledged as an inevitable limitation in the current study. The focus was on evaluating OOP privileges during the rehabilitation phase and urine drug test results during the aftercare period. The study covered patients discharged during the entirety of 2023.
Participants and Instruments
Participants
The study population consisted of patients admitted to the USTRC and attending the aftercare clinic. A total of 93 patients were initially identified. However, the final sample size was reduced to 72 due to missing data for several covariates.
The inclusion criteria were patients discharged from USTRC in 2023 and for whom complete medical records, including OOP privileges and urine drug test outcomes, were available. The exclusion criteria were patients with incomplete records for the key variables of interest.
Instruments
Data were extracted from the Cerner electronic health record system, ensuring standardized documentation and access to relevant clinical and demographic information.
Procedures for Data Collection
Data Sources
Medical records, accessed through the Cerner system, were used to extract detailed patient information; OOP privileges (frequency, duration, and urine drug test outcomes) were reviewed. Urine drug test results were collected during the aftercare phase.
Variables
Primary Variables
OOP privileges (frequency and duration).
Urine drug screening (UDS) outcomes (positive or negative results).
Secondary Variables
Clinical data: Comorbid personality disorders, duration of inpatient treatment (used as a proxy for engagement/motivation), and forensic history.
Demographic data: Age, gender, family status, nationality, and occupation.
Outcome Variable
Relapse is defined as at least one substance (apart from nicotine and medications prescribed by a treating doctor) being detected in the urinalysis. We conformed to the thresholds set out by the substance detection machine manufacturer. The urine drug test results will determine whether drug use has been resumed, categorized into timeframes from 1 week of discharge and up to 26 weeks, covering a 6-month period in aftercare.
The Data Analysis
Demographic and clinical characteristics of the participants were summarized using measures of central tendency (mean, median) and dispersion (standard deviation, interquartile range) for continuous variables, and frequency distributions for categorical variables.
The relationship between OOP privileges and urine drug test results was analyzed using logistic regression models to assess predictors of relapse. The exploratory statistical analysis examined the occurrence of OOP with the occurrence of relapse at the specified relapse categories using chi-squared tests (Fisher’s exact test where appropriate) and survival analysis (Kaplan-Meier and Cox proportional hazards methods). Multivariable regression models adjusted for potential confounders, including comorbid personality disorders and forensic history, were performed to identify independent predictors of successful recovery.
Results
Sociodemographic Data
The current study included (n = 72) patients with confirmed SUD diagnosis (Table 1). There were (n = 28, 38.9%) patients who were granted OOP privilege, compared to (n = 44, 61.1%) who were discharged without getting the OOP privilege.
