
Abstract
Objective:
To use the opioid use disorder (OUD) cascade of care to explore the OUD treatment experiences and preferences of pregnant and postpartum people with OUD who experienced incarceration during pregnancy.
Method:
We conducted 12 semi-structured interviews with pregnant and postpartum people with OUD who were either currently incarcerated or in a residential treatment program with experience of perinatal incarceration. The interview guide was developed using a trauma-informed approach and Reproductive Justice framework. Interview transcripts were analyzed using the rigorous and accelerated data reduction technique and a generalized inductive approach with the codebook developed a priori with topical codes from the interview guide and then expanded with interpretive codes.
Results:
We identified themes along the OUD cascade of care. Treatment engagement was shaped by individual readiness and the availability of treatment, both in the community and during incarceration. Medications for opioid use disorder (MOUD) initiation was limited in some instances by the availability of the medication and, in many instances, stigma limited the desire for and ease of MOUD initiation. Participants described potential facilitators (navigation, gender-responsive services) and barriers (lack of mental health care, unmet preferences in terms of treatment format/structure) to retention in care in the community after incarceration. Participants had limited experience with sustained remission and did not identify incarceration as an effective strategy for sustained remission.
Conclusions:
Incarceration is not an effective strategy for sustained remission. Individual, organizational, and structural supports are required to support attempts at recovery that are initiated during incarceration.
Highlights
Themes included readiness, availability, stigma, navigation, and gender-responsiveness.
Incarceration is not an effective strategy for sustained remission.
Incarceration may represent a period of increased readiness for treatment.
Multi-level supports should be strengthened to support recovery, particularly in the transition back into the community.
Introduction
The number of people experiencing the intersection of the perinatal period, opioid use disorder (OUD), and incarceration has increased substantially in recent years, as evidenced by an increasing number of referrals for treatment from the criminal legal system. 1 These incarcerations occur both in jails, where people are incarcerated pre-trial and for short sentences, and in prisons, where people are generally incarcerated for longer sentences. The national prevalence of OUD among pregnant people in prisons in the United States is 26%, and in US jails is 14%, although there is significant geographical variation; at 1 prison in North Carolina, 58% of pregnant people met the criteria for OUD.2,3 Large proportions of pregnant people with OUD become enmeshed in the US criminal legal system as a result of punitive approaches to substance use that emerged from the legacy of racialized regulation of reproduction and family formation.4,5 The perception of some in the criminal legal system that incarceration is an effective way to intervene on OUD in pregnancy further reinforces this cycle.6,7 These approaches necessitate a consideration of the unique treatment needs and preferences of people with perinatal OUD who experience incarceration.
The cascade of care framework developed as a response to the opioid epidemic is effective at conceptualizing the way that people enter treatment for OUD. 8 Starting with a diagnosis of OUD, one is followed by engagement in care, initiation of medications for opioid use disorder (MOUD), retention in treatment for >6 months, and ultimately remission. Overall, the cascade helps to highlight structural and programmatic gaps in service provision. Overlaying the criminal legal continuum, from law enforcement and court interactions, pre-trial detention, jail and prison incarcerations, to community re-entry and probation and parole encounters, onto the OUD cascade, as Brinkley-Rubinstein et al have done, highlights additional levels of complexity facing people with OUD who experience incarceration. 9 Further layering the timeline of pregnancy and postpartum emphasizes the challenges particular to the perinatal period, where incarceration may be relied upon to a greater extent than other facets of the criminal legal system. 6 Figure 1 shows the OUD cascade framework and criminal legal continuum in the context of pregnancy and postpartum.
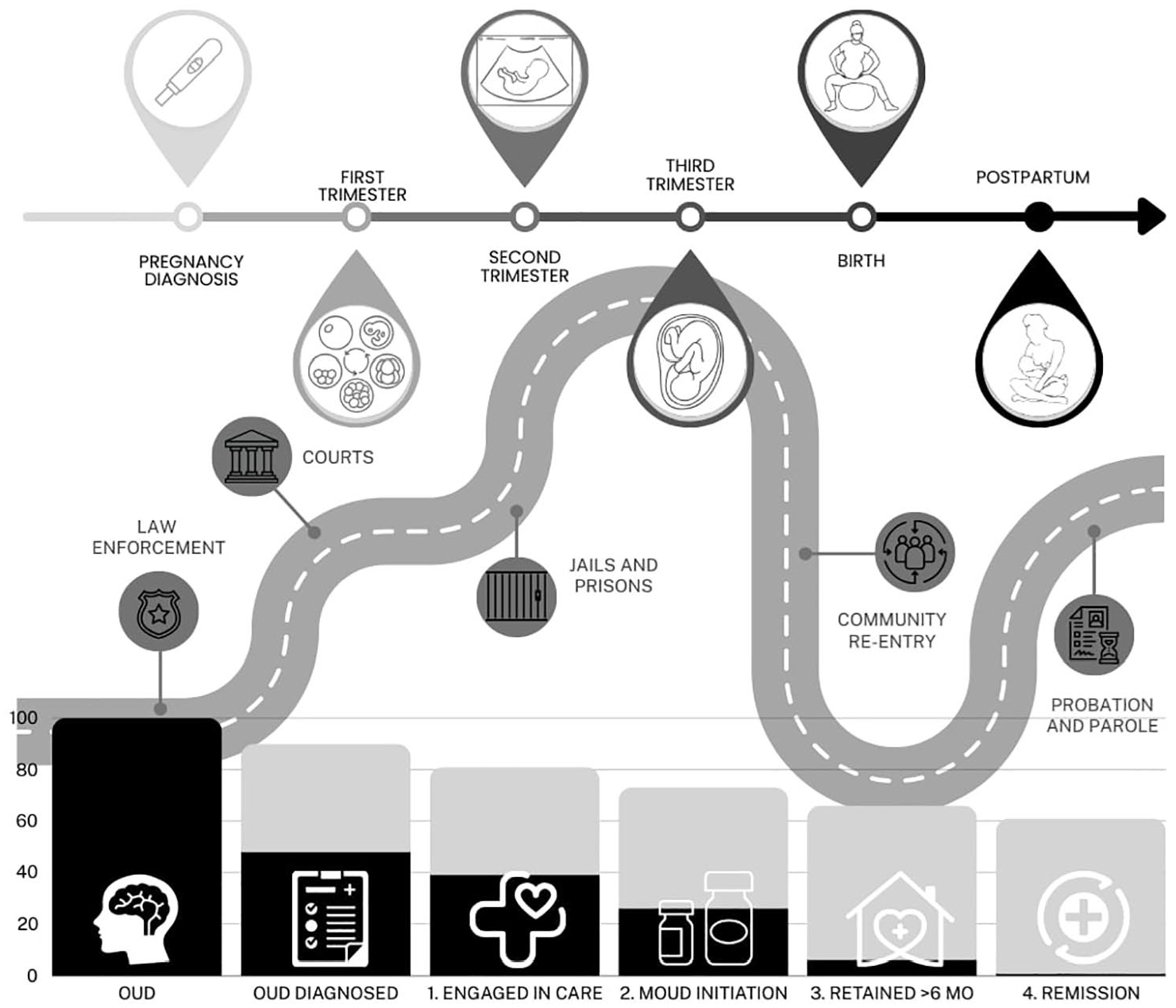
The OUD cascade of care (bottom) is shown as a histogram with light gray bars showing 90% targets of success at each stage and black bars show current estimates based on existing jail and prison data.3,8,10,11 The criminal legal continuum is shown as a winding road through each of the 5 points of contact (law enforcement, courts, jails and prisons, community re-entry, and probation and parole). The pregnancy and postpartum timeline is illustrated with progressive phases of pregnancy, birth, and postpartum. Notably, the linear progress through pregnancy and birth and the often non-linear experience of criminal legal involvement can intersect at any point or at multiple points for a given individual. Additionally, each stage of the OUD cascade of care is implicated throughout pregnancy and in each criminal legal setting.
