
Abstract
Background:
This study examined the risk perceptions related to driving after cannabis use (DACU) among Canadian and US adults who used cannabis in the past six months.
Methods:
Perceptions of danger, normative beliefs, perceived likelihood of negative consequences, and other driving-related variables were collected via online surveys in Canadian (n = 158; 50.0% female, 84.8% White, mean age = 32.73 years [SD = 10.61]) and US participants (n = 678; 50.9% female, 73.6% White, mean age = 33.85 years [SD = 10.12]). Driving cognitions and DACU quantity/frequency were compared between samples using univariate analyses of variance, and Spearman’s (ρ) correlations were performed to examine associations between driving cognitions and DACU quantity/frequency.
Results:
The two samples did not significantly differ in self-reported level of cannabis use, lifetime quantity of DACU, or the number of times they drove within two hours of cannabis use in the past three months (Ps > .12). Compared to US participants, Canadians perceived driving within two hours of cannabis use as more dangerous (P < 0.001, ηp2 = 0.013) and reported more of their friends would disapprove of DACU (P = 0.03, ηp2 = 0.006). There were no differences in the number of friends who would refuse to ride with a driver who had used cannabis (P = 0.15) or the perceived likelihood of negative consequences (Ps > 0.07). More favorable perceptions were significantly correlated with greater lifetime DACU and driving within two hours of use (ρ = 0.25-0.53, Ps < 0.01).
Conclusions:
These findings reveal differences in distal risk factors for DACU between Canada and the US and may inform prevention efforts focusing on perceptions of risk and social acceptance of DACU.
Highlights
Risk perceptions and other attitudes about driving after cannabis use are understudied in Canadian adults who report using cannabis.
Compared to US adults who use cannabis, we found that Canadian adults who use cannabis perceived driving after cannabis use to be more dangerous and more friends would disapprove of doing so.
In both samples, more favorable attitudes were correlated with higher frequency of driving after cannabis use.
These results may have implications for prevention efforts focusing on perceptions of risk and social acceptance of driving after cannabis use.
Introduction
People in Canada and the United States (US) have seen expanding access to cannabis following the legalization of both medicinal and recreational use.1,2 Canadians have been able to access cannabis for medical purposes since 2001, but the Cannabis Act legalized recreational use at the federal level as of October 2018. 3 As of May 2023, recreational use is legal in 23 US states and the District of Columbia, and medicinal use is legal in 38 states and the District of Columbia.4,5 With expanded access, there is increasing emphasis on understanding potential harms to individuals and public health,6,7 including driving after cannabis use (DACU). 8
Expansion in legal access to cannabis in Canada and the US is associated with increased rates of DACU in both countries.9,10 Approximately 4.7% of US residents aged 16 years and older reported DACU in 2018, 11 and 29.5% of US cannabis users reported DACU from 2016 to 2018. 12 The percentage of motor vehicle accident fatalities involving cannabis increased from 9.0% in 2000 to 21.5% in 2018. 13 Rates of DACU are comparable in Canada with national survey data indicating that between 15% and 20% of Canadian adults who use cannabis reported driving within two hours of use.14,15 An online survey study of Canadian young adults between the ages of 16 and 30 years (n = 870) found that over a third of respondents who reported using cannabis in the last year also reported DACU while over 40% of the full sample reported riding in a car with a driver who had been using cannabis. 16
Drivers under the influence of cannabis may experience impairments in their driving ability such as decreased motor coordination, poorer ability to divide attention between two simultaneous tasks, and increased lane deviation.17,18 However, these performance impairments do not always correspond to participants’ beliefs about their driving ability. Wickens et al. 19 reported that some people who use cannabis believed cannabis has a positive impact on their driving. Consistent with these findings, Aitken et al. 20 reported that drivers who use cannabis believed it to be a safe drug for driving. Some drivers drove more slowly and cautiously, while others drove faster to avoid attracting attention. Among 180 Australian adults who reported driving within one hour of cannabis use, only 7% of participants described their driving ability as quite impaired, 42% indicated slight impairment, and 50% believed there was no impairment. 21 In the same study, more than half of people endorsing DACU reported that the likelihood of being caught by police or having an accident was unlikely or very unlikely. 21
Another approach to studying how attitudes and perceptions contribute to impaired driving is to examine driving-related cognitions as distal risk factors for driving after use of substances. 22 Common driving-related cognitions include perceptions of the dangerousness of driving after substance use, perceived likelihood of experiencing negative consequences (e.g., being stopped by police, having an accident), and normative beliefs about peer acceptance of driving after substance use. Several studies of US adults who use cannabis have found that more favorable attitudes and risk perceptions are associated with increased quantity and frequency of DACU.23 –26 For example, McCarthy et. al. 26 found that lower perceived dangerousness, lower perceived likelihood of negative consequences, and greater peer acceptance were associated with increased engagement in DACU among US college students. Participants in McCarthy et. al.’s study 26 perceived DACU as more acceptable by their peers and potential negative consequences as less likely compared to driving after alcohol use. Arterberry et. al. 23 replicated many of these findings in another college sample but also showed that more favorable cognitions predicted the frequency of riding in a car with a driver who had been smoking cannabis. Similar associations between cognitive variables and DACU behaviors have been reported in other samples of US college students.24,27 In comparison, studies of community adults who use cannabis remain limited, 25 underscoring the need for replicating these findings outside of university samples.
