
Abstract
Background:
People who inject drugs (PWID) may develop skin and soft tissue infections because of limited access to sterile injection supplies and education regarding safer injection techniques. The purpose of this study was to assess wound care experiences, knowledge, and practices among individuals accessing community-based services and inform service provision for PWID.
Methods:
Using convenience sampling, participants of an organization that engages with PWID in Austin, Texas, were engaged in a multiphase mixed-methods study. Phase 1 (N = 39) included completion of a 23-item quantitative survey; eligibility required injection drug use in the past 30 days. Phase 2 (N = 20) included brief semi-structured interviews to explore wound care practices. Participants received $20 grocery store gift cards for participating in each phase. Qualitative data were analyzed using an analytic matrix to identify themes.
Results:
PWID reported injecting methamphetamine, heroin, and fentanyl; 53.8% (21/39) injected more than 1 substance. The same proportion (21/39) had experienced at least 1 injection-related wound in the past 6 months and reported often or always self-treating injection-related wounds. Their reasons included confidence in self-treating, lack of perceived wound severity, and experience of stigma. Interview participants described their experiences with infections, how they cleaned wounds and obtained antibiotics, how they decided when to seek medical care (eg, wound severity, confidence in self-treatment), and barriers to seeking care (eg, stigma, financial concerns).
Conclusions:
Needs for wound care treatment and education among PWID are currently unmet, and stigma from health care providers remains a challenge to seeking early intervention for infections. Delivering wound care services and education through community-based organizations that have established credibility and connection may enhance access to care.
Highlights
People who inject drugs (PWID) in Austin, Texas, are likely to experience injection-related wounds and typically attempt self-treatment while avoiding care from conventional health care professionals.
Embedding licensed health care professionals in community organizations that engage with PWID, or providing basic wound care and triage training to paraprofessionals in these organizations, may improve outcomes.
Introduction
People who inject drugs (PWID) are at high risk of developing skin and soft tissue infections (SSTIs) with an estimated prevalence of 44%.1,2 Risk factors for developing SSTIs include non-sterile injection techniques and supplies, injecting subcutaneously or intramuscularly instead of intravenously, repeated injections at the same site, larger needles, unstable housing, and poor nutritional status.1,3,4 PWID avoid seeking medical care after developing an infection because of confidence in their ability to treat the wound; preference for self-treatment; perceived lack of severity of the wound; and other barriers to seeking medical care.4-6 Injection-related infections can be treated with antibiotics if identified promptly, but self-treating SSTIs and delaying care can make treatment more challenging; can worsen infections; and can lead to life-threatening conditions, amputation, or death.7,8 Addressing this challenge is urgent, as a projected 257,800 people will die from infective endocarditis—just one of several significant downstream risks from inadequately treated injection-related wounds—from 2020 through 2029. 9
Community-based organizations that provide other services to facilitate safer substance use and prevent overdose among PWID could potentially serve as touchpoints for wound care service delivery due to their established credibility and trust with the community.1,10 However, these organizations encounter barriers to offering services, making wound care resources less accessible. 11 They also rarely employ licensed health professionals with conventional training to provide wound triage and treatment.12,13
A 2022 rapid needs assessment in Austin, Texas, identified opportunities for improved care of injection-related SSTI and immunization against communicable diseases. 14 The assessment confirmed that participants avoided engagement with conventional health care professionals because of stigma and negative experiences; however, limited data were collected regarding self-care knowledge and practices. Accordingly, this study sought to better understand wound care self-treatment experiences, SSTI knowledge, and treatment seeking decision-making processes among PWID to inform future service provision and educational interventions.
Methods
Using a convenience sample, the study team engaged participants at a community-based mobile program that provides a range of preventive, screening, and referral services to people who use drugs in Austin, Texas, in a 2-phase pilot study: a survey (Phase 1) and brief interviews (Phase 2). This study was conducted from February to June 2023. The findings of the preceding rapid needs assessment, conducted from February to March 2022, informed the development of the instruments for this study.