At each point along the OUD cascade, with each step as a prerequisite for the next, there are gaps in our understanding of how the impacts of incarceration during pregnancy might affect progress. In terms of identification of OUD, pregnant people may be the most likely to be screened during criminal legal involvement, as the health of the pregnancy is a societal priority; they are often also prioritized for referral for MOUD during incarceration. 12 Screening for OUD within the criminal legal system ranges from validated verbal screening tools, 13 to assessing self-report, to urine drug tests, 2 to screening only for acute withdrawal syndromes. 14 Access to OUD treatment varies tremendously geographically and across criminal legal settings. Although behavioral health services for substance use disorders have been described within prison settings,15,16 systematic data on the availability of these services during pregnancy are lacking. About 60% to 80% of carceral facilities provide MOUD in pregnancy, however, only 20% to 50% will initiate treatment if MOUD was not already prescribed in the community.2,10
Treatment is rarely, if ever, continuous from the community into carceral facilities and back to the community. In one sample from a North Carolina prison, approximately 30% of pregnant people with OUD were receiving MOUD before incarceration. 3 Although continuation of MOUD in jails and prisons is increasingly the standard of care, approximately one-third of US facilities still manage OUD during pregnancy using withdrawal.2,10 Challenges with housing, transportation, employment, and medical care all complicate retention in OUD treatment following incarceration. 17 Beyond these competing priorities, the common practice in prisons and jails of withdrawal of MOUD postpartum results in discontinuity of treatment and may also introduce negative associations with MOUD that decrease enthusiasm for re-initiation.2,10,18,19 Continuity of care may also be prioritized or offered only to those who will still be pregnant when they return to the community. 3
Treatment needs and preferences of pregnant and postpartum people returning to the community following incarceration have not been examined in the literature. In this qualitative study, we aimed to explore the OUD treatment experiences and preferences of pregnant and postpartum people with OUD who experienced incarceration during pregnancy.
Methods
Eligibility
Eligible participants were 18 years old or older and met the clinical criteria for OUD. Our study did not have exclusion criteria based on gender, race, or ethnicity.
Setting
We recruited participants from 2 settings: a perinatal substance use disorder treatment program located in North Carolina and the prenatal clinic at the North Carolina Correctional Institute for Women (NCCIW) in Raleigh, North Carolina, a part of the state prison system. Both methadone and buprenorphine were available during pregnancy at NCCIW during the study period, although facility protocol dictated withdrawal of these medications postpartum if the individual remained incarcerated. 3 Statutes in North Carolina make it possible for jail facilities to send individuals requiring care beyond the capacity of the jail to the state prison system; this occurs with some frequency, so pregnant individuals seen in the NCCIW clinic represent a mixture of people awaiting trial, serving short jail sentences, and serving longer prison sentences. Participants in the treatment program had experienced perinatal incarceration with either a prison or jail in North Carolina.
This research study was approved by the Institutional Review Board (IRB #20-3559 and #21-2040) at our institution and the North Carolina Department of Adult Corrections Prison Research Review Committee (HS #2107-01).
Recruitment and Enrollment
Participants were recruited between September 2021 and April 2022. The study team presented the study to several group sessions at the treatment program and provided NCCIW clinic nurses postcard-sized flyers to share with all pregnant or postpartum individuals presenting at the prenatal clinic. In order to maintain privacy in both settings, we did not track the number of people who were informed about the study. Participants provided verbal consent following an informed consent discussion. Participants from the treatment program were given a $50 gift card for their participation. Participants at NCCIW did not receive incentives due to prison policy.
Interviews and Safety Monitoring
A female-identified, certified doula and childbirth educator with extensive qualitative interview experience used a scripted interview guide and conducted the interviews via Webex/Zoom. NCCIW did not permit recording of the interviews so 2 additional team members took notes anonymously and off-video. Interviews lasted about an hour. The interviewer was equipped to provide emotional support and referrals when needed. The interview guide was created using a trauma-informed perspective 20 and a Reproductive Justice theoretical framework. 21 We chose these frameworks in recognition of the fact that all people who have experienced incarceration experience trauma and also experience the systematic societal devaluing of their reproductive capacity through limitations on their rights to give birth and parent in safe environments, in addition to and as a result of their incarceration. 4 By incorporating person-first language, frequent check-ins with verbal consent to continue the interview, explicitly framing the participant as the subject expert, and emphasizing strengths, among other strategies, our goal was that the interview guide would implicitly affirm participants’ contributions to the research and to their families and society.
Data Analysis
The interview transcriptions were contemporaneous notes, with an emphasis on verbatim documentation of participant responses. The interview guide was reviewed after 4 interviews. As no major changes were made, the pilot interviews were included in our total sample. We used the rigorous and accelerated data reduction (RADaR) technique. 22 The RADaR technique can be used with any theoretical framework. Briefly, this method entails reducing transcribed interview data to excerpts relevant to the research question within an Excel spreadsheet 23 and applying codes to those excerpts, organizing the excerpts according to the codes, and then reducing the interview data again to identify illustrative quotes for each code. Using a generalized inductive approach, the codebook was developed a priori with topical codes from the interview guide and then was expanded with interpretive codes identified during open coding of initial interviews. Each interview was coded independently by 2 to 3 coders, and disagreements were resolved through discussion. Members of the research team drafted an overarching thematic framework, which was revised through discussion with the entire research team until inductive thematic saturation was reached. 24 While we conducted as many interviews as were feasible during a study period complicated by pandemic precautions, we did find that we reached a high degree of data saturation, meaning that subsequent interviews began to echo prior transcripts. 24 Pseudonyms were assigned to all participants for attribution in the text. We report demographic information about the participants but have not reported any subgroup sizes of 3 or smaller to limit the risk of deductive disclosure.
Results
In total, we conducted 12 interviews (6 at NCCIW and 6 at the treatment program). All participants identified either as female or non-binary. The majority self-identified as White and non-Hispanic/Latina (n = 8) and smaller numbers as Black/African American, Hispanic/Latina, or Asian. The majority experienced incarceration during pregnancy (between 16 and 37 weeks gestational age), rather than postpartum, in either a jail, prison, or both. Most participants had also experienced incarceration previously (average 3 prior incarcerations, range 0-6+). Participants had an average of 2 children (range 1-5) and experienced an average of 11 weeks of perinatal incarceration (range 1-25 weeks).
Themes were identified describing participants’ perspectives on the barriers and facilitators to engagement, availability of MOUD and stigma associated with MOUD initiation, participants’ prior experiences with treatment in the community, and their aspiration toward remission despite limited experiences with sustained recovery. Since injectable naltrexone and injectable buprenorphine were not recommended in pregnancy at the time that the interviews were conducted, participant comments about MOUD focused on methadone and sublingual buprenorphine. Participants also described the types of treatment services they would like to have received or believed would be useful for others. We did not identify substantive differences by setting; while some of our participants interviewed in the prison setting expressed thoughts about the transition to the community that were more hypothetical, the majority were also able to draw on their prior experiences of incarceration in responding to the interview prompts. Table 1 and Figure 2 show the identified themes organized according to the OUD cascade.