Relative to studies of people who DACU and driving-related cognitions in the US, data on these same measures in people from Canada are notably lacking. In the study by Goodman et. al. 16 Canadian younger adults who rated DACU as less risky reported higher frequency of engagement in DACU. Despite these initial findings, understanding the risk perceptions of Canadians who DACU remains a priority area for research, 28 and no studies have directly compared US and Canadian samples. Comparing US and Canadian samples is scientifically important, given the rapidly shifting legal landscape concerning cannabis use in both countries. Differences in legalization also result in variability in public messaging, psychoeducation, and other prevention campaigns concerning cannabis risks and harms, including DACU. To further expand the US literature on DACU among community adults and add new data from Canadian community adults, the current study examined perceptions, driving behavior, and cannabis use among Canadian and US adults who reported recent cannabis use in the past six months.
Methods
Compliance, Ethical Standards, and Ethical Approval
This study was approved by the Institutional Review Board of the University of Kansas Human Research Protection Program (Project #3566; Study Title: Investigating Decision Making and Personality Correlates of Behavior) on August 18, 2017. All participants provided written informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Participants
The current study involved secondary data analyses from two larger studies on the behavioral economics of cannabis us.29,30 The data analyzed here are distinct from those of the previous publications.
Canadian Sample
Data were collected from the Canadian sample between November 2017 and February 2018. Recreational cannabis was illegal in Canada at the time of data collection; cannabis was legalized federally in October 2018. 3 Participants from the Canadian sample were recruited from the Population Assessment for Tomorrow’s Health registry maintained by the Peter Boris Centre for Addictions Research at McMaster University and from the Hamilton, Ontario, community using print and electronic advertisements. A study invitation was sent to participants in the registry or community participants who responded to study advertisements. Interested participants were invited to complete an initial online screening survey to verify their age (18 years or older) and self-reported use of cannabis in the past six months. Qualifying participants were sent a second email with a link for instructions to complete the survey for the study. Participants who completed the study received a $20 electronic gift card. The data collection period was limited to four months and a total of 158 participants were enrolled during this period (see Table 1 for sample characteristics).
Participant Characteristics, Driving-Related Cognitions, and Driving Behaviors.
