
Abstract
Background:
Methamphetamine and other stimulant use are increasing across Mexico while treatment options and public funding remain scarce for substance use treatment. This study examined the attitudes and perspectives of service providers who work with persons who use stimulants in Mexico.
Methods:
Semistructured qualitative interviews were conducted with 20 service providers in diverse cities in the northern and central regions of Mexico, from healthcare centers and harm reduction community-based organizations (CBOs). All interviews were audio-recorded, transcribed, and de-identified. We conducted a thematic analysis to identify and compare common themes and patterns among participants, including portrayal of persons who use stimulants, dynamics of use, attitudes toward persons who use stimulants, and treatment availability and effectiveness.
Results:
First, service providers considered that persons who use stimulants have more complex backgrounds than others who use other substances. Second, although most providers mentioned trauma, pain, and the risk environment, CBO providers also stressed the importance of accounting for hedonism for understanding stimulant use trajectories. Third, treatment options are based on the type of services the institutions provide, usually constrained to guidelines for any substance use. In a few cases, cocaine treatment guidelines are used regardless of the type of stimulant used. Fourth, although health care services are abstinence-based, providers acknowledge the effectiveness of harm reduction approaches. In contrast, CBOs provide person-centered options.
Conclusions:
Overall, although service providers are aware of the increase in stimulant use, stigmatizing attitudes are prominent among some of them. However, providers in CBOs were more sensitized to their communities’ specific needs. Public policy recommendations include training to eliminate institutional stigmatization, the importance of first-person language, harm reduction effectiveness, and implementing community-based interventions to improve stimulant use-related services.
Highlight
This research points to the need for policies that incorporate training for health providers in person-first language and for reducing stigma toward persons who use stimulants.
There is a potential interest in health professionals to incorporate harm reduction strategies in public settings.
Introduction
Internationally, stimulant use has steadily increased over the last decade. 1 In Mexico, according to the most recent official public data, more than half of the persons who sought care in the past year were for amphetamine-type stimulants (ATS; 59.8% total; 59.7% of men; 60.6% of women). 2 In the same period, treatment for cocaine use represented 6.8% of the care sought (7.2% men and 4.2% women). 2 Specifically in the Metropolitan Area of Mexico City, substance use treatment is primarily sought for cocaine (including crack cocaine), ranging from 14.1% to 22%. 2 These proportions are 2- and 3-fold the national average (8.2%). 3 Although still lower than the national average (30.2%), ATS treatment-seeking has increased from 1.1% in 2013 to 8.9% and 17.2% in 2023.2,4
Most substance use interventions at the national and international levels have aimed for abstinence.5,6 However, as with other substances,7,8 such interventions have reported inconclusive results regarding their effectiveness in treating stimulant use.9-12 Alternatives to abstinence-based programs, such as harm reduction, may be more effective for this specific type of substance use.13,14 Persons may be more likely to express a willingness to access harm reduction interventions rather than abstinence-based programs, 15 depending on the stage of change they may be. 16 The current Mexican federal administration has shown a public interest in addressing substance use through a harm reduction perspective. 17 However, to our knowledge, there is still no public intervention from this perspective.
Previous studies have analyzed the stakeholders’ perceptions of substance use treatment barriers.18-20 However, the perspectives and experiences of treatment providers are also essential to assess opportunities and barriers to implementing changes in substance use treatment.21-23 Therefore, we aimed to learn about the experience of persons employed at public and private health services, as well as harm reduction community-based organizations (CBOs) that serve persons who use stimulants in Mexico. Specifically, we inquired about the care strategies they used and the results they obtained based on their perspective of stimulant use and the persons who use them.
Methods
In the following paragraphs, we detailed the methods using the consolidated criteria for reporting qualitative research (COREQ) checklist. 24
From September to December 2022, we conducted semistructured interviews with health professionals recruited through a convenience sampling methodology. Participants provided psychosocial treatment, harm reduction services, and other services (eg, sexually transmitted infections screening, prevention, and treatment) in Mexico’s Northern and Central regions. 27 participants were contacted by email, of whom 20 were interviewed, and 7 did not reply for unknown reasons. The interviewers met participants in the providers’ work locations in a quiet setting. If their agenda did not match or were in different cities, the interviews were performed via Zoom (n = 8). The first author knew some of the participants through their work in harm reduction. A couple of participants were acquaintances of collaborators of the research team; however, none of the interviewer–interviewees dyads comprised persons who had previously known each other. The interviews were conducted by 4 interviewers, all previously trained in health and social science procedures; they were all research assistants completing their undergraduate (2 cis-women) and graduate (2 cis-men) thesis projects in psychology.