Themes and Associated Codes From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022.
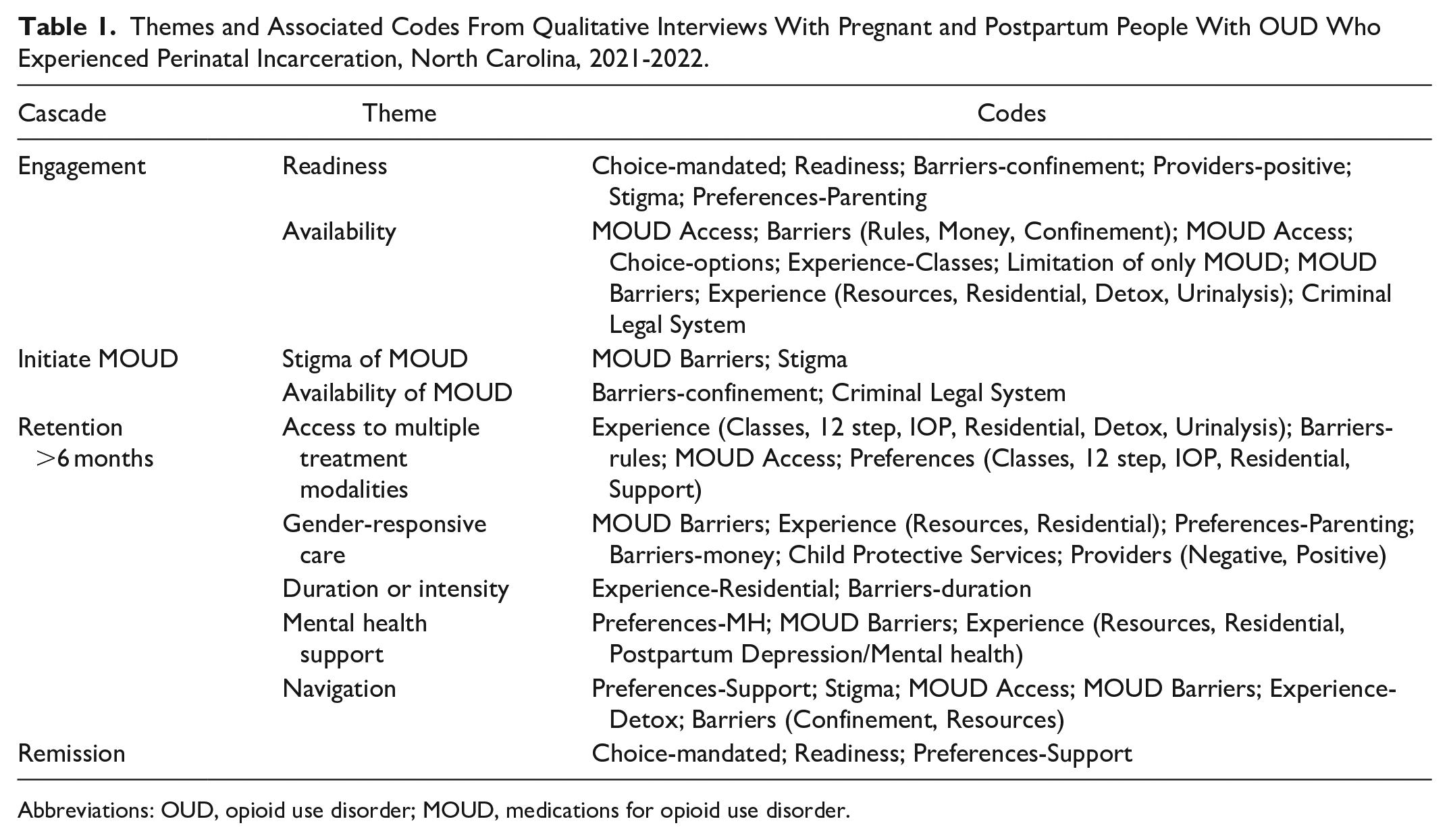
Abbreviations: OUD, opioid use disorder; MOUD, medications for opioid use disorder.
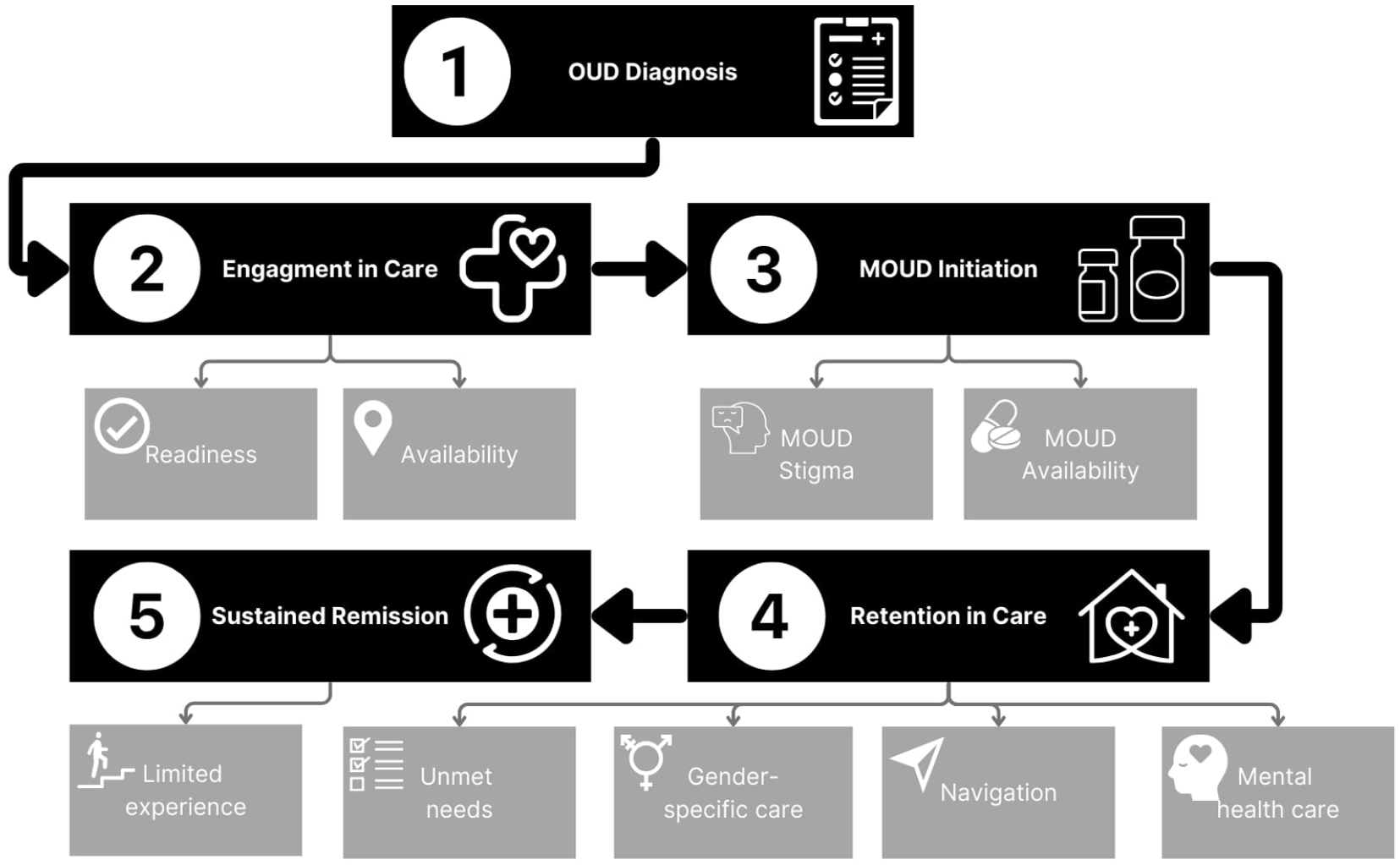
Identified themes from qualitative interviews with pregnant and postpartum people with OUD who experienced perinatal incarceration, organized according to the OUD cascade of care, North Carolina, 2021-2022. Although aspects of some themes appeared at multiple steps (eg, individuals talked about the need for parenting-specific resources such as childcare for MOUD initiation, in addition to the broader theme of gender-specific care discussed in the context of retention in treatment), they are placed in the figure based on their predominant context in the interviews.
