
Abstract
Background:
Screening and brief interventions (SBI) can help identify opioid safety risks and healthcare professionals can accordingly intervene without a significant increase in workload. Pharmacists, one of the most accessible healthcare professionals, are uniquely positioned to offer SBI. To design an effective intervention with high potential for implementation, we explored pharmacist needs and barriers regarding SBI for opioid use disorders.
Methods:
Using the Consolidated Framework for Implementation Research (CFIR), we conducted 11 semi-structured 60-minute interviews with community pharmacists. We used a purposeful sample of English-speaking pharmacists practicing in varied pharmacies (small independent, large-chain, specialty-retail) and positions (managers, owners, full-time/part-time pharmacists). Transcriptions were analyzed using deductive content analysis based on CFIR constructs, followed by inductive open coding. Utilizing a theoretical framework for data collection and analysis, a diverse sample of pharmacist roles, peer debriefing, and 2 independent coders for each transcript, altogether increased the credibility and transferability of our research. Data collection and analysis continued until data saturation was achieved.
Results:
Pharmacists described good working relationships with colleagues, organization cultures that were open to new initiatives, and believed the SBI to be compatible with their organization goals and pharmacy structure, which are facilitators for future SBI implementation. Pharmacists were motivated by improved patient outcomes, more patient interaction and clinical roles, representing facilitators at the individual level. They also described stigma toward patients, mixed need for change, and lack of knowledge regarding SBI, which are potential barriers to be addressed. Pharmacists believed that the SBI model was adaptable, not complicated, and benefits outweighed implementation costs.
Conclusions:
We addressed current SBI literature gaps—mainly lack of focus on implementation and contextual data, through rigorous implementation-focused qualitative research. Our exploratory findings have direct implications on future pharmacy-based SBI implementation.
Introduction
Prescription-opioid-involved death rates increased by 16% in 2020, despite the declining trend in opioid prescribing rates observed since 2012. 1 While stricter opioid prescribing guidelines have not sufficiently addressed opioid safety concerns, they have also led to opioid access issues. 2 Prevention interventions such as screening, education, prescription monitoring programs, and naloxone dispensing can reduce risky opioid use and promote opioid safety, while ensuring appropriate medication access. 3 Community pharmacists are uniquely positioned to offer opioid use disorder (OUD) prevention interventions due to their high accessibility and medication expertise. 4 Pharmacists can aid in primary prevention of OUD by counseling patients regarding safe medication use and be involved in secondary (screening) and tertiary (harm reduction) prevention. 4 However, in the United States, the role of the community pharmacist in OUD prevention has been limited.
One secondary-tertiary prevention model for risky substance use is the Screening, Brief Intervention, and Referral to Treatment (SBIRT) model. SBIRT is a comprehensive, early intervention for individuals at risk for substance use disorder (SUD) that may involve subsequent referral to more intensive treatment. 5 The SBIRT must be brief, comprehensive, universal, and address a specific behavior in a non-substance abuse treatment facility. 5 The less comprehensive model—screening and brief interventions (SBI) have been studied more extensively.6 -8 SBI research indicates that patients already meeting criteria for diagnosis of a disorder will need more intensive treatment than brief interventions. 9 This necessitates novel SBI for patients who have not yet developed an OUD, rather than only focusing on patients with OUD. Additionally, different brief interventions other than counseling must be explored. While efficacy evidence for alcohol-focused SBI is strong, effectiveness data in real-world settings are mixed. 10 Future implementation barriers must also be considered during the design phase of the intervention. Finally, existing SBI research has focused on inpatient primary care and emergency settings, 11 but outpatient settings such as community pharmacies have not been studied extensively.
Efforts to utilize the community pharmacists as a resource in all types of OUD prevention, including SBI have amplified recently.4,12 Screening using prescription drug monitoring programs (PDMP)13,14 and brief interventions such as naloxone dispensing15,16 or opioid counseling have been studied in pharmacy settings. 17 While emerging research on pharmacy-based SBI for OUD shows promising results,18,19 barriers such as lack of clinical information and discomfort in talking to patients exist. 20 Community pharmacists can be a valuable resource in prevention and treatment of OUD, if such barriers are addressed. Therefore, it is essential to first explore needs and barriers among community pharmacists and accordingly design SBI.
The development of a pharmacy-based SBI must incorporate pharmacist views in initial design. This will lead to the development of an intervention that is more feasible for pharmacists to deliver, with greater chance of successful implementation. To design an effective SBI with high potential for implementation, we explored such needs and barriers regarding SBI among community pharmacists dispensing opioid prescriptions. We expected to identify needs such as training to deliver intervention and barriers such as managing time and balancing responsibilities.
