
Abstract
Background:
In Texas, the expansion of access to effective treatments for opioid use disorder remains a significant public health challenge. This study aimed to demonstrate the application of the Successful Healthcare Improvement from Translating Evidence in Complex Systems (SHIFT-Evidence) framework in developing and implementing a statewide network for office-based opioid treatment (OBOT) to underserved populations.
Methods:
We identified systemic gaps in access to medications for opioid use disorder (MOUD) across Texas, using a targeted needs assessment of barriers and facilitators to buprenorphine prescribing. Findings were integrated into a planning template based on SHIFT-Evidence, which guided the identification of additional barriers across the health care system and iterative selection of strategies to address implementation barriers at multiple health care system levels, drawing on the Expert Recommendations for Implementing Change taxonomy. Strategies were prioritized based on feasibility and impact. To evaluate the program’s effectiveness in expanding access to MOUD, we conducted a descriptive analysis of data from the Texas Department of State Health Services’ Clinical Management for Behavioral Health Services data system to assess geographic reach and clients served within the program.
Results:
Applying SHIFT-Evidence provided a structured process for identifying key barriers occurring at multiple levels (patient, prescriber, and prescriber organization) and selecting tailored strategies to address each. This approach supported the successful development and expansion of an OBOT provider network, increasing access to treatment services from 6 provider organizations (10 locations) serving 52 clients in fiscal year 2019 to 23 provider organizations (48 locations) serving 1311 clients in fiscal year 2023.
Conclusions:
The comprehensive, multilevel approach supported by the application of SHIFT-Evidence effectively facilitated prioritization and planning to address systemic gaps across multiple health care system levels. The successful enhancement of treatment access highlights the framework’s utility in supporting improvements within complex health care systems.
Keywords
Highlights
Demonstrates the practical utility of the SHIFT-Evidence framework for comprehensive planning and implementation of complex, large-scale public health initiatives.
Provides evidence for the effectiveness of integrating multi-level strategies in achieving systemic healthcare improvements.
Highlights the value of implementation frameworks for overcoming barriers in expanding treatment for substance use disorders.
Introduction
Buprenorphine is an evidence-based medication for the treatment of opioid use disorder (OUD) that is accessible outside of traditional licensed opioid treatment programs. 1 The Food and Drug Administration’s approval of buprenorphine in 2002 provided a means to expand access to medication for opioid use disorder to outpatient settings, including primary care and substance use treatment programs. 1 Despite buprenorphine’s effectiveness and the unremitting opioid overdose epidemic in the United States,2,3 uptake into office-based treatment locations has remained slow.
Texas is the second-largest state in the United States in terms of land area and population, representing approximately 9% of the total United States population across its 254 counties.4,5 Preliminary data estimate the 2021 OUD prevalence for Texas adults ages 18 and older at 2.03%, slightly lower than the national estimated prevalence of 2.09%. 6 However, this still represents a substantial number of individuals, with approximately 609,600 people in Texas affected by OUD. The 12-month-ending provisional counts of overdose deaths in Texas as of August 2023 are 5566 drug overdose deaths (56% were opioid related), a 65% increase compared to August 2020. 7
The lack of access to evidence-based treatment for OUD (ie, medications for opioid use disorder [MOUD]) is well-recognized and multifaceted.8,9 The Health Resources and Services Administration (HRSA) currently designates 181 areas across 154 Texas counties, approximately 60% of Texas’s counties, as being medically underserved. 10 Medically underserved areas are geographic regions, usually counties, that have a shortage of primary care health services. 11 Moreover, the availability of health care providers who prescribe buprenorphine for OUD is more than half the national average, estimated to be approximately 5.46 buprenorphine providers per 100,000 in Texas compared with 14.3 providers per 100,000 individuals nationally. 12 Treatment access is further compounded by the high rate of Texas residents without health insurance. Texas has the highest number of uninsured individuals in the United States: 17% of Texans (or 4.9 million people) were uninsured in 2022, more than double the national average of 8%. 13 Additionally, 81% of the uninsured in Texas are of working age (ages 19-64), which is also the age range of most people with an OUD who are seeking treatment.