Phase 1 consisted of a 23-item quantitative survey assessing demographic information, injection practices, injection-related complications, wound care practices, and likelihood of using wound care services (Supplemental Appendix). Examples of injection-related complications, types of wounds, and methods of self-treating wounds were given by researchers while conducting each survey. In February and March 2023, study team members approached individuals seeking services at the site, shared information about the study, and screened for eligibility after obtaining consent. Participants needed to have injected drugs at least once in the past 30 days and be able to complete the survey in English. Study team members recorded survey responses on physical copies of the survey. Participants (n = 39) received a $20 grocery store gift card upon completing the survey.
In Phase 2, study team members conducted brief semi-structured interviews (up to 15 minutes) with PWID receiving services at the site in June 2023 using an interview guide (Supplemental Appendix). Recruitment, screening, and eligibility criteria were the same as for Phase 1. Topics included experience with injection-related infections, knowledge of infections, wound care practices, decisions to seek health care for wounds, and preferences for wound care resources. Interviews were recorded electronically with participant permission and transcribed. Participants (n = 20) received a $20 grocery store gift card.
The Institutional Review Board at The University of Texas at Austin approved this study via expedited review, and participants provided verbal informed consent. No identifying or linking information was collected at either phase. Each phase of the study was conducted independently. Participants could have been in one or both phases of the survey, and the number of participants that completed both phases was unknown. All quantitative data in both phases were self-reported by participants. Demographic characteristics are displayed in Table 1. Interview participants included more representation from racial/ethnic minorities, males, and persons who are unhoused/transient than the survey.