Methods
Theoretical and Conceptual Frameworks
Designing for Dissemination and Implementation
The study used the principles under the processes domain and corresponding actions in the Designing for Dissemination and Implementation framework to guide study design and methods. 21 The potential actions were adapted to be specific to the study (Table 1).
Designing for Dissemination Principles and Corresponding Actions.
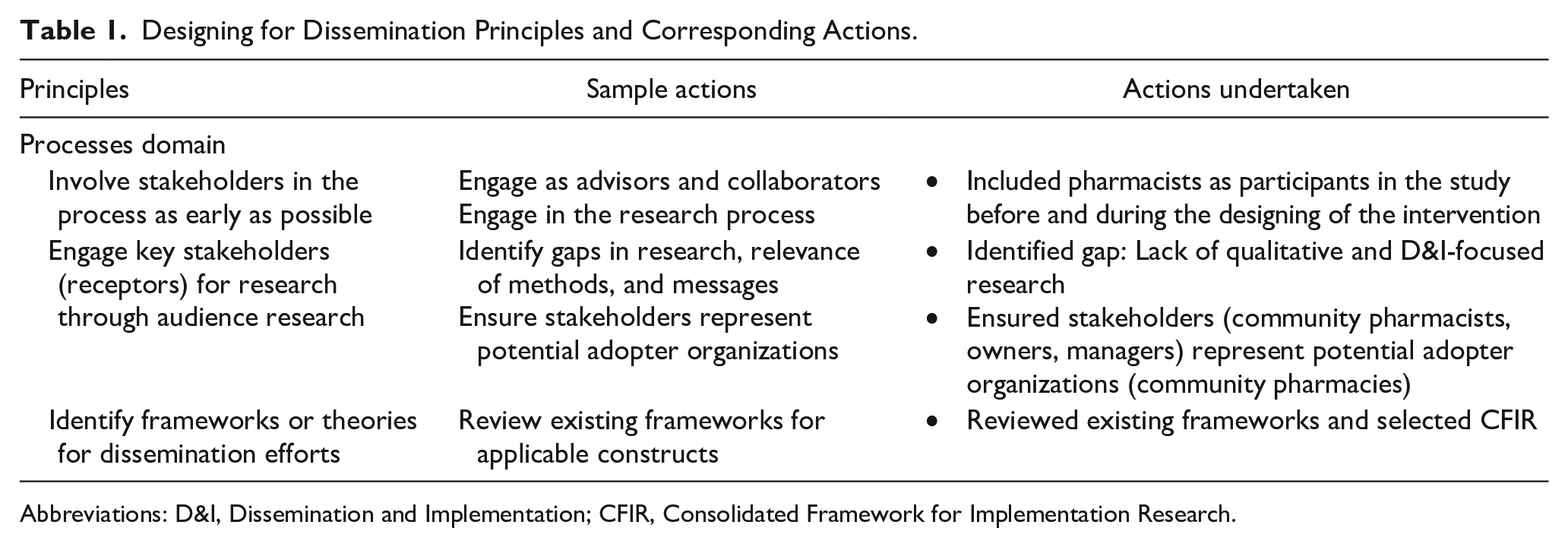
Abbreviations: D&I, Dissemination and Implementation; CFIR, Consolidated Framework for Implementation Research.
Consolidated Framework for Implementation Research
The Consolidated Framework for Implementation Research (CFIR) was developed by identifying and combining various theories that facilitated translation of research findings into practice. 22 Not all constructs under the CFIR domains are appropriate for intervention design, as some are implementation specific. The constructs that were appropriate and included have been bolded in Table 2. The CFIR interview guide 23 was used to develop specific interview questions and the accompanying codebook template was used for initial deductive coding of interview data.
CFIR Constructs (With Bolded Constructs Included in the Study).