Engagement in Treatment
Participants described past attempts to engage in recovery from substance use disorders. When discussing engagement, 2 themes dominated: their individual readiness for abstinence, and the availability and accessibility of treatment options in their community.
Readiness
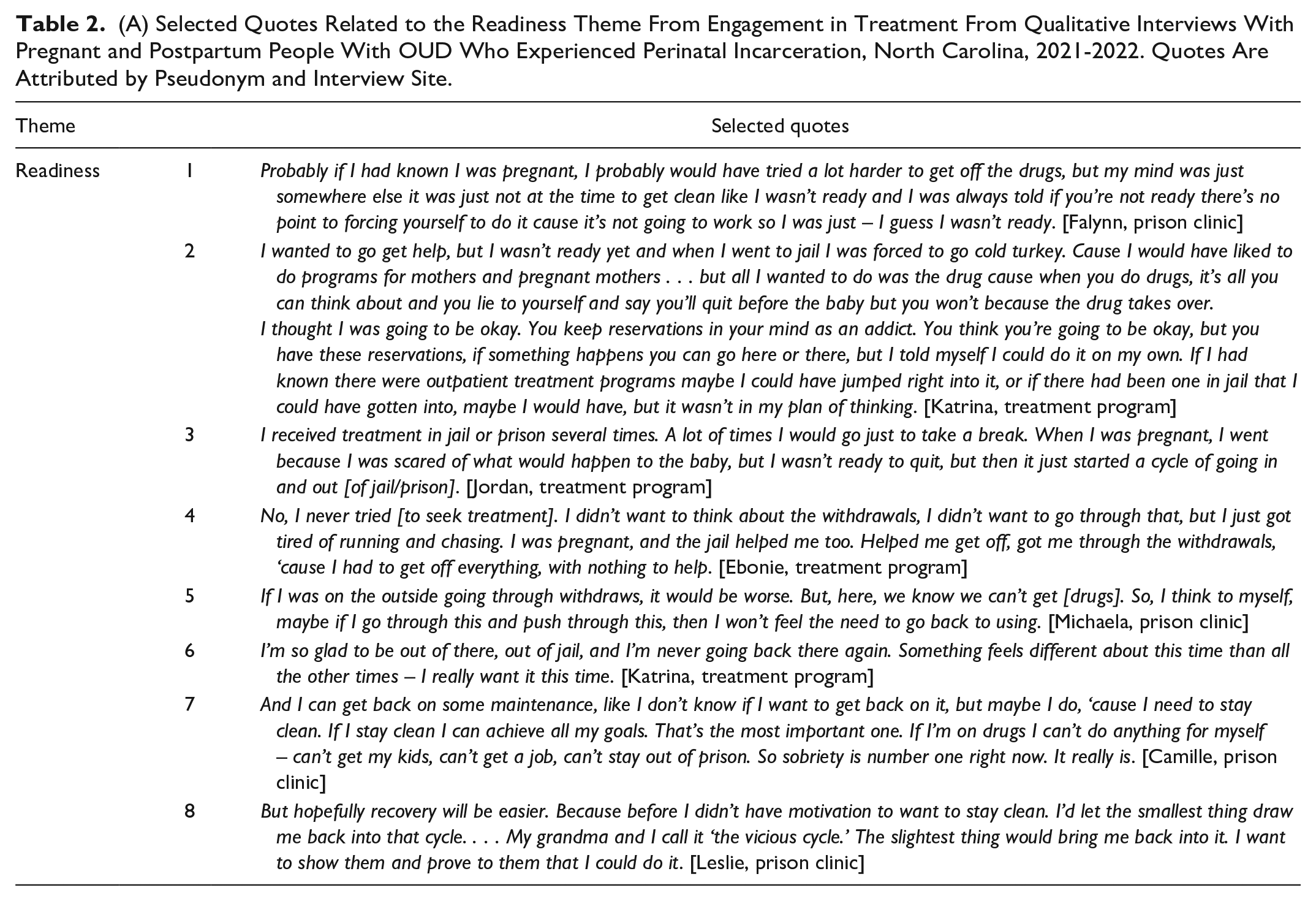
Participants iterated the belief that treatment attempts are unlikely to be successful unless the individual has some degree of readiness or commitment to sobriety. The idea of readiness was often used by participants as a way of constructing a recovery narrative that predicted their current or future success at recovery. In the description of past failed attempts to achieve lasting recovery, participants talked about being unready (Table 2A: 1). In some cases, including for Katrina (treatment program, full quote Table 2A: 2), lack of readiness was described as a reservation to treatment. “I wanted to go get help, but I wasn’t ready yet and when I went to jail I was forced to go cold turkey.” Some participants described incarceration as a place where detoxification or sobriety could predictably be achieved—at least temporarily—with or without readiness for treatment (Table 2A: 3-5). Readiness was also described as a kind of motivation for treatment and a reason for hope (Table 2A: 6 and 7). “But hopefully recovery will be easier. Because before I didn’t have motivation to want to stay clean” [Leslie, full quote Table 2A: 8].
(A) Selected Quotes Related to the Readiness Theme From Engagement in Treatment From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022. Quotes Are Attributed by Pseudonym and Interview Site.
(B) Selected Quotes Related to the Availability Theme From Engagement in Treatment From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022. Quotes Are Attributed by Pseudonym and Interview Site.