Demographic Characteristics of PWID in Austin, Texas, Who Participated in Surveys or Interviews.
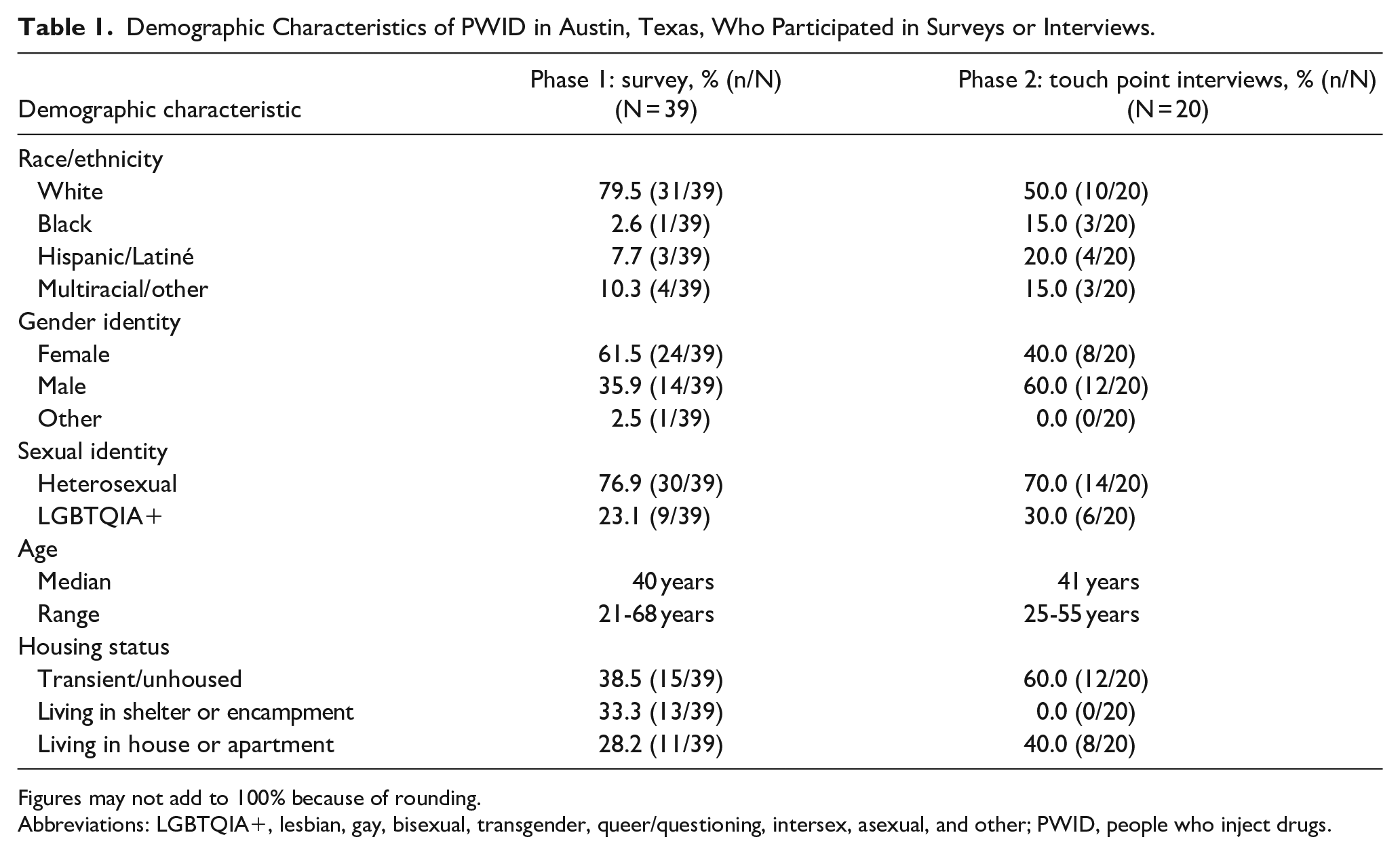
Figures may not add to 100% because of rounding.
Abbreviations: LGBTQIA+, lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual, and other; PWID, people who inject drugs.
Analysis
Descriptive statistics from the quantitative data were calculated. For the qualitative data, 1 senior researcher (H.K.) deductively coded transcript data into an analytic matrix (Microsoft Excel 2024) based on interview topics. 15 A second senior researcher (J.C.) reviewed the themes; both discussed themes and exemplar quotes in team meetings. The senior researcher (H.K.) summarized the themes within topics and identified exemplar data.
Results
More than half of Phase 1 participants had injected more than 1 substance in the past 30 days (Table 2), and the most commonly injected substances were methamphetamine, heroin, and fentanyl. More than half had at least 1 injection-related wound in the past 6 months and reported often or always self-treating injection-related wounds. Reasons for self-treating wounds included confidence in self-treating, lack of perceived wound severity, and stigma encountered in health care settings. Most participants would likely use wound care services at a site run by a community-based organization that works with PWID. Nearly three-fourths would prefer staff from community-based organizations that work with PWID to deliver wound care services, and most wanted individuals with medical credentials to provide wound care.
Behavioral Characteristics Among PWID Who Participated in the Survey in Austin, Texas.