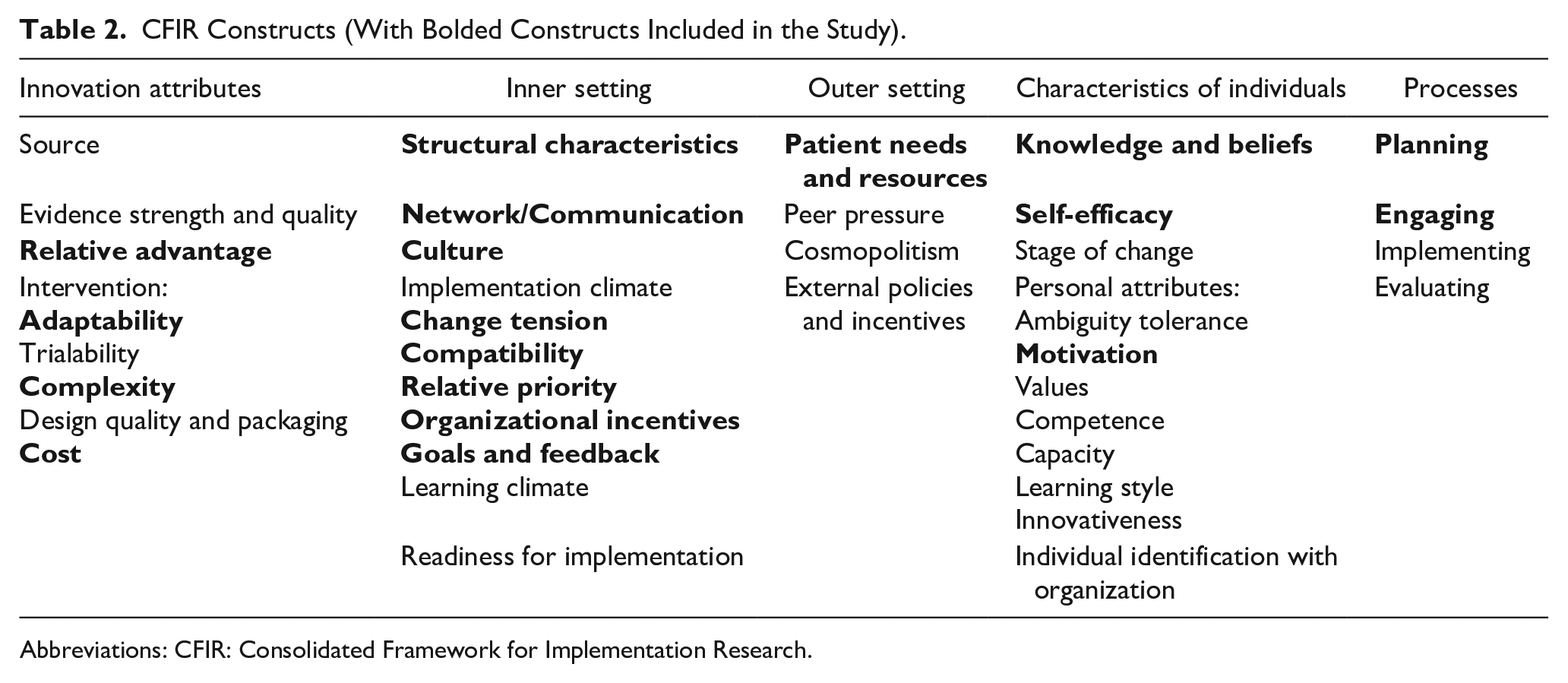
Abbreviations: CFIR: Consolidated Framework for Implementation Research.
Study Sample
Generally, 10 to 20 participants are considered sufficient for theory-based qualitative studies using content analysis approaches.24,25 Initially, the sample was planned to include 15 participants. However, the final sample size was reduced due to higher information power of the completed interviews. 25 This was gained by sample specificity (purposive sampling rather than convenience), using an applied CFIR, the strong quality of dialogue (lengthy, in-depth interviews), and the exploratory nature of analysis (identifying patterns/themes rather than in-depth phenomenological description). 25 Thus, interviews were conducted until data saturation was achieved, that is, no new dimensions regarding the topic emerged. 26 A purposive sample of English-speaking community pharmacists practicing in a Midwestern state was used. Exclusion criteria were practicing in a non-retail setting or not licensed to practice in the state. All types of community pharmacies (small/independent vs large pharmacy chain) were included because the intervention was intended for any type of community pharmacy. Moreover, variance in practice characteristics in the sample was beneficial to gain richer qualitative data. Although, the interview guide remained consistent, probing questions depending on the different practice settings were included. The Institutional Review Board at the authors’ institution exempted the study procedures.
Data Collection
An advertisement in the Pharmacy Practice Enhancement and Action Research Link (PearlRx) newsletter describing the study opportunity and contact information of the researchers was placed. The newsletter emails were linked to a Qualtrics screening form to identify eligible pharmacists. A reminder email was sent 3 weeks after the first email. Pharmacists were also recruited using an informal list curated by the study team for other studies. All emails sent to pharmacists on this list included an information sheet that described the study in detail.
All semi-structured interviews were conducted virtually using university-approved web-conferencing software. The lead researcher (DR) with prior experience in qualitative methods conducted all the interviews. Verbal informed consent was solicited prior to beginning the interview. The 60-minute interviews were audio-recorded. Auto-generated transcripts from the software were used for data analysis. Pharmacists received $50 incentive for participation.