Demographic and Clinical Factors Among Participating Patients and Unadjusted Effect on Documented Relapse.
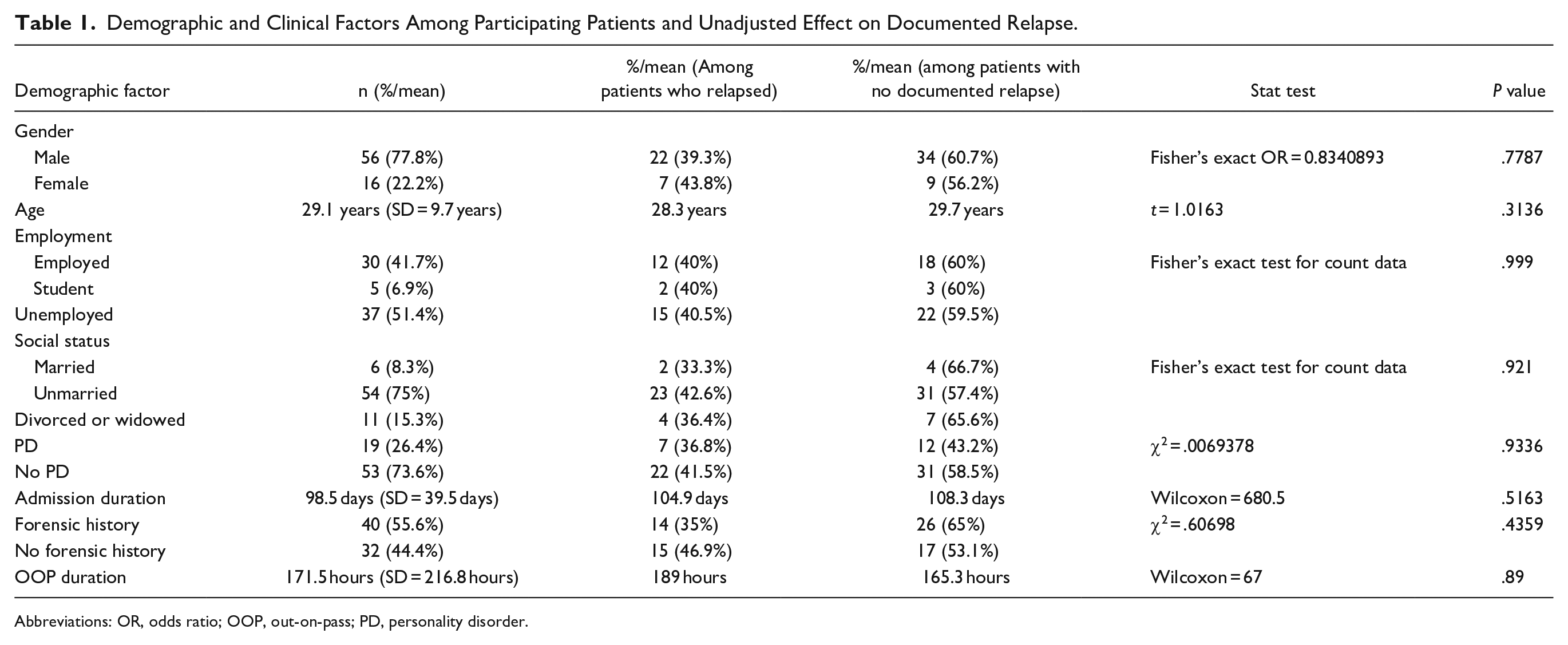
Abbreviations: OR, odds ratio; OOP, out-on-pass; PD, personality disorder.
Notably, (n = 29, 40.3%) of the patients relapsed into SUD at some point during the weekly urine drug testing, with the majority (n = 59.7%) not showing evidence of relapse during the same period.
In terms of age, the mean age was 29.1 years (SD = 5.93 years), ranging between 20 years old and 55 years old. The median age was 29 years.
The mean age among patients who relapsed into substance use during the study period was 28.3 years compared to a mean age of 29.7 years who did not (however, this difference was not statistically significant; t = 1.0163, P = .3132).
In terms of sex, men constituted (n = 56, 77.8%) of the participants, whereas women were (n = 16, 22.2%) of them. However, (n = 22, 39%) of male patients relapsed, compared to (n = 7, 43.8%) of female patients who relapsed during the same period. Again, this difference was not statistically significant (χ2 = .001031, P = .9744).
In terms of occupation status, (n = 30, 41.7%) of the participants were employed, of whom (n = 12, 40%) relapsed post-discharge, whereas the unemployed were (n = 37, 51.4%), of whom (n = 15, 40.5%) relapsed. Clearly, this difference was not statistically significant (χ2 = .0021847, P = .9989).
In terms of duration of inpatient treatment, the mean duration of inpatient treatment was 106.9 days (SD = 39.5 days), ranging between 21 and 286 days. The median duration of inpatient treatment was 98.5 days. The mean duration of inpatient treatment among patients who relapsed into substance use during the study period was 104.9 days compared to a mean duration of inpatient treatment of 108.3 days who did not (however, this difference was not statistically significant; Wilcoxon = 680.5, P = .5163).
In terms of duration of OOP in hours, as shown in Table 3, the mean duration was 177.5 hours (SD = 216.8 hours), ranging between 3 hours and 1080 hours. The median duration of OOP in hours was 100 hours. The mean duration of OOP in hours among patients who relapsed into substance use during the study period was 189 hours, compared to a mean duration of OOP in hours of 165.3 hours who did not (however, this difference was not statistically significant; Wilcoxon = 67, P = .5163).
Primary Objective
To find out whether there is a significant association between receiving OOP privileges during the inpatient period and the urine drug test results after discharge, we applied the Kaplan-Meier survival analysis method with the log-rank test to examine statistical significance. This method is of substantial statistical robustness and has been followed over the years by researchers in the region till very recently. 66 The survival time duration was calculated till time to positive UDS for each patient during aftercare assessment. According to the Kaplan-Meier analysis results, the median time-to-relapse was substantially reduced, almost halved, by applying OOP privilege. The median time-to-relapse among patients granted OOP leave was 84 days, whereas the median time-to-relapse among patients discharged without OOP was 42 days.