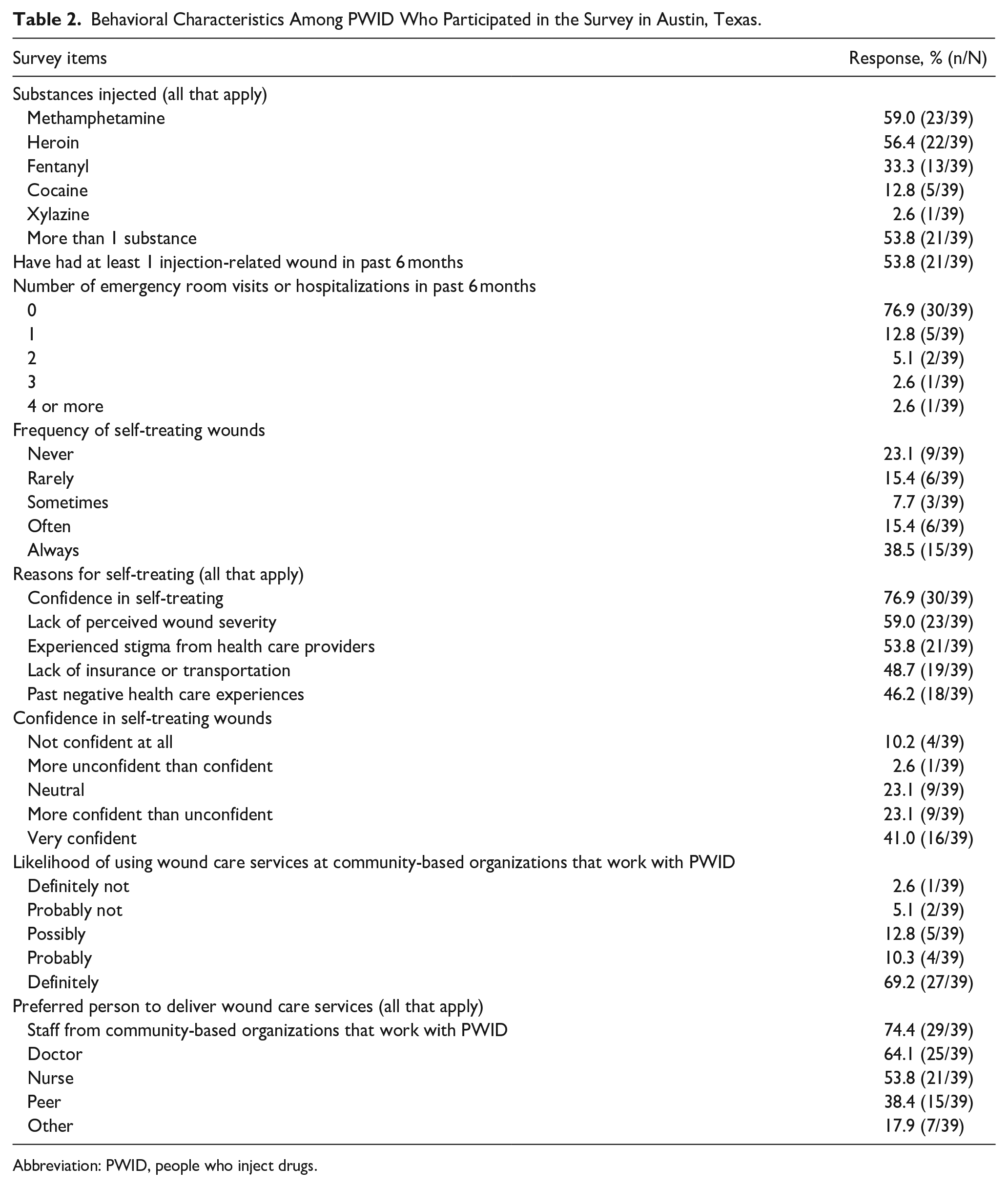
Abbreviation: PWID, people who inject drugs.
Knowledge of SSTIs
Table 3 provides themes with exemplar quotes shared by interview participants in Phase 2. Participants were knowledgeable about symptoms of infection; they identified inflammation, redness, pain, abscesses, pus, necrosis, and fever as signs of infection. A few referred to cellulitis, staph infections, and methicillin-resistant Staphylococcus aureus. Knowledge of infections came from several sources: (1) personal experience with infections, (2) other PWID who had experienced infections, and (3) materials or education from community-based organizations that work with PWID or health care professionals.
Interview Themes With Exemplar Quotes From PWID Who Participated in Interviews in Austin, Texas.
