
Abstract
Background:
Substance use disorders (SUDs) represent a significant global public health challenge, with affected individuals often exhibiting poor dietary habits, nutritional deficiencies, and compromised mental and physical health. This scoping review evaluates existing literature on dietary intake in individuals with SUDs, focusing on the potential benefits of plant-based dietary interventions for improving nutritional status and supporting recovery.
Methods:
A scoping review was conducted following PRISMA guidelines. Four databases were searched using PICO-based terms, targeting studies assessing dietary intake in patients with SUD, particularly plant-based interventions. Inclusion criteria were studies reporting macro- and micronutrient intake among patients with SUD, while studies lacking direct dietary intake data were excluded. Study quality was appraised using the STROBE checklist.
Results:
The search yielded 1142 potential articles, with 6 meeting inclusion criteria (4 from the United States and 2 from Iran). Patients with SUD exhibited significant deficiencies in iron (−16.8%, P = .04), folate (−15.0%, P = .04), and vitamins E and A, alongside diets high in simple carbohydrates and unhealthy processed foods. Plant-based dietary interventions were associated with improved Healthy Eating Index scores (P < .001), increased resilience (+31%, P = .031), and enhanced self-esteem (P = .043). High energy intake and low multivitamin use were reported among methadone-treated patients, emphasizing the need for dietary interventions to address nutrient gaps and support recovery.
Conclusion:
Plant-based dietary interventions may offer a promising strategy to address nutrient deficiencies and improve mental health outcomes in patients with SUD. However, studies are limited, with small sample sizes and variability in dietary assessments. Future research, including randomized controlled trials, is needed to establish the efficacy and feasibility of integrating plant-based nutrition into SUD treatment programs. Addressing barriers such as socioeconomic challenges and food access is also crucial for implementing effective dietary interventions.
Highlights
Individuals with substance use disorders (SUDs) commonly exhibit deficiencies in key nutrients, including iron, folate, and vitamins A and E, while consuming diets high in simple carbohydrates and processed foods.
Plant-based dietary interventions were associated with improved nutritional status, higher Healthy Eating Index scores, increased resilience, and enhanced self-esteem, highlighting their potential role in addiction recovery.
Despite promising findings, research on plant-based nutrition in SUD treatment remains limited, underscoring the need for larger studies and randomized controlled trials to assess feasibility, effectiveness, and barriers to implementation.
Introduction
Substance use disorder (SUD) is a recognized international public health crisis, with millions of individuals affected globally across various substance dependencies, including opioids, alcohol, and stimulants.1,2 The rising numbers of drug-related fatalities and hospitalizations worldwide underscored the severity of this issue. Between 2000 and 2014, in the United States alone, nearly half a million individuals died from drug overdoses, with opioids accounting for a majority of these deaths in recent years. 3 Similar patterns are observed internationally, with countries like Canada, Australia, and several European nations reporting escalating drug-related mortality rates.4,5 The opioid crisis is one of the most notable aspects of SUDs, but increasing misuse and dependency on various substances have resulted in a broad public health burden that warrants attention to SUDs overall.
Poor nutritional health is well-documented among individuals with SUDs, which is often exacerbated by a lack of nutritional knowledge, erratic dietary habits, and a predisposition toward high-sugar, low-nutrient foods.6,7 Studies indicate that patients with SUDs, particularly those with opioid use disorder, frequently consume insufficient amounts of vegetables, fruits, and whole grains and are prone to nutritional deficiencies in essential vitamins and minerals.6,8 Additionally, individuals with SUD often experience weight fluctuations and irregular eating patterns. When actively using substances, many report diminished interest in food, often substituting it with low-cost, convenience foods.6,9,10 Conversely, during abstinence, there is an increased prevalence of binge eating and disordered eating behaviors. 11 Such dietary habits may further compromise their physical health and potentially impede recovery efforts.
