
Abstract
Background:
The COVID-19 pandemic has impacted public infrastructure and healthcare utilization. However, regional variation in opioid-related harm secondary to COVID-19 remains poorly understood. This study aimed to measure the regional variation in the association between stay-at-home orders (SAHOs) and nonfatal opioid-related emergency medical services (EMS) transfers in the United States.
Methods:
In this interrupted time series design, counts of nonfatal opioid overdoses were identified in each week between July 29, 2019 and December 27, 2020 from the National Emergency Medical Services Information System Dataset. A longitudinal, interrupted time series model was used to compare the change in the number of nonfatal opioid overdose transfers between the pre-pandemic period (July 29, 2019-January 6, 2020) and the pandemic period (June 1, 2020-December 27, 2020). The time period between January 7, 2020 and May 31, 2020 was treated as a washout period to account for state-level variation in the timing of SAHO implementation.
Results:
We identified 277 141 adult nonfatal opioid-related overdose EMS transfers in the United States across all census regions. After implementation of the SAHO, EMS transfers significantly increased in all regions, with an increase most notable in the Southern United States (2161, 95% CI: 1699-2623 transfers per week). In the post-SAHO period between June 1 and December 27, 2020, EMS transfers declined from this regional peak in the Southern, Midwestern, and Northeastern United States. No change in trend was observed in the Western United States.
Conclusion:
These findings underscore the importance of tailoring public health policies regionally. While most regions saw a modest decline in opioid-related EMS transfers after an initial increase, the COVID-19 pandemic led to notable increases in opioid-related EMS transfers nationwide. Future research should focus on identifying public health strategies to counteract the deleterious effects of the COVID-19 pandemic on opioid-related morbidity.
Keywords
Background
Opioid-related emergency department visits increased by 37% between December 2019 and December 2020. 1 Despite significant efforts to counter opioid-related morbidity and mortality in recent years, the opioid crisis continues to impact emergency medical services (EMS) and first responders across the United States. 2 As the overdose crisis continues, EMS providers have been forced to respond to an increasing number of fatal and nonfatal opioid overdoses, particularly among younger adults in public places. 3 The marked increase in overdose-related EMS utilization can likely be attributed to 2 distinct phenomena: fentanyl and xylazine contamination increasing the toxicity of the American drug supply and the onset of the COVID-19 pandemic.4 -6
Early in the COVID-19 pandemic, opioid prescribing declined by as much as 34% nationally before returning to pre-pandemic levels. 7 This phenomenon is likely attributable to patient reluctance to seek in-person care, state-level policies intended to minimize nonessential in-person care, and evolving restrictions on telehealth prescribing of controlled substances during the early stages of the pandemic.6,8 Despite the potential interpretation of a reduction in opioid prescribing as a net positive, an increase in high-risk illicit drug use likely undermined the potential benefit to public health. 9 Wainwright and colleagues reported that the urine drug tests’ results during the COVID-19 pandemic had a 1.67-fold increase in the odds of containing fentanyl compared to those obtained prior to the pandemic. 9 The available evidence suggests that the onset of the COVID-19 pandemic undermined valuable progress made in reducing the burden of opioid-related harm in the United States. The United States, however, is a large and diverse country, and prior evidence suggests that the impacts of the opioid epidemic varied both regionally and supra-regionally, even before the COVID-19 pandemic began. 10
Changes in the frequency and characteristics of EMS visits may be an advanced indicator of changes in opioid morbidity. Prior evidence demonstrated a nationwide increase in EMS transfers following state-level stay-at-home order (SAHO) implementation. 11 Regional variation in this phenomenon, however, remains unmeasured. The United States is a vast country with significant sociodemographic variation at the regional level. Measuring regional differences in the trajectory of opioid-related morbidity in the wake of SAHO implementation can provide policymakers and public health authorities with useful information to focus future opioid response efforts. Therefore, this study aimed to measure regional variation in nonfatal opioid overdose-related EMS transfer activity before and after implementing the US COVID-19 SAHO.