Interviews explored pharmacists’ roles in OUD prevention and individual characteristics, pharmacy culture in general and specific to SBI (inner setting), and their perceptions of the SBI model (intervention characteristics). Additional questions regarding education and practice settings were also added to the pharmacist interview guide. The interview guide was piloted in the initial interviews and probing questions regarding typical process of dispensing opioid medications were added. Following the SBI knowledge question, if pharmacists reported not being familiar with the model, a brief description of the SBI model 5 was given. The sample interview questions linked to the CFIR constructs are provided as Supplemental Digital Content.
Data Analysis
Interview transcripts were analyzed using deductive and inductive content analysis by 3 researchers (DR, CM, MM). We conducted deductive analysis based on the CFIR constructs followed by an inductive approach using descriptive and open coding to identify other relevant codes not covered by CFIR. Two researchers independently coded each interview transcript and discussed their coding in detail. Any conflicts in the coding were resolved at this stage. Finally, DR abstracted all categories into themes and then matched them to the CFIR constructs. Two researchers (OS, JF) who were not involved in the data collection process reviewed the final matched themes to improve credibility and trustworthiness of the findings.
Rigor
Qualitative rigor was achieved by establishing credibility and confirmability through purposeful sampling, using the CFIR to guide data collection and analysis, achieving data saturation, using multiple coders for analysis (analyst triangulation), and peer debriefing. 27
Results
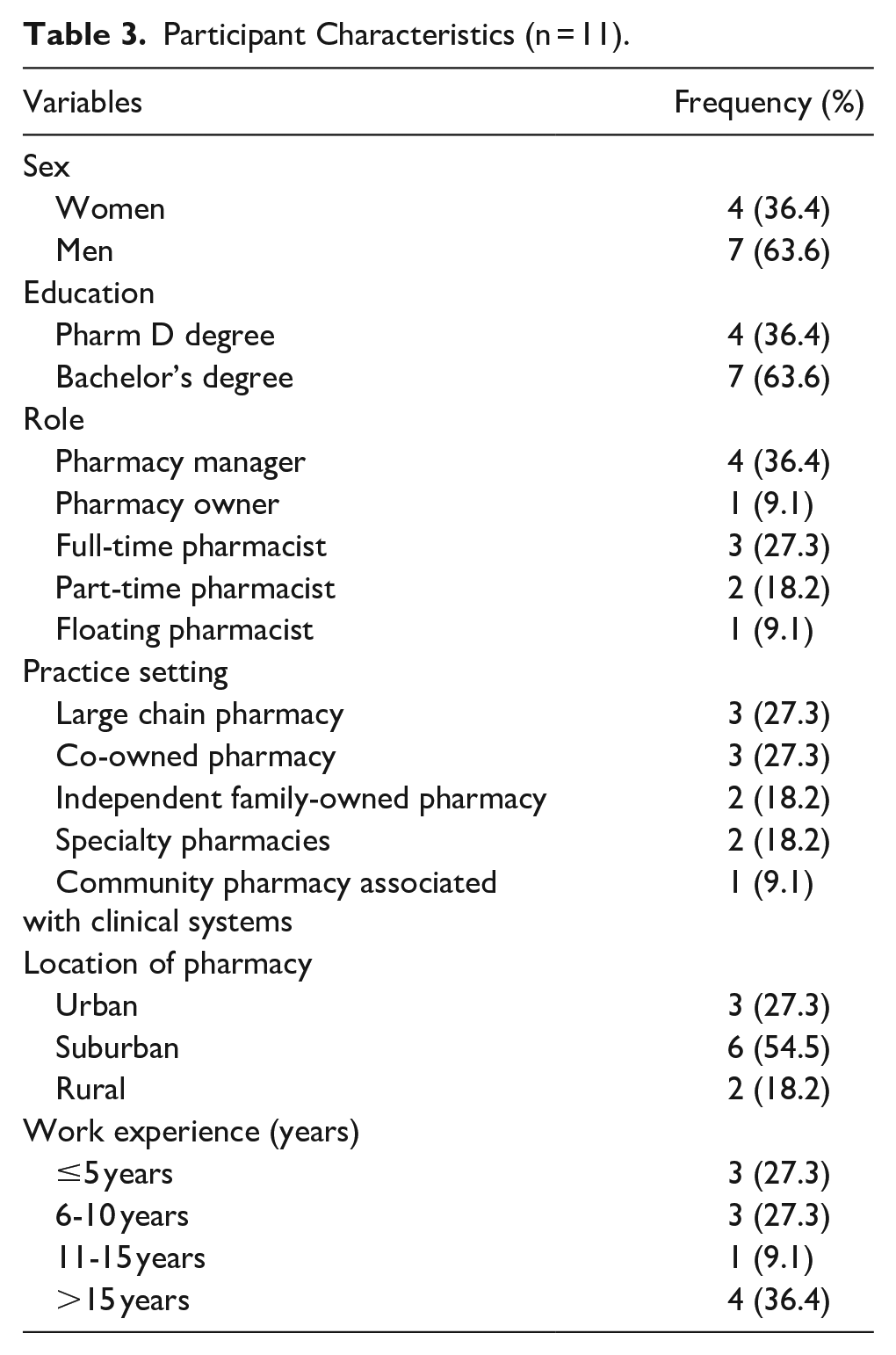
Eleven semi-structured interviews were completed virtually with community pharmacists. Sample characteristics are shown in Table 3. Salient themes from the deductive analysis have been categorized using CFIR domains and constructs and described below. Themes from inductive analysis have also been matched to CFIR constructs wherever possible and included below. Representative quotes and summary of the themes are included in Table 4.