There were (n = 29, 40.3%) of the participants who were relapsed with a documented UDS of illicit substances during their evaluation during aftercare clinical assessment. The median time-to-relapse was 28 days (4 weeks after discharge from inpatient treatment). Time-to-relapse ranged between 7 days (week one post-discharge) and 182 days (week 26 post-discharge).
The overall number granted OOP privileges during their inpatient stay was (n = 28, 28.9%). Relapse rate among those granted OOP was (n = 7, 25%). This relapse rate jumped to (n = 22, 50%) among those who were not granted the OOP privilege. However, this unadjusted difference was not statistically significant (χ2 = 3.4673, P = .06259). Notably, the unadjusted difference in relapse rates between OOP and non-OOP groups is not statistically significant (P = .06259). However, when we adjusted the survival analysis to the set of demographic variables of age, gender, and social status, in addition to the clinical variables of personality disorder diagnosis and forensic history, a significant difference emerged in terms of the effect of OOP on relapse rates.
Furthermore, we included all the covariates in the multivariable model without exclusion as they were all deemed clinically important. We did not use any exclusion or stepwise methods in the selection of covariates.
Upon examination of the time-to-relapse among our participants categorized into those granted OOP and those not granted, it was clear that relapse into positive UDS was far more accelerated among patients not granted OOP privileges during their inpatient hospital stay.
The number of patients (total/at risk) by the end of the 182-day period was (n = 6, 14%) for the no OOP group, compared to (n = 10, 34.5%) in the OOP group.
The difference in terms of time-to-relapse was substantially better for patients who were granted OOP, as illustrated in Figure 1, compared to those who were not (χ2 = 4.5, P = .034).
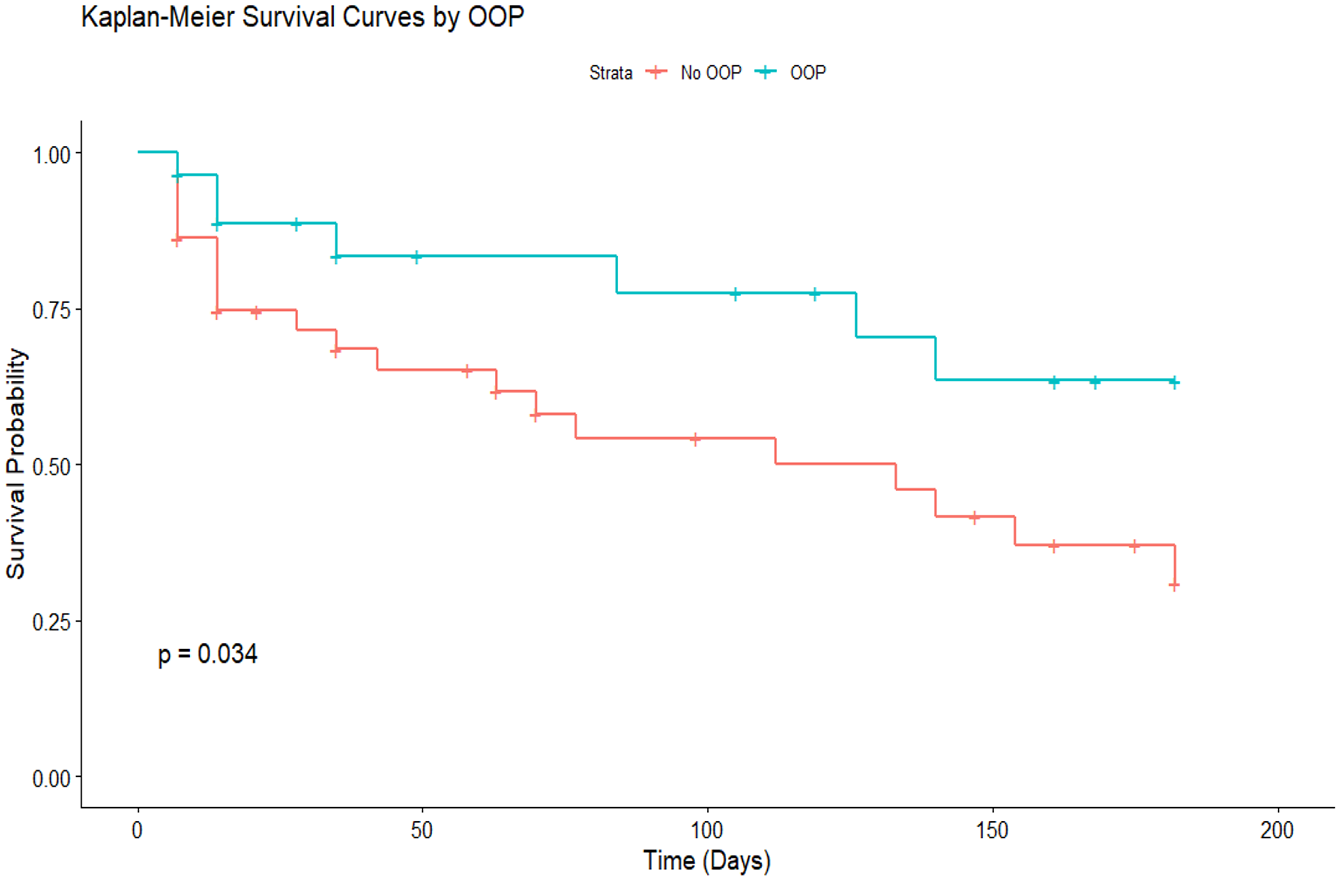
Survival analysis of relapse probability based on out-on-pass status.
