
Abstract
Background:
For structurally marginalized populations, including people who use drugs (PWUD), equitable access to healthcare can be achieved through healthcare access supports. However, few studies characterized utilization of formal (eg, outreach workers, healthcare professionals) and informal (eg, friends/family) supports. Therefore, we sought to estimate the prevalence of and factors associated with receiving each type of support among PWUD.
Methods:
We used data from 2 prospective cohort studies of PWUD in Vancouver, Canada, in 2017 to 2020. We constructed separate multivariable generalized linear mixed-effects models to identify factors associated with receiving each of the 3 types of supports (ie, healthcare professionals, outreach workers/peer navigators, and informal supports) compared to no supports.
Results:
Of 996 participants, 350 (35.1%) reported receiving supports in the past 6 months at baseline, through informal supports (6.2%), outreach workers (14.1%), and healthcare professionals (20.9%). In multivariable analyses, HIV positivity, chronic pain, and avoiding healthcare due to the past mistreatment were positively associated with receiving supports from each of healthcare professionals and outreach workers. Men were less likely to receive any types of the supports (all P < .05).
Conclusions:
Utilization of healthcare access supports was relatively low in this sample. However, formal supports appeared to have reached PWUD exhibiting more comorbidities and experiencing discrimination in healthcare. Further efforts to make formal supports more available would benefit PWUD with unmet healthcare needs, particularly men.
Keywords
Highlights
Healthcare access supports are important to ensure equitable access to healthcare for structurally-marginalized people who use drugs (PWUD), but little is known about how commonly PWUD use such supports and the types of supports they use.
In our sample of 996 PWUD in Vancouver, Canada, we found that 35% received healthcare access supports at baseline in 2017-2020, mostly commonly through healthcare professionals (21%) followed by outreach workers/peer navigators (14%) and informal supports (e.g., friends, family) (6%).
While formal supports (i.e., healthcare professionals and outreach workers/peer navigators) appeared to have reached PWUD exhibiting more comorbidities and experiencing discrimination in healthcare, 23% of those who did not receive any supports reported unmet healthcare needs, and men were less likely to use any supports.
Further efforts to make formal supports more available would benefit PWUD with unmet healthcare needs, particularly men.
Introduction
People who use drugs (PWUD), especially through intravenous use, have a high burden of disease including infectious diseases such as HIV and hepatitis C virus (HCV) as well as psychiatric conditions and chronic pain.1-4 The high level of medical and psychiatric complexity among PWUD contribute to an overall high healthcare need as well as an increased difficulty accessing healthcare services. 5 Many PWUD seeking care face stigma and discrimination, difficulties accessing transport, and cost barriers in areas without universal healthcare.6-10 These factors likely contribute to delays in seeking care 11 and an increase in emergency room visits in lieu of accessing primary care services. 12 It is no surprise that there is high prevalence of unmet healthcare need among PWUD. A prior study from Vancouver, Canada, found that 25% of 889 community-recruited PWUD reported an unmet healthcare need in 2017 to 2018. 13 Another cross-sectional study from Edmonton, Canada, reported a higher prevalence of unmet need for substance use and mental health-related care (82%) among 320 street-involved PWUD who were not accessing any specialty mental health or addiction treatment in 2014. 14
Improving access to care to meet the care needs of structurally marginalized groups is a topic of concern in addiction research.3,4,12-14 Multiple models of care have been proposed, including integrated health services that include allied health professionals, such as social workers.3,4 What many of these models do not address is the need for supports to help access their services. Due to significant comorbidity and the effects of substances, many PWUD would benefit from support accessing services, keeping appointments, and completing investigations. 4 Support can come in many forms: for some it may be the help of family and friends, for others it may come in a formal form of help from peer navigators and outreach workers, and still others may go directly to their healthcare professionals for this kind of assistance. By definition, peer navigators have lived experience and training consistent with the population they are serving. 15 They generally provide social support, role modeling, and outreach services.15,16 Outreach workers are trained individuals who also provide social support and outreach services but do not necessarily have lived experience with the population they serve. Outreach workers and peer navigators have been key to health services reaching priority populations; however, this has mostly been studied in specific disease and situation-targeted cases such as motherhood, 4 psychiatric illness, 17 incarceration,18,19 homelessness, 16 addiction treatment,20,21 and chronic illnesses such as HIV.22-25 This disease-specific research approach is mirrored in the services available. For example, the Assertive Community Treatment (ACT) program 26 and the Seek and Treat for Optimal Prevention of HIV/AIDS (STOP HIV/AIDS) 27 teams in Vancouver are both outreach services for people with psychiatric conditions and HIV, respectively. Furthermore, few studies have examined the prevalence and characteristics of PWUD who use supports from outreach workers and peer navigators in real-world settings.