Participant Characteristics (n = 11).
Qualitative Themes and Representative Quotes.
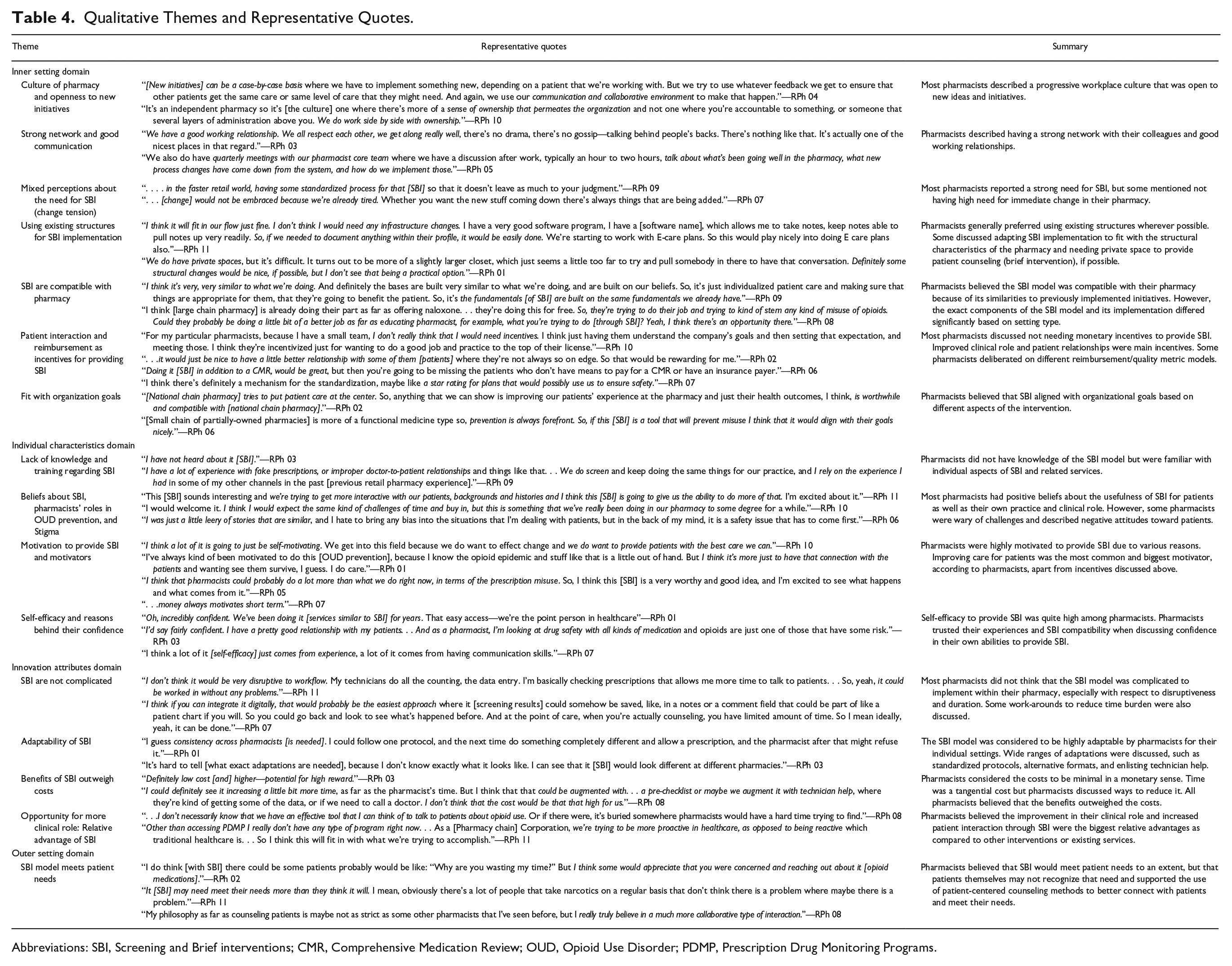
Abbreviations: SBI, Screening and Brief interventions; CMR, Comprehensive Medication Review; OUD, Opioid Use Disorder; PDMP, Prescription Drug Monitoring Programs.