Improving the nutritional intake of individuals with SUDs is suggested to play a supportive role in recovery.6,12 Although the direct role of nutrition in the detoxification process is not yet fully understood, preliminary evidence indicates that addressing nutritional deficiencies may enhance physical health, stabilize mood, and reduce relapse risk. However, many individuals with SUDs lack access to proper nutritional guidance or support within treatment programs, which could serve as a critical area for intervention.6,13,14
Plant-based diets, which emphasize whole, minimally processed plant foods such as fruits, vegetables, legumes, nuts, seeds, and whole grains, may offer a promising approach for addressing nutritional deficiencies in populations with SUD. The theoretical basis for their benefits lies in their anti-inflammatory and neuroprotective properties, which have been shown to improve both physical and mental health.15 -17 Nutrient-dense plant-based foods are rich in essential vitamins, minerals, fiber, and antioxidants, all of which contribute to reduced inflammation and oxidative stress—2 factors often exacerbated by substance use and implicated in cognitive dysfunction and mood disorders.16,18,19 Additionally, omega-3 fatty acids, magnesium, and B vitamins, commonly found in plant-based diets, play critical roles in neurotransmitter synthesis and mood regulation, potentially alleviating symptoms of depression and anxiety frequently observed in populations with SUD.20 -22
Despite the known associations between poor nutrition and adverse health outcomes in populations with SUD, there remains a lack of comprehensive research assessing specific macro- and micronutrient intake across different populations with SUD. This information gap limits the understanding of dietary needs that could optimize treatment outcomes. While some research has focused on nutritional biomarkers in patients undergoing opioid replacement therapy, few studies investigate actual dietary intake and its potential role in supporting addiction recovery for broader populations with SUD.
The purpose of this scoping review was to evaluate the existing research on the macro- and micronutrient intake of individuals with SUDs, with a specific focus on plant-based dietary intake. For this review, a plant-based diet is defined as one that emphasizes whole, minimally processed plant foods such as fruits, vegetables, legumes, nuts, seeds, and whole grains, while limiting or excluding highly processed plant-based foods and animal products. This review aimed to determine whether plant-based dietary modifications, particularly those focused on unprocessed or minimally processed foods, could support addiction recovery and enhance overall health outcomes in patients with SUDs.
Methods
A scoping review was conducted in adherence to PRISMA guidelines. The primary outcomes of interest in this review were to evaluate the nutritional intake of individuals with SUDs, with a particular emphasis on studies involving plant-based diet interventions assessed through direct dietary intake methods or biomarker analysis.
Inclusion and Exclusion Criteria
Studies were included if they involved individuals diagnosed with SUDs across various treatment settings, such as opioid replacement therapy, methadone maintenance, or general populations with SUD. Eligible studies were required to report direct dietary intake assessments, including food frequency questionnaires, 24-hour dietary recalls, or biomarker analyses, with a particular focus on macro- and micronutrient intake, as well as plant-based dietary interventions.
Exclusion criteria were applied to studies that solely assessed nutritional status without evaluating direct dietary intake or failed to report macro- or micronutrient data. Studies were also excluded if they included participants with significant or unaddressed comorbidities, such as severe eating disorders, that could confound dietary intake findings. Additionally, studies focusing exclusively on pediatric populations (<18 years) or animal studies were excluded to maintain the focus on adult human populations. These criteria were designed to ensure that the included studies directly aligned with the review’s objectives of evaluating dietary intake patterns, particularly plant-based interventions, in individuals with SUDs.
Search Strategy
Search terms were formulated using the PICO framework. Participants (P) included individuals with SUDs across various treatment settings. Intervention (I) focused on dietary intake assessments, particularly plant-based diet interventions, and included methods such as food frequency questionnaires, 24-hour recalls, and biomarker analyses. Comparisons (C) consisted of studies that evaluated dietary intake in SUD patients with or without plant-based dietary interventions or compared intake levels against standard dietary guidelines. Outcomes (O) were any reported measures of macro- and micronutrient intake. Studies were excluded if they solely assessed nutritional status without focusing on direct dietary intake or plant-based dietary intake.
Screening and Study Selection
Three electronic databases—PubMed, Embase, and Scopus—were searched for relevant articles in English. The search strategy was initially developed in PubMed and included a combination of keywords and medical subject headings relevant to substance use, plant-based diets, and dietary intake, and was then adapted for other databases.
Title screening was conducted by 1 author, and abstracts were reviewed independently by 2 authors against inclusion criteria. Additional studies were identified through reference reviews of relevant papers. All articles meeting the inclusion criteria were retrieved in full for a detailed assessment. In cases of disagreement, a third reviewer was consulted. The full-text screen process, as illustrated in Figure 1, was managed using the EndNote and Covidence software.