In 2017, the Vancouver Coastal Health Authority sought to develop an evidence-based, community-directed model of interdisciplinary primary care for the residents of the Downtown Eastside (DTES) of Vancouver, BC. 28 The DTES neighborhood is characterized by high rates of marginalization, substance use, and infectious disease. 29 This model of care, called the Downtown Eastside Second Generation Strategy (DTES-2GS), included establishing 3 primary care clinics with integrated care teams in January 2018, improving access to outreach supports, improving cultural competency, and trauma informed training for staff and a substantial increase in peer roles.28,30 In light of the implementation of the DTES-2GS, with its focus on peer support work and outreach workers, we sought to determine the prevalence of, and factors associated with the use of different supports accessing healthcare among PWUD in Vancouver. We included formal supports such as peer navigators and outreach workers, informal supports such as the help of friends and family as well as the support of healthcare professionals such as nurses, doctors, and social workers in our evaluation.
Methods
Data Sources and Study Sample
We used data from the DTES-2GS evaluation study. This study sought to collect information on PWUD’s experiences with healthcare access and nonclinical quality of care, measuring experiences such as perceived discrimination, access, and cultural safety. 31 The 2GS evaluation study was nested within 2 ongoing prospective cohort studies of community-recruited PWUD in Vancouver, Canada: The Vancouver Injection Drug Users Study (VIDUS) and the AIDS Care Cohort to evaluate Exposure to Survival Services (ACCESS). The VIDUS and ACCESS studies have been previously described in detail. 32 In short, VIDUS enrols adult (aged 18 years or older) PWUD who are HIV-seronegative and injected drugs in the month prior to enrolment. ACCESS enrols adult PWUD who are HIV-seropositive. Both cohorts recruit participants through word-of-mouth and street outreach from a frontline office in the DTES. The cohorts are harmonized and administer the same questionnaires by trained interviewers every 6 months, and nurses draw blood for HIV and HCV serology during the visit. Recruitment for the 2GS evaluation study was described in detail elsewhere. 13 In brief, VIDUS and ACCESS participants who completed an in-person study follow-up visit between December 2017 and November 2018 were invited to participate in the 2GS evaluation study as a supplement to the parent cohorts through a convenience sampling approach until 1000 participants were enrolled in the 2GS evaluation study. The 2GS study participants were asked to complete both the parent cohorts and 2GS questionnaires at their biannual study follow-up visits until March 2020. Participants were given $15 CAD honoraria for completing each of the 2GS evaluation study questionnaires and $40 CAD for completing each of the parent cohort study questionnaires. Our frontline research staff have employed intensive community-based methods to maintain high follow-up rates, including obtaining contact information for 2 persons who know the participant and conducting regular outreach to areas frequented by our participants. They have also established/seek to establish rapport with our participants, which has helped minimize some reporting bias such as social desirability bias. Ethics approval for the VIDUS, ACCESS, and the 2GS evaluation study was granted by the Providence Health Care/University of British Columbia Research Ethics Board and Simon Fraser University Research Ethics Board.
For the present analyses, we restricted our sample to the VIDUS or ACCESS participants who completed at least one 2GS evaluation study questionnaire and the matched parent cohort study questionnaire between December 2017 and March 2020 and reported having had a health issue that required medical attention in the past 6 months. Figure 1 delineates how the analytic sample was derived.
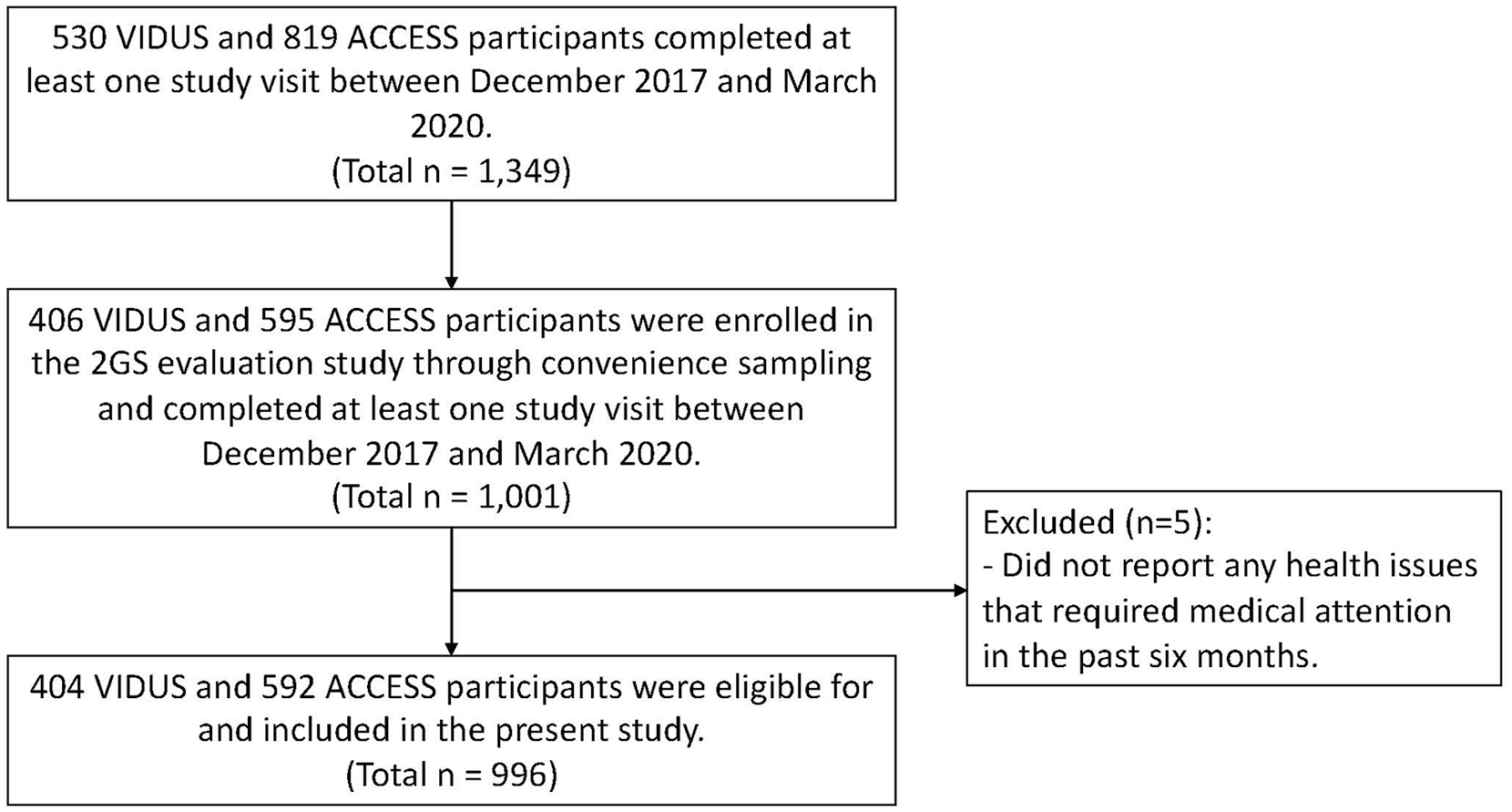
Determination of the analytic sample.
Study Measures