Inner Setting Domain
Theme: Culture of Pharmacy and Openness to New Initiatives
Most pharmacists described a progressive workplace culture that was open to new ideas and initiatives. Although most pharmacists described the culture as collaborative, one pharmacist mentioned a more top-down approach, with newer employees not being involved in creating change. One pharmacist also noted that despite having a good working culture, the ongoing pandemic led to a busy and high-pressure environment leading to stress and burnout.
Theme: Strong Network and Good Communication
Pharmacists described having a collaborative network and good working relationships with colleagues, including supervisors, leadership, and subordinates. Communication channels varied, including meetings, emails, educational sessions, and feedback loops. Pharmacists typically used their immediate supervisors for problem-solving but also had avenues to communicate with leadership.
Theme: Mixed Perceptions about the Need for SBI (Change Tension)
While many pharmacists believed there was a strong need for SBI, some also said there was no sufficient need for change (change tension) to overcome barriers. Pharmacists who described positive work cultures typically believed that workflow changes to include SBI would be welcome and could create a system to integrate existing services. A few pharmacists stated that change tension was low because of already busy work schedules or unsupportive supervisors.
Theme: Using Existing Structures for SBI Implementation
Most pharmacists did not perceive a need for structural changes for the optimum implementation of SBI. However, the exact process of SBI implementation was specific to the setting. For example, many pharmacists discussed the need to create a documentation system but described various formats (electronic records, written hard copy protocols, or standardized forms). They stated that other needs such as private space for patient counseling could be met by modifying the waiting area to resemble a doctor’s office and offering more privacy.
Theme: SBI are Compatible with Pharmacy
Pharmacists from all types of settings believed SBI were compatible with their pharmacy settings, mainly due to the similarity of the SBI model with other previously implemented initiatives. However, the actual components and process of providing SBI differed based on the existing work processes. For example, in smaller independent and specialty pharmacies, participants discussed patient-centered counseling as the brief intervention while fast-paced large chain pharmacies mentioned naloxone as the most appropriate brief intervention. Pharmacists also discussed how SBI would build on existing initiatives to improve effectiveness.
Theme: Patient Interaction and Reimbursement as Incentives for Providing SBI
Organizational incentives required for providing SBI were closely linked to the individual motivator (discussed below). Most pharmacists identified primary incentives of increased clinical role and patient interaction through SBI. Some discussed various models of reimbursement such as incorporating SBI as a “Comprehensive Medication Review (CMR)” service, using models such as the “cognitive billing” through the Medicaid fee-for-service plans, or incorporating SBI services as part of quality ratings or other insurance plan metrics.
Theme: Fit With Organization Goals
Almost all pharmacists reported that the SBI model aligned with their organizational goals. Pharmacists recognized different aspects of SBI as fitting with their respective organizational goals, including prevention, patient-centered care, or specific focus on OUD initiatives.
Individual Characteristics Domain
Theme: Lack of Knowledge and Education/Training Regarding SBI
Pharmacists in general were unfamiliar with SBI. However, when given a brief explanation of the model, some felt that their routine practice currently incorporated elements of screening or brief intervention. Pharmacists reported not receiving any education or training related to SBI. Only 1 pharmacist reported training in motivational interviewing (a practice session regarding smoking cessation during PharmD training). However, all pharmacists had good knowledge regarding opioid safety and were familiar with identifying inappropriate prescriptions, naloxone dispensing, and counseling patients.
Theme: Beliefs About SBI, Pharmacist Roles in OUD Prevention, and Stigma
Most pharmacists had positive beliefs about the SBI model. They believed SBI would be helpful in increasing opioid safety and improving patient outcomes. They also discussed SBI increasing patient interaction, giving them the ability to provide more clinical services. This tied into their perceived current role as a gatekeeper rather than clinician in OUD prevention and treatment. Although pharmacists discussed challenges of time and stakeholder buy-in, they were optimistic of SBI being an effective tool, if implemented within existing workflows. However, some pharmacists also expressed skepticism or bias against patients with opioid prescriptions, indicating the presence of stigmatizing attitudes.
