
Abstract
Introduction:
Despite the high cannabis use rates among sexual minority (SM) individuals, less research has examined factors related to cannabis use among SM (vs. heterosexual) individuals, especially in places with legal medical cannabis retail markets and high structural stigma, like Oklahoma.
Methods:
Data were from a survey of Oklahoma adults, including 3020 females (18.6% SM) and 2279 males (10.1% SM). Bivariate analyses examined associations of sexual identity with cannabis-related factors (i.e., perceived harm, positive attitudes, marketing exposure, depressive symptoms, anxiety symptoms) and cannabis use and use severity (i.e., past 30-day use, daily/near-daily use, cannabis use disorder [CUD] symptoms). Logistic regression examined associations of sexual identity and cannabis-related factors with cannabis use and use severity among females and males, separately.
Results:
SM (vs. heterosexual) females reported greater odds of past 30-day cannabis use and daily/near-daily use, lower harm perceptions, greater marketing exposure, and higher rates of depressive/anxiety symptoms. Lower harm perceptions and greater marketing exposure were associated with greater odds of past 30-day use, whereas marketing exposure was associated with greater odds of daily/near-daily use. SM (vs. heterosexual) males reported greater odds of daily/near-daily use and higher rates of depressive/anxiety symptoms.
Conclusions:
SM (vs. heterosexual) females reported higher rates of cannabis use, whereas SM (vs. heterosexual) females and males reported higher rates of daily/near-daily cannabis use. Potential targets for cannabis-related health campaigns aimed at reducing use differences include correcting misinterpretations of harm that may emanate from cannabis marketing efforts among females and addressing depressive symptoms among males.
Highlights
Sexual minority (vs. heterosexual) females displayed greater odds of any past 30-day cannabis use.
Sexual minority (vs. heterosexual) females and males displayed greater odds of daily/near-daily cannabis use.
Among sexual minority females, findings may be related to cannabis marketing exposure and harm perceptions.
Among sexual minority males, findings may be related to depressive symptoms.
Introduction
Cannabis is the most commonly used federally illicit substance among US adults, with current use rates doubling from 7% in 2013 to 16% in 2022. 1 Although cannabis may have medical utility when used appropriately (e.g., treating chronic pain), 2 unintended public health consequences may occur. Cannabis use (defined as any cannabis use, more frequent cannabis use, or cannabis use disorder [CUD] across studies) is associated with motor vehicle crashes, mental health problems, and use of other substances (e.g., tobacco, alcohol).2,3 Moreover, individuals may develop CUD, which has behavioral, social, and psychological ramifications.4,5
Certain minoritized individuals, including those identifying as a sexual minority (SM; i.e., gay/lesbian, bisexual, or another nonheterosexual identity) person, display higher rates of cannabis use relative to heterosexual individuals.6 -12 In 2018, 37.6% of SM adults reported past-year cannabis use, relative to 16.2% of heterosexual adults.13,14 Some findings suggest important differences in cannabis use with regard to sex (i.e., sex assigned at birth)9,15 and gender (i.e., current gender identity), 16 with the association between sexual identity and any past 30-day cannabis use being stronger for females9,15 and women 16 relative to males9,15 and men. 16 SM individuals also are more likely to meet criteria for CUD (i.e., continued use of cannabis despite significant impairment 17 ) 10 and are more likely to engage in daily cannabis use 8 relative to heterosexual individuals.