Materials and Methods
Study Design and Data Source
We applied a longitudinal, interrupted time series design to data from the 2019 to 2020 National Emergency Medical Services Information System (NEMSIS) to measure regional changes in the rate of nonfatal opioid overdose-related EMS transfers resulting from SAHO implementation. This study was approved by the University of Houston’s Research Ethics Committee (approval no. 3630) on April 12, 2022. NEMSIS collates reports of EMS transfers from over 10 000 EMS organizations in all 50 US states, the District of Columbia, and Puerto Rico. 12 Each record in the public use file contains information on the reason for the call, the ultimate disposition of the patient, and the US census region. The number of EMS transfers related to nonfatal opioid overdose in each region was counted for each week between July 29, 2019 and December 27, 2020, and grouped by US census region (Midwest, South, Northeast, and West). Eligible EMS transfers were defined as those in which naloxone was administered before or after EMS personnel arrived on scene or those that were ultimately coded as opioid overdoses (ICD-10: T40.X). 1 These weekly counts served as the primary outcome measure in the analysis. A binary indicator variable was used to group weekly counts into pre- and post-COVID-19 SAHO implementation periods. The pre-pandemic period was defined as the period between July 29, 2019 and January 6, 2020, and the post-stay-at-home implementation period was defined as the period between June 1, 2020 and December 27, 2020. The exact implementation date of pandemic-related SAHO varied widely between states with the last implementation occurring on May 27, 2020. For this reason, the period between January 7 and May 31, 2020 was treated as a washout period to account for varying initiations of SAHO implementation. Note that EMS transfers that occurred in Puerto Rico were not included in the analysis as Puerto Rico is not assigned to a US census region.
Statistical Analysis
The total number of nonfatal opioid overdoses in each week before and after the implementation period was summarized and graphed descriptively. Initial visual inspection of the trends indicated that the changes in the rate of EMS transfers over time were generally linear in the pre- and post-pandemic periods and supported the use of a linear time series structure. An autoregressive, interrupted time series model was specified for each US census region to estimate the impact of SAHO implementation on nonfatal opioid overdose-related EMS transfers.13,14 Each model included a term for the secular trend in pre-pandemic EMS transfers, the change in the rate of transfers in the post-pandemic period, and a third term representing the immediate change, or level change, in the number of weekly EMS transfers between the pre- and post-SAHO implementation periods. Initial models for each region were estimated using ordinary least squares linear regression. The Durbin–Watson statistic was then evaluated for autocorrelation. 14 In the event that the Durbin–Watson statistic was less than 1.5 or over 2.5, autoregressive terms were added to control for noise caused by the correlation between consecutive observed counts. 15 The number of autoregressive terms was determined by reviewing the autocorrelation and partial autocorrelation function estimated from an ordinary least squares time series model and estimating subsequent autoregressive models with the determined number of autoregressive terms using the Yule–Walker method. The Durbin–Watson statistic was then reassessed, and this process was repeated until the Durbin–Watson statistic fell between 1.5 and 2.5 suggesting adequate control of autocorrelation. All models were estimated using PROC AUTOREG in SAS Version 9.4 (SAS Institute Inc, Cary, NC, USA).
Results
There were 277 141 adult nonfatal opioid-related overdose EMS transfers observed between July 29, 2019, and December 27, 2020, among EMS organizations reporting to NEMSIS. Over the duration of the study period, the Southern region saw the highest number of total transfers (South = 134 732; West = 43 190; Northeast = 46 800; Midwest = 52 419). In the interrupted time series model, the number of weekly EMS transfers were trending negatively in the Western region of the United States in the pre-pandemic period (−12 transfers per week; 95% CI: −18; −5 transfers per week) but no significant trend was observed prior to SAHO implementation in other census regions.
In the post-SAHO implementation period (June 1-December 27, 2020), the number of opioid-related EMS transfers increased significantly in all regions (Midwest: 903; 95% CI: 493-1312 transfers per week, Northeast: 731; 95% CI: 541-922 transfers per week, West: 830; 95% CI: 617-1043 transfers per week), but the increase was most pronounced in the Southern United States, where nonfatal overdose EMS transfer volume increased by an estimated 2161 (95% CI: 1699-2623) transfers per week. In the post-implementation period, transfers trended slightly down from the observed peak until the end of the study period on December 27, 2020. The observed decreasing trend ranged from −27 (95% CI: −43, −10) transfers per week in the Midwest to −14 (95% CI: −20, −7) transfers per week in the Northeast. EMS transfers in the Western United States remained elevated with no change in trend (4 transfers per week, 95% CI: −4, 12 transfers per week) through the post-implementation period. Of note, the diagnostics from the ordinary least squares models in each region all demonstrated some degree of positive autocorrelation (Durbin–Watson <1.5). This led us to proceed with the addition of a single-lag autoregressive term in each regional model, which led to satisfactory control of autocorrelation. Table 1 contains a summary of all 4 regional models, and Figure 1 contains a graphical depiction of the estimated changes in EMS transfers over time along with a scatter plot of the observed number of EMS transfers in each region.