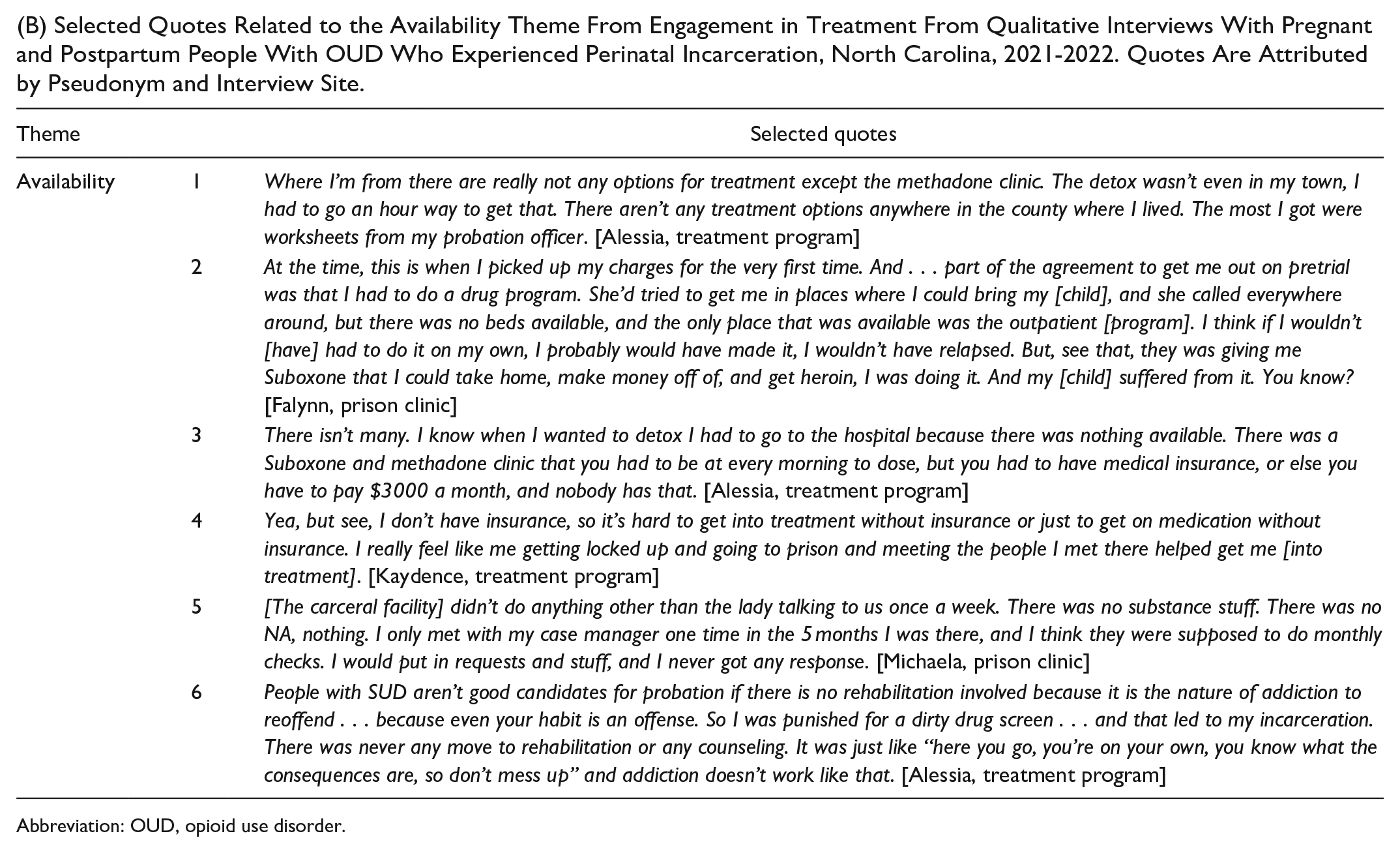
Abbreviation: OUD, opioid use disorder.
Pregnancy or motherhood was also mentioned often as the source of this motivation and readiness, including “I know I’ll do good ‘cause the motivation is my baby. That’s my number one priority. . .” [Blake] and “When I’m in active addiction I don’t want to be alive. . .So having [my baby in treatment] gave me something to live for” [Dakota]. Although participants did describe structural challenges to accessing treatment while pregnant or parenting, these ideas were generally not directly linked to the readiness or motivation that a new baby might provide.
Availability
Although most participants had pursued or engaged in community-based treatment services prior to incarceration, there were no instances where participants reported that incarceration interrupted a productive trajectory of treatment engagement. A lack of available or desirable services was repeatedly cited as a reason for failure to engage or remain engaged in treatment services, such as Alessia’s stating “The detox wasn’t even in my town, I had to go an hour way to get that.” Or as Falynn described a prior attempt at entering treatment, “but there was no beds available” (full quotes Table 2B: 1 and 2). Lack of health insurance was also presented as a barrier to treatment (Table 2B: 3).
For 1 participant, incarceration was seen as a vehicle for accessing treatment in the absence of health insurance (Table 2B: 4), but treatment was not depicted as readily available in incarcerated settings by other participants. For example, Michaela said “[The carceral facility] didn’t do anything other than the lady talking to us once a week. There was no substance stuff. There was no NA, nothing” (full quote Table 2B: 5). Neither did participants consistently view community supervision as an effective way to access treatment services. One participant suggested, “People with SUD aren’t good candidates for probation if there is no rehabilitation involved because it is the nature of addiction to reoffend. . . and that led to my incarceration. There was never any move to rehabilitation or any counseling” [Alessia] (full quote Table 2B: 6).
Overall, participants described a non-linear trajectory of SUD recovery: cyclical in episodes of both treatment and incarceration. Pregnancy was described as a motivator in episodic feelings of readiness, yet the inaccessibility or insufficiency of treatment programs, both in the community and in carceral settings, was given as an impediment to continued engagement or recovery success.
Initiation of MOUD
Layered onto the many barriers to engagement with treatment, participants also shared specific challenges related to initiation of MOUD—stigma due to MOUD and lack of availability of MOUD.
Stigma and MOUD
Many participants talked about facing stigma related to substance use in pregnancy, generally, both during incarceration and afterward. For some, this included judgment by oneself and by others related to the incorrect interpretation of buprenorphine treatment as another addiction or substitution of one drug for another. For example, Leslie said, “I’d feel bad starting something that I want to stop – starting that vicious cycle” (full quote in Table 3: 1). One participant expressed her dismay at being derided by the facility staff for receiving MOUD which would be discontinued if she were to give birth while she was incarcerated (Table 3: 2). These stigmatizing attitudes and beliefs are contrary to the evidence that MOUD significantly improves outcomes in pregnancy and postpartum and decreases the risks of returning to use, of overdose, and of death. 25
Selected Quotes Related to Initiation of MOUD Themes From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022. Quotes Are Attributed by Pseudonym and Interview Site.
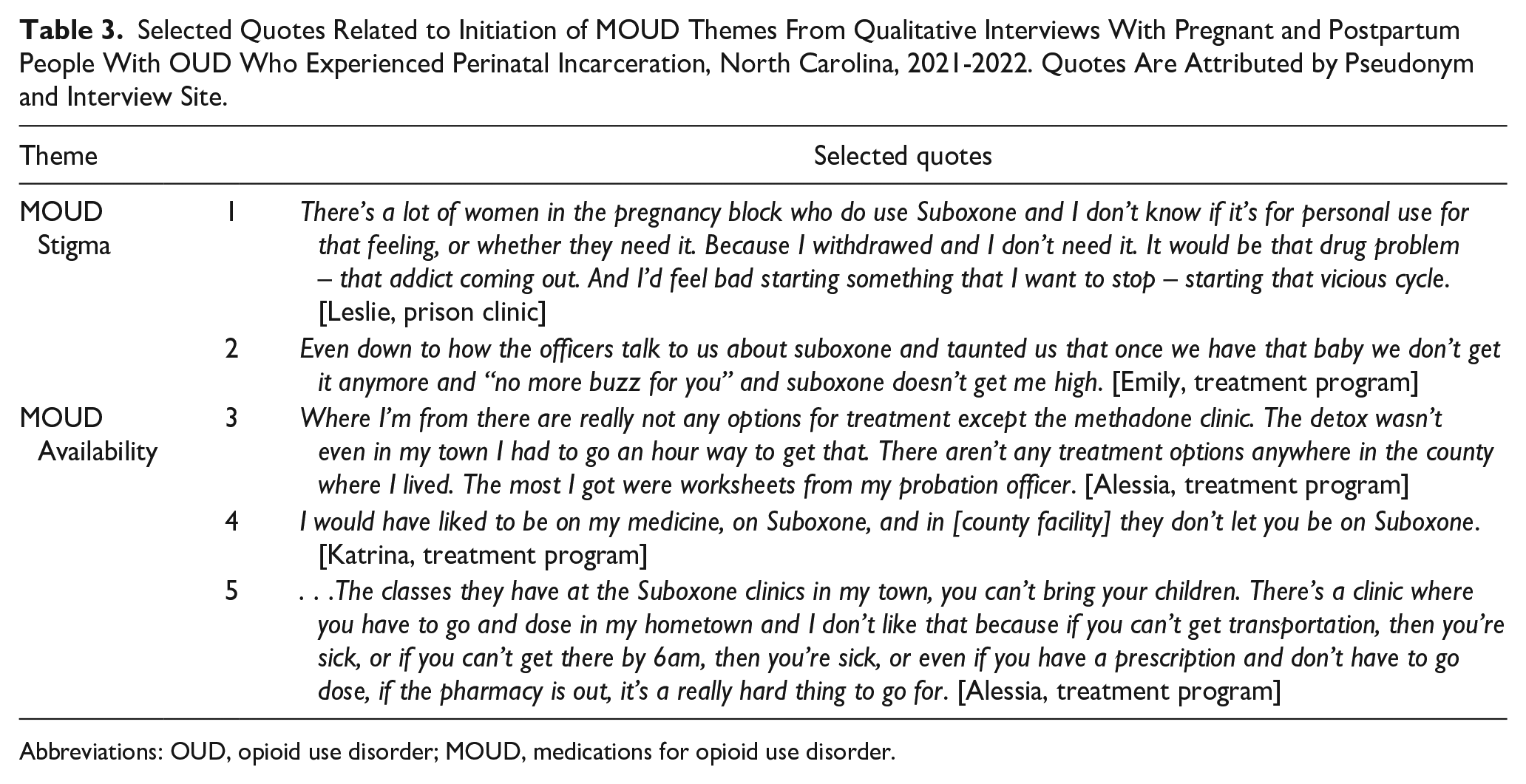
Abbreviations: OUD, opioid use disorder; MOUD, medications for opioid use disorder.