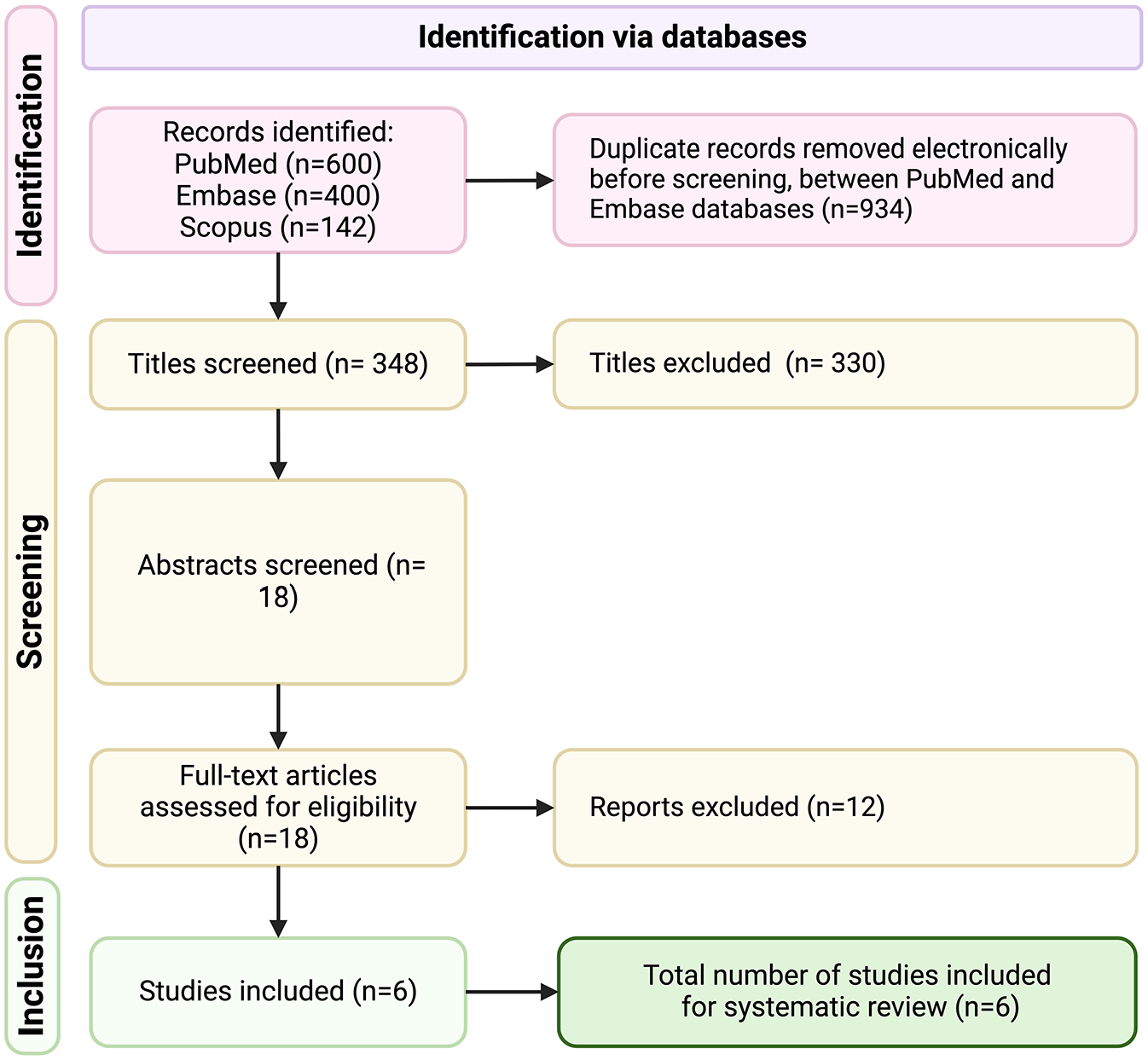
PRISMA study selection flow diagram.
Data Extraction and Analysis
Data from each included study were synthesized narratively, focusing on macro- and micronutrient intake levels, with specific attention to plant-based diet interventions. Methods used for data collection were recorded, and a descriptive summary of study characteristics and results was developed by the chief investigator. Nutritional intake data were tabulated to facilitate direct comparison between and to evaluate trends across studies.
Quality Assessment
The quality of the studies included were appraised using the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist. The checklist was applied to assess methodological quality across 6 domains and 22 criteria. Quality assessment was conducted independently by 2 reviewers, with a third reviewer consulted to resolve any discrepancies.
Results
The electronic search process initially yielded 1142 potential articles. After removing 934 based on title screening and duplicates, 194 papers remained for abstract screening against inclusion criteria. Reference checks of screened articles identified an additional 4 papers, leading to 18 articles for a full-text review. Of these, 12 were excluded for not meeting the inclusion criteria of investigating both nutritional intake and plant-based dietary interventions among individuals with SUDs. Ultimately, 6 studies (Table 1) were included in the final analysis.17,23 -27 Among these, 2 were conducted in Iran, and 4 were based in the United States.
Characteristics of Studies Included in This Study.