The prevailing explanation for substance use differences among SM, relative to heterosexual people is based on Minority Stress Theory, which suggests that SM individuals face stressors (e.g., discrimination) as a result of the stigmatization of their minoritized sexual identity.18,19 This stress is theorized to increase mental health symptoms (e.g., depression, anxiety) and deplete coping resources, which may lead to increased coping-related substance use. 20 A growing body of literature has linked SM stressors (e.g., discrimination,21,22 structural stigma, 23 social rejection 24 ) to differences in past-year cannabis use, 23 past 30-day use,24,25 and higher CUD rates.21,22
Research is sparse regarding other factors that may contribute to cannabis use among SM individuals. Cannabis-related perceptions (e.g., perceived harm to health) and marketing exposure may also contribute to cannabis use differences. SM (vs. heterosexual) individuals report lower levels of perceived harm to health related to cannabis use, 26 which is related to a greater likelihood of past 30-day cannabis use among adults, broadly.27 -33 Regarding cannabis marketing exposure, research has primarily focused on adolescents and young adults and suggests that SM individuals report greater exposure to cannabis marketing (via magazine/newspaper, storefront, online, billboards/signs), but this work did not assess the role of exposure on cannabis use.34,35 However, cannabis marketing exposure is associated with increased odds of current cannabis use among individuals, generally.36 -41
Cannabis use may be especially prevalent among SM individuals residing in Oklahoma, where there is greater stigma toward SM individuals, potentially leading to greater mental health symptoms and in turn, cannabis use. 42 Moreover, Oklahoma legalized medical cannabis in 2018 and has the second-most cannabis dispensaries per capita relative to any other state. 43 Thus, SM individuals residing in Oklahoma may be commonly exposed to cannabis marketing and have positive perceptions regarding cannabis (which is associated with greater marketing exposure 44 ), further contributing to elevated rates of cannabis use.
Although elevated rates of cannabis use among SM individuals are evident, less is known about the range of factors that may be associated with cannabis use and use severity among SM, relative to heterosexual adults. Moreover, research on SM cannabis use is lacking in places with legal cannabis retail markets, high structural stigma, and pronounced SM substance use, like Oklahoma.45,46 This work is critical to inform public health efforts aimed at reducing cannabis use among this vulnerable population, particularly as further cannabis legalization across the United States is likely. 47 To identify factors associated with differences in cannabis use among SM versus heterosexual individuals, the current study examined associations between sexual identity and potential cannabis-related factors (i.e., perceived harm to health, positive cannabis perceptions, cannabis marketing exposure, depressive symptoms, anxiety symptoms). We then examined associations of sexual identity and these cannabis-related factors with cannabis use and use severity (i.e., any past 30-day use, daily/near-daily use, CUD symptoms). Based on the aforementioned literature, we hypothesized that SM (vs. heterosexual) individuals would display greater odds for current cannabis use, daily/near-daily cannabis use, and CUD symptoms. Moreover, SM (vs. heterosexual) individuals were expected to report lower cannabis-related harm perceptions and greater positive attitudes toward cannabis; a greater proportion of SM individuals was expected to report cannabis marketing exposure, depressive symptoms, and anxiety symptoms. Lower harm perceptions, greater positive attitudes, marketing exposure, and depressive and anxiety symptoms were hypothesized to predict greater odds of each cannabis-related outcome.
Methods
Participants and Procedures
Participants were adults (≥18 years old) living in Oklahoma (verified by self-reported zip code). Potentially eligible individuals in the Lucid Marketplace were sent a study invitation, and those who passed the initial screening and provided consent were eligible to complete the survey. A total of 5394 participants completed the survey. The sample was closely aligned with the racial and ethnic demographics of Oklahoma (i.e., 75.3% White, 8.9% Black, 0.4% Native Hawaiian or Pacific Islander, 8.4% American Indian or Alaskan Native, 5.6% more than one race, 9.5% Hispanic). 48 There was a higher proportion of female participants relative to the state population (56.8% vs. 50.1%). 48 The median household income of study participants was $30 000 to $39 999, compared with a median income of $56,956 among Oklahomans, and 92.7% of participants reported completing high school/GED, compared with 88.7% of Oklahomans. 48 Participants were compensated based on incentives provided by the panel to which they belonged (e.g., cash, gift cards, points to redeem reward prizes or gift cards; equating to roughly $1). Our final analytic sample included 5299 adults with data on sexual identity. Procedures were approved by the Site University of Oklahoma Health Sciences Center IRB.