Availability of MOUD, But Little Else
Participants’ experiences with trying to access MOUD were bimodal, with one group of participants reporting easy access and another describing difficulty. Many of those who reported straightforward access MOUD expressed frustration that other behavioral health services were not available in the same setting, stating “Where I’m from there are really not any options for treatment except the methadone clinic” [Alessia, full quote Table 3: 3]. Another participant shared, “. . .some doctors write scripts for suboxone but there is only real help for addictions in bigger cities like Raleigh, Wilmington, Durham, etc” [Falynn].
Those who described difficulty accessing MOUD identified barriers including practical issues like insurance coverage and childcare, and carceral facility policies interfering with MOUD (Table 3, line 4). Kaydence shared, “Yea, but see, I don’t have insurance, so it’s hard to get into treatment without insurance or just to get on medication without insurance.” Alessia emphasized transportation and childcare as barriers (Table 3: 5).
Retention in Treatment
Many of the participants shared reflections on the factors that prevented them from continuing treatment and specific interventions they believed would improve their ability to stay in treatment in the future. Some participants highlighted these needs by identifying gaps in what was available during incarceration, while others contrasted their desires and preferences with what they accessed previously in the community. Some participants also highlighted the importance of retention in treatment (Table 4: 1 and 2).
Selected Quotes Related to Retention in Treatment Themes From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022. Quotes Are Attributed by Pseudonym and Interview Site.
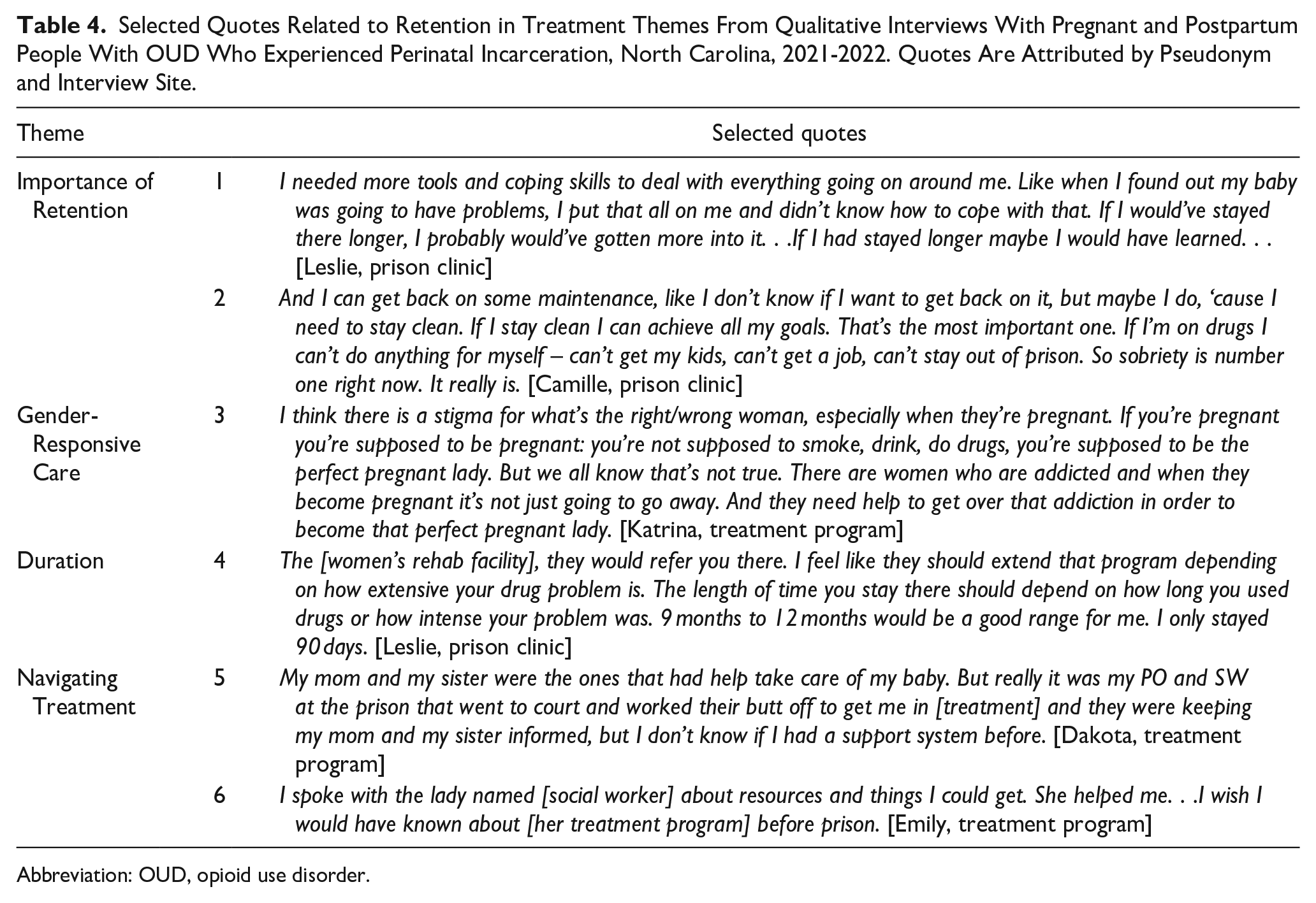
Abbreviation: OUD, opioid use disorder.