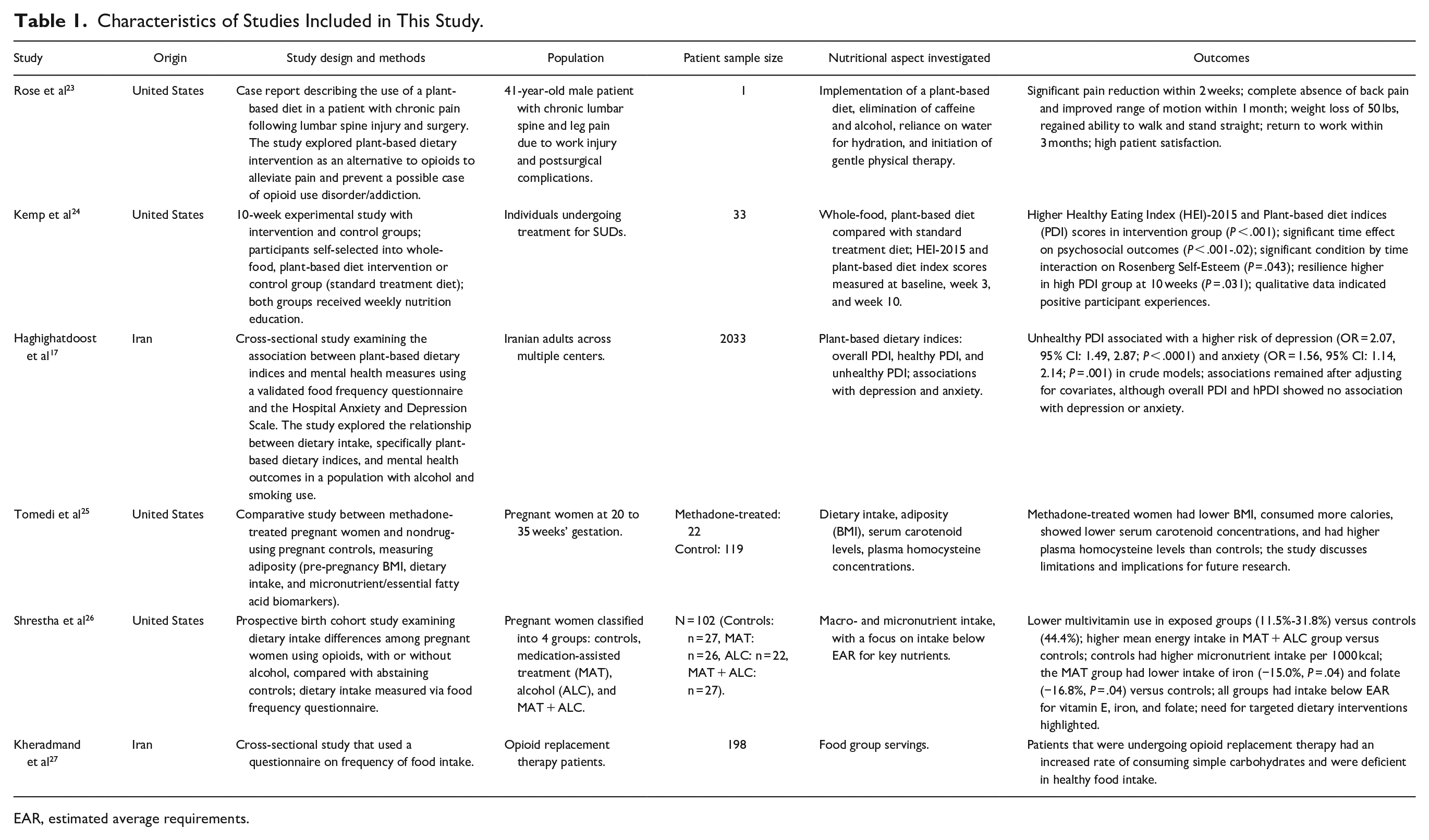
EAR, estimated average requirements.