Theme: Motivation to Provide SBI and Motivators
Pharmacists were highly motivated to provide SBI. Preventing OUD and risky behaviors and improving patient outcomes by providing the best care possible were the most important motivators. They also discussed the opportunity to provide more clinical services and connect with patients through SBI as important motivators. Some pharmacists discussed reimbursement as a necessary long-term motivator.
Theme: Pharmacists’ Self-efficacy and Confidence
Pharmacists reported feeling very confident in their ability to provide SBI due to prior experience or practice with OUD prevention interventions, compatibility of SBI with setting or current practice (if barriers to implementation were addressed), or years of work experience as a pharmacist.
Innovation Attributes Domain
Most pharmacists suggested that screening should be brief (needing <5 minutes) and augmented by PDMP. Potential brief interventions suggested were: (1) naloxone dispensing, (2) contacting prescribers about inappropriate opioid prescriptions, (3) patient education or counseling, and (4) referral to treatment.
Theme: SBI are Not Complicated (in Terms of Disruptiveness or Duration)
Pharmacists believed SBI are easy to implement and not complicated. They did not perceive it to be disruptive to their workflow if its implementation was tailored to their setting. All but one pharmacist believed SBI were not time-intensive because of the brief nature of the screening (<5 minutes) and intervention (10 minutes). Some pharmacists also suggested using technicians, digital screening, or having the patient complete screening independently to reduce time burden.
Theme: Adaptability of the SBI Model
As described previously, all pharmacists discussed adaptation of the SBI model in terms of individual components to be included and the process of providing the intervention, based on inner setting constructs. Adaptations ranged from minor changes such as creating a standardized protocol for providing SBI to larger changes such as incorporating providers into the intervention protocol as stakeholders or creating a digital SBI.
Theme: Benefits of SBI Outweigh the Costs
All pharmacists perceived SBI to require minimal costs and mostly included printing costs for paper materials. Most did not perceive the time needed as a significant cost because the SBI model is designed to be brief. However, some pharmacists mentioned that there could be revenue loss if pharmacists refused to fill potentially inappropriate prescriptions or provided interventions that took longer than 15 minutes. All pharmacists believed benefits outweighed costs significantly.
Theme: Opportunity for More Clinical Role: Relative Advantage of SBI
Most pharmacists did not provide prevention interventions specific to OUD that involved any patient interaction. Pharmacists saw opportunities for more clinical services and patient interaction as the biggest advantage of SBI over other interventions. Pharmacists from smaller independent pharmacies perceived SBI as a great addition to existing services or replacement of previously implemented but discontinued interventions.
Outer Setting Domain (Construct: Patient needs)
Theme: SBI Model Meets Patient Needs
All pharmacists believed that SBI met the needs of their patients, based on previous experiences specific to opioid prescriptions. Pharmacists believed the potential increase in patient knowledge regarding opioid safety through SBI would be the biggest factor in meeting needs, even if patients are unaware of knowledge gaps. Additionally, pharmacists discussed using patient-centered counseling methods to better connect with patients.
Discussion
This study resulted in identifying pharmacist perceptions and barriers regarding OUD SBI for the community pharmacy setting. With respect to the inner setting, pharmacists described important facilitators for effective implementation of SBI, including positive working cultures and strong communication with colleagues and supervisors. Existing communication channels within pharmacies could also be used to disseminate information about SBI and provide avenues for linking potential adopter organizations in the future. However, a possible barrier to future implementation was the mixed perceptions about the need for change. Although all pharmacists believed SBI would be beneficial to patients, some pharmacists suggested there was a stronger need to reduce pharmacist workloads, rather than add to them. Involving technicians and using digital technologies in SBI implementation may help address this barrier. However, impact of digital interventions on healthcare professionals’ workload and efficiency is still an emerging topic of research.28,29
Pharmacists generally had positive perceptions of compatibility and fit with organization goals, which are important facilitators of future SBI implementation. SBI components and its implementation format will need to be adapted for different pharmacies to ensure maximum compatibility, which also relates to the high adaptability of the SBI model. Similarly, while most pharmacists stated that no infrastructure changes would be needed, many adaptations were recommended. For example, for creating private space for consultation, some suggested making minor changes to the existing pharmacy layout, while others suggested providing handouts to reduce the amount of information that is shared verbally, to reduce privacy risk.