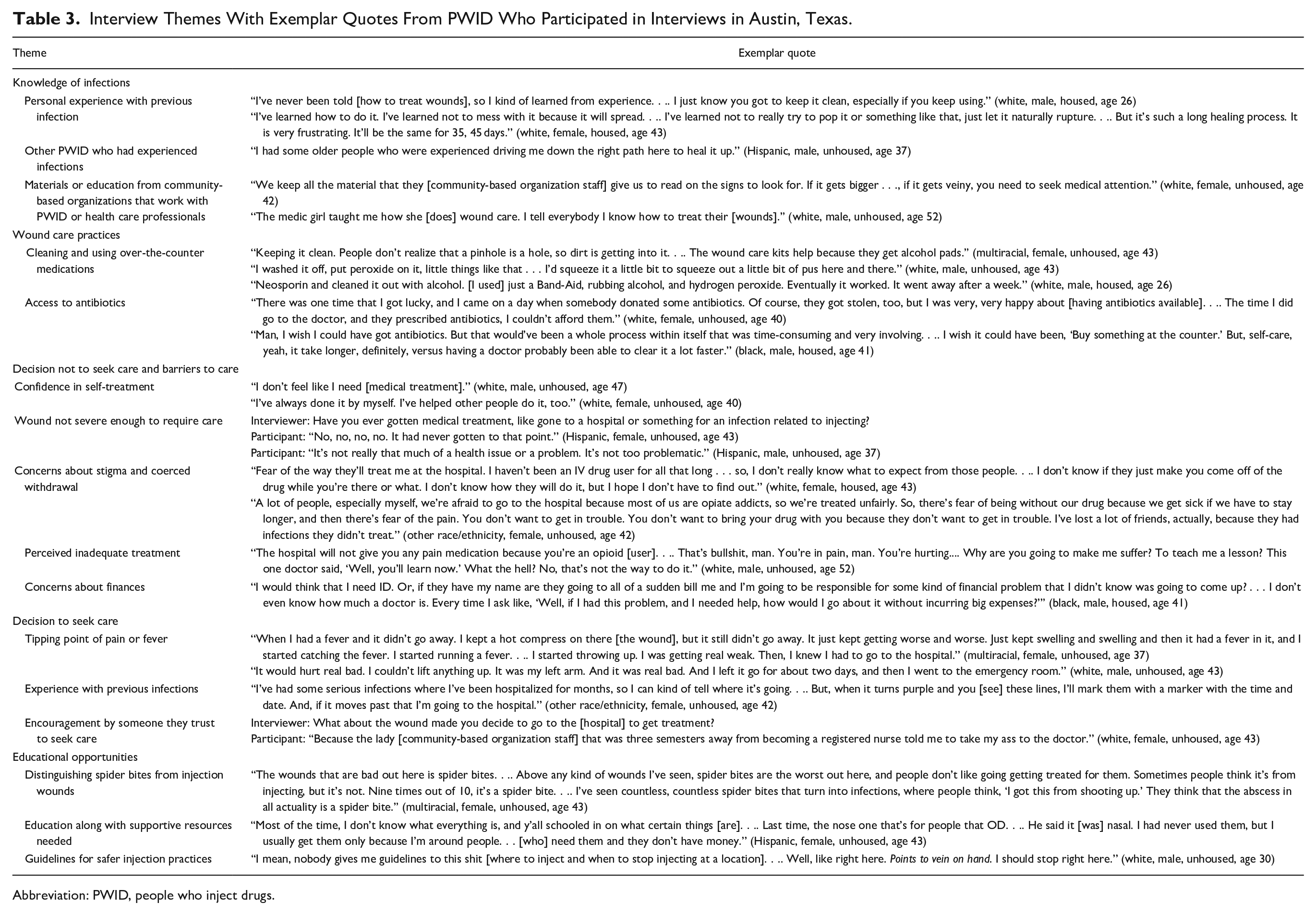
Abbreviation: PWID, people who inject drugs.