We developed the interview guide (Supplemental Material 1), which consisted of the following topics: (1) characteristics of persons who use stimulants (eg, Overall, are there any features that distinguish persons who use stimulants from those who engage in other types of substance use?), (2) context and dynamics of use (eg, In which contexts are stimulant used by the persons you treat? [eg, for studying, weight loss, sexual, partying]), (3) interventions (eg, Could you please describe what the stimulant use treatment you provide consists of? [eg, length, techniques, goals]), (4) availability of services and referral system (eg, Which health services [eg, medical, psychological] are available for persons who use stimulants?), and (5) substance use policies (eg, Are you aware of the changes implemented in April 2022 in the General Health Law regarding mental health and substance use disorders?). For the interviews, all participants agreed to be audio-recorded about sharing their experience providing services to persons who use stimulants and signed an informed consent form. Interviews lasted approximately an hour, and notes were taken at discretion. All participants were interviewed once, and they did not review the transcript.
Each interview was professionally transcribed, and 2 research team members independently coded them based on the codebook. The codebook was designed based on the interview guide; emerging topics were added by the 2 research members when needed. A third member read all the transcripts and resolved potential discrepancies. After coding, they performed content analysis 25 to identify common attitudes and perspectives toward persons who use stimulants. All the analyses were performed using the NVivo 10 software. 26 Participants did not provide feedback on findings. The Ethics Committee of the Faculty of Psychology, Universidad Nacional Autónoma de México approved this study.
Results
The sample consisted of 20 health professionals who provide services to persons who use stimulants in Mexico (Table 1). More than half of the participants were men (55%), had a median age of 38, lived in the central region of the country (65%), had a median of 8 years of experience, and almost half worked at primary care centers (45%).