Nationally, statewide approaches to expanding access to office-based opioid treatment (OBOT) for OUD are largely based on a Hub and Spoke model, which has been lauded as a method for assisting rural areas that are especially impacted by OUD. 14 A primary aim of the Hub and Spoke system, as described by Brooklyn and Sigmon, 15 is for patients to transfer between hub and spokes bidirectionally. For example, once patients have stabilized on buprenorphine at a hub site, they may be referred to a spoke provider for follow-up in their own community; patients can later be transferred back to a hub if they destabilize in the spoke setting. 15 Several states have implemented versions of a Hub and Spoke model to expand access to MOUD in office-based settings, including Vermont, California, and Washington State, and have seen positive results, including substantial increases in providers serving patients with OUD, and increased ability to manage patients in their local communities.15-17
While the Hub and Spoke model has shown effectiveness in various states, its adoption and implementation are influenced by unique local challenges and conditions. Factors such as the COVID-19 pandemic, the increasing prevalence of fentanyl, and regulatory changes (eg, such as the requirement of a waiver [the so-called X-waiver] to prescribe buprenorphine prior to 2023), have further complicated the landscape of MOUD treatment. These developments underscore the need for coordinated, long-term, and multilevel strategies tailored to state-level efforts.18-20 Grounding these comprehensive efforts in health care improvement and implementation frameworks, such as the Successful Healthcare Improvement from Translating Evidence (SHIFT-Evidence), provides a structured roadmap for addressing such complex challenges. The SHIFT-Evidence framework helps guide programs toward success by leveraging best practices in structured and systematic implementation, facilitating continuous improvement, and adapting to evolving conditions. In this paper, we describe our application of the SHIFT-Evidence framework for planning and implementing a tailored Hub and Spoke model to meet the unique challenges of MOUD expansion across Texas.
Methods
In the Fall of 2019, UT Health San Antonio entered into a contractual agreement with the Texas Health and Human Services Commission (Texas HHSC) agency as part of the Texas Targeted Opioid Response public health initiative. The objective of this partnership was to conceptualize, procure, and implement services aimed at enhancing the availability of MOUD through the delivery of OBOT for individuals with OUD. This effort emphasized meeting the treatment needs of individuals lacking insurance coverage, residing in geographically remote or rural areas, grappling with polysubstance use, and/or historically underserved by health care services. 21
Implementation Framework
Our approach to program development and implementation planning was grounded in SHIFT-Evidence, which was developed based on an analysis of best practices in implementation across regional and national health care systems in the United Kingdom. 22 This framework proposes a series of 3 strategic principles, each with 4 associated rules.
The first principle, act scientifically and pragmatically, balances the need for fidelity to evidence-based practices with the need to adapt practices to meet local needs and context. Associated rules for this principle include leveraging existing resources and infrastructure, using data to drive decisions, and iteratively testing and refining interventions. These rules encourage implementation efforts that are evidence-based, adaptable, and sustainable, ensuring that interventions remain effective and relevant to the local context.
The second principle, embrace complexity, acknowledges that health care delivery requires collaboration and coordination among many individuals acting within a dynamic context. Associated rules for this principle include building a shared understanding of the problem, codesigning solutions with implementation partners, engaging partners early and often, and facilitating continuous learning to adapt to emerging needs. These rules emphasize the importance of partner engagement and adaptability, ensuring that interventions are collaboratively designed and responsive to the complexities of health care environments.
The third principle, engage and empower, explicitly builds in partner participation to ensure the introduction of novel practices into routine care in a manner that is feasible, acceptable, compatible with existing workflows, and sustainable.23,24 Associated rules for this principle involve fostering active participation from all relevant parties, integrating interventions into routine practice, and continuously monitoring and evaluating progress. These rules are intended to ensure partner buy-in, seamless integration of new practices into existing systems, and ongoing assessment to ensure interventions remain effective and aligned with organizational needs.