Our primary outcome measure was utilizing healthcare access support in the past 6 months and derived by asking participants if anyone helped them access the care they needed for their health issues. The “help” was further described as: help making referrals to healthcare providers, help making appointments, and accompaniment to the hospital or clinic. Participants who responded “yes” to the question were further asked who provided them with healthcare access supports, with categories described as follows: family member or friend, peer navigator, outreach worker, healthcare professional, and other (description box provided). We renamed and combined the categories to better reflect where the funding for these supports were coming from. “Informal supports” were defined as help from informal supporters and professionals (excluding healthcare professionals), mostly including friends and family but also a small number (n = 6) of reports of police officers, parole officers, etc. This category reflects help received from those who are not specifically paid to render this service.
As both peer navigators (ie, individuals with lived experience) and outreach workers (ie, people trained to help marginalized populations) help their clients/peers access healthcare and are paid positions, and outreach workers can be with lived experience, we combined them into a category called “outreach worker.” Indeed, the distinction between the 2 roles was not highlighted during our surveys. Accordingly, among 361 reports of outreach workers (the combined category), there were only 12 reports of peer navigators. This indicated that some peer navigators might have been reported as outreach workers because peer navigators often conduct outreach. Also, these descriptors were not associated with any specific treatment programs, or we did not ask our participants which programs the outreach workers and/or peer navigators were affiliated with because our study aim was to characterize the utilization of healthcare access supports more generally and not to evaluate every single program of care separately.
Healthcare professionals remained unchanged and reflected those who are highly trained and may often find themselves offering this kind of support when working with systematically marginalized populations but whose job description may not formally include these services. While we did not provide a specific definition of healthcare professionals to our study participants, they usually referred to medical professionals (eg, doctors, nurses) who work in a clinic or hospital. Some participants also provided their answers in open-text format under the “other” category, which were recategorized by the authors (GR, KH, SK and BN) into either one of the new categories or no help received.
We selected explanatory variables thought to affect availability and utilization of healthcare access supports by considering Anderson’s behavioral model of health service use, 33 clinical experience by the authors (GR and SK), and previous work on this dataset. 13 Predisposing factors included: age (continuous per year older), self-identified gender (men vs women, transgender, nonbinary, and other), ethnicity/ancestry (white vs Indigenous or people of color), educational attainment (less than high school diploma vs completed high school diploma or more), current relationship status (legally married, regular partner living together, or regular partner not living together vs all other responses), homelessness, DTES residency, and employment. An enabling factor was attachment to primary care, defined as having a family physician or clinic that they feel comfortable going to as used in a previous study. 13 Need-based variables included: drug use patterns (ie, ≥daily nonprescribed use of opioids, ≥daily use of stimulants [ie, cocaine, crack cocaine, or crystal methamphetamine], ≥daily alcohol use, having experienced nonfatal overdose and enrolment in a drug or alcohol treatment program), having experienced physical violence, avoidance of healthcare due to the past poor treatment, 34 self-reporting unmet healthcare need, 13 incarceration, and chronic health conditions (ie, anxiety symptoms derived from the Patient-Reported Outcome Measurement Information System [PROMIS] short-form anxiety score [moderate to severe vs mild to none], 35 chronic pain, defined as reporting pain that has persisted for greater than 3 months, 36 HIV status [positive vs negative], and self-reported HCV status [positive vs negative or unknown]). Because the analytic sample consisted of people who used substances, we considered the following variables as potential comorbidities beyond substance use: anxiety symptoms, chronic pain, and HIV/HCV seropositivity. All behavioral variables referred to the past 6 months and were dichotomized as yes versus no unless otherwise stated.