Of the 6 included studies, Kemp et al was the only study that explicitly examined a structured plant-based dietary intervention and its outcomes in individuals with SUDs. Kemp et al demonstrated significant improvements in dietary quality, resilience, and self-esteem among participants following a whole-food, plant-based diet compared with those on a standard treatment diet. The remaining studies primarily explored general dietary intake patterns or nutrient deficiencies in populations affected by SUDs. For instance, Shrestha et al and Tomedi et al focused on pregnant women undergoing methadone treatment, highlighting deficiencies in key micronutrients such as iron, folate, and vitamin E, alongside high caloric intake from nonnutritive sources. Similarly, Kheradmand et al and Haghighatdoost et al examined broader dietary patterns, reporting high consumption of simple carbohydrates and processed foods among opioid replacement therapy patients and an association between unhealthy plant-based diets and increased risks of depression and anxiety. The inclusion of the Rose et al case study is justified because it explored the use of a plant-based diet to alleviate chronic pain and potentially reduce reliance on opioids in a patient experiencing significant postsurgical complications. This aligns with the broader themes of dietary strategies for managing substance use and reducing the risk of opioid dependency. However, it is important to acknowledge the inherent limitations of this case study. As a single-patient report, the findings lack generalizability and are not supported by controlled experimental data. Additionally, the absence of a confirmed SUD diagnosis limits the direct applicability of its conclusions to substance use disorder populations. Despite these limitations, the case study provides valuable supplementary evidence of the potential utility of plant-based dietary interventions in reducing opioid reliance, particularly in individuals at risk of developing opioid use disorder. Its inclusion in this review serves to highlight a gap in the current literature and underscore the need for further research into the role of plant-based diets in both prevention and recovery contexts for populations with SUD.
Overall, while the evidence for plant-based dietary interventions in patients with SUD remains limited, the findings underscore prevalent nutrient deficiencies, poor dietary patterns, and the potential role of plant-based strategies in addressing these gaps. These results highlight the need for further research to evaluate the efficacy and implementation of structured plant-based interventions in this population.
Study Characteristics and Focus on Plant-Based Diets
The included studies examined various aspects of dietary intake in patients with SUD, with several focusing on populations undergoing opioid replacement therapy (ORT) or methadone maintenance treatment. However, a notable gap exists in studies explicitly investigating plant-based dietary intake in this population, highlighting the need for targeted research.
Studies that incorporated plant-based or whole-food dietary interventions, such as Kemp et al, demonstrated clear improvements compared with those on standard diets. Kemp et al reported that participants following a whole-food, plant-based dietary intervention achieved significantly higher Healthy Eating Index (HEI-2015) scores (P < .001), indicating improved dietary quality. Additionally, the intervention group experienced notable psychosocial benefits, including a 31% improvement in resilience (P = .031) and a significant increase in self-esteem (P = .043), compared with the control group. 24 These findings suggest that structured plant-based diets not only address dietary deficiencies but also play a supportive role in improving mental health outcomes for individuals undergoing SUD treatment.
In contrast, studies like Shrestha et al and Tomedi et al evaluated dietary intake among pregnant women undergoing methadone treatment. Both studies highlighted key micronutrient deficiencies (eg, vitamin E, iron, and folate) and high caloric intake from nonnutritive sources such as sweets.25,26 For example, Shrestha et al reported that iron intake in the methadone-assisted treatment group was 15% lower (P = .04) and folate intake was 16.8% lower (P = .04) compared with controls. These findings underscore the need for interventions that emphasize nutrient-dense, plant-based foods to address these deficiencies and promote healthier outcomes for this vulnerable population.
Across the reviewed studies, macro- and micronutrient intake assessments often revealed deficits in fiber, essential fatty acids, and several vitamins (eg, A, E, thiamine), which are abundant in plant-based foods. The studies by Ii et al, Waddington et al, and Alves et al demonstrate that patients with SUDs typically consume higher levels of sodium and saturated fats, which a plant-based diet could potentially correct. For instance, a shift toward whole grains, legumes, vegetables, and fruits could improve fiber intake and reduce reliance on processed, high-sodium foods.
Additionally, both Haghighatdoost et al and Kheradmand et al highlighted dietary patterns that could be addressed through plant-based interventions for patients with SUDs.17,27 Haghighatdoost et al observed that a high intake of unhealthy plant-based foods, characterized by simple carbohydrates and processed items, was associated with an increased risk of depression and anxiety among Iranian adults. This finding suggests that an unhealthy plant-based diet could exacerbate mental health issues rather than alleviating them. Similarly, Kheradmand et al found that ORT patients had a high intake of simple carbohydrates and a deficiency in nutrient-dense foods, such as complex carbohydrates, fruits, and vegetables. These patterns of low-nutrient, high-sugar diets indicate where a shift toward a balanced, whole-food, plant-based diet could be beneficial, potentially reducing depressive symptoms and enhancing overall mental health by increasing essential nutrient intake. Together, these studies underscore the potential for plant-based dietary interventions to transform dietary patterns in populations with SUD, promoting better mental and physical health outcomes.