Sociodemographic Characteristics of Health Professionals That Provide Services to People Who Use Stimulants in Mexico (N = 20).
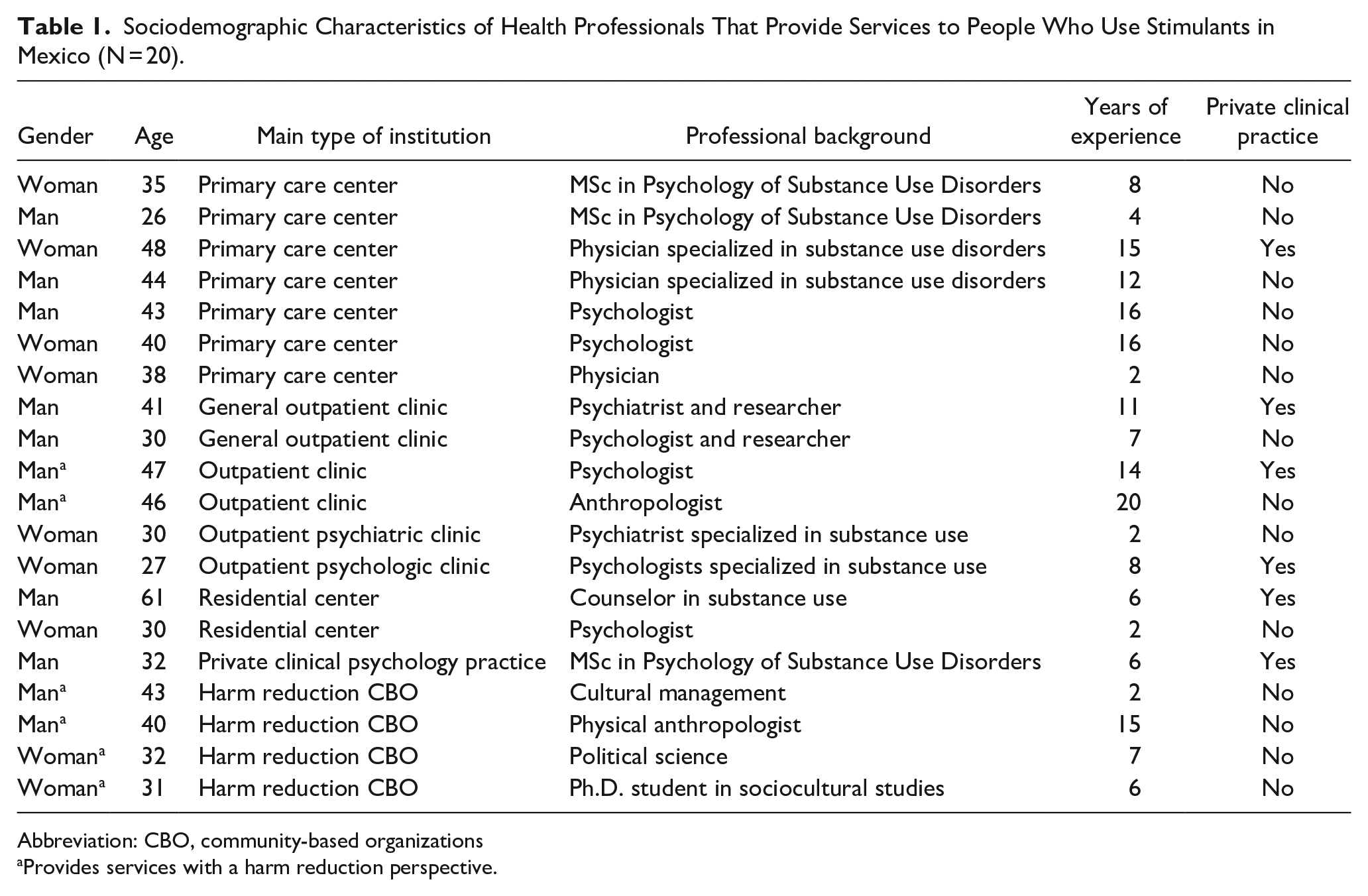
Abbreviation: CBO, community-based organizations
Provides services with a harm reduction perspective.
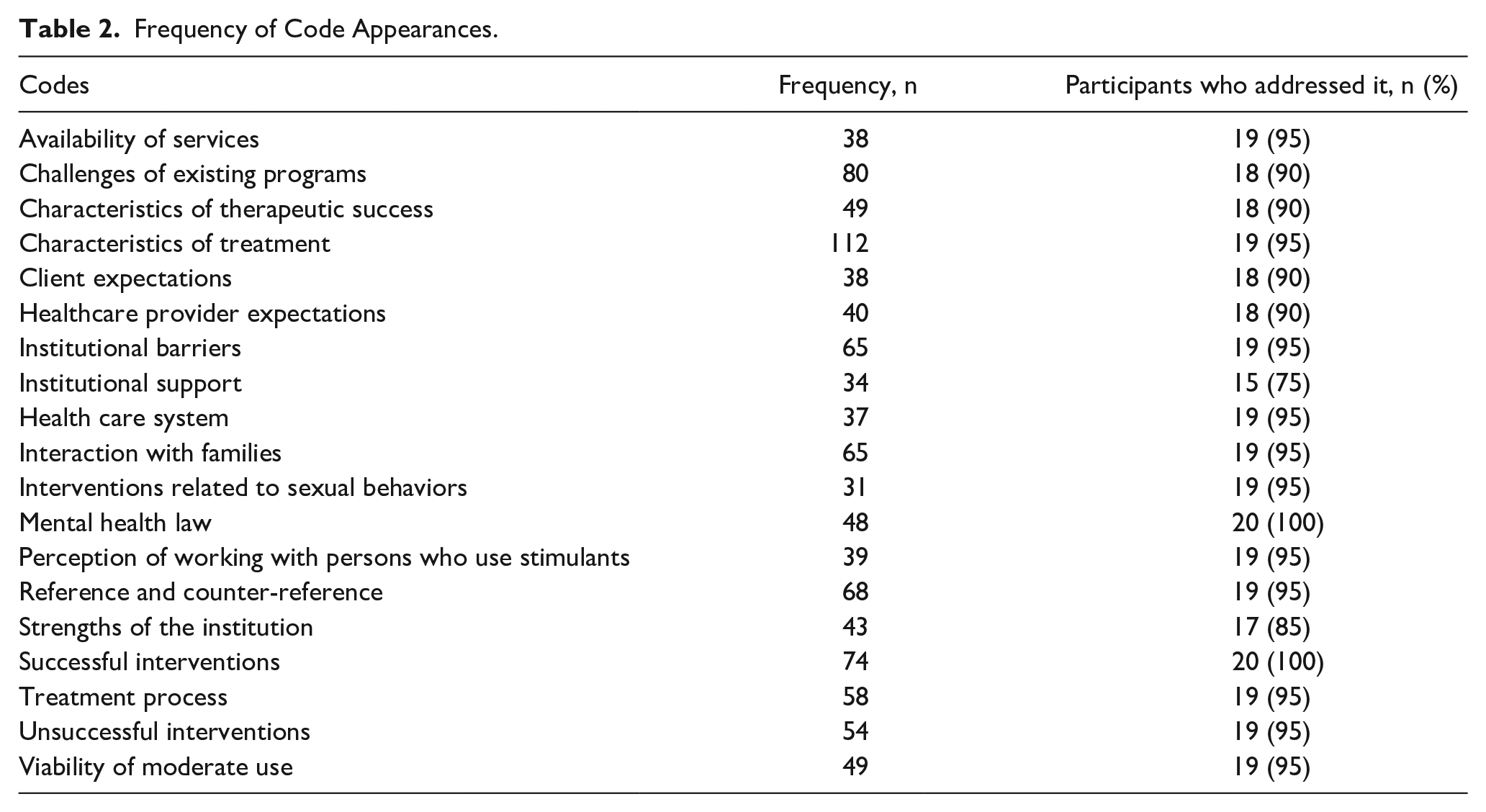
Based on the interviews and fieldwork, we identified 19 codes (Table 2); 2 major themes were identified: (1) the portrayal of persons who use stimulants and (2) interventions for stimulant use. In the following paragraphs, we present the findings. For the quotes we selected to sustain our analyses, we used the closest terms in English to evidence the differences in wording and style participants used to express themselves. In each quote, the participant’s gender, age, and main employer were identified.
Frequency of Code Appearances.
Portrayal of Persons Who Use Stimulants
Based on the target population service providers usually engage with, they perceived different characteristics of persons seeking treatment for stimulant use. In the following paragraphs, we elaborate on the (1) sociodemographic characteristics, (2) stimulant use initiation, (3) continued stimulant use, (4) mental health and traumatic experiences, (5) sexual diversity, and (6) women who use stimulants.
Sociodemographic Characteristics
Most of them agreed that they were seeing a younger population compared to persons seeking treatment for other substances. However, this portrayal differed in terms of educational attainment and socioeconomic status. Some participants considered stimulant use to be steadily increasing among persons with higher education, formal jobs, and higher socioeconomic status. In contrast, others thought most persons who use stimulants have low educational attainment and informal jobs.
Participants located in the Northern region emphasized the higher prevalence of stimulant use among sex workers and persons unhoused with an informal income source, such as persons who work in recycling (“recicladores”), working-class persons, construction workers, and migrants.