Parameter Estimates from 4 Autoregressive Interrupted Time Series Models Estimating the Effect of COVID-19-Related Stay-at-Home Order Implementation on the Number of Nonfatal Opioid Overdose EMS Transfers.
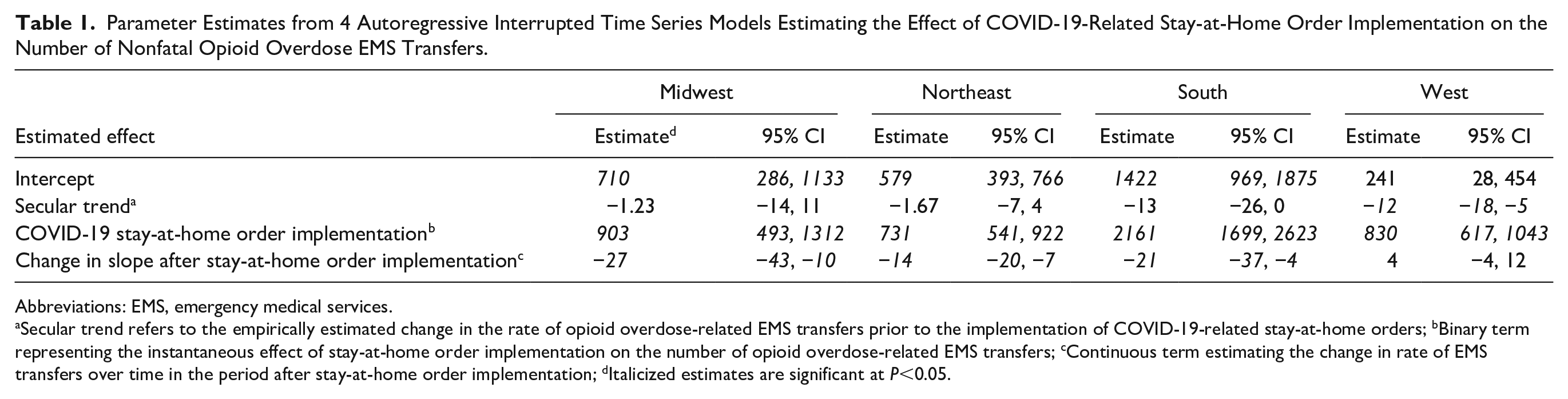
Abbreviations: EMS, emergency medical services.
Secular trend refers to the empirically estimated change in the rate of opioid overdose-related EMS transfers prior to the implementation of COVID-19-related stay-at-home orders; bBinary term representing the instantaneous effect of stay-at-home order implementation on the number of opioid overdose-related EMS transfers; cContinuous term estimating the change in rate of EMS transfers over time in the period after stay-at-home order implementation; dItalicized estimates are significant at P<0.05.
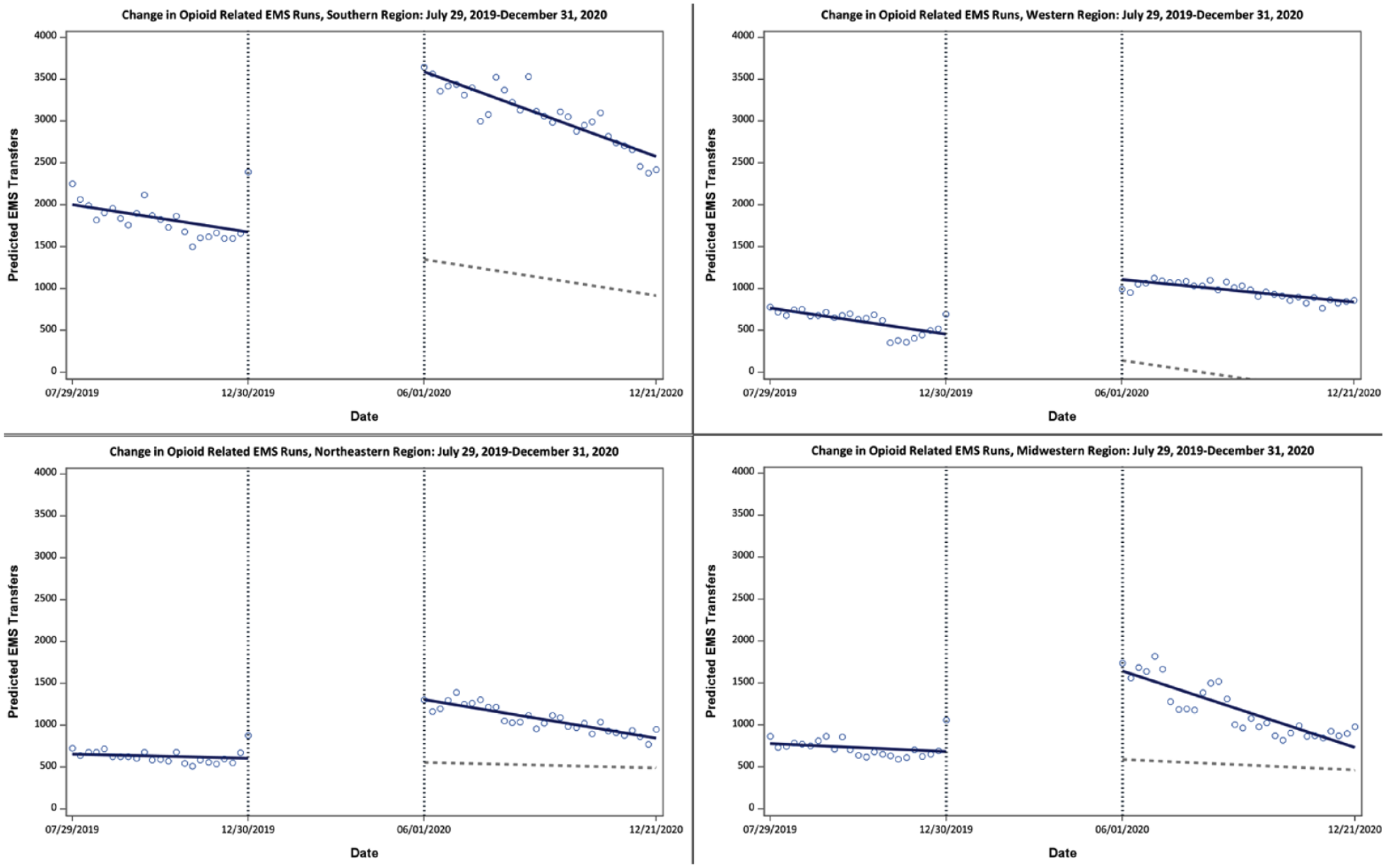
Results of 4 autoregressive time series models reported the change in opioid-related EMS transfers resulting from the implementation of COVID-19-related stay-at-home orders in each US census region.
Discussion
Previous studies have examined the impact of the COVID-19 pandemic on the opioid crisis at the national, individual state, and individual county levels, limiting generalizability.11,16,17 In contrast, our study focuses on regional variation in opioid-related EMS transfer activity. This study is the first to assess the connection between the COVID-19 pandemic and the SAHO on the weekly frequency of nonfatal opioid-related EMS runs between US census regions. Our study results indicate regional inconsistencies in the effect of SAHO implementation on opioid-related EMS transfers in the United States. Prior to the implementation of COVID-19-related SAHO, the rate of nonfatal overdose-related EMS transfers was essentially consistent from week to week in all but the Western census region, where the number of transfers was observed to decline week over week. All regions saw a significant, stepwise increase in the number of nonfatal opioid overdose-related EMS transfers immediately after SAHO implementation suggesting an association between the 2 phenomena. After regional increases of up to 2161 transfers per week in the Southern census region, declines in the number of weekly EMS transfers throughout the United States were tepid at best throughout the remainder of the calendar year 2020.