SHIFT-Evidence also recommends using coordinated implementation strategies occurring at multiple levels of the health care system (eg, patient, prescriber, prescriber organization) to facilitate impactful change. We selected SHIFT-Evidence as a guiding framework because it is based on real-world implementation findings, supports the development of multilevel and multifactorial implementation approaches, and is aligned with the needs and values of our partnership with Texas HHSC. In approaching the development of a statewide OBOT-delivery initiative, we drew upon the framework to identify barriers at multiple system levels and develop a systematic implementation plan, as described below.
Operationalizing SHIFT-Evidence
Our multidisciplinary program implementation team, comprised of experts in implementation science, substance use disorder (SUD) treatment, service coordination, evaluation, and data management, developed a practical instrument to operationalize SHIFT-Evidence into a format that was more accessible enabling the team to apply the framework systematically. This effort resulted in a planning template that structured the framework’s 3 principles and associated rules along the vertical axis, with relevant health care system levels (patient, prescriber, and prescriber organization) delineated horizontally across the top (see Table 1). Under each health care system level, columns provided space for detailing critical information about barriers, implementation strategies, and approach.
SHIFT-Evidence Planning Tool.
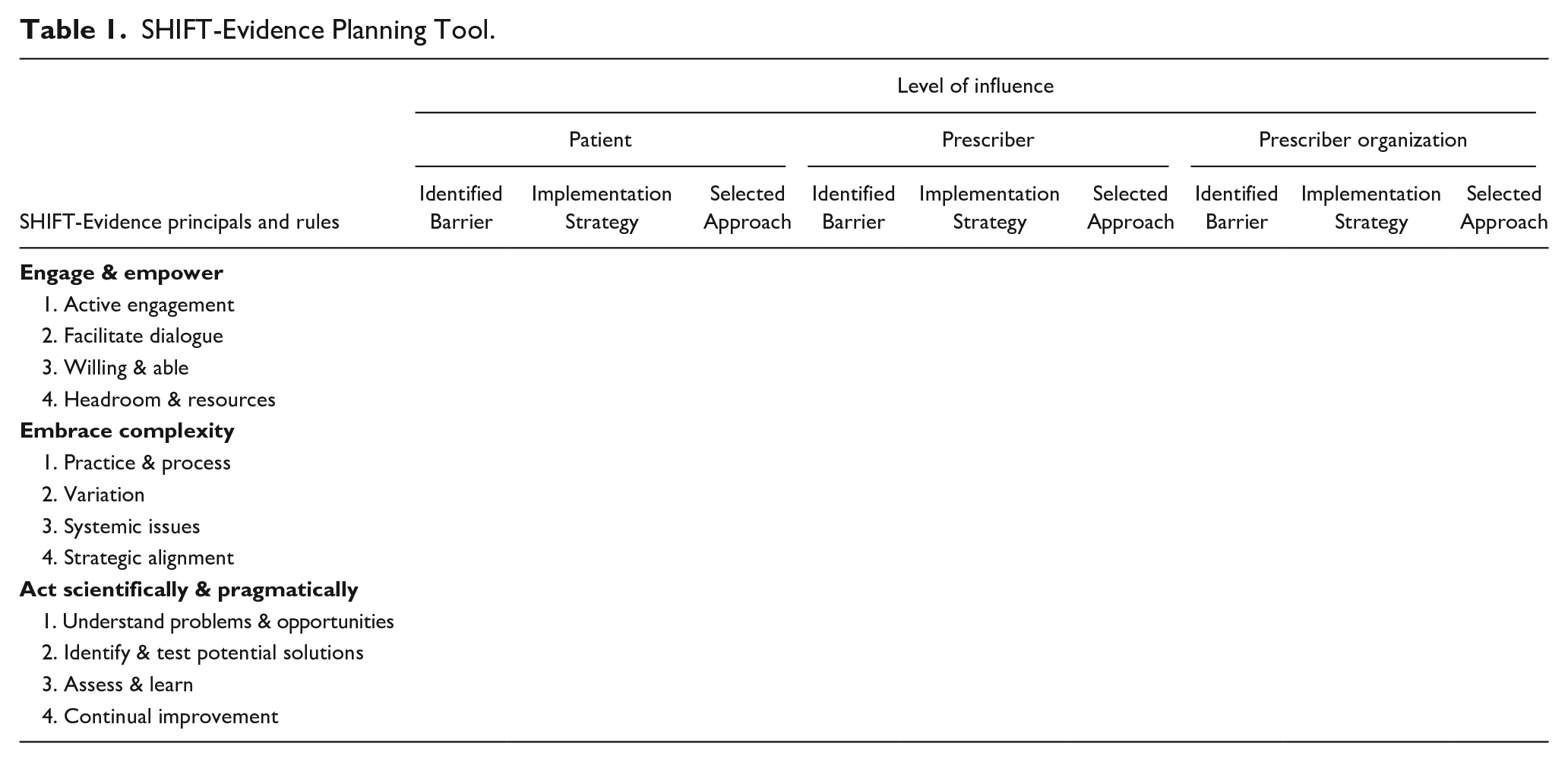
The design of the planning template enabled a more accessible and actionable approach to applying the 3 main principles and associated rules of SHIFT-Evidence. This allowed for a thorough delineation of key barriers across all health care system levels and framework constructs. We describe the full sequence of steps, from needs assessment to program development and implementation, in the Results section.
Program Evaluation
Once the program, Texas Medications for Opioid Use Disorder (TxMOUD), was launched, program evaluation efforts focused on assessing prescriber organization adoption and network reach as primary indicators of success. Provider organization adoption, that is, the cumulative number of providers contracted with TxMOUD year over year, signifies the organizational commitment to integrating or expanding MOUD in their treatment facilities. Network reach encompasses the count of individuals receiving MOUD at any of the contracted treatment facilities, as well as the geographical distribution of these facilities across the state. Utilizing a descriptive analysis of data from the Clinical Management for Behavioral Health Services (CMBHS) system, we tracked the evolution of provider organization adoption and network reach to understand the program’s progress from its initial launch in Spring 2020 through August 2023.
Results