Even after adjusting for all other sociodemographic and clinical variables, only granting OOP was associated with improvement in recovery rates and reductions in the hazard ratio (HR) for relapse during the aftercare period, as demonstrated in Table 2.
Cox Regression Analysis of Factors Associated with Relapse Risk.
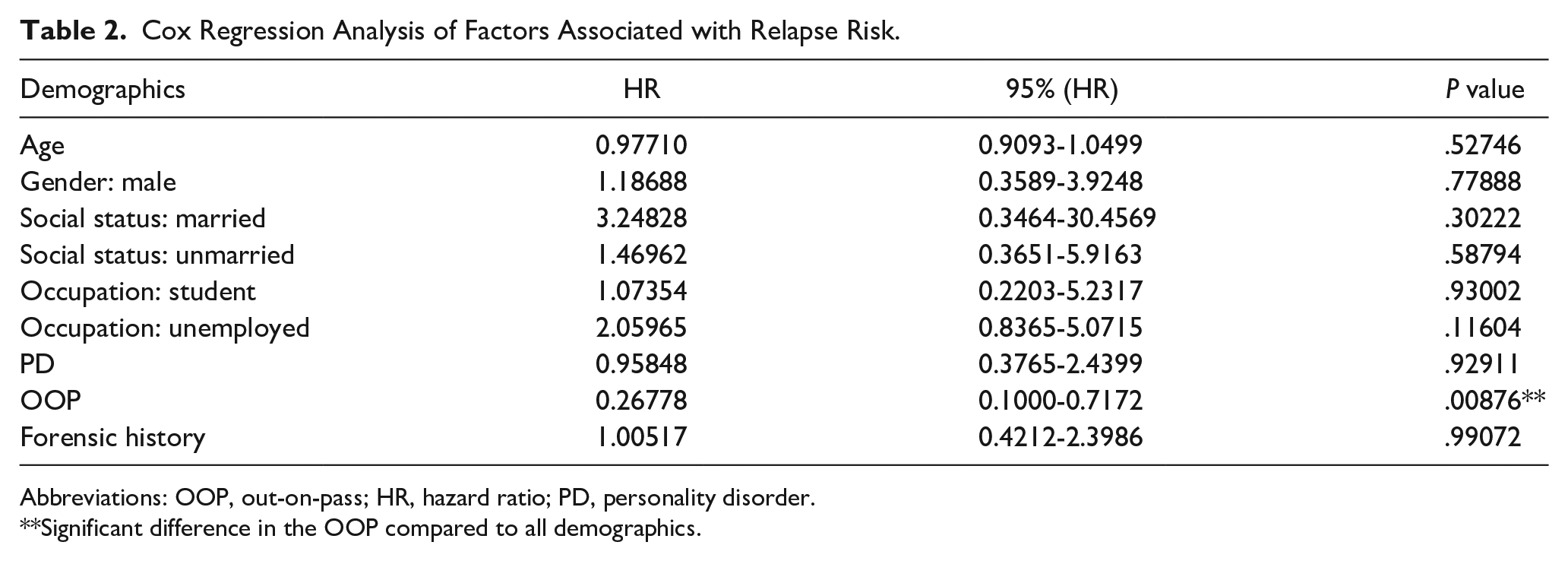
Abbreviations: OOP, out-on-pass; HR, hazard ratio; PD, personality disorder.