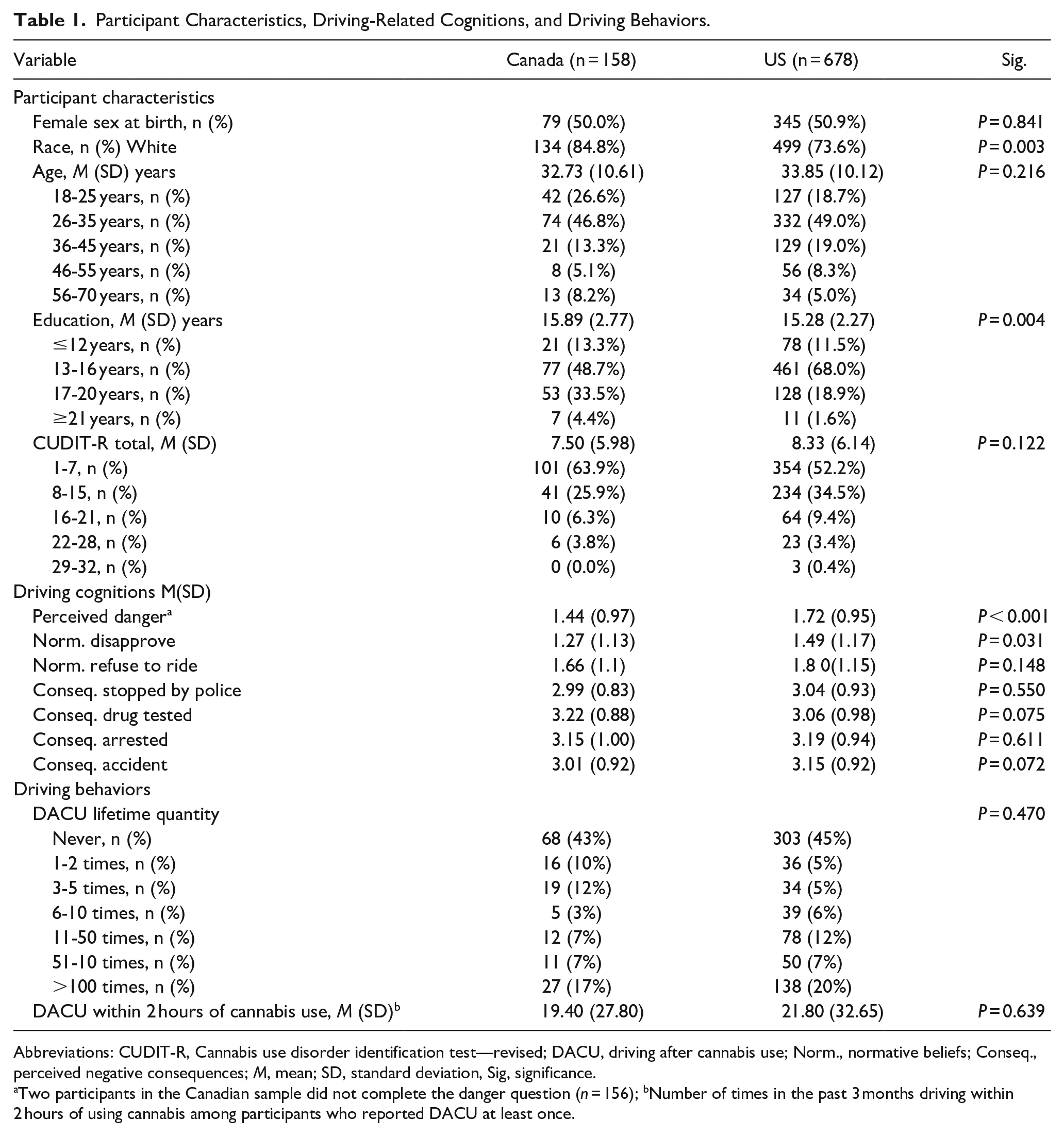
Abbreviations: CUDIT-R, Cannabis use disorder identification test—revised; DACU, driving after cannabis use; Norm., normative beliefs; Conseq., perceived negative consequences; M, mean; SD, standard deviation, Sig, significance.
Two participants in the Canadian sample did not complete the danger question (n = 156); bNumber of times in the past 3 months driving within 2 hours of using cannabis among participants who reported DACU at least once.
US Sample
The US sample was recruited through the Amazon Mechanical Turk (MTurk; www.mturk.com) online crowdsourcing platform from September 2017 to December 2017. Participants were required to have a minimum 95% approval rating on at least 100 previous MTurk surveys, and only one response per internet protocol (IP) address was allowed. A two-stage study design was utilized to reduce bias due to demand characteristics. 29 An initial general survey available to all MTurk workers included a few embedded cannabis questions. Participants who were aged 18 years or older and reported any cannabis use during the past six months were invited to complete the second stage. Participants received $2 for completing the screening survey and $5 for completing the second stage. A total of 678 participants completed the full study (see Table 1 for sample characteristics).
Measures
Study data for the Canadian sample were collected using the Research Electronic Data Capture (REDCap, https://projectredcap.org/resources/citations/).31,32 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources. Data for the US sample were collected using Qualtrics XM Survey Software (Provo, Utah, US). Prior to beginning the study, participants reviewed an information statement and provided electronic informed consent in REDCap or Qualtrics.
Demographics
Participants reported demographic information using a self-report questionnaire. Variables assessed differed slightly across samples, with common variables including age, sex assigned at birth, race (specific categories varied between the US and Canada), and education.