Statistical Analysis
Baseline characteristics of participants stratified by receiving any help accessing healthcare versus no help received were examined using the Pearson’s Chi-square test for categorical variables and the Wilcoxon rank sum test for continuous variables.
Univariable and multivariable generalized linear mixed-effects models under a binomial family with logit link were used to identify factors associated with utilizing healthcare access supports, using all eligible observations, which included multiple observations per person. Any missing observations were treated as missing. We fit 4 models, including 1 comparing utilizing any healthcare access supports versus no supports, and the other 3 comparing each of the 3 types of supports versus no supports. We first fit univariable models for each explanatory variable and each of the 4 outcome variables, respectively. We did not make any corrections to alpha in the univariable analyses because our modeling approach was exploratory. Then, in all 4 models, explanatory variables were included in the multivariable analysis if they were associated with the outcome at the P < .10 level in the univariable analysis. We employed this modeling approach to avoid overloading independent variables. However, as sensitivity analyses, we also fit 4 multivariable models that included all 22 explanatory variables regardless of their associations with the outcomes in univariable analyses. All P values were 2-sided. Analysis was conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). We filled out the STrengthening the Teporting of OBservational studies in Epidemiology (STROBE) check list in the Supplemental Materials.
Results
Of the 1001 VIDUS/ACCESS participants who completed at least one 2GS evaluation study questionnaire between December 2017 and March 2020, 996 (99.5%) reported having had a health issue that they felt required medical attention in the past 6 months and were eligible to participate in the present analysis. The median number of interviews completed per person during the study period was 3 (first, third quartiles: 2, 4). Table 1 presents the baseline characteristics of the sample. As shown, 8 