Overall, the included studies demonstrated that patients with SUD, particularly those undergoing ORT, have poor dietary quality, with diets characterized by high intake of nonnutritive, high-calorie foods and significant nutrient deficiencies. Plant-based interventions that emphasize nutrient-dense, whole foods—such as fruits, vegetables, legumes, and whole grains—have the potential to improve dietary patterns, reduce deficiencies, and enhance mental health outcomes. These findings reinforce the need for further research to evaluate the implementation and efficacy of structured plant-based interventions in SUD treatment programs, particularly in comparison with standard treatment diets.
The results of this review underscore the distinct and multifaceted benefits of structured plant-based dietary interventions compared with standard treatment diets in addressing the nutritional and mental health challenges faced by individuals with SUDs. Kemp et al’s study stands out as the only investigation to directly implement a structured whole-food, plant-based dietary intervention, demonstrating significant improvements in dietary quality, resilience (+31%, P = .031), and self-esteem (P = .043) over a 10-week period. These findings highlight the potential for plant-based diets to transcend the limitations of traditional treatment diets by not only addressing widespread nutrient deficiencies but also enhancing key psychosocial outcomes critical for sustained recovery. In contrast, other studies, such as Shrestha et al and Tomedi et al, revealed that standard dietary patterns in populations with SUD undergoing methadone or ORT often fail to meet essential nutrient requirements. For instance, methadone-treated groups exhibited significantly lower iron (−15%, P = .04) and folate (−16.8%, P = .04) intake alongside high caloric consumption from nonnutritive sources, highlighting a critical gap in nutritional adequacy. Similarly, studies like Haghighatdoost et al and Kheradmand et al associated unhealthy dietary patterns, including high consumption of simple carbohydrates and processed foods, with increased risks of depression and anxiety.
This comparison underscores the transformative potential of plant-based diets to address these gaps. By emphasizing nutrient-dense, whole-food consumption—such as fruits, vegetables, legumes, and whole grains—plant-based interventions offer a holistic strategy to combat nutrient deficiencies while simultaneously mitigating mental health challenges. Furthermore, the ability of these diets to deliver measurable psychosocial benefits, as shown in Kemp et al, sets them apart from conventional treatment diets, which primarily focus on symptom management without addressing underlying dietary imbalances. These findings advocate for the integration of plant-based dietary interventions as a superior alternative to standard approaches in SUD treatment, highlighting their potential to deliver both immediate and long-term benefits to this vulnerable population. Future research should focus on expanding these insights through rigorous comparative studies, ensuring that plant-based strategies can be effectively tailored to diverse populations with SUD.
Discussion
SUDs pose a significant public health challenge, characterized by high relapse rates and extensive physical, psychological, and social implications. 28 Nutritional deficiencies and poor dietary habits are common among people with SUDs, which may exacerbate both physical and mental health issues, impeding recovery.6,12 This investigation aimed to examine the role of plant-based dietary intake in improving nutritional and mental health outcomes for patients with SUD. While our review highlights the potential benefits of plant-based diets, it is important to clarify that only 1 study (Kemp et al) explicitly investigated a structured plant-based dietary intervention and its outcomes in patients with SUD. Other studies primarily assessed general dietary intake, nutrient deficiencies, or unhealthy dietary patterns in populations with SUD, providing indirect insights into how plant-based nutrition might address these gaps.
Omega-3 fatty acids, abundant in foods such as flaxseeds, walnuts, and algae-based sources, have demonstrated neuroprotective and anti-inflammatory properties that are directly relevant to SUD recovery.22,29 Chronic substance use has been shown to induce neuroinflammation and impair dopaminergic signaling, contributing to cravings and relapse. 30 Omega-3 fatty acids can help mitigate these effects by reducing pro-inflammatory cytokines and promoting synaptic plasticity, thereby supporting brain health and potentially improving mood regulation and cognitive function. For instance, studies have indicated that supplementation with omega-3 fatty acids may reduce depressive symptoms and anxiety, both of which are common comorbidities in populations with SUD.22,31
B vitamins, including folate, thiamine (B1), pyridoxine (B6), and cobalamin (B12), play critical roles in energy metabolism, neurotransmitter synthesis, and neural repair. 32 Individuals with SUDs, particularly those with alcohol use disorder, frequently exhibit deficiencies in B vitamins due to malabsorption and poor dietary intake.33,34 Folate and B12 are essential for the synthesis of monoamine neurotransmitters, such as serotonin and dopamine, which are often dysregulated in SUD.35,36 Incorporating B vitamin-rich foods, such as leafy greens, legumes, and fortified plant-based products, into dietary interventions may help address these deficiencies and support neurocognitive recovery.