Measures
Covariates
Participants reported their age, race (White, Black/African American, Asian, Native Hawaiian/Other Pacific Islander, American Indian/Alaskan Native, more than one race), ethnicity, income (≤$19,999, $20,000-$39,999, $40,000-$59,999, $60,000-$79,999, $80,000-$99,999, ≥$100,000), employment status (full time, part-time, unemployed and looking for work, unemployed and not looking for work, homemaker, student, retired, unable to work or disabled, other), education (less than bachelor’s degree and more than bachelor’s degree), health insurance (i.e., Medicare, Medicaid, Military/Veteran’s, private, no insurance), and whether they had a medical cannabis license (yes/no) issued by the Oklahoma Medical Marijuana Authority. Age at first cannabis use was assessed by asking participants to indicate their age when they first tried cannabis.
Sexual Identity by Sex Subgroup
Participants were asked, “Do you consider yourself: straight/heterosexual, lesbian or gay, bisexual, transgender, another sexual identity, questioning, queer, don’t know/not sure, refuse to answer?” The transgender response option was excluded from analyses due to the small sample size (n = 4 females, n = 6 males) and because it was included only at Wave 1. Participants who declined to report their sexual identity (n = 3 females, n = 4 males) were coded as missing and excluded from the analyses. Participants were categorized as straight/heterosexual or SM (lesbian/gay, bisexual, another sexual identity, questioning, queer, do not know/not sure aggregated). Regarding sex, participants were asked, “What is your biological sex: male, female?”
Cannabis-Related Factors
Participants reported on cannabis-related perceptions, cannabis marketing exposure, and mental health symptoms. Cannabis harm perceptions were assessed by asking, “How much do you think people harm themselves when they use cannabis?” on a 4-point scale (1 = no harm to 4 = a lot of harm). Positive attitudes toward cannabis use were assessed with 3 items: (1) cannabis is not addictive; (2) cannabis is safer to use than prescribed pain medications; and (3) cannabis is an effective treatment for general health conditions, on a 5-point scale (0 = strongly disagree to 4 = strongly agree; α = 0.80). Responses were averaged with higher scores indicating more positive attitudes.
To assess cannabis marketing exposure, participants were asked whether they saw each of the following in the past 30 days: (1) ads or promotions (e.g., billboards, posters) for a cannabis dispensary; (2) social media user-generated content related to cannabis products; (3) ads or promotions for cannabis products or dispensaries when reading a newspaper or magazine; and (4) ads or promotions for cannabis products when using the Internet (α = 0.74). Participants were classified as reporting any (vs. no) cannabis marketing exposure in the past 30 days if they endorsed seeing at least one marketing source.
Participants completed the Patient Health Questionnaire (PHQ-2), 49 which includes two items assessing depressive symptoms and the Generalized Anxiety Disorder (GAD-2) Questionnaire, 50 which includes 2 items assessing anxiety symptoms. Participants were asked, “Over the last 2 weeks, how often have you been bothered by the following problems: little interest of pleasure in doing things; feeling down, depressed, or hopeless; feeling nervous, anxious, or on edge; and not being able to stop or control worrying” on a four-point scale (1 = not at all to 4 = nearly every day). Responses to the first two items were summed to create a total depressive symptoms (α = 0.84) score, and responses to the last two items were summed to create a total anxiety symptoms (α = 0.88) score. Individuals who received a score at or above the cutoff (≥3) were coded as experiencing depressive or anxiety symptoms, respectively.
Cannabis Use and Use Severity
Participants indicated the number of days they used cannabis in the past 30 days (0-30). Those who reported using ≥1 day were classified as having used cannabis in the past 30 days. Among those who reported past 30-day cannabis use, we created a variable indicating daily/near-daily cannabis use (yes/no to using ≥20 of the past 30 days). 51 Participants who reported past 30-day use completed the three-item Cannabis Use Disorder Identification Test—Short form (CUDIT-SF) to assess CUD symptoms (α = 0.76). 17 CUDIT-SF scores range from 0 to 12 with scores ≥2 indicating a positive screen for CUD and <2 indicating a negative screen.