Access to Multiple Treatment Modalities
Participants described diverse formats and content preferences, which included a desire for supportive housing, individual counseling, 12-step meetings, and classes focused on parenting, coping skills, and building healthy relationships. Reflecting on treatment modalities during incarceration, Blake said, “I wish we could have like a group counseling session,” while Dakota reported, “There’s no NA groups or access to the NA book; I asked and asked but nobody had one. There’s no religious services or anything like that, you’re just stuck in a cell.” Other participants commented on the effects of the COVID-19 pandemic in the community, including Emily, “Because of the pandemic, they don’t do AA or NA meetings. I personally enjoy AA/NA meetings. I’ve been in addiction for 17 years and I’m only 32. And when I don’t have anyone to reach out to, I can call people in 12-step.” Regarding treatment in the community, Leslie said, “They should do more one-on-one rather than group sessions because people were afraid to speak up about their problems or the source.”
Gender-Responsive Care
Multiple participants identified that a lack of support specific to women was a barrier to committing to treatment. In addition to the pregnancy- and parenting-specific material resources identified above, 1 participant described the need for treatment programs to address stigma related to gender and pregnancy status, “I think there is a stigma for what’s the right/wrong woman, especially when they’re pregnant. . .And they need help to get over that addiction in order to become that perfect pregnant lady” [Katrina, full quote Table 4: 3]. Another participant described the need for treatment that addresses parents’ interpersonal relationships, saying, “Every interaction you have with your spouse is altering that newborn’s brain because it’s growing. So you need gender-specific treatment for fathers and mothers” [Alessia]. Only 2 participants discussed the role of infant custody as a potentially coercive element of treatment retention related to parenting, similar to the way that incarceration might increase initiation with or without readiness. Emily stated, “. . .if you go to the program in [CITY], you sign a contract and say they’re stepping in for CPS, but if you leave the program CPS will step in, so that’s a forced thing.”
Duration or Intensity of Treatment
Some participants shared that some residential programs did not offer adequate flexibility in duration. For example, “I feel like they should extend that program depending on how extensive your drug problem is. The length of time you stay there should depend on how long you used drugs or how intense your problem was” [Leslie, full quote Table 4: 4].
Mental Health Support
Multiple participants discussed the importance of concomitant mental health treatment and the potential for perinatal or postpartum mood and anxiety changes to affect OUD. For example, Camille shared, “I feel like if I have more mental health treatment, it would help drug addiction. The mental part of my drug addiction. Many times, I’ve relapsed in the past cause I haven’t been on the right mental health meds. I’m not blaming it on that entirely, but it plays a big part.” Several participants discussed the lack of mental health support during incarceration, for example, “Unless you’re like super crazy it’s hard – there’s a waiting list to see the psychiatry staff in there. . .[Therapy] helped, I’ve had a lot of stuff happen to me in my life. I feel like talking about it would have helped” [Kaydence]. The same participant also described her positive experiences with mental health care in a community-based treatment program, “I like the fact I can Zoom or call my therapist within reasonable hours.”
Navigating Treatment
Figuring out the next steps for treatment was another barrier to retention, particularly for participants who engaged with treatment initially during incarceration. Participants who reported successful navigation often identified key individuals in the process, such as Dakota (“. . .But really it was my PO and SW at the prison that went to court and worked their butt off to get me in [treatment]. . .”) and Emily (“I spoke with the lady named [social worker] about resources and things I could get.”) (full quotes in Table 4: 5 and 6).
Other participants described feeling like they didn’t know where to go to continue treatment. For example, Katrina said that if someone in the jail had been able to help, she would have “jumped into [treatment]. . .But they didn’t, so I didn’t have a plan.” Alessia also described her experiences without someone to help navigate, “It was just like ‘here you go, you’re on your own, you know what the consequences are, so don’t mess up’ and addiction doesn’t work like that.”
Remission
Participants expressed motivation and readiness for recovery at the time of the interview. Particularly among incarcerated interviewees, the readiness they described was aspirational, with limited past experiences of sustained recovery. For example, Camille described wanting to try recovery again, “I want to go to treatment. I was in rehab before, and it was very helpful. I took it very serious and I want that again, I need that again. Even after being locked up. I need it there.”
Of the participants in the community and in the prison setting, none described sustained remission of their substance use disorder. Instead, incarceration was mentioned as a strategy to interrupt a period of active use or initiate a recovery attempt, but not as an effective strategy for sustained remission. Dakota reported, “And it wasn’t until I relapsed and went to prison that I got any help because in jail they didn’t ask me any questions if I had any help or anywhere to go or offer any help. . .” (full quote, Table 5: 1). Participants identified treatment in carceral settings as limited and insufficient with the transition into the community characterized by a lack of support, leading to a high risk of relapse or reversion to previous behaviors.
I had been told that when you go to jail there’s a case manager for you, but I never met with a case manager. If that were a thing, if someone could have shared some resources with me and helped me come up with a different game plan for after I left, that would have helped and prevented some issues that came up later on. . . [Alessia, full quote, Table 5: 2]
Selected Quotes Related to Remission Themes From Qualitative Interviews With Pregnant and Postpartum People With OUD Who Experienced Perinatal Incarceration, North Carolina, 2021-2022. Quotes Are Attributed by Pseudonym and Interview Site.
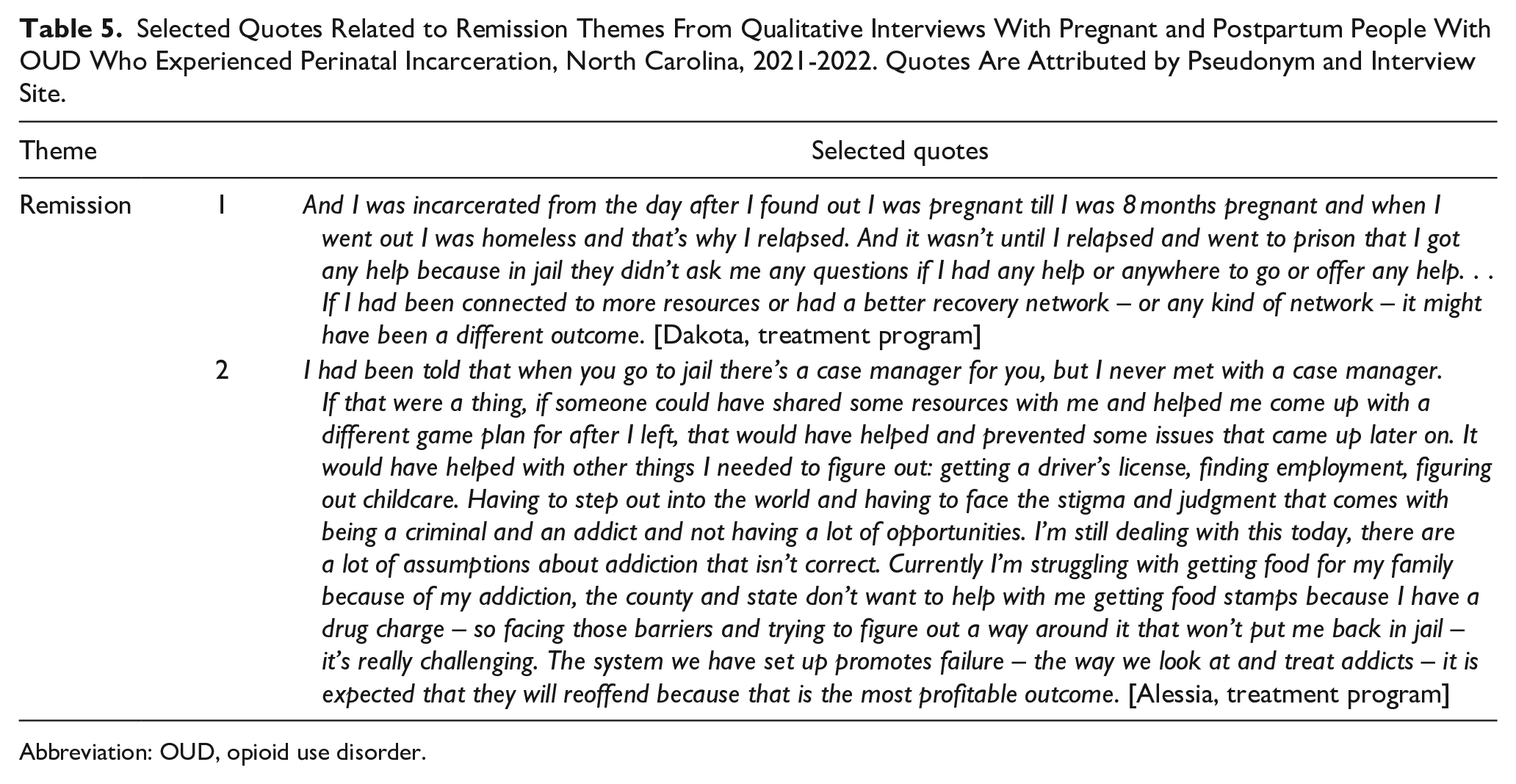
Abbreviation: OUD, opioid use disorder.