Early in the pandemic, the Drug Enforcement Administration and Substance Abuse and Mental Health Services Administration made significant policy changes to promote continuity of care for patients with opioid use disorder and those receiving chronic opioid therapy for chronic pain. While these efforts may have been successful in preserving access to treatment, 18 the results presented here suggest that merely keeping up with the pace was insufficient. During the pandemic, the number of nonfatal opioid-related overdoses increased across all census regions of the United States, suggesting that the COVID-19 pandemic tangibly disrupted access to harm reduction and treatment services. Such findings highlight the need to reassess regional resource allocations and to address geospatial and demographic disparities in opioid-related morbidity and mortality that may have become more prominent as the COVID-19 pandemic has evolved.
Surveillance strategies aimed at monitoring changes in EMS volume can be an essential part of this approach to public health evaluation. EMS records can provide an early signal of highly localized morbidity impact and aid communities in addressing evolving trends in opioid-related harm. 10 However, an increase in nonfatal opioid-related EMS transfers may not always accurately reflect opioid overdose mortality due to delays in reporting, underutilization of healthcare, or misclassification of death. For instance, if patients are found dead on scene or die in transit, this may lead to underreporting in NEMSIS or other comparable EMS registries. Multiple data sources and trends should be evaluated by future researchers to fully understand the impact of the opioid epidemic during the COVID-19 pandemic.