variables had ≤2.5% of missing observations while the anxiety variable had 8.5%. At baseline, 595 (59.9%) participants self-identified as men and the median age was 50 (first, third quartiles: 41, 57) years. In total, 350 (35.1%) reported receiving healthcare access supports in the past 6 months, including 62 (6.2%) accessing informal supports, 140 (14.1%) accessing outreach workers, and 208 (20.9%) accessing healthcare professionals. The prevalence of reporting unmet healthcare needs at baseline was not significantly different between those who did and did not receive any supports (27.1% vs 23.2%, P = .170). The prevalence among those who accessed informal supports was 25.8%, while it was 26.4% among those accessing outreach workers and 27.4% among those accessing healthcare professionals.
Baseline Sample Characteristics Stratified by Utilizing Healthcare Access Supports Among People Who Use Drugs in Vancouver, British Columbia, Canada, Between December 2017 and March 2020 (n = 996).
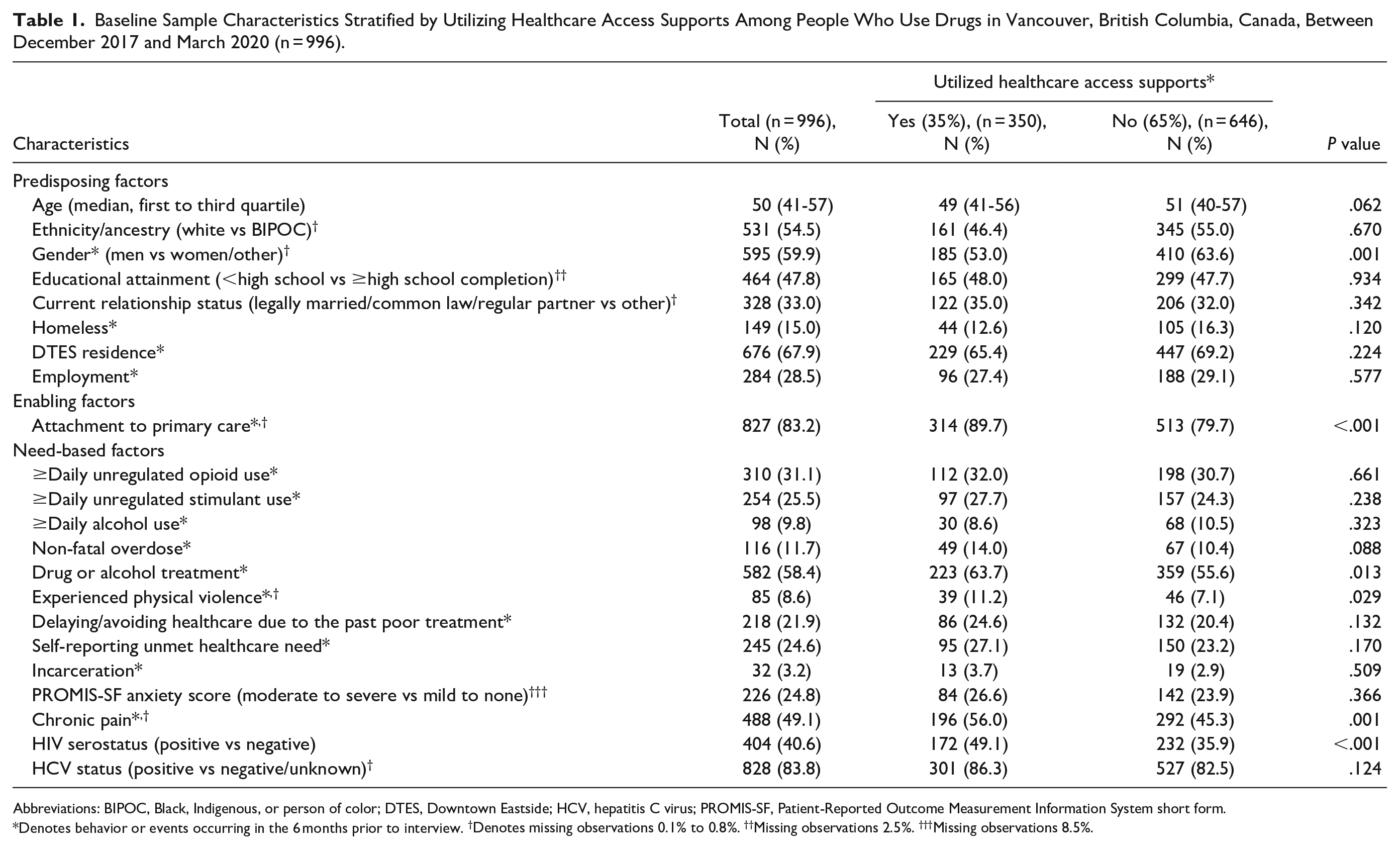
Abbreviations: BIPOC, Black, Indigenous, or person of color; DTES, Downtown Eastside; HCV, hepatitis C virus; PROMIS-SF, Patient-Reported Outcome Measurement Information System short form.
Denotes behavior or events occurring in the 6 months prior to interview. †Denotes missing observations 0.1% to 0.8%. ††Missing observations 2.5%. †††Missing observations 8.5%.
In multivariable analyses (Table 2 and Figure 2), attachment to primary care (adjusted odds ratio [AOR] = 2.35, 95% confidence interval [CI] 1.70-3.25), avoiding seeing healthcare due to poor treatment (AOR = 1.44, 95% CI 1.11-1.86), chronic pain (AOR = 1.42, 95% CI 1.18-1.73), and living with HIV (AOR = 1.82, 95% CI 1.48-2.24) were all independently and positively associated with utilizing any supports. Conversely, older age (per year older) was negatively associated with utilizing any supports (AOR = 0.97, 95% CI 0.96-0.99). Men were also negatively associated with utilizing any supports (AOR = 0.58, 95% CI 0.47-0.72).
Univariable and Multivariable Generalized Linear Mixed-Effects Model Identifying Factors Associated With Utilizing Each of the 3 Types of Healthcare Access Supports Among People Who Use Drugs in Vancouver, Canada, from December 2017 to March 2020 (n = 2976).