Needs Assessment Survey
In the initial phase of our project, we began with a needs assessment grounded in SHIFT-Evidence principles, focusing on the identification and understanding of the prevailing challenges associated with MOUD prescribing within Texas. 22 The team developed and deployed a survey to understand barriers and facilitators faced by Texas prescribers in providing care to individuals with OUD, specifically through MOUD. The survey was distributed to prescribers within the GetWaivoredTX network. 24 The GetWaivoredTX network, a training initiative aimed at expanding access to MOUD through a statewide X-waiver training initiative, served as an ideal context for assessing prescriber challenges due to its active engagement with health care providers across the state.
Barrier Identification and Prioritization
Survey responses revealed several main barriers to MOUD prescribing, including a lack of mentoring, with prescribers indicating a need for experienced mentors to guide them through prescribing and managing MOUD. The lack of knowledge on how to get started with MOUD also emerged, highlighting the necessity for clear, accessible guidelines and initial support. Additionally, a lack of available training and support emerged, as prescribers expressed the need for comprehensive training programs and ongoing support to build confidence and competence in MOUD prescribing. It is important to note that at the time of this survey (2020), prescribers were still required to obtain an X-waiver to prescribe buprenorphine, a significant barrier to increasing the number of clinicians capable of offering this treatment. Other barriers included the complexity of the X-waiver process, a perceived lack of professional support and referral networks, and difficulties accessing reimbursement for treatment. 25 For further details on the prescriber barriers identified, readers are referred to Lanham et al (2022).
Beginning with the results of the needs assessment, the team engaged in a series of working meetings and systematically analyzed and integrated findings into the planning template, ensuring alignment with the SHIFT-Evidence principles, rules, and relevant health care system levels. This integration was facilitated through a series of structured working meetings, where the planning template served as a critical tool for categorizing and discussing the identified barriers. These discussions not only contextualized the data within the framework but also expanded the scope of the analysis to encompass additional health care system levels, that is, considering not only prescriber-level barriers but also barriers at the level of the patient and prescriber organization, drawing on expert insights and the latest academic research on SUD treatment interventions. Given the robust array of barriers identified, the program team recognized the need to distill the list to isolate barriers most likely to impact program success.