Cannabis Use
Participants reported their cannabis use and cannabis-related problems using the revised version of the Cannabis Use Disorders Identification Test (CUDIT-R). 33
Driving-Related Cognitions
Participants completed items assessing three domains of driving-related cognitions adapted from previous research on driving after cannabis and alcohol use.22,23,26 To permit comparisons between samples, the same wording was used for all cognition items. Consistent with prior studies,23,24,26 the term “marijuana” was used for these questions, and participants were instructed that “smoking marijuana” referred to any consumption of marijuana or cannabis. To align with the coding scheme used in previous studies, all driving cognition items were recoded such that higher values reflect greater acceptance or more favorable attitudes toward driving after marijuana use. The first domain assessed perceived dangerousness of driving after marijuana use. Participants used a four-point Likert scale to indicate how dangerous they thought it was to drive within two hours after smoking marijuana. Response options included: not at all dangerous (3), a little dangerous (2), somewhat dangerous (1), and very dangerous (0). Two participants in the Canadian sample did not complete the danger question. The second domain assessed normative beliefs about driving after marijuana use. Participants were asked how many (0-3) of their closest friends (1) would disapprove of driving while/after smoking marijuana and (2) would refuse to ride with someone who was driving while/after smoking marijuana. The third domain assessed perceived likelihood of negative consequences following driving after marijuana use. Participants responded to four items asking how likely they think a driver their age would be stopped by the police, drug tested, arrested, or have an accident from driving during or after smoking marijuana. These questions used a four-point Likert scale: not very likely (3), somewhat likely (2), likely (1), and very likely (0). An average score was generated across the four items.
Driving Behaviors
DACU was assessed using questions adapted from the previous research. 26 Participants were first asked if they had ever driven after smoking marijuana; participants who responded no were coded as never or zero for all subsequent items. Next, participants reported the number of times in the past three months they had driven “less than two hours after smoking marijuana.” In Addition, participants reported how many total times in their lives they have driven after smoking marijuana using a multiple-choice question with seven options ranging from never to over 100 times.
Data Analysis
Independent samples t-tests and chi-square tests were used to test for demographic differences between the Canadian and US samples. Differences in driving cognitions were examined using univariate analyses of variance, including partial η2 effect sizes. Spearman’s correlations were used to examine continuous associations among driving cognitions, driving behaviors, and cannabis use severity.
Results
The Canadian sample had a higher percentage of non-White participants (χ2 = 8.76, P = 0.003) and a higher total years of education (t(834) = 2.92, P = 0.004). However, the small difference in education (~0.6 years) was not considered practically significant. Cannabis use and problems assessed by the CUDIT-R did not significantly differ between the samples (P = 0.122). Driving behavior variables are presented in Table 1. The samples did not significantly differ on lifetime quantity of DACU (P = 0.470) or quantity of DACU within two hours of use in the past three months (P = 0.639).
Descriptive statistics for the driving cognitions variables are presented in Table 1 and frequency distributions for each variable are presented in Figure 1. For the driving cognition variables, Canadian participants perceived DACU as significantly more dangerous than US participants (F[1,832] = 11.23, P < 0.001, ηp2 = 0.013). Canadian participants also reported that more of their friends would disapprove of DACU (F[1,834] = 4.67, P = 0.031, ηp2 = 0.006), but did not differ from US participants on the number of friends who would refuse to ride with a driver who had been using marijuana (F[1,834] = 2.10, P = 0.148, ηp292; = 0.003). Finally, Canadian and US participants did not significantly differ in their ratings of the likelihood of being stopped by police, drug tested, arrested, or having an accident following DACU (Ps = 0.072-0.550).