They seek for recycling materials, they work in construction, [. . .] in (City in the Nothern region) we saw the same profile [compared to another city outside of the Metropolitan Area of Mexico City], working class, sex workers, migrants [. . .]. Woman, 31, CBO.
In contrast, a participant working in Mexico City at a public clinic made a stigmatizing depiction of marginalized persons who use stimulants: They are persons that failed academically and, consequently, there is a cycle of poverty, right? Imagine the misery and fragility because they are already engaged in urban tribes that prevail in some parts of the city. . . most of the time, their substance use leads them to.. not prostitution [sic] as such, but some agreement with someone in exchange for substances. Man, 47, Outpatient clinic.
It can be noted that while both participants referred to sex work, the language and patronizing tone differed in the latter quote.
Stimulant Use Initiation
Reasons for initiation also varied according to participants’ own lived experiences. For instance, participants working in harm reduction services and with lived experience considered curiosity a key factor (“I think [stimulant use] starts with curiosity and experimentation, but I also think it is a way to connect with others” Man, 43, Primary Care Center). In contrast, persons who did not report prior stimulant use considered mainly the context as a critical factor (“The risk environment, the family uses [substances], places in which there is high criminality and substance use.” Woman, 27, Outpatient Psychologic clinic).
Continued Stimulant Use
There were different theories on the rationale of continued stimulant use after the experimentation phase. Some participants considered that persons engage in stimulant use due to hedonic sensation-seeking: [. . .] pleasure related to sex but also the simple pleasure, to be fulfilled, to feel good, right? [. . .] not only the pleasant effect that the substance provides pharmacologically, but the pleasure of self-fulfillment and, in a way, the self-exploration, it is a subjective effect. Woman, 32, CBO.