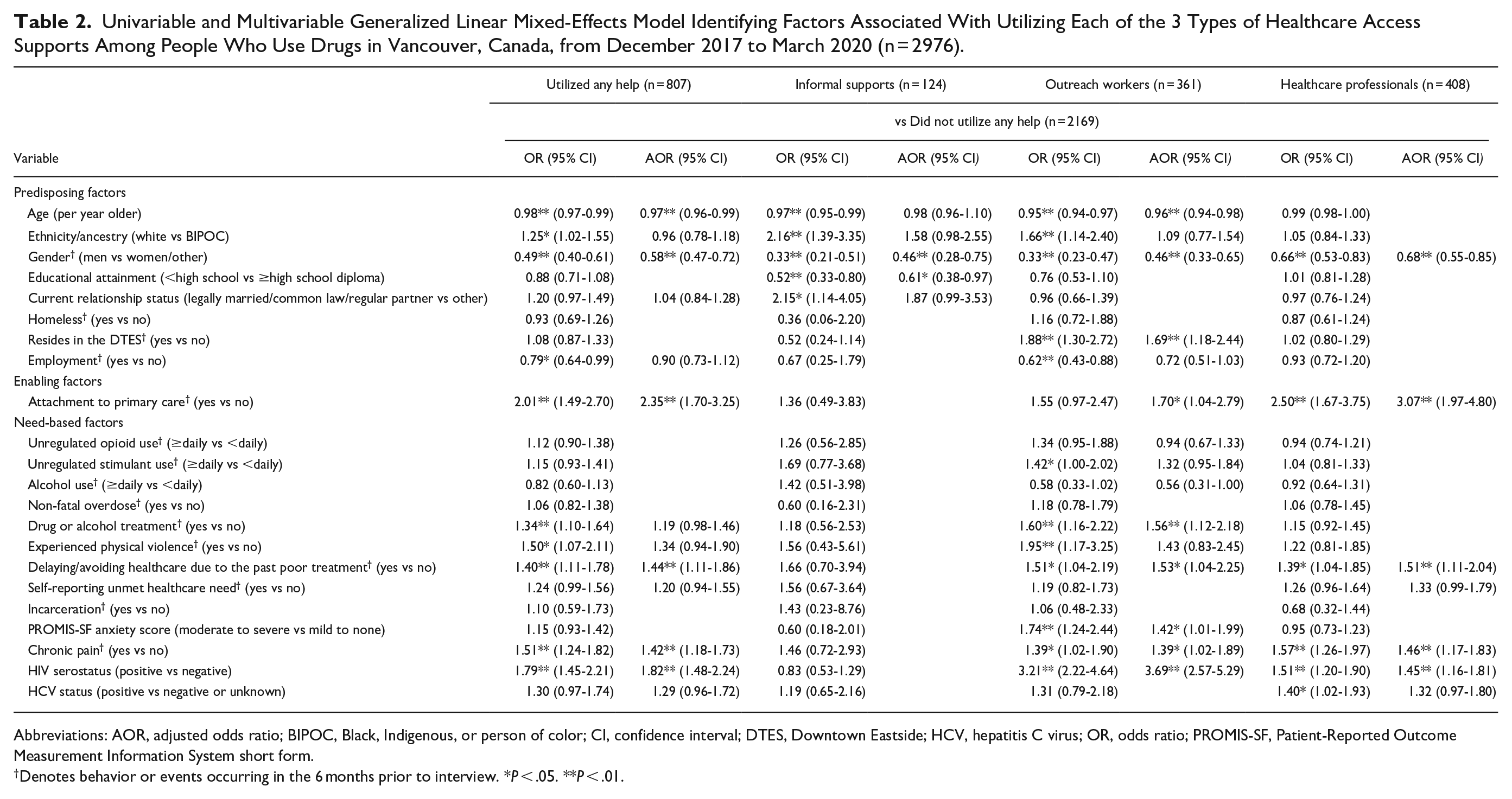
Abbreviations: AOR, adjusted odds ratio; BIPOC, Black, Indigenous, or person of color; CI, confidence interval; DTES, Downtown Eastside; HCV, hepatitis C virus; OR, odds ratio; PROMIS-SF, Patient-Reported Outcome Measurement Information System short form.
Denotes behavior or events occurring in the 6 months prior to interview.*P < .05. **P < .01.
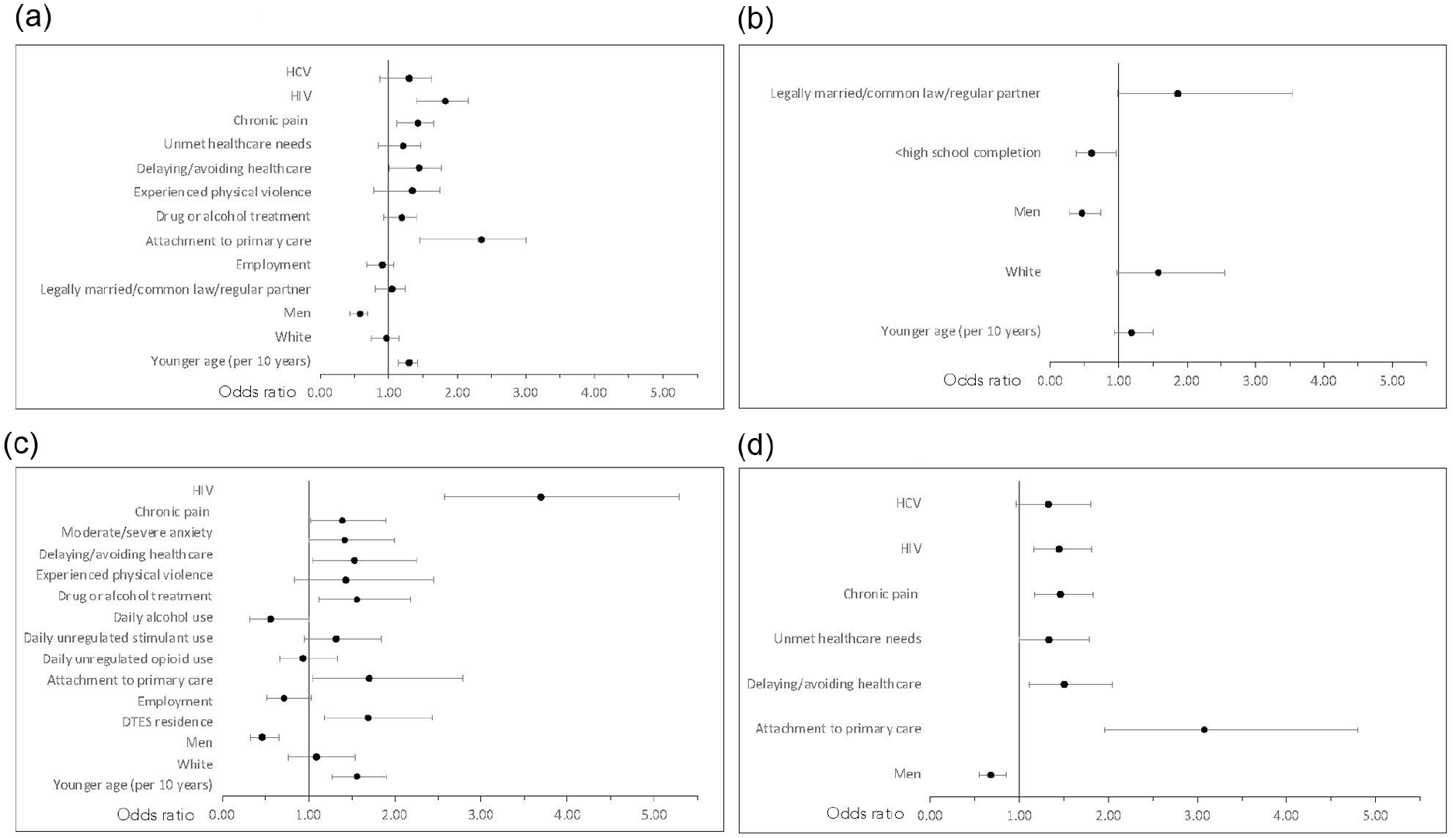
Forest plots of the multivariable analyses results. (A) Utilized any help. (B) Informal supports. (C) Outreach workers. (D) Healthcare professionals.
As for the support type-specific independent associations, as shown in Table 2, attachment to primary care, avoiding seeking healthcare due to the past poor treatment, chronic pain, and living with HIV were all positively associated with utilizing outreach workers and healthcare professionals, respectively, but not with informal supports. Living in the DTES, drug or alcohol treatment and moderate/severe anxiety symptomology, and younger age were significantly associated with utilizing outreach worker supports only, while having an education level of less than high school diploma was negatively associated with accessing informal supports only. The results of the sensitivity analyses are shown in Supplemental Table 1. As shown, the factors that remained significantly associated with utilizing any supports were identical with those found the primary analyses. The support type-specific independent associations were also almost identical with a few exceptions.
Discussion
Among a cohort of 996 PWUD, 35% endorsed utilizing healthcare access supports in the past 6 months at baseline. Those who received supports were more likely to report attachment to primary care, avoidance in seeking healthcare due to the past mistreatment, chronic pain, and living with HIV. Those who sought and received support from healthcare professionals had similar characteristics as those who utilized healthcare access supports in general. In addition to the aforementioned factors, those accessing outreach workers were more likely to live in the DTES, be enrolled in drug or alcohol treatment, and have moderate to severe symptoms of anxiety. Those who received help from informal supports were more likely to have completed high school and men were less likely to receive any forms of support.