Antioxidants, including vitamins C and E, selenium, and polyphenols, help combat oxidative stress, which is heightened in populations with SUD due to the metabolic burden of substance metabolism and the associated inflammatory response.37,38 Oxidative stress contributes to cellular damage, neurodegeneration, and impaired immune function, which can hinder recovery. 39 Antioxidant-rich plant-based foods, such as berries, citrus fruits, and cruciferous vegetables, can help neutralize reactive oxygen species and promote cellular repair. 40 For example, vitamin C supports the synthesis of norepinephrine and cortisol regulation, both of which are critical in stress response and addiction recovery.41,42
The Kemp et al study is notable for demonstrating significant improvements in dietary quality, resilience (+31%, P = .031), and self-esteem (P = .043) among participants following a structured whole-food, plant-based diet compared with standard treatment diets. This study suggests that plant-based interventions may play a meaningful role in improving both nutritional intake and mental health outcomes for individuals in SUD recovery. In contrast, the remaining studies, such as Shrestha et al and Tomedi et al, focused on pregnant women undergoing methadone treatment and reported widespread nutrient deficiencies (eg, iron, folate, and vitamin E) alongside high caloric intake from nonnutritive foods. Similarly, Kheradmand et al found that ORT patients had diets dominated by simple carbohydrates and were deficient in nutrient-dense foods, such as fruits, vegetables, and whole grains. These findings underscore the need for interventions that emphasize nutrient-dense foods, like those found in plant-based diets, to address dietary imbalances. The inclusion of the Rose et al case study in this review requires further clarification. While the patient did not have a confirmed diagnosis of SUD, the study explored the use of a plant-based diet to alleviate chronic pain and prevent potential opioid use disorder, aligning with the broader theme of dietary strategies to reduce reliance on opioids. This case provides supplementary evidence of the potential utility of plant-based diets in reducing opioid use risk, albeit in a different context.
Our review builds on these findings by suggesting that plant-based diets, rich in essential nutrients such as omega-3 fatty acids, fiber, folate, and antioxidants, could play a role in addressing the nutrient deficiencies and poor dietary quality often seen in populations with SUD. Importantly, the quality of plant-based intake matters, as demonstrated by Haghighatdoost et al, unhealthy plant-based patterns dominated by processed foods and refined sugars were associated with increased risks of depression (OR = 2.07, P < .0001) and anxiety (OR = 1.56, P = .001). This emphasizes the need for structured, whole-food-based interventions to avoid exacerbating mental health issues. Despite the potential benefits of plant-based nutrition, implementing such interventions presents practical challenges. Cost remains a major barrier, as fresh fruits, vegetables, and whole foods are often more expensive than processed, high-calorie alternatives, particularly in low-income and rural settings where SUD rates are often higher. Additionally, limited access to fresh foods in food deserts or treatment centers with constrained resources may impede the feasibility of plant-based diets. Addressing these challenges would require targeted interventions, including subsidized food programs, education on affordable meal preparation, and partnerships with community organizations to improve food accessibility. Another critical consideration is the risk of nutritional deficiencies if plant-based diets are not properly balanced. Poorly planned plant-based diets can lack essential nutrients such as vitamin B12, iron, and omega-3 fatty acids, which are already deficient in many populations with SUD. Structured nutritional counseling and ongoing monitoring are essential to ensure plant-based dietary interventions are nutritionally adequate and tailored to individual needs.
There are several limitations in this review that warrant attention. First, the number of studies explicitly investigating plant-based dietary interventions in populations with SUD is limited, with only 1 study (Kemp et al) meeting this criterion. The other included studies examined general dietary intake or nutrient deficiencies without implementing structured plant-based diets. While these findings provide indirect insights, they introduce assumptions regarding the potential role of plant-based nutrition in SUD treatment. Additionally, most studies were observational, increasing the likelihood of confounding variables influencing outcomes. Factors such as socioeconomic status, cultural norms, and food accessibility may further affect the generalizability of the findings. The inconsistency in dietary assessment tools, such as food frequency questionnaires and 24-hour recalls, may also limit the accuracy of reported dietary patterns. The included studies in this review were predominantly conducted in the United States and Iran, which may limit the generalizability of the findings to other regions with distinct dietary practices, cultural attitudes, and healthcare systems. In the United States, dietary habits are often characterized by high consumption of processed foods, refined sugars, and saturated fats, whereas in Iran, traditional diets may include higher intakes of whole grains, legumes, and fresh produce.19,43,44 These dietary differences could influence the relevance and effectiveness of plant-based dietary interventions in populations with SUD across different cultural contexts. Moreover, access to plant-based foods varies significantly between regions, with socioeconomic disparities and geographic factors playing a critical role. 45 In low-income countries, limited infrastructure and food insecurity may hinder the feasibility of implementing structured plant-based interventions. Similarly, in some cultures, the concept of a plant-based diet may not align with traditional dietary patterns or may face resistance due to cultural norms, religious beliefs, or food preferences. These factors must be considered when interpreting the findings and designing interventions.