Data Analysis
Analyses were conducted among females (n = 3,020) and males (n = 2,279) separately using SPSS v29 (Released 2022; IBM Corp.). Bivariate analyses (i.e., chi-square tests, independent samples t-tests) examined associations between sexual identity and covariates (i.e., age, race/ethnicity, income, employment, education, health insurance, medical cannabis license, age at first cannabis use), cannabis-related factors (i.e., cannabis harm perceptions, positive attitudes, cannabis marketing exposure, mental health symptoms), and cannabis use and use severity (i.e., past 30-day cannabis use, daily/near-daily use, CUD symptoms). Crude (i.e., including sexual identity only) and adjusted (i.e., including sexual identity, cannabis-related factors, and covariates) logistic regression models examined associations of sexual identity and cannabis-related factors with odds of: (1) past 30-day cannabis use; (2) daily/near-daily cannabis use; and (3) CUD symptoms, controlling for sociodemographic variables (selected based on prior literature2,44,52 -57 and preliminary analyses indicating associations between selected covariates and outcome variables at P < 0.05). Thus, three crude and three adjusted multinomial logistic regression models were run for females and males, respectively. Missing data comprised ≤5% of all analyses; participants with missing data were excluded from analyses (Little’s test for missingness completely at random: Ps > 0.05).
Results
Cannabis-Related Factors and Cannabis Use Among Females
Among females, 18.6% identified as SM, 81.4% as heterosexual, and 33.5% reported past 30-day cannabis use (Table 1). A greater percentage of SM (vs. heterosexual) females were younger, racially and ethnically diverse (i.e., non-Hispanic other race, Hispanic), reported lower income (i.e., less than $20 000), were unemployed, uninsured, and had a medical cannabis license. A lower percentage of SM females reported having at least a bachelor’s degree. Additionally, SM females initiated cannabis use at a younger age. In terms of cannabis-related factors, SM (vs. heterosexual) females reported lower cannabis harm perceptions. A greater percentage of SM (vs. heterosexual) females reported cannabis marketing exposure, depressive symptoms, anxiety symptoms, past 30-day cannabis use and daily/near-daily cannabis use.