The South experienced a dramatic increase in the number of weekly EMS transfers after SAHO implementation increasing by an estimated 2161 transfers per week between the last week of the pre-COVID period and the first week after SAHO implementation. The Southern states appear to be disproportionately bearing the burden of the US opioid crisis yet remain under-resourced in attempts to ebb the increasing flow of morbidity and mortality. The opioid epidemic provides a striking example of differential state-level resource allocation and prioritization in the United States. 19 Individuals in the Southern United States are less likely to have access to preventative care and are significantly more likely to be uninsured than those in other regions.19,20 More recent findings suggest that individuals in the South may also be less likely to have access to medication for opioid use disorder and other substance use disorder treatment services.18,21,22 While the analysis presented here may, at face value, convey a foregone conclusion that the pandemic led to increases in opioid-related EMS transfers, a closer reading shows an evolving overdose crisis with regional shifts in morbidity that have not yet been addressed by public health authorities. There is a clear and present need for the South to respond to the crisis at their doorstep. This response will require significant policy changes in many states and commensurate efforts to garner public support.
Limitations
This analysis is not without limitations. EMS agencies self-report to NEMSIS. Incompatibility in local data collection may lead to underreporting of opioid-related EMS transfers. This inconsistency is particularly significant if there are differences in fatality rates among each region, which can underestimate or overlook severity and consequences of the SAHO on the opioid crisis. The risk of underreporting indicates the need for future researchers, policymakers, and public health officials to reference multiple data sources to more comprehensively evaluate the impact of the COVID-19 pandemic on rates of opioid overdose.
Additionally, NEMSIS data are limited to information collected at the point of care by EMS and does not include information related to subsequent hospitalizations or long-term outcomes meaning that patients who expired at the hospital or after discharge would have been reported as nonfatal overdoses. Finally, we used a simple linear time series model to estimate changes in nonfatal opioid overdose resulting from SAHO implementation. This decision was intended to improve interpretability. Still, the observed trends were linear, and attempts were made to control for autocorrelation where appropriate. Model fit was generally acceptable, indicating that our approach was appropriate, but more precise modeling approaches, including autoregressive interrupted moving average modeling, generalized linear modeling, or join point regression, may have led to better fitting but less interpretable results. Despite these limitations, this study applied a widely accepted definition of nonfatal opioid overdose, and our results are largely concordant with other literature, supporting the observed regional changes.18,23
Conclusion
This study highlights the need for a comprehensive and coordinated response to address the opioid overdose epidemic, including ensuring access to quality healthcare, mental health services, and addiction treatment. These changes will require collaboration among healthcare providers, public health agencies, and community organizations to address the root causes of the overdose crisis. Public health organizations and policymakers can also use these findings at a regional level to develop effective strategies and prevention programs to mitigate the impact of the opioid crisis.
Supplemental Material
sj-docx-1-saj-10.1177_29767342231208823 – Supplemental material for Regional Variation in Opioid-Related Emergency Medical Services Transfers During the COVID-19 Pandemic: An Interrupted Time Series Analysis
Supplemental material, sj-docx-1-saj-10.1177_29767342231208823 for Regional Variation in Opioid-Related Emergency Medical Services Transfers During the COVID-19 Pandemic: An Interrupted Time Series Analysis by Sahar Yazdanfard, Douglas Thornton, Prachet Bhatt, Bilqees Fatima, Javeria Khalid, Juhyeon Song and Tyler Jordan Varisco in Substance Abuse
Footnotes
Author Contributions
SY was responsible for conceptualization, writing-original draft, writing-review and editing, and data curation. DT was responsible for supervision, project administration, conceptualization, investigation, and resources. JS was responsible for writing-revising and editing. PB, BF, and JK were responsible for writing-original draft and data curation. TV was responsible for formal analysis, methodology, conceptualization, investigation, project administration, supervision, writing-original draft, and writing-revising and editing. All authors contributed sufficiently to receive credit as authors on the final article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Thornton is a consultant for the Texas and Missouri Plaintiff’s Steering Committees for Opioid Litigation and a member of the Texas Opioid Abatement Fund Council. Dr. Varisco receives funding from the Foundation for Opioid Response Efforts.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board’s approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.