Our findings suggest that plant-based nutrition has potential as an adjunctive strategy to address the nutritional and mental health challenges faced by individuals with SUDs. While the evidence remains preliminary, the promising results from Kemp et al and the observed nutrient deficiencies in other studies highlight a clear need for targeted dietary interventions. However, additional research—particularly randomized controlled trials—will be necessary to evaluate the efficacy, feasibility, and long-term outcomes of plant-based dietary interventions in populations with SUD.
Future research should focus on conducting randomized controlled trials to evaluate the effects of whole-food, plant-based diets on recovery outcomes, including nutritional biomarkers, relapse rates, and mental health. Additionally, studies should investigate the role of specific nutrients found in plant-based foods, such as omega-3 fatty acids, fiber, and antioxidants, in addressing neurocognitive and psychological outcomes in patients with SUD. It is equally important to explore strategies to overcome barriers to implementation, such as cost, accessibility, and cultural considerations, particularly in underserved communities where access to fresh, nutrient-dense foods may be limited. These efforts will provide a clearer understanding of the feasibility, efficacy, and long-term impact of plant-based dietary interventions on improving recovery outcomes for individuals with SUDs.
While this review identifies significant gaps in research on plant-based dietary interventions in populations with SUD, it also highlights their potential as a promising strategy for improving nutritional and mental health outcomes. Structured and well-balanced plant-based diets, supported by nutritional counseling and accessible food programs, could address the prevalent dietary deficiencies observed in populations with SUD and provide a valuable, holistic approach to enhancing recovery outcomes.
Conclusion
This scoping review highlights the potential of plant-based dietary interventions to support recovery and improve health outcomes in individuals with SUD. Our findings reveal that patients with SUD, particularly those undergoing ORT, often consume diets high in nonnutritive foods and are deficient in essential nutrients such as fiber, iron, folate, and vitamins A and E. Plant-based diets, rich in whole grains, fruits, vegetables, and legumes, offer a promising strategy to address these deficiencies while potentially leveraging their anti-inflammatory and neuroprotective effects to improve mental health outcomes. The clinical implications of these findings underscore the importance of integrating nutritional counseling and plant-based dietary interventions into SUD treatment programs. Structured dietary support could enhance recovery by addressing physical health deficits, stabilizing mood, and reducing relapse risk, ultimately providing a more holistic approach to SUD care. To address current knowledge gaps, future randomized controlled trials should focus on assessing the efficacy of whole, minimally processed plant-based dietary interventions in improving both physical and mental health outcomes in populations with SUD.
To address current knowledge gaps, future randomized controlled trials should focus on assessing the efficacy of whole, minimally processed plant-based dietary interventions in improving both physical and mental health outcomes in populations with SUD. These trials should evaluate changes in nutrient biomarkers, such as iron, folate, and omega-3 fatty acids, to better understand the impact of plant-based diets on addressing common deficiencies. Mental health outcomes, including reductions in symptoms of depression, anxiety, and relapse rates, should also be a primary focus to determine the psychological benefits of dietary interventions. Additionally, studies should investigate the feasibility of implementing plant-based nutrition programs in both clinical and community-based SUD treatment settings, considering practical factors such as patient adherence, accessibility, and cost. Finally, future research should explore the role of socioeconomic barriers and access to plant-based foods to ensure equitable implementation and sustained benefits for diverse populations with SUD. By addressing these gaps, future research can provide stronger evidence to inform the integration of plant-based dietary interventions into standard SUD treatment protocols, enhancing both physical and mental health outcomes in this vulnerable population.
Footnotes
Acknowledgements
The authors would like to extend their sincere gratitude to the librarians at the Moody Medical Library, University of Texas Medical Branch, for their invaluable assistance and support. Their expertise and dedication in providing essential resources greatly facilitated the completion of this research.
Data Availability Statement
The data used in this systematic review are derived from previously published studies, which are cited throughout the manuscript. As this study synthesized data from publicly available sources, no new data were generated or analyzed. Further details on data sources can be obtained from the referenced articles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance,Ethical Standards,and Ethical Approval
As this study is a systematic review of previously published data, it did not involve human participants and was therefore exempt from Institutional Review Board (IRB) approval in accordance with the guidelines at the University of Texas Medical Branch.
Informed Consent Statements
Informed consent was not required for this study as it utilized publicly available data from published literature, ensuring compliance with ethical standards for systematic reviews.