We are not aware of any previous work characterizing the use of different types of healthcare access supports among PWUD in real-world settings. We found that those who received healthcare access supports were generally characterized by increased comorbidities—including chronic pain and HIV seropositivity—compared to those who did not. This difference may be partially explained by the disease-specific targeted supports available in our study setting, such as the STOP HIV/AIDS team for those living with HIV 27 and the ACT team for active psychiatric disorders. 26 Despite the high comorbidities and the finding that they were more likely to report avoiding seeking healthcare due to the past poor treatment, this group of PWUD were not necessarily more likely to report unmet healthcare needs, which is encouraging as it may imply that the healthcare access supports may be filling the important gap. However, disease-specific supports unlikely address the full range of comorbidities experienced by those who accessed supports. For example, those with chronic pain do not have access to disease-specific supports in our study setting. In fact, we also found that suffering from chronic pain and avoiding healthcare were both associated with accessing formal supports. Chronic pain is estimated to affect 1 in 4 adult Canadians and cost the economy an estimated $40.4 billion in 2019 alone. 37 Misunderstanding of pain in relation to addiction is prevalent 38 and physicians are often reluctant to prescribe opioid analgesics to PWUD for fear of diversion, 39 often denying it altogether.40,41 Even among providers experienced in treating comorbid chronic pain and substance use, their clinical practices vary widely. 42 In our previous study, chronic pain was associated with unmet healthcare needs. 13 More work needs to be done to address chronic pain and other comorbidities commonly experienced by PWUD.