In prioritizing barriers, the program team used an iterative process of consulting with state-level partners and local experts (eg, addiction psychiatrists) to reach a consensus on the most important and feasible barriers to address across health care system levels, considering budget constraints and resources. For example, the need for MOUD education and support was identified as a key barrier for both the individual prescriber and prescriber organizations. By identifying such cross-level similarities, the program was able to streamline efforts, addressing the barriers through shared interventions that could be applied across levels. This approach optimized the use of limited resources while ensuring that the most pressing challenges were addressed effectively and efficiently.
Mapping and Customizing Implementation Strategies
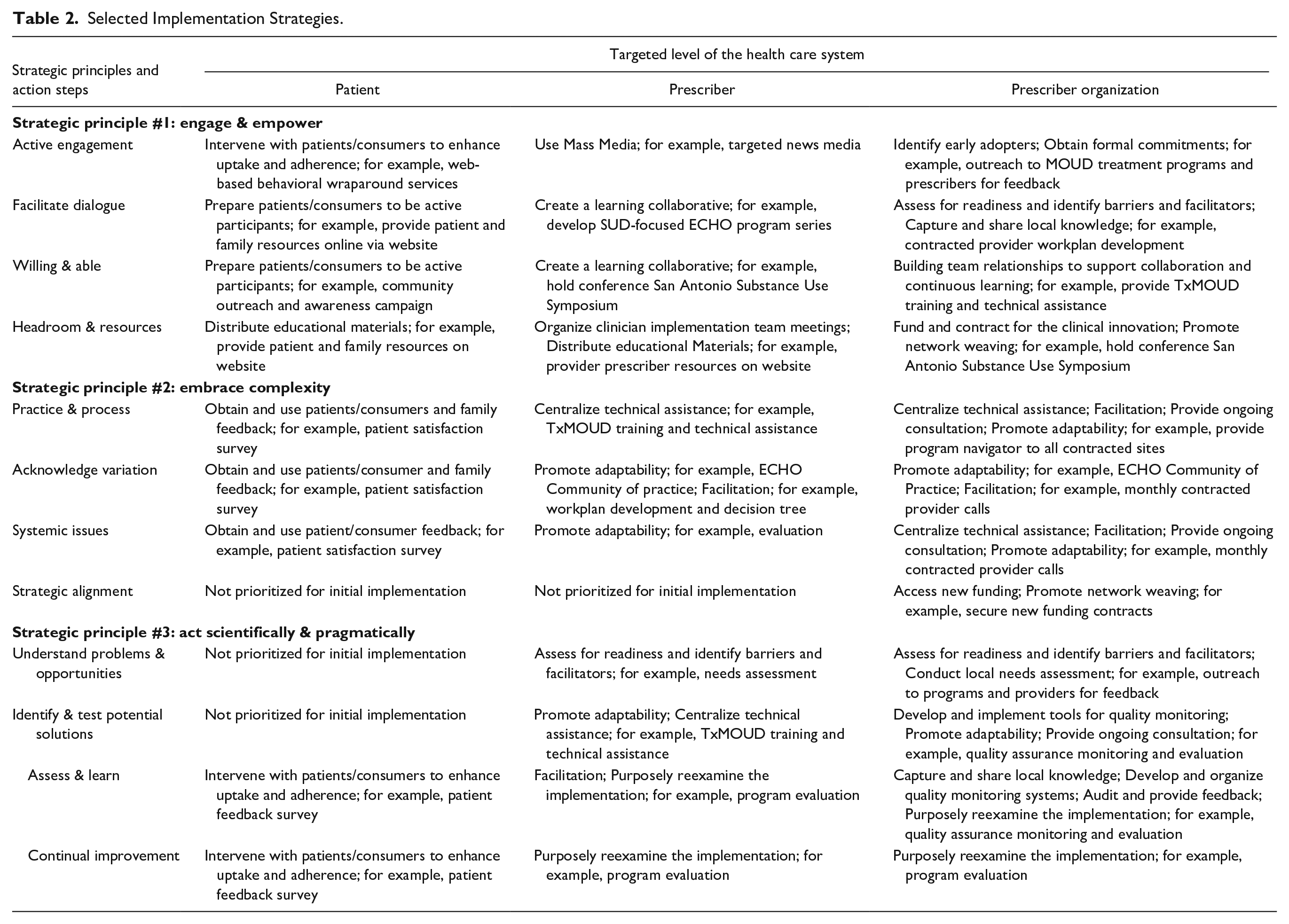
The team then engaged in a comprehensive mapping process to begin considering appropriate implementation strategies to address each barrier. Utilizing the Expert Recommendations for Implementing Change (ERIC) taxonomy 26 as a foundational guide and aligned with common steps for matching strategies with barriers, 27 this collaborative effort involved integrating empirical data on effective strategies, expert consensus on local context and resources, and insights derived from prior experience with affiliated programs. Mapping of implementation strategies to barriers was facilitated through and documented within our SHIFT-Evidence planning template, which also prompted continued focus on the simple rules of balancing evidence and pragmatism, embracing complexity, and engaging and empowering. During this phase, several key strategies emerged as priorities, including active engagement and empowerment of patients/consumers through interventions and educational materials, the creation of learning collaboratives, and the identification of early adopters to champion the implementation efforts. Subsequently, the team focused on customizing each strategy to meet Texas’s unique needs, operationalizing them synergistically with local conditions and resources. For example, recognizing Texas’s vast rural areas and the limited access to specialized SUD treatment resources in these regions, the team leveraged the Extension for Community Healthcare Outcomes (ECHO) model to disseminate educational tele-mentoring sessions focused on SUD treatment throughout the state. ECHO sessions were designed to support local health care providers in implementing evidence-based practices for managing OUD. This customization ensured that even providers in remote areas could access expert guidance and training aligned with national- and state-level standards. The result of this process was a comprehensive, multifaceted, state-level plan to increase the availability of MOUD, ultimately incorporating several large-scale initiatives, including a SUD-specific ECHO program, the GetWaivoredTX training program, 24 Recovery Texas (online treatment hub), and an innovative contingency management application. Table 2 provides a selective overview of the strategies within the planning template, illustrating examples of operationalization.