Significant difference in the OOP compared to all demographics.
According to our current dataset (HR = 0.27, 95% CI: 0.10-0.72, P = .008), granting of OOP during inpatient treatment of SUD is associated with 73.2% reduction in the post-discharge relapse hazard (95% CI: reduction of 28.3%-90% in HR), indicative of the fact that between 3 and 9 persons out of every 10 will be prevented for potential relapse by granting OOP during the 26 weeks following discharge compared to those not granted OOP as shown in Table 2 (P = .00876).
Secondary objectives
First, we employed a Cox Proportional Hazards nested model with a term for total duration of OOP and another term for the frequency of OOP on time-to-relapse. The frequency of OOP among the group who were not granted OOP was considered 0.
Notably, the mean frequency for OOP was 2 times (ranging between 0 and 20 times). The median was 0. The mean frequency among the patients who relapsed was 0.9 times (compared to a mean of 2.8 times among those who did not). This difference was statistically significant when we used the Wilcoxon rank-sum test (Wilcoxon = 776.5, P = .04391) (Table 1).
However, incorporating time-to-relapse in a more comprehensive Cox Survival model, we noted an HR of 0.842, indicative of a 15.8% reduction in risk of relapse if the frequency of OOP increases by one more time. Nonetheless, the result did not reach statistical significance (P = .0584).
Second, to assess the impact of OOP privileges on the likelihood of relapse following discharge from a rehabilitation center. We employed a nested logistic regression model on the crude relapse/no relapse variable as we assessed the impact of OOP as a predictor of future relapse during the 26-week period. The odds ratio (OR) for the impact of OOP on the predictability of relapse was 0.333 (indicating a 66.7% reduction in relapse risk if patients were granted OOP), 95% CI: 0.118 to 0.942. This was statistically significant (P = .0318).
Discussion
To our knowledge, this is the first study examining the risk of substance abuse relapse in an aftercare setting after discharge from a period of inpatient stay in Qatar. Our data analysis revealed a notable association between OOP privileges and relapse. Patients granted OOP exhibited significantly better recovery trajectories, including a lower relapse risk and a longer median time-to-relapse. By the 26-week follow-up, a substantially higher proportion of OOP patients remained relapse-free (34.5%) compared to the no-OOP group (14%), as shown in Table 3. Furthermore, the survival analysis demonstrated in Figure 1 indicated that patients granted OOP had significantly longer time-to-relapse than those without OOP, an effect which was statistically significant (P = .034), underscoring OOP’s role in promoting sustained recovery during the critical post-discharge period.
Comparison of Relapse Rates Between Patients With and Without Out-On-Pass Privileges.

These findings align with studies supporting progressive reintegration into the community; however, other studies involving psychiatric populations have reported less favorable post-discharge outcomes, such as extended hospital stays, higher rates of psychiatric readmissions, and poor correlation with duration of leave.50,54 Studies supporting living in protective environments, such as the Oxford House model, show reduced relapse rates and improved community involvement.67,68 Like these programs, OOP emphasizes gradual reintegration, allowing patients to practice recovery skills in real-world settings while maintaining clinical support. Yet “sober living houses” or “halfway houses” have yielded variable outcomes depending on patient demographics and treatment settings.69-71 These inconsistencies underscore the need for further investigation to enhance the understanding of the treatment interventions.
Regarding HR in Table 2, the unadjusted relapse rate was higher among patients who did not receive OOP (50%) compared to those who did (25%). Although this difference was not statistically significant, it suggests that factors beyond OOP privileges—such as patient-specific characteristics—could play a critical role in recovery. Nevertheless, after adjusting for sociodemographic and clinical variables, OOP privileges were associated with a significant reduction in the HR for relapse. Specifically, granting OOP privileges was linked to a 73.2% reduction in the relapse HR (95% CI: 28.3%-90%, P = .00876). This adjusted analysis indicates that OOP privileges may reinforce and contribute to long-term recovery while reducing the risk of relapse, regardless of demographic and clinical factors.