Other providers reported a more complex analysis, which included the context of this hedonic sensation-seeking. For them, most of their clients come from dysfunctional families, and by using substances with persons with similar backgrounds, they compensate for the perceived lack of support. Clients tend to suffer negligence and abandonment; their relatives and toxic family environments forget they exist, and belonging to a social network makes them feel better.
Mental Health and Traumatic Experiences
In terms of mental health, there are some characteristics identified with the profile of stimulant use, such as having low self-esteem, depressive disorders, unsolved grief, feelings of guilt, sadness, anger, fear, history of trauma, loss of meaning, and constant frustration. Also, it may be more likely for someone to use stimulants if they find them useful: Several people develop an addiction [sic] or a problematic crystal meth use because of two elements: trauma and pain [. . .] it is unlikely that a person develops an addiction [sic] or a problematic use without a background of childhood trauma or without having been neglected, without emotional pain throughout their childhood or adolescence. Man, 46, Outpatient clinic
Most of their clients have experienced traumatic events throughout their life span, including sexual violence during childhood and grief for the loss of someone close. Providers also identified an impulsive profile among persons who use stimulants, which impacts their decision-making processes and coping styles: Impulsiveness is a trait that I see more often in persons who use stimulants, but not in persons that use other substances like depressors or hallucinogenics. The latter have more caution; they control themselves more [. . .] In this addictive profile, they [persons who use stimulants] tend to be impulsive persons who do not assume responsibility for their behaviors and their consequences, they do not assess the consequences of their acts and may even already have psychotic episodes. Man, 43, Primary Care Center.
Sexual Diversity
Participants were asked about their thoughts on stimulant use by persons from the LGBT+ community and women regardless of their sexual orientation. Most of the sample considered LGBT+ persons who use stimulants face several situations that have a great effect on them at a social level, including violence, homophobia, traumatic events, social exclusion, marginalization, and stigma. In this context, some persons have a heightened social vulnerability because they live with HIV. Providers stated that some of their clients who live with HIV use stimulants as a way “to escape from reality” and cope with stigma and social exclusion.
Women Who Use Stimulants
In the case of women, most providers considered weight control as the main reason women use stimulants. However, several participants also elaborated on more profound, more complex associations with stimulant use. A participant stated that women do not engage like men do in “self-destructive behaviors” because women support Mexican households. Consequently, women have to have a “stoic attitude.” In contrast, others considered that vulnerability for women is related to machismo, sexual violence, economic violence, low socioeconomic status, and isolation perpetrated by their partners and children: Among the women I have treated, [their stimulant use] is associated with their social context. Most of the time, they are women in high vulnerability, from violent families, with a history of abuse who engage in this, say, this dynamic of dating partners that offer them [substances]. However, cases of women that I have seen who have a stimulant use disorder are very vulnerable. They are women with high levels of poverty or women that have an extremely violent background, that is, for crystal meth. In terms of cocaine, they are women that are more, say,. . . college students, or who have completed high school, even with an undergraduate degree. Woman, 30, Residential center.
Women’s use was also reported by other participants to be related to their partners. That is, it is a private and intimate substance use that their partners promote.
Interventions for Stimulant Use
There was a wide range of perspectives on interventions for stimulant use. We report them in the following subthemes: (1) treatment options, (2) treatment goals for persons who use stimulants, (3) providers’ expectations, (4) characteristics of successful stimulant use interventions, and (5) unsuccessful interventions for stimulant use.
Treatment Options
Treatment services offered for stimulant use vary according to the approach, therapeutic strategies, and length of the intervention. Most providers offered psychological treatment based on cognitive-behavioral treatment for cocaine use, regardless of the type of stimulants they use. Assessment, diagnosis, and interventions typically used include intake, standardized assessments, motivational interviewing, cognitive restructuring, psychoeducation, and substance use behavior functional assessment. Moreover, treatment is focused on creating more awareness about their substance use, weighing negative over positive consequences with the aim of finding alternative behaviors, usually abstinence-based. In terms of psychosocial approaches, providers also used Social and Recreational Counseling: Due to the type of substance use [stimulants], and the consequences it has had on their lives, we work with Social and Recreational Counseling. This program includes elements such as functional behavior assessment, mood regulation, life goals setting, communication abilities, social abilities, and recreational abilities; sometimes we also include job seeking and maintenance. Woman, 35, Primary Care Center.