The relatively low utilization of formal supports (ie, healthcare professionals or outreach workers) observed across our study sample (35%) despite the high levels of comorbidities and structural marginalization may be partially explained by the inadequate availability of formal supports in our study setting. In a study of homeless youth in Alberta, Canada, 80% utilized targeted peer and professional supports. 43 While our results cannot directly be compared to this pilot intervention, given that 68% of our study sample resided in the DTES at baseline where the DTES-2GS established integrated care clinics that involved outreach workers and put an emphasis on better coordinated care, 28 one may expect higher coverage of formal supports. In particular, our findings that men were less likely to utilize any supports accessing healthcare indicate that more targeted outreach efforts are needed for men who use drugs. Furthermore, the finding that 23% of those who did not receive any support reported unmet healthcare needs at baseline indicates that more could be done for this subpopulation as well, and some may benefit from increased access to formal health accesses supports such as outreach workers. Increasing the coverage of formal supports is also important given that informal supports would impose a substantial burden on families and peers.
Our results also indicated that PWUD receiving supports from outreach workers and peer navigators may have had the highest burden of disease (eg, moderate to high anxiety symptomology, HIV, and chronic pain) and were also more likely to avoid accessing care due to poor treatment in the past. Yet, there was no significant association between unmet healthcare needs and receiving supports from outreach workers. These findings suggests that outreach workers might have played an important role in alleviating some of the unmet healthcare needs for this high priority subpopulation of PWUD. A large body of literature demonstrates the multitudes of health and social benefits outreach workers and peer navigators can offer in disease and situation-specific situations as well as in randomized control trials.4,10,16-25,44 Our study advances the knowledge in this field by characterizing the utilization of outreach workers’ services among a large sample of PWUD in a real-world setting where structural changes in the primary care system have been implemented (ie, DTES-2GS). More research needs to be done to quantify the benefit outreach workers and peers provide to PWUD clients to identify gaps in coverage and advocate for increased support for these vital services. Also, as peer workers tend to be exploited, particularly but not limited to in community-based harm reduction service sites, 45 there is a need to ensure that peer navigators be adequately compensated and supported for the important work they provide.
There are some limitations to this study. First, the study sample was not randomly recruited, and therefore might not necessarily be generalizable to all PWUD in Vancouver. Second, many of the variables were self-reported, which may contribute to reporting bias. Third, because our study aim was to characterize the overall utilization of different types of healthcare supports in our study setting, we did not ask our participants which specific programs the help (eg, outreach workers) was associated with. This limits our ability to evaluate the effects of each specific program such as ACT teams. Last, as the majority of the explanatory variables used the same time frame (ie, in the past 6 months) with the outcome variables, we are unable to establish the temporal sequence between the explanatory and outcome variables.
Conclusion
In sum, we found that 35% of our sample of PWUD in Vancouver received some forms of support when they accessed healthcare at baseline between December 2017 and March 2020. The relatively low utilization of formal supports (ie, healthcare professionals or outreach workers) despite the high levels of comorbidities and structural marginalization indicated the need to enhance the availability of formal supports. While we identified heterogenous characteristics of PWUD across different types of healthcare support utilized, receiving formal supports was associated with higher comorbidities, including HIV and chronic pain. Further efforts to make formal supports more available would benefit PWUD with unmet healthcare need, particularly men.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241249870 – Supplemental material for Characterizing the Use of Healthcare Access Supports Among People Who Use Drugs in Vancouver, Canada, 2017 to 2020: A Cohort Study
Supplemental material, sj-docx-1-saj-10.1177_29767342241249870 for Characterizing the Use of Healthcare Access Supports Among People Who Use Drugs in Vancouver, Canada, 2017 to 2020: A Cohort Study by Kanna Hayashi, Gabrielle Rabu, Zishan Cui, Sukhpreet Klaire, Fahmida Homayra, Michael-John Milloy and Bohdan Nosyk in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The VIDUS and ACCESS studies take place on the unceded territory of the Coast Salish Peoples, including the territories of the xwməθkwəy̓əm (Musqueam), Skwxwú7mesh (Squamish), Stó:lō and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations. The authors would like to thank the study participants as well as current and past researchers and staff; their time and efforts have been an invaluable contribution to this research.
Author Contributions
GR and KH conceptualized the study. KH, BN and MJM obtained funding. ZC conducted the statistical analyses. GR and KH drafted the initial manuscript. All authors participated in interpreting the results, contributed to the writing of the manuscript, provided critical feedback to the manuscript, and approved the final manuscript draft for submission.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MJM is the Canopy Growth professor of cannabis science at the University of British Columbia, a position established through arms’ length gifts to the university from Canopy Growth Corporation, a licensed producer of cannabis in Canada, and the Government of British Columbia’s Ministry of Mental Health and Addictions. He has no personal financial relationships to the cannabis industry. The other authors report no potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Canadian Institutes of Health Research (CIHR; PJT-15924) and National Institutes of Health (NIH; U01DA038886, U01DA021525). KH holds the St. Paul’s Hospital Chair in Substance Use Research and is supported in part by the NIH (U01DA038886), a Michael Smith Health Research BC Scholar Award, and the St. Paul’s Foundation. GR is supported by the NIH-funded International Collaborative Addiction Medicine Research Fellowship (R25-DA037756). BN holds a St. Paul’s Hospital CANFAR Chair in HIV/AIDS Research. MJM is supported by the US NIH (U01-DA0251525).
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.