In the interpretation of the results from the secondary objective (Table 1), we observed that patients who relapsed had a significantly lower mean frequency of OOP privileges (0.9 occurrences) compared to those who did not relapse (2.8 occurrences), as demonstrated by the Wilcoxon rank-sum test (P = .04391). While the Cox proportional hazards model indicated a 15.8% reduction in relapse risk for each additional OOP privilege, this finding did not reach statistical significance. Taken together, these trends suggest that optimizing the frequency and duration of OOP privileges could provide additional benefits in sustaining recovery. Unlike conventional voluntary step-down programs, the OOP functions as an earned privilege contingent upon treatment progress (Table 1), transforming potential coercion into a motivational therapeutic tool promoting better recovery outcomes (Figure 1). These results may indicate a potential dose-response relationship between the frequency of OOP privileges and relapse prevention, warranting further investigation.
In addition, the nested logistic regression model of relapse likelihood further supported the protective role of OOP privileges against relapse. The OR for relapse among patients granted OOP privileges was 0.333, indicating a 66.7% reduction in relapse risk during the 26-week follow-up period (95% CI: 0.118-0.942, P = .0318). This reinforces earlier findings and emphasizes the importance of incorporating OOP as a predictive factor in relapse prevention strategies.
Notably, this model operates within a legal framework that blends healthcare with judicial oversight. Thus, the positive outcomes observed suggest that even in compulsory treatment environments, OOP can enhance recovery when combined with family engagement and structured supervision. Importantly, the efficacy of OOP within a court-mandated treatment challenges the assumptions that compulsory treatment is less effective, suggesting that structured reintegration can harmonize judicial and treatment recovery goals.
In light of these results, the clinical implications of these findings call attention to the potential of OOP privileges as a therapeutic tool in managing SUD during rehabilitation treatment. However, it is crucial to contextualize these findings within the broader literature, as there is limited research specifically focused on therapeutic leave policies for individuals undergoing residential SUD treatment. Therefore, findings encourage clinicians to integrate structured and monitored OOP privileges into individualized treatment plans to enhance recovery outcomes and lower relapse risks.
Still, a range of confounding variables were not evaluated in the current study, namely, severity of addiction, previous treatment history, medication type, treatment adherence, and strength of family support. Future studies need to include such potential confounding factors in their effect on relapse rates in patients who were granted OOP.
Strengths and Limitations
Despite the promising results, this study has several limitations that should be considered when interpreting the findings. The sample size was relatively small, which may have limited the statistical power of some analyses. The study relied on UDS as the primary measure of relapse; hence, sole reliance on positive urinalysis for a working definition of relapse may not mirror the reality of a patient’s situation. The findings are derived from one specific rehabilitation center, which may have unique practices and culture, thereby limiting broader applicability. In addition, the study lacks randomization, as patients were not randomly selected for the OOP, introducing selection bias, potentially impacting the generalizability of the findings. Another limitation is that the unmeasured social support may overestimate OOP’s effect. Given the nature of SUD patients, patients who relapse will likely not attend for a urinary drug screen. Hence, the probability of missing data will realistically depend on the test result. Data were, therefore, assumed to be non-randomly missing. This is considered a limitation and must be borne in mind when interpreting the results of the study. Finally, the nature of the mandated care might result in patients who are expected to satisfy legal requirements, but the outcomes remain unclear due to the absence of a comparison between voluntary and mandated individuals.
The strength of this study lies in its uniqueness, addressing a topic that is virtually nonexistent in the literature and rarely explored in the context of SUDs.
Conclusion
This study highlights the importance of OOP privileges in reducing the risk of relapse after discharge from mandated treatment care settings. It indicates that such privileges can lead to better recovery trajectories, longer times to relapse, and lower relapse rates for individuals recovering from SUD.
While many studies support the benefits of therapeutic leave and OOP-like privileges in fostering autonomy and improving relapse outcomes, some question their effectiveness. These differing perspectives underscore the need to tailor OOP protocols to meet individual needs and clinical contexts, ensuring they promote recovery without increasing risks or vulnerabilities.
The findings suggest that carefully integrating OOP privileges into treatment protocols for SUD can enhance recovery outcomes.
Further research is necessary to validate these findings, optimize the frequency and duration of OOP privileges, refine guidelines for implementing them in SUD residential treatment programs, and assess their impact on broader recovery outcomes, including quality of life and functional reintegration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open Access funding provided by the Qatar National Library.
Compliance,Ethical Standards,and Ethical Approval
This study, identified under the protocol number (MRC-01-24-380), was approved by the Institutional Review Board of the Medical Research Center at Hamad Medical Corporation on 17 July 2024, ensuring that all aspects of the study comply with ethical standards and regulations.