Selected Implementation Strategies.
Program Infrastructure
Following the completion of the SHIFT-Evidence planning template, a comprehensive program infrastructure was established to enact the implementation plan, leveraging the academic medical setting’s dynamic environment and faculty expertise. Program services were directly supported by a diverse team of program directors, managers, and coordinators, many with prior personal and professional experience in SUD, along with specialists in financial and contracting services, quality assurance and process improvement, communications, education, data and evaluation, and information technology. Program services launched in Spring 2020.
Evaluation Findings and Key Insights
TxMOUD’s delivery of services was facilitated through subcontracts with OBOT provider organizations. These services encompass 2 core components: (1) MOUD, including prescription and/or administration of medications like buprenorphine or extended-release injectable naltrexone; and (2) counseling and behavioral therapies. Selection criteria for OBOT provider organizations prioritized readiness to enroll patients, provider capacity, location in high-priority or rural areas, and serving specific populations, including pregnant individuals and those at risk of opioid overdose. Contracting requirements included having a prescriber with a current X-waiver, capacity or referral capability for behavioral counseling, training on the state’s CMBHS system, and the ability to participate in treatment network activities such as the SUD-focused ECHO program. Each funding application underwent an assessment of the selection criteria outlined above using a standardized rubric. The scoring tool provided definitions for each criterion and the associated priority scoring level (0: Low Priority; 1: Medium Priority; and 2: High Priority). Scores were totaled across all criteria to determine the priority level for funding, ensuring a fair and consistent evaluation of all applicants. In the spring of 2020, TxMOUD received a total of 19 formal inquiries from organizations interested in participating. Approximately 8 months after contracting with Texas HHSC in August 2019, the first prescriber organization (hereafter OBOT provider) was contracted in May 2020. By the end of the fiscal year (FY), an additional 3 OBOT providers were contracted and began providing services across 6 treatment sites strategically located in and around major metropolitan areas, serving 58 clients between June 2020 and September 2020. The network’s reach expanded significantly in subsequent years, growing to 16 OBOT providers and 26 treatment sites in FY 2021, serving 544 clients, and further expanding to 25 OBOT providers across 38 sites by FY 2022, serving 1329 clients. By FY 2023, the network included 32 OBOT providers managing 44 treatment sites, serving 1635 clients (see Figure 1).