Personal experiences entailed self-managed infections and those requiring hospitalization. Infections requiring hospitalization and intensive medical intervention left impressions about monitoring wounds carefully. Knowledgeable others helped participants recognize and care for infections, and several participants described helping others care for wounds. Sometimes, other individuals offered incorrect information. For example, 1 participant received advice to cut open bumps with razor blades but learned, “Anytime I’ve done something like that, it’s turned out worse” (white, female, housed, age 43). A few participants mentioned that resources from community-based organizations that work with PWID or medical personnel helped them to understand the symptoms and the need for care. Resources included written materials and education about wound care from community-based staff with medical knowledge.
Wound Care Practices
Wound care practices entailed using over-the-counter antiseptics (eg, hydrogen peroxide, rubbing alcohol, Bactine), topical ointments (eg, Neosporin, Tiger Balm), and hot or cold compresses, while striving to keep the wound clean, dry, and covered. Interview participants used public restrooms, “bleach water,” or saline solutions to wash their wounds. Keeping wounds clean presented a significant challenge to participants without housing; one said, “Nothing is sterile out here” (other race/ethnicity, female, unhoused, age 42). Keeping the wound covered meant relying on bandages and gauze, although participants could not routinely afford these supplies and reported they depleted supplies in the kits from the mobile site. Several participants commented that they have had supplies stolen from them.
Having antibiotics available early, without interaction with hospitals, was desirable among participants. One commented that having antibiotics would be a “game changer” (white, male, housed, age 33). Occasionally, participants had obtained prescription antibiotic medications and ointments from donations or family. Several asserted that early antibiotic treatment would reduce healing time relative to self-treatment with over-the-counter medications. Participants also recommended having increased access to supplies, such as gauze, tape, and other antibacterial products.
Decision Not to Seek Care and Barriers to Care
Interview participants reported they could manage their most recent wounds effectively and felt their most recent wound was not severe enough to require medical intervention. They expressed concerns about stigma and recalled negative experiences in health care settings; they noted financial and other barriers to care. They were concerned that interactions with the health care system could lead to forced withdrawal from substances.
Decision to Seek Care
For a few participants, fever or severe pain was the tipping point for going to the emergency department. Experience with infections guided decision-making, as participants could determine when the infection was beyond their ability to self-treat. One participant described a careful monitoring strategy based on her experience with wounds that informed her decision to seek care (see Table 3 for more detail). Finally, encouragement by someone they trust to seek care helped a few participants pursue medical intervention.
Educational Opportunities
Participants shared recommendations that point to educational opportunities. A few noted that PWID may have difficulty distinguishing injection wounds from spider bites, which are a risk when living unhoused. Another shared that education alone would not be sufficient, as she has difficulty remembering the uses of various materials. Another suggested having guidelines for safer injection practices.
Most survey and interview participants wanted someone who is knowledgeable and licensed to provide wound care. As one said, “Somebody that knows exactly what they are doing, how to do it . . . do the whole thing, drain them, wound care, everything . . . a professional” (multiracial, female, unhoused, age 37). Though participants were agnostic about the medical degree, many wanted access to antibiotics but noted they could not afford the prescriptions.
Discussion
Participants had confidence in their ability to treat wounds, along with knowledge of common symptoms gained from experience, knowledgeable others, or community-based staff. Incorrect information is still shared. Education can address misinformation by distinguishing what types of wounds are present, when wounds require medical intervention, and what injection practices would prevent wounds. Having confidence in self-treatment in the absence of cleaning supplies and medical knowledge can compound challenges, as individuals may delay treatment until the infection becomes severe.