Incentives and motivators to provide SBI primarily included improved opioid safety and patient outcomes, more patient interactions, and improved clinical role in OUD prevention. These motivators can be emphasized during future SBI implementation to facilitate greater reach and adoption of SBI in pharmacies. However, for higher sustainability, reimbursement for providing SBI may be necessary, depending on the state regulations regarding pharmacist reimbursement. 30 Apart from these motivators, providing resources and fitting SBI into the workflow of the pharmacy are essential, especially in fast-paced retail settings. 31
We found that pharmacists were not familiar with the SBI model but were familiar with some components, such as naloxone and PDMP. However, evidence regarding naloxone dispensing32,33 and PDMP use14,34 among pharmacists is mixed. While pharmacists have knowledge regarding naloxone and are willing to dispense it, they do not feel comfortable initiating these discussions with patients.32,33 Similarly, pharmacy PDMP use is restricted by lack of integration within pharmacy systems.14,34 Finally, none of the pharmacists reported having received any formal education or training regarding SBI for SUD, which is not surprising as substance-use specific education in pharmacy schools in the United States is lower than the recommended levels. 35 Pharmacists believed that lack of time, clinical information, and buy-in from upper management could be barriers to SBI implementation, which is congruent with previous research. 36 However, an additional barrier in our sample was presence of negative and stigmatizing attitudes toward patients taking opioid medications. Although few pharmacists openly discussed stigma and bias, many pharmacists were afraid of offending patients or labeling them as “addicts.” Our previous research suggests that there is a relationship between pharmacists considering screening as important and higher stigma toward patients with SUD, 37 which makes screening a punitive measure rather than an avenue to offer clinical services. These knowledge and beliefs barriers must be addressed through specific training-based implementation strategies, and SBI must be packaged as a harm reduction effort to avoid patient harm. Despite these barriers, pharmacists were highly confident in their ability to provide SBI because they had experience with many individual components or had offered similar interventions previously.
With respect to the SBI model itself, most pharmacists believed it was not complicated. They also believed that duration could be shortened by using technicians or digital methods for screening. To ensure that innovation is not disruptive but tailored to the settings and workflow, a highly adaptable intervention is necessary. Allowing for flexibility of adaptation must be balanced with ensuring intervention standardization and consistency across settings. Finally, the costs of implementation were not believed to be high because SBI could be tailored to routine practice. The brief nature of the SBI model and minimal supply costs (printing handouts/forms) also reduced perceived time investment. Pharmacists also believed that the benefits associated with SBI were much higher than the costs, as there was no existing SBI-like intervention in their pharmacies, which relates to the relative advantage of SBI over other interventions.
A study limitation is that pharmacists were sampled from lists formed based on interest in participating in research. Pharmacists in our sample could also be highly interested in improving care for OUD, which may have influenced our themes. Although we have attempted to increase credibility of our findings by showing disagreement among pharmacists and highlighting contrasting aspects of themes, care must be taken when generalizing our findings as the sample was from one Midwestern state. Although pharmacists serving many different roles (managers and owners) and practicing in a variety of settings were recruited in our study, we did not include pharmacy technicians. Opioid prescribers and OUD-treatment providers are also stakeholders who must be involved in future research. Finally, our study focused only on the SBI portion of the SBIRT model. Although some pharmacists mentioned needing resources for referral, creating a warm handoff for the patient, and increasing access to medications for OUD, this was not a major theme. Future research should explore the referral to treatment component further by engaging treatment providers and connecting them with pharmacists within the same study.
Conclusion
Our study aimed to address the existing limitations in the current SBI literature—mainly the lack of focus on SBI implementation and gaps in contextual data, through rigorous implementation-focused qualitative research. We conducted qualitative interviews with pharmacy stakeholders to identify needs and barriers to participate in SBI. We have also focused on implementation of SBI by using designing for dissemination and implementation principles and the CFIR to design the study measures and interpret findings. We identified several important needs among pharmacists regarding OUD prevention that could be addressed by SBI. We also identified barriers to participation in SBI as well as solutions to address these challenges. Our exploratory findings have direct implications on future research where SBI can be piloted within community pharmacy settings.
Supplemental Material
sj-docx-1-saj-10.1177_29767342231211428 – Supplemental material for An Implementation-Focused Qualitative Exploration of Pharmacist Needs Regarding an Opioid Use Disorder Screening and Brief Intervention
Supplemental material, sj-docx-1-saj-10.1177_29767342231211428 for An Implementation-Focused Qualitative Exploration of Pharmacist Needs Regarding an Opioid Use Disorder Screening and Brief Intervention by Deepika Rao, Christine McAtee, Meg Mercy, Olayinka O. Shiyanbola and James H. Ford II in Substance Abuse
Footnotes
Author Contributions
DR originated the project and obtained funding with the support of OS and JF. DR led data collection and analysis with the support of CM and MM. DR drafted the initial article. All authors participated in interpreting the results, contributed to the writing of the article, provided critical feedback to the article, and approved the final article draft for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Sonderegger Research Center for Improved Medication Outcomes. DR also received the Joseph B. Wiederholt Fellowship, 2021 to support this project. Supporting organizations had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board’s approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.