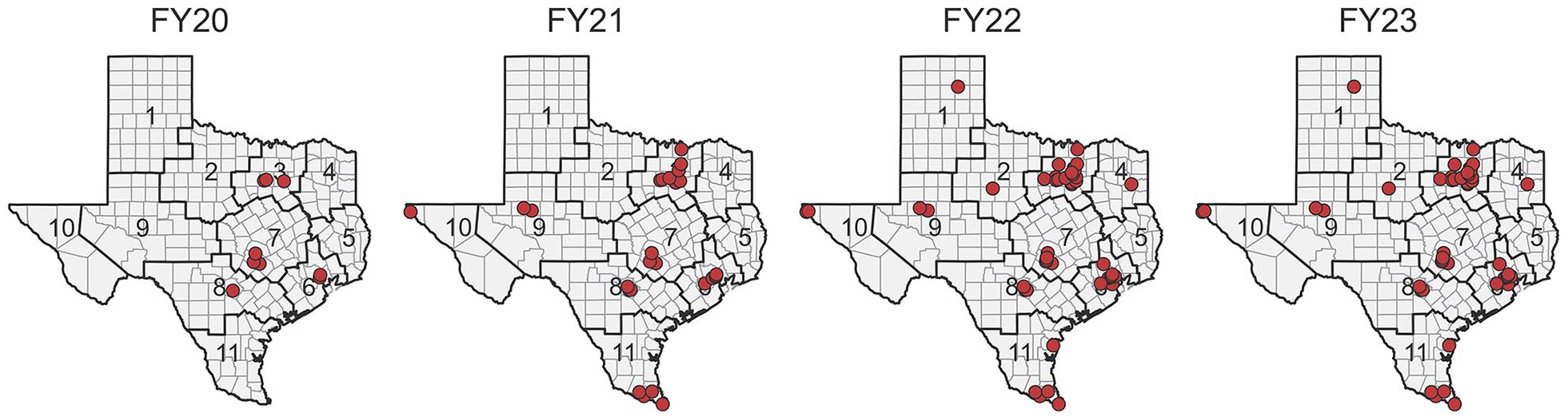
OBOT provider network expansion by public health region (FY20-23).
This expansion also facilitated the program’s reach across Texas, starting in FY 2020 with an OBOT provider presence in 4 Texas Public Health Regions (PHR), state-designated regions created for public health service delivery by Texas HHSC, then extending to 7 PHRs by FY 2021 and achieving physical locations in 10 of the 11 total PHR regions by FY 2022. The program reach was maintained in FY 2023 with providers serving metropolitan, urban, and rural communities across the state.
The success of this program in expanding access to MOUD was grounded in the structured planning process guided by SHIFT-Evidence. The framework facilitated the identification and analysis of barriers across multiple health care system levels, allowing for a detailed understanding of challenges to MOUD implementation. The planning template developed through SHIFT-Evidence was essential in organizing this complex information and ensuring the alignment of strategies with system needs. By systematically prioritizing these barriers and mapping tailored strategies, the team was able to efficiently operationalize multilevel interventions, adapting them to the unique characteristics of Texas’s health care landscape. The iterative refinement of strategies through continuous consultation and feedback enabled the program to maximize resource use, resulting in the effective expansion of MOUD services across the state.
Conclusion
This study demonstrates the successful application of the SHIFT-Evidence framework to develop and implement a statewide network of OBOT providers, expanding access to MOUD for underserved populations across Texas. By identifying systemic gaps and barriers at multiple levels of the health care system, this approach supported the methodical selection of implementation strategies aligned with SHIFT-Evidence’s principles, resulting in a multifaceted and synergistic implementation plan.