In contrast, persons who work at CBOs considered treatment goals and intervention strategies must be client-based and consented by them. They also mentioned that interventions do not necessarily need to seek abstinence but harm reduction approaches, which include providing paraphernalia (eg, pipes, lip balm), drug-checking services, psychoeducation, and other harm reduction strategies (eg, condoms, lubricants, dental care). Harm reduction approaches were clearly acknowledged as not treatment per se but an intervention that focuses on meeting and supporting people where they are at We have a harm reduction program, which is not treatment but an approach, harm reduction counseling. We refer to treatment when the person needs it and agrees to engage in treatment. We also provide kits that include syringes or disposable pipes. We also provide psychotherapy. Man, 46, Outpatient HIV Clinic.
Pharmacological treatment may include stimulant-assisted therapy (eg, methylphenidate and topiramate) and prescriptions for any comorbidity the person may have. This usually includes antidepressants, mood stabilizers, anxiolytics, anticonvulsants, and antipsychotics. In addition, a participant mentioned that antihistaminics are used to control physical craving symptoms. A participant delved into their use of pharmacological treatment: I have seen success, or at least more treatment adherence, when combining a stimulant with a craving regulator. In this case, we use topiramate with methylphenidate or bupropion. Woman, 30, Residential center.
Treatment Goals for Persons Who Use Stimulants
There was a notable difference between providers in mainstream treatment services and harm reductionists in terms of treatment goals. Most of the participants employed at health institutions stated that the final aim of treatment must be abstinence and complete remission due to the deleterious physical and psychological harms caused by stimulant use. However, they also mentioned that the goals of the intervention need to be set along with the persons who use stimulants to establish a therapeutic alliance and increase the odds of treatment adherence. In contrast, participants from CBOs reflected on how challenging abstinence may be for persons who use stimulants. As such, short-term goals of decreasing substance use and harm reduction strategies are pertinent intervention approaches.
Providers’ Expectations
Most participants reported that their main expectation is to achieve treatment adherence since it is the only way to achieve their clients’ treatment goals. More specifically, participants associated treatment adherence with the disposition and motivation for change, and family support. Some participants considered a decrease in stimulant use as part of a loop of mood changes. That is, mood may improve once the client decreases/abstains from stimulant use, and this may relate to maintaining a better emotional state from the clients’ mood prior to decreasing their use. Consequently, providers expect more functional behaviors in the social, family, and work spheres.
While most of the participants stated that their main treatment goal is always abstinence, harm reductionists addressed how abstinence as a core element stigmatizes persons who are not reaching that stage, even if they aim for it.
When we aim for 100% abstinence, clients get tired of always getting the same information. They do not engage in a trusting way to services. Man, 46, Outpatient HIV clinic.
Few participants acknowledged the difficulties of achieving decreases in stimulant use. Consequently, they do not aim for abstinence per se, or they do not consider it as a short-term treatment goal. This recognition of the complexities of achieving abstinence includes external factors that the client cannot control. Realistic expectations include that most of the time, clients do not achieve abstinence but a more controlled stimulant use that allows them to regain stability. In this case, the complexities include stigma and social exclusion, as a participant expressed: There are persons able to control this [stimulant use], and they can keep on with their lives while using. However, it is hard. Unfortunately, since there is no information, no support from anyone or any public institution that assist. . . not only that, there is stigma [at public institutions] and people isolate. Man, 40, CBO.
Characteristics of Successful Stimulant Use Interventions
The most mentioned factor was the person-based approach, including scheduling appointments with a flexible schedule, follow-ups, and setting goals based on the client. Other characteristics include a multidisciplinary team, training to avoid stigma, and reinforcing in the clients the importance of social support and networks: That they realize they are more than their substance use. This allows me to have better results because treatment is not only addressing their use but also other areas, like getting a job, going back to school, and so on. This allows me to have a better result during follow-ups because they are having more and more reinforcers other than substance use. Woman, 40, Primary Care Center.
Providers considered that treatment success depended on the motivation of their clients rather than on the treatment approach they used. Commitment and motivation to change are considerably important to achieving treatment goals: Persons that get the most out of treatment are the ones that are constant. It does not matter if it [treatment approach] is cognitive-behavioral, AA, pharmacological. . . people that have. . . or are still able to be constant, of being longer in treatment, are more likely to be successful. Man, 30, General outpatient clinic.