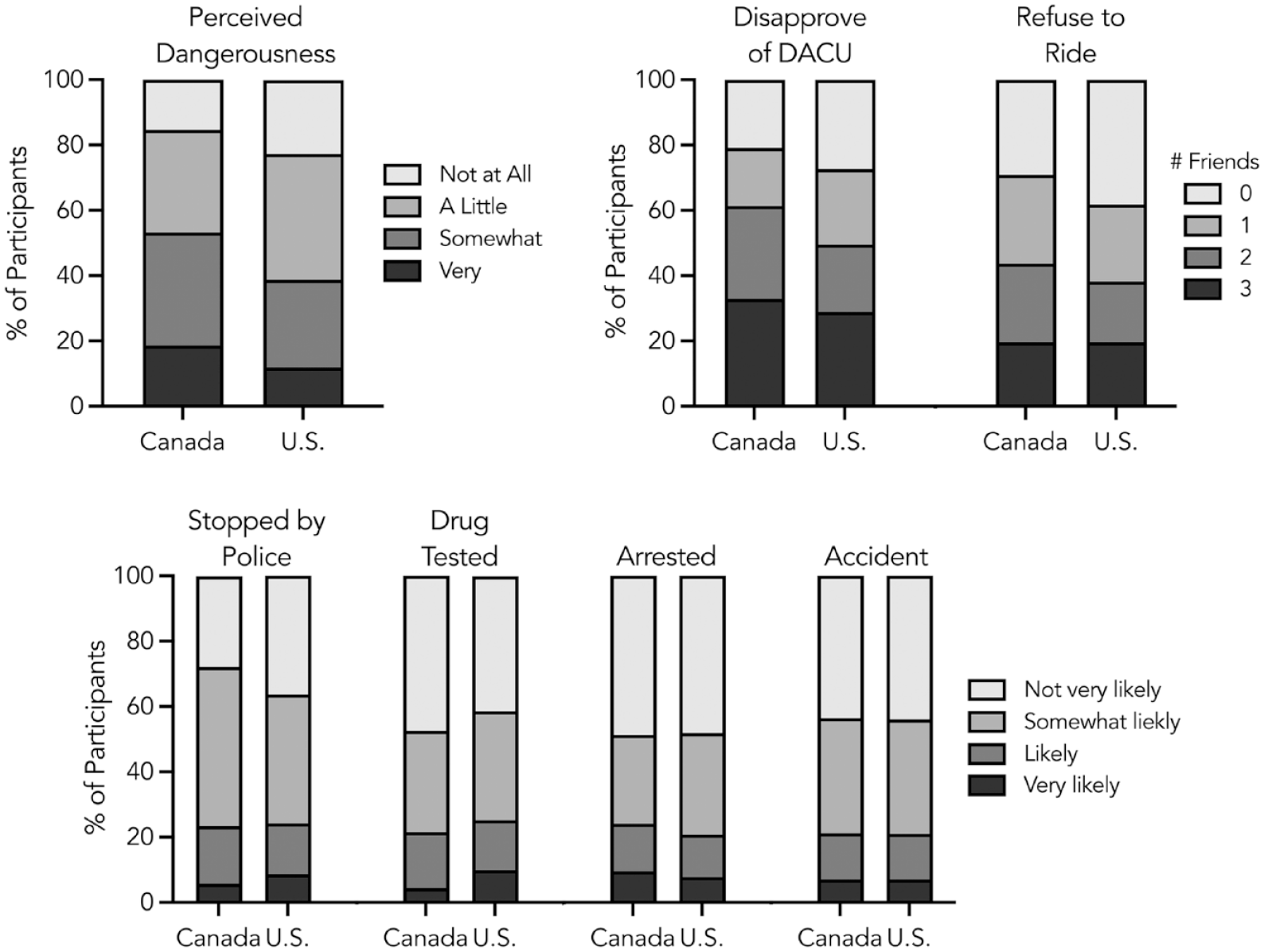
Responses to driving-related cognitions items among Canadian and US participants.
Spearman’s correlations are presented in Table 2. To reduce the number of variables, correlations were run using the mean ratings for normative beliefs and negative consequences.23,26 The driving variables were all significantly positively correlated with each other (ρ = 0.44-0.59, Ps < 0.01). Greater cannabis use severity measured by the CUDIT-R was positively correlated with more favorable driving cognitions and greater DACU quantity in lifetime and within two hours of use (ρ = 0.18-0.50, Ps < 0.01). Driving cognitions were also positively correlated with the frequency of engaging in DACU. Perceived dangerousness (ρ = 0.50-0.52, Ps < 0.01), normative beliefs (ρ = 0.47-0.53, Ps < 0.01), and perceived negative consequences (ρ = 0.37-0.41, Ps < 0.01) were correlated with lifetime reported instances of DACU. Similar associations were found for driving within two hours of use (see Table 2).
Spearman’s Correlations Between Driving-Related Cognitions and Driving Behavior.