Wound care treatment can most effectively be addressed by licensed health care professionals. However, because of financial barriers and stigmatizing interactions, receiving this care may not be feasible or desirable for PWID. Participants indicated sites run by community-based organizations were preferred places to receive wound care education, treatment, and supplies. Efforts to make hospitals and other conventional medical settings more welcoming and supportive for PWID are also urgently needed. As 1 participant quote noted, people who use drugs face likely withdrawal in these settings because of institutional policies that prohibit the use of non-prescribed substances and the lack of consistent implementation of evidence-based practices to adequately manage withdrawal with prescribed medications.16,17 Likewise, the challenges associated with having supplies stolen and depleting supplies suggest providers should consider alternative approaches to ensure that PWID have access to supplies to self-treat wounds. Although this study focuses on typical bacterial infections that occur at injection sites, emerging substances (eg, xylazine) may generate different types of wounds that do not currently have standardized clinical guidelines for management. 18
Behavioral, educational, and clinical interventions to prevent and facilitate timely treatment of wounds among PWID have been developed for implementation in various settings. Prominent examples include motivational interviewing approaches for health care professionals to educate and encourage participants to embrace safer practices, and models for syringe services programs to implement enhanced services using existing paraprofessional staff.10,13,19,20 However, available evaluations of these approaches indicate limited efficacy and describe challenges with implementation, particularly for interventions provided by paraprofessionals. These staff may experience uncertainty regarding their scope of practice and require frequent retraining as the drug supply and associated health risks evolve. Participants in this study reported a preference for licensed health care professionals to provide wound care services, but employing such professionals is costly and relying on volunteers may lead to inconsistent availability, poor continuity, and challenges reconciling strict health care culture with low barrier approaches to care in community-based programs. Additional research to identify optimal models for service integration in community organizations that serve PWID is urgently needed.
This study has several limitations, including reliance on a convenience sample with an unknown number of individuals participating in both phases. Thus, we cannot link responses between phases. The survey and interview guide were not developed based on a specific theoretical framework, but simply to expand upon the findings of a previous rapid needs assessment. Although most interview themes had representation across gender and racial/ethnic identities, 1 theme about differentiating wounds and spider bites was more salient for persons who are unhoused. Participants’ self-report of drugs they have injected may not be accurate, particularly given limited access to drug checking supplies. The generalizability of these findings to settings that differ substantially from Austin, Texas, is unknown. In Texas, syringe services programs and community drug checking services are generally considered to be illegal. Furthermore, there is little evidence of xylazine or other alpha-2 adrenergic agonists emerging in the local drug supply. Regions with other legal contexts and drug supplies may find that PWID have differing needs and preferences related to wound care.
Conclusions
Needs for wound care treatment and education among PWID are currently unmet, and stigma from health care providers remains a barrier to seeking early intervention for infections. Delivering wound care services and education through community-based organizations that have established credibility and connection with PWID may enhance access to care.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251334203 – Supplemental material for Wound Care Practices Among People Who Inject Drugs in Austin, Texas
Supplemental material, sj-docx-1-saj-10.1177_29767342251334203 for Wound Care Practices Among People Who Inject Drugs in Austin, Texas by Hannah P. McCullough, Heather Kane, Jessica Duncan Cance, Chryssandra Tatum, Lindsey J. Loera, Lorie Kmetz and Lucas G. Hill in Substance Abuse
Footnotes
Acknowledgements
The authors thank Berkin Kutluk, Amber Tran, Dalaina Dreymala, Eric Lumanog, Leah Nealis, Grace Ukazim, and Claire Zagorski for providing logistical support.
Author Contributions
HPM: conceptualization, investigation, and writing—original draft; HK: conceptualization, methodology, formal analysis, and writing—original draft; JDC: conceptualization, methodology, and writing—review and editing; CT: formal analysis, and writing—original draft; LJL: project administration, and writing—review and editing; LK: conceptualization, methodology, and writing—review and editing; and LGH: funding acquisition, methodology, supervision, and writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project team was supported by funding from the Texas Targeted Opioid Response, a public health initiative operated by the Texas Health and Human Services Commission through federal funding from the Substance Abuse and Mental Health Services Administration (SAMHSA) grant award number 1H79TI081729. However, the funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation of the manuscript; or the decision to submit the article for publication. The content of this study does not represent the official view of SAMHSA or the Texas Health and Human Services Commission.
Compliance,Ethical Standards,and Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board at The University of Texas at Austin approved this study via expedited review and participants provided verbal informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.