Most of the participants considered that evidence-based approaches are the most successful, especially cognitive-behavioral therapy (CBT) and contingency management for stimulant use and relapse prevention. In addition to CBT, pharmacological treatment, behavioral approaches, and even mindfulness are considered effective if adapted to the client’s needs. Regarding pharmacological approaches, participants considered the best approach was the combination of pharmacological and psychosocial interventions and to collaboratively work with interdisciplinary teams.
Other participants referred to harm reduction as the most successful approach because its philosophy allows persons to reflect on their use without judgment and assess the risks and contexts of use. Also, it provides useful techniques for safer use, including overdose prevention and first aid techniques. A change in narrative is also advised: . . . discrimination and eradication of stigma is a key aspect. This is an extremely difficult topic because we have introjected the structural discrimination towards persons who use stimulants, and we need, to at least, begin by sensitizing [treatment providers]. Man, 40, CBO.
Providers with lived experience of stimulant use stressed the importance of peers in treatment; they have a broader perspective compared to other providers who only have a professional perspective. Also, participants commented on the importance of having group meetings in settings in which treatment is provided individually, as well as the participation of family and significant others for support.
Unsuccessful Interventions for Stimulant Use
Treatment that is only based on guidelines without considering the nuances of the context of each client tends to be unsuccessful. Also unsuccessful treatment approaches are those that do not include in their teams persons with lived experience. Other unsuccessful approaches involve treating all substance use the same way.
Another frequent practice that some providers identified was the misconception of sexualized substance use (known as chemsex in different contexts; however, there is controversy regarding using the term by those who engage in it in Mexico) and the specific needs of persons who engage in chemsex: When I started treating chemsex, I found that people frequently sought treatment for it in sexual and reproductive care clinics, but they did not address the affective components. Psychologically, there was zero understanding of what occurred intimately, in their sexuality. At that point, the persons stop attending their appointments. Other people would seek sexual health care at one clinic and substance use treatment at a different place. Treating sex and substance use independently left patients feeling confused and guilty, which is related to dropping out of both treatments. Man, 32, Private clinical psychology practice.
Discussion
We sought to examine the attitudes and perspectives of service providers on persons who use stimulants in Mexico, where stimulant use has exponentially increased in the past decade.27,28 Overall, they acknowledged the specific needs persons who use stimulants have. However, providers in CBOs were more sensitized to their communities’ specific needs. Service providers in health professions reported to be more constrained to institutional guidelines.
Service providers elaborated on the rationale for the first and continued use of stimulants. While all were valid and based on their professional experience, some focused on immediate factors, while others elaborated on the complexity of the background in which persons choose to explore stimulant use. Immediate factors were mostly related to substance availability, as has also been reported in other settings. 29 Across both sets of reasons for stimulant use (ie, immediate and life-span context), there were also 2 prevailing theories: negative life events and hedonic sensation-seeking. There is evidence of the association between adverse events and stimulant use disorders, especially if those events occurred during childhood.30-32 Less research has been published related to hedonic stimulant use. A report found that there is a considerable proportion of persons who report pleasure as the main motive of stimulant use and that, for some, it may be possible not to develop risky use patterns.31,33 In Mexico, hedonic reasons have recently been explored; a study in Ciudad Juarez found that pleasure was reported by a quarter of the sample of men as the reason for crystal meth initiation. 34 In a previous study of our research team among gay and bisexual men who have sex with men 35 we found a similar proportion of reasons for initiation, but more than half of the sample reported pleasure as the main reason for current use, which was mostly related to sexualized use. Overall, more research is needed to explore the hedonism and stimulant use. In this line, it is also important to continue exploring the nuances of the use of “sexualized stimulant use” and “chemsex” in international settings. For some persons who engage in sexualized stimulant use in Latin America, the term “chemsex” does not fully cover the experience in low- and middle-income settings, in which the intersection of racialization, homonegativity, and other stigmas are more violent than in other settings.36,37
Our results highlight the need to address the stigma of health professionals toward women seeking substance use treatment in terms of access and quality of service provided to them. Women who use stimulants were considered more vulnerable than men. Some providers considered they generally had lived more violence and in a riskier environment than men. Also, providers reported on the potential initiation of substance use related to their partners and family contexts. This contributes to evidence on gender dynamics in substance use initiation38,39 other than injection. Other providers also elaborated on the increased barriers women face when they need treatment. Noncompliance with traditional gender roles may transform social support from significant others into negative attitudes, which may generate internalized stigma.40,41 While some persons who use stimulants may have comorbid mental disorders and may have suffered violence, the profiling and overgeneralization of such features further increase the stigma and reduce the likelihood of generating rapport and treatment engagement.