Discussion
This qualitative analysis of interviews with pregnant and postpartum people with OUD who experienced incarceration during pregnancy identified several themes at each stage in the OUD cascade of care. Notably, incarceration for our participants did not disrupt a productive trajectory of treatment engagement but was one of many factors shaping the non-linear experience of navigating OUD. Participants identified readiness for treatment and the availability of treatment as important determinants for engagement with care. MOUD initiation, in some instances, was limited by availability and, in many situations, the desire for and ease of MOUD initiation was limited by stigma. Participants described potential facilitators (system and care navigation, gender-responsive services) and barriers (lack of mental health care, unmet treatment format/structure preferences) to retention in care. Finally, participants had limited experience with sustained remission and did not identify incarceration as an effective strategy for sustained remission.
Our findings add depth and richness to the existing literature characterizing the OUD cascade of care in the context of incarceration for a perinatal population. Beginning with engagement with treatment, participants with OUD and perinatal incarceration identified readiness and accessibility as key determinants. Readiness, or the motivation to change, has been described in the psychological literature as a characteristic or state that might promote therapeutic change. 26 Although readiness has been correlated with engagement in some smaller studies, 27 larger studies have not borne this out. 28 For participants in this study, it may be that the drive to create and share optimism about recovery from OUD and returning to the community was the basis for the emphasis on readiness, particularly readiness at the time of the interview compared with in the past.29-32
Treatment availability limitations identified in this study are consistent with other research. Beyond the potential effects of limited personal resources for accessing community-based treatment, there are long-standing geographic disparities in OUD treatment access that, despite some improvement in recent years, disproportionately affect those with public insurance 33 in the Southeastern United States and in rural areas.34,35 Additionally, there are substantial gaps in OUD treatment in carceral settings, including inadequate rates of MOUD provision,2,3,10 geographical and facility differences in methadone versus buprenorphine use10,36 and very limited behavioral health services.15,16 The theme of stigma as a barrier to MOUD initiation is also not unique, with a systematic review identifying clinician, peer, societal, and regulatory stigma as barriers to MOUD initiation. 37
Unlike prior literature describing competing priorities as primary barriers to retention following incarceration during pregnancy, 17 we found gaps in services or unmet treatment needs. This may stem from our participants being interviewed either during incarceration, before the competing priorities in the community felt salient, or while in a residential treatment program, where many of those competing priorities were addressed by the program. It is notable that these gaps or unmet needs are not exclusive to retention in care but instead capture more nuanced dimensions of overall treatment availability and accessibility of MOUD. However, at these earlier steps in the OUD cascade of care, the more glaring absence of any OUD treatment clinicians in some geographical areas or in jails and prisons rendered less obvious the specific treatment needs of pregnant and postpartum people with OUD and incarceration experience.
This qualitative study has limitations. Our data come from a relatively small qualitative sample of people with OUD who experienced incarceration during pregnancy with the purpose of generating hypotheses and exploring theoretical underpinnings. This limitation is mitigated somewhat by the fact that our sample demographics largely mirrored the demographics of the population of pregnant people with OUD imprisoned in our state. 3 We did not have sufficient data, however, to delve into differences in experience by facility type (ie, jail vs prison). Identifying distinct trajectories based on specific incarceration experiences when using any qualitative may be complicated, given that this population bears a disproportionate burden of incarceration, and thus has accrued a diversity of experiences in jail and prison facilities during pregnancy, postpartum, and during other periods of their lives.
Another limitation is that because half of the interviews were conducted inside a state prison facility participants may not have shared some experiences, even though substantial precautions were taken to ensure participant privacy and confidentiality. Some participants did state that, newly starting a new recovery journey during incarceration, their minds were “clear,” and they felt comfortable talking with our study team. Participants affirmed that they would have chosen to participate even if they had not been incarcerated, due to their desire to share their stories, help others, and advocate for change. 38
In conclusion, our findings suggest points of intervention to support progress along the cascade of care. First, reducing criminal legal system contact for pregnant people is critical, but for those individuals who do experience incarceration, this may be a period of increased readiness for treatment. Improving access to behavioral health services and MOUD during incarceration would leverage this readiness. Broad efforts to increase OUD treatment and MOUD access in the community are also important. Second, individual psychoeducation as well as stigma-mitigation interventions hold the potential to increase MOUD initiation. Third, policy interventions that increase access to case management, mental health care, and gender-responsive OUD treatment during incarceration and in the community are likely to improve retention. Although incarceration does not represent an effective strategy for sustained remission for opioids, recognizing it as a setting in which recovery attempts may be initiated reinforces the need to strengthen the individual, organizational, and structural supports required to sustain that attempt, particularly in the transition back into the community.
Footnotes
Acknowledgements
The authors would like to acknowledge Timelie Horne, Joia Freeman, Hendree Jones, Kim Andringa, Senga Carroll, Dr. Elton Amos, and the prenatal clinic nursing staff at the North Carolina Correctional Institution for Women for their invaluable contributions, without which this research would have been impossible.
Author Contributions
Dr. Knittel acquired funding, conceptualized the study, supervised data collection, led the analysis, the writing of the original draft, and review and editing of the manuscript. Ms. Black and Ms. Kerr participated in the data analysis and writing the original draft. Ms. Bazemore and Ms. Reddy participated in the data collection, the data analysis, and writing the original draft. Ms. Jackson led the data collection, participated in the analysis, and writing the original draft. Dr. Martin participated in the data analysis and review and editing of the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute of Child Health and Human Development (NICHD) (Knittel, K12HD103085, PI Neal-Perry). Ms. Kerr’s time was supported by the North Carolina Diversity and Inclusion Pathway Program, a part of the University of North Carolina at Chapel Hill Center for AIDS Research (P30AI050410). Dr. Martin’s time was supported by the National Institute on Drug Abuse (K23DA053507).
Compliance,Ethical Standards,and Ethical Approval
This research study was approved by the Institutional Review Board (IRB #20-3559 and #21-2040) at our institution and the North Carolina Department of Adult Corrections Prison Research Review Committee (HS #2107-01). Individual participants gave verbal informed consent to participate in the research.
Data Availability Statement
Due to the sensitive nature of the data, it is not publicly available. Researchers interested in working with the data may contact the lead author (Dr. Knittel,
Preprints
A version of manuscript was presented at the Academic Consortium on Criminal Justice Health conference in Phoenix, AZ, April 2024.