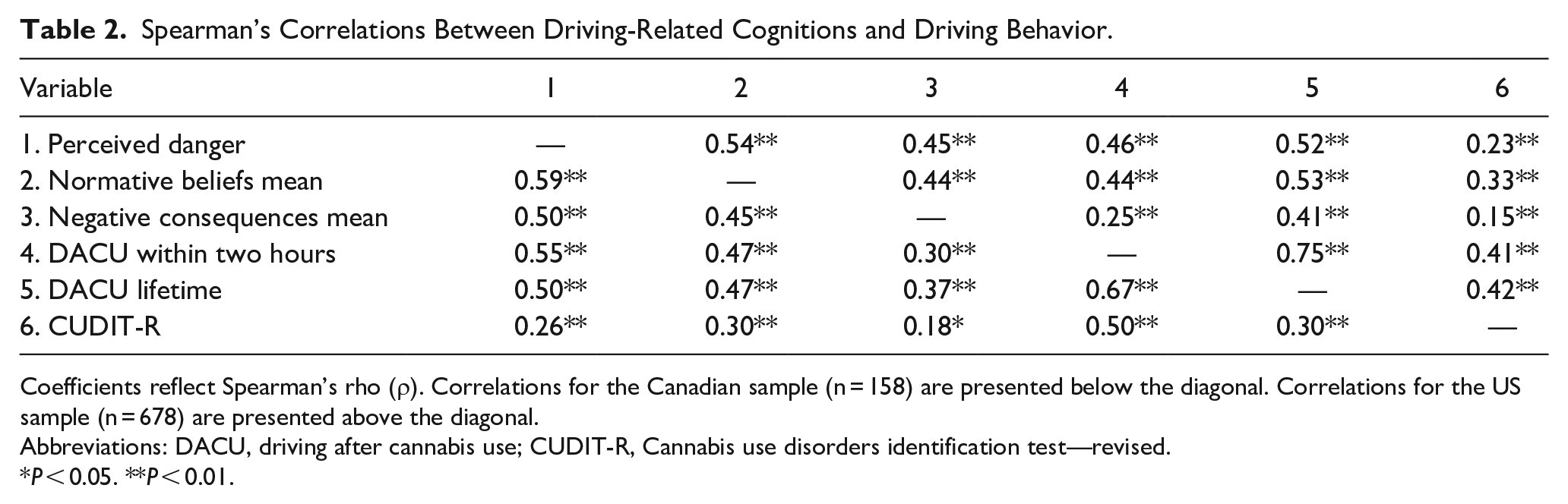
Coefficients reflect Spearman’s rho (ρ). Correlations for the Canadian sample (n = 158) are presented below the diagonal. Correlations for the US sample (n = 678) are presented above the diagonal.
Abbreviations: DACU, driving after cannabis use; CUDIT-R, Cannabis use disorders identification test—revised.
P < 0.05. **P < 0.01.
Discussion
The current study provides insights into the psychological correlates and driving behavior of people who engage in DACU in Canada and the US Canadian participants perceived DACU as more dangerous than US participants and they reported more friends who would disapprove of DACU. However, their beliefs about the number of friends who would refuse to ride with a driver who had been using cannabis and the perceived likelihood of experiencing negative consequences did not significantly differ from the US sample. Results of the correlation analyses indicated that more favorable cognitions were associated with greater lifetime and recent quantity of DACU. Collectively, these results are consistent with previous studies focused on US samples.23,25 –27
The findings from the Canadian sample make a unique and important contribution to the literature on DACU. The only published study to date to examine risk perceptions related to DACU among Canadians 16 included survey questions that are conceptually related to the cognition items used here. Specifically, participants were asked to rate the extent to which cannabis increases the risk of getting into an accident and how likely it is that a driver would be stopped by police or charged. Those items are most closely aligned with the perceived negative consequences ratings in the current study, although differences in question wording and response options complicate direct comparisons. For instance, only 8% of Canadians in the current study reported that an accident was “very likely,” compared to 39% of participants in Goodman et al.’s study, 16 who responded that DACU increases accident risk by “a lot.” On the other end, 34% of Canadians in the current study responded that an accident was “not very likely,” compared to only 5% who responded “not at all” in Goodman et. al.’s study. 16 Ratings for being stopped by police were more comparable (i.e., 7%-8% of participants in the two studies said it was “very likely/extremely likely” and 14%-18% said it was “likely”). Despite the similarities in likelihood of being stopped by the police, the participants in Goodman et al.’s study 16 believed it was more likely that a driver would be charged compared to the ratings of likelihood of being arrested in the current study.