There is a need to train healthcare providers to identify the specific needs of people who use stimulants and, based on this, to set goals and design treatment. Moreover, it is essential to address the stigma that health personnel may have toward this population. Stigma may be one of the main treatment barriers and it may also be related to drop-out. Interventions to reduce stigma among healthcare personnel, including person-centered strategies and contact-based interventions, may be important components to achieve effective treatment outcomes.42,43 Also, first-person language has been consistently shown to be important to building rapport and ameliorating treatment barriers related to promulgated and anticipated stigma. 44
While acknowledging the complexities of stimulant use, including the risk environment, public health providers referred only have clinical guidelines for cocaine use, which are used to treat any stimulant. Although this may be the only option for providers, the inadequacy of the treatment may result in a treatment barrier in the future. Therefore, it is recommended that treatment policies engage in a person-centered approach and continue to seek effective methamphetamine treatment options. 45
Cognitive-behavioral techniques are effective for substance use treatment.46,47 However, there may be cognitive dissonance between recognizing the increased vulnerability of social contexts and using techniques such as functional behavior assessment. The health providers interviewed in this study were sensitized to their clients’ needs but reported challenges integrating this knowledge into their practice. This is an important barrier that could be addressed through changes in institutional policies and a more person-centered approach.48,49 Another important avenue for future research is medication treatment. The effectiveness of achieving abstinence from stimulant prescription for amphetamine-type use disorders remains controversial.50,51 Bupropion or a combination of bupropion-naltrexone has shown the most promising results.52,53
This study has several limitations. First, we relied on self-reporting of participants’ own practices. However, we purposively recruited participants from a broad range of service providers to increase the diversity of experiences and perspectives. Second, we also note the risk of social desirability bias, which could have interfered with the expression of unpopular accounts of the needs of persons who use substances. However, based on our findings, this may not have been a considerable risk for the study. Third, we were unable to interview service providers from the southern region of the country. Epidemiological data suggest that stimulant use is not as prevalent as in other regions, 54 but we were unable to investigate it further.
In summary, this research points to the need for policies that incorporate training for health providers in person-first language55-57 and for reducing stigma toward persons who use stimulants. There may be a potential interest in health professionals to incorporate harm reduction strategies, given the increased treatment seeking for stimulant use, especially methamphetamine.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241311665 – Supplemental material for Attitudes and Perspectives of Service Providers on Persons Who Use Stimulants in Northern and Central Mexico
Supplemental material, sj-docx-1-saj-10.1177_29767342241311665 for Attitudes and Perspectives of Service Providers on Persons Who Use Stimulants in Northern and Central Mexico by Claudia Rafful, Leonardo Jiménez-Rivagorza, Daniela Peralta, María Elena Medina-Mora and Andrés Mota in Substance Use & Addiction Journal
Footnotes
Acknowledgements
This study was funded by the Programa de Apoyo a Proyectos de Investigación e Innovación Tecnológica (PAPIIT) IA301422 Project. We thank Nely Gutiérrez, Missael Morales-Gutiérrez, María José Adaya, and Geram Melo for conducting and transcribing some of the interviews. We also thank Dr. Shoshana Berenzon at the National Institute of Psychiatry, Mexico for providing the analytical software. We also thank Pablo Caseiro for the feedback and input.
Author Contributions
CR: conceptualization, methodology, writing original draft, review and editing, and funding acquisition. LJ-R: investigation and writing – original draft. DP: verification and investigation. MEM-M: resources, and writing – review and editing. AM: formal analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Dirección General de Asuntos del Personal Académico, Universidad Nacional Autónoma de México (IA301422; PI: Rafful).
Compliance,Ethical Standards,and Ethical Approval
This study was approved by the Ethics Committee of the Faculty of Psychology, Universidad Nacional Autónoma de México (UNAM) on May 4, 2022 (FPCE_10022022_H_AC). Respondents gave written consent before starting interviews and additional consent for audio recording the interviews.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.