Our application of SHIFT-Evidence illustrates the utility of the framework in planning and implementing complex, large-scale public health initiatives by supporting coordinated efforts that systematically drive the consideration of factors across the health care system, even amid a shifting health care landscape. As a result, we were able to orchestrate a coordinated approach to MOUD expansion that provided opportunities to “engage and empower” our implementation partners, connecting with prescribers and prescriber organizations and supporting their connections with patients. Further, our integration of ERIC strategies into our process allowed us to employ a standardized language for describing and categorizing proven implementation strategies and tailor our approach to the local context. This principle is central to SHIFT-Evidence and critical to the success of systemic improvements.28,29
Moreover, this work highlights the value of implementation frameworks such as SHIFT-Evidence in understanding and adapting to the local context and dynamics within the health care system, which proved instrumental in identifying and addressing specific challenges to evidence-based care delivery.30-32 The use of the planning template also enabled the team to identify barriers occurring at or interrelated across multiple levels (eg, stigma around substance use) and to strategically select strategies that could be deployed across multiple levels of the health care system, maximizing impact and condensing efforts. These kinds of practical public health planning tools may be particularly significant in the realm of SUD treatment, where barriers to access and implementation are prevalent and multifaceted. 33 The use of SHIFT-Evidence also provides flexibility to iterate and adapt implementation strategies over time to respond to the changing landscape of SUD treatment. For example, after the X-waiver requirement was discontinued with the passage of the Consolidated Appropriations Act of 2023, and new requirements for SUD education were instituted for new or renewing DEA licenses through the Medication Access and Training Expansion (MATE) Act, efforts were shifted from X-waiver training to assisting prescribers understand the new DEA requirements, maintaining alignment with the principle of engaging and empowering. By demonstrating SHIFT-Evidence’s utility in this area, our study adds to the growing body of literature advocating for the use of implementation frameworks to facilitate the widespread adoption of effective treatments. 34
Despite the many strengths of the SHIFT-Evidence framework, few operational guidelines were available to guide its practical application. To bridge this gap, we developed a planning template that provided structure to support the team in systematically identifying barriers and implementation opportunities across multiple health care system levels. This template facilitated discussion, prioritization, and selection of strategies, allowing the team to develop a synergistic set of initiatives tailored to the Texas health care landscape.
Our primary goal was to develop and implement a set of implementation initiatives that could effectively enhance access to evidence-based care for OUD within underserved communities across Texas. SHIFT-Evidence emerged as a pivotal tool in this work, enabling us to discern critical gaps in the health care landscape and to develop an integrated, multilevel program, ultimately creating a unique Hub and Spoke model tailored for Texas. Our experience underscores the value of a comprehensive planning framework like SHIFT-Evidence in addressing complex health care challenges.
Footnotes
Authors’ Contributions
CDB: Conceptualization, writing—original draft, methodology, and visualization; EF: Conceptualization, writing—review and editing, and methodology; TK-W: Writing—review and editing; JSP: Conceptualization, methodology, writing—review and editing, and funding acquisition. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by Texas Targeted Opioid Response, a public health initiative operated by the Texas Health and Human Services Commission (Texas HHSC) through federal funding from the Substance Abuse and Mental Health Services Administration (SAMHSA) grant award number (HHS001046900001, HHS000562000001, and HHS000878900001), and funding from the National Institute on Drug Abuse (NIDA) DA054881, DA020024, and DA057659. The views expressed do not necessarily reflect the official policies of NIDA, SAMHSA, or the Texas HHSC, nor does the mention of trade names, commercial practices, or organizations imply endorsement by NIDA, SAMHSA, or the Texas HHSC.
Compliance,Ethical Standards,and Ethics Approval
Institutional Review Board approval was not required.
Anonymized Material
UT Health San Antonio, Texas Health and Human Services (Texas HHSC), GetWaivoredTX, Texas Targeted Opioid Response, Texas Medications for Opioid Use Disorder (TxMOUD). 25