Apart from the differences in specific questions and response options, heterogeneity in participant samples in Goodman et al.’s study and our study may explain some of these differences. One potential explanation for why the current Canadian participants reported a lower likelihood of accidents is that the current study focused exclusively on people who reported cannabis use in the past six months, while Goodman et. al. 16 surveyed a general sample of young adults (42% of their sample reported never using cannabis). Overall rates of engagement in DACU also differed between studies. Approximately 80% of the participants in Goodman et. al.’s study 34 reported never driving within two hours of use, whereas only 57% of the current sample reported never doing so. Participants in the current study were also older, on average, than in Goodman et. al.’s study 34 (i.e., 49% of the current Canadian participants were above the age of 30 years, the upper age limit in Goodman et. al.’s). It is possible that the current Canadian participants had more life experiences with DACU—and doing so without experiencing any consequences—thereby reducing their risk perceptions due to confirmation bias. Unfortunately, we do not have data on actual experiences of negative consequences to empirically test this hypothesis.
The second contribution of this study is the direct comparison of DACU cognitions and behaviors between the US and another country. Although there were some differences in the survey methodology and recruitment approaches between the samples, identical items were used to assess driving cognitions and DACU behavior. The ratings for perceived danger suggested that Canadians had more risk-averse attitudes/perceptions toward DACU. Roughly 19% of Canadians rated DACU as “very dangerous,” compared to 12% of US participants. At the other end of the rating scale, 23% of US drivers viewed DACU as “not at all dangerous,” compared to only 15% of Canadians. The differences between the Canadian and US participants are intriguing because they are not due to greater cannabis use in the US participants (i.e., the groups did not significantly differ in total CUDIT-R score). Differences in perceived danger among Canadians did not appear to correspond to the differences in self-reported quantity and frequency of engaging in DACU, at least not at the level of group means. The two samples reported comparable lifetime DACU and number of times driving within two hours of using cannabis in the past six months. At the individual level, participants from both countries who perceived DACU as less dangerous, more socially acceptable, and less likely to lead to consequences reported higher quantity. A possible explanation for the differences in driving-related cognitions could be differences in geographic distribution of the participants. Participants on MTurk were recruited from across the US, whereas the Canadian participants were drawn from a single metropolitan area in southern Ontario (see below for a discussion of how prevention efforts in Ontario may have influenced risk perceptions and attitudes). Ultimately, the scope of this research did not permit us to consider other factors that may have explained the differences between countries such as personality factors, substance use motives, or other measures of decision-making. Studies on driving after alcohol use have reported that these factors influence driving cognitions and driving behaviors eg, 35,36 but this remains an open question in the context of DACU.
These findings may have implications for prevention and intervention efforts that specifically target driving perceptions or attitudes to reduce engagement in DACU.37,38 Prevention efforts aiming to reduce substance-impaired driving commonly target perceptions and beliefs about negative consequences. 39 Federal and provincial governments in Canada have emphasized increased risk of accidents, injuries, or fatalities associated with DACU in various guidelines and public messaging. However, these messages have not always focused on risky attitudes or social acceptance among people who use cannabis. For example, the Canadian Lower Risk Cannabis Use Guidelines 40 discuss increased risks of DACU but mostly focus on psychological and behavioral impairments associated with cannabis use as well as legal detection thresholds. Public messaging around cannabis and driving from the Province of Ontario addressed the perceived danger more directly by stating, “Driving a vehicle while you’re impaired by cannabis is illegal and dangerous. . . You are not a safer driver when you’re high.” 41 Ontario also made these messages more visible at the point of sale for legalized cannabis outlets. The Ontario Cannabis Store—the Government of Ontario’s online cannabis dispensary—includes an informational page on cannabis and driving as part of their Cannabis Made Clear series. 42 Specifically, the Ontario Cannabis Store page states, “Driving after consuming cannabis is both dangerous and illegal.” Our results suggest that designing messaging around peer norms and social disapproval of DACU may complement these safety-focused messages.
While there is mixed evidence to support the efficacy of messaging focused on peer norms, some research suggests that messaging focused on peer norms has been associated with safer decision-making, less harmful alcohol use, and engagement in other healthy behaviors when the messaging has been implemented effectively.43 –46. In the case of impaired driving, one study evaluated a statewide social norm marketing campaign in Montana that was designed to reduce drinking and driving behavior. 47 This study found that messaging focused on peer norms was associated with small but significant increases in the rate of designated driver use and decreased rates of drinking and driving in young adults when messaging reached the target audience. We are not aware of any studies implementing social norm interventions to address DACU. Thus, more research is needed to evaluate whether psychoeducation messages focusing on social norms or other driving-related cognitions are effective in reducing the prevalence of DACU.
There are several limitations to consider when interpreting these results. The most important considerations are related to the sample sizes and representativeness of the participants. The Canadian sample was a convenience sample recruited from a hospital research registry and from the community over a relatively short enrollment time window. Accordingly, the sample size is relatively small. Although the Canadian sample was balanced by sex assigned at birth and had sufficient variability in terms of age and education level, most participants (84%) reported their race as White. Participants also were recruited from a single city in one Canadian province (Ontario). These demographic characteristics and geographic constraints likely limit the generalizability of these findings to the broader population of Canadian adults who use cannabis. However, data from the 2017 wave of the nationally representative Canadian Cannabis Survey 48 —the same year that the current Canadian data were collected—indicated that among adults who reported cannabis use in the past year, 50% reported that cannabis affects driving and 19% reported it had no effect on driving. This is comparable to the current study, where 53% of the Canadian participants reported that driving within two hours of cannabis use was either “somewhat” or “very” dangerous, while comparatively fewer participants (15.4%) reported it was “not at all” dangerous. Concerns about representativeness also apply to the US MTurk sample. Unfortunately, we are not aware of comparable nationally representative data on US adults’ attitudes related to impaired driving. However, our participant demographics (i.e., age, sex at birth, and race) are generally consistent with published studies and other reports on the demographic characteristics of MTurk workers.49,50
Beyond sample characteristics, it is important to note that these data are cross-sectional and were collected in 2017-2018 prior to federal legalization of cannabis in Canada and at a time when a smaller number of US states had legalized medical or recreational cannabis. Therefore, these data are outdated and may not reflect the current perceptions and attitudes of people who DACU in Canada and the US. It is worth noting that the only published data from the Canadian sample 34 also collected pre-legalization data at the same time as the current data (October 2017). Future research is needed to replicate these findings in a post-legalization sample of Canadians to understand if these perceptions, attitudes, and behaviors have shifted. A final limitation of the US MTurk sample that was emphasized in the first article using these data 29 is that the survey did not include explicit attention check items to screen for automated or low-effort responding. Although front-end qualifications were employed (i.e., minimum number of previous MTurk submissions, approval ratings, and IP address tracking), these may not be sufficient to ensure data integrity. Although multi-stage attention checks and data screening are now considered best practice standards in crowdsourcing,51,52 the current data were collected at a time when the full extent of the data integrity issues with crowdsourcing was not well understood. Interpretations of the MTurk results should be made with appropriate caution.
The findings of the present study affirm previous research that suggests that when people endorse favorable perceptions of DACU, they are more likely to engage in DACU. While this association has been studied in the US, this study expands on this subject by providing novel insights into DACU cognitions and behaviors of Canadians, although updated research with contemporary samples is needed to determine if these perceptions and attitudes have changed with expanded access to cannabis following federal legalization. Informed by an understanding of the perceptions and attitudes of people who DACU, tailored prevention and treatment efforts aimed at the people most likely to engage in this behavior can be made to promote safe decision-making concerning driving.
Footnotes
Acknowledgements
The authors are grateful to the staff and trainees of the Peter Boris Centre for Addictions Research at McMaster University for their contributions to data collection. We also thank Dr. James MacKillop for contributions to the design of the studies from which these data were obtained. Finally, we are grateful to the family of Patrick Guthrie for supporting postsecondary addiction research at the University of Kansas. The generous support of the Patrick Guthrie Hawks for Hope Fund enabled William Davis to contribute to the current research.
Author Contributions
MA originated the project and collected the data. WJD, BPM, and MA conducted the analyses and interpreted the findings. All authors participated in interpreting the results, contributed to the writing of the article, provided critical feedback to the article, and approved the final article draft for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Cofrin Logan Center for Addiction Research and Treatment at the University of Kansas, the Peter Boris Centre for Addictions Research at McMaster University, and the Michael G. DeGroote Centre for Medicinal Cannabis Research at McMaster University. William Davis was supported by the Patrick Guthrie Hawks for Hope Fund at the University of Kansas. Supporting organizations had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Compliance,Ethical Standards,and Ethical Approval
This study was approved by the Institutional Review Board of the University of Kansas Human Research Protection Program (Project #3566; Study Title: Investigating Decision Making and Personality Correlates of Behavior) on August 18, 2017. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.