Participant Characteristics and Bivariate Analyses Examining Differences Between Females Identifying as Sexual Minority Versus Heterosexual, N = 3020.
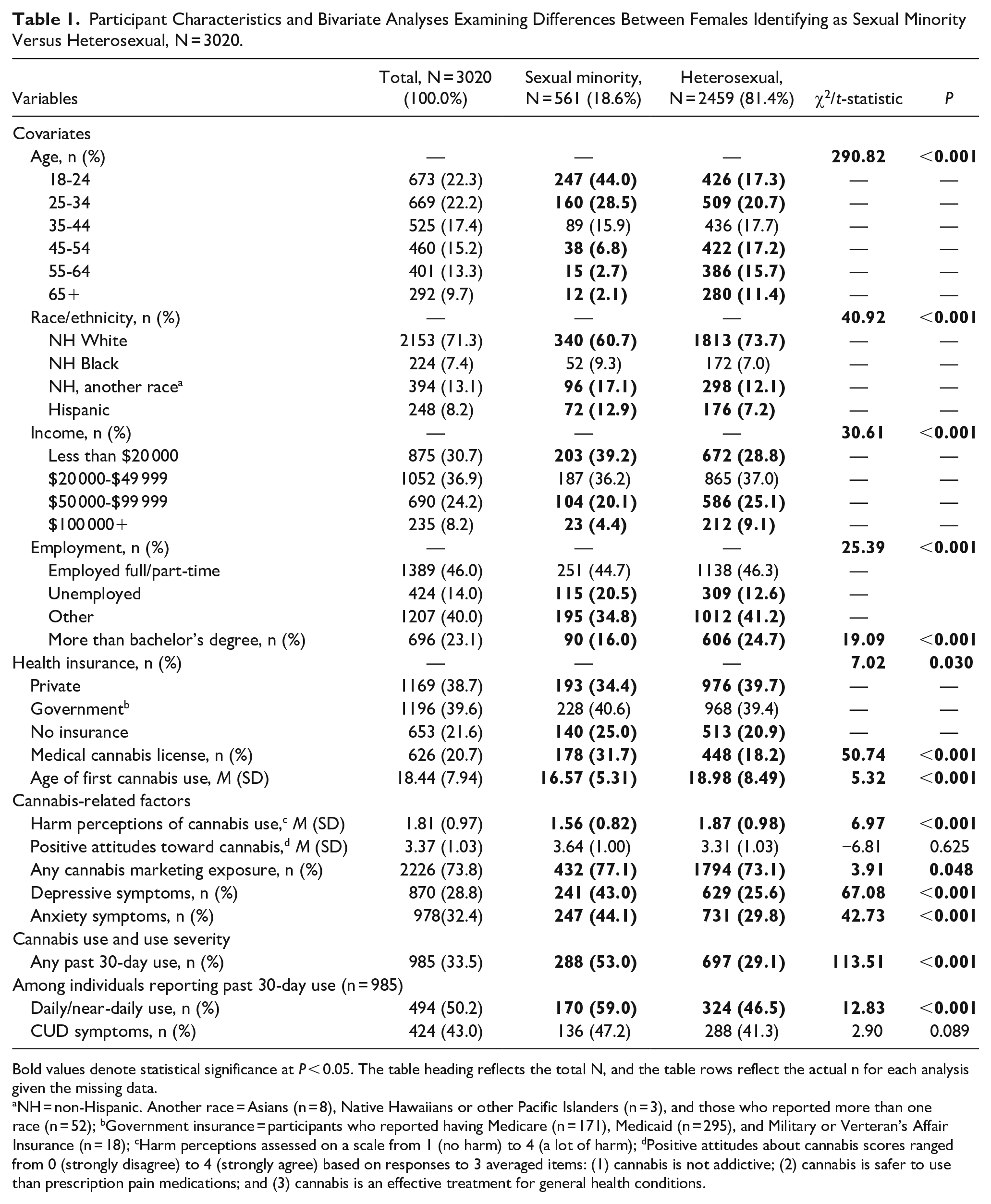
Bold values denote statistical significance at P < 0.05. The table heading reflects the total N, and the table rows reflect the actual n for each analysis given the missing data.
NH = non-Hispanic. Another race = Asians (n = 8), Native Hawaiians or other Pacific Islanders (n = 3), and those who reported more than one race (n = 52); bGovernment insurance = participants who reported having Medicare (n = 171), Medicaid (n = 295), and Military or Verteran’s Affair Insurance (n = 18); cHarm perceptions assessed on a scale from 1 (no harm) to 4 (a lot of harm); dPositive attitudes about cannabis scores ranged from 0 (strongly disagree) to 4 (strongly agree) based on responses to 3 averaged items: (1) cannabis is not addictive; (2) cannabis is safer to use than prescription pain medications; and (3) cannabis is an effective treatment for general health conditions.
Multivariable logistic regression examining associations among SM status and past 30-day cannabis use, daily/near-daily cannabis use, and CUD symptoms adjusting for sociodemographic covariates are presented in Table 2. SM (vs. heterosexual) females reported greater odds of past 30-day cannabis use and daily/near-daily use, in both crude and adjusted models. Lower harm perceptions, greater positive attitudes toward cannabis, and cannabis marketing exposure were associated with greater odds of past 30-day use. Positive attitudes toward cannabis and cannabis marketing exposure were associated with greater odds of daily/near-daily use. Only greater perceived harm of cannabis use was associated with greater odds of CUD symptoms.
Crude and Adjusted Odds Ratios Predicting Any Past 30-Day Cannabis Use (Among All Females [N = 3020]), Daily/Near-Daily Cannabis Use, and CUD Symptoms (Among Females [N = 985] Who Reported Past 30-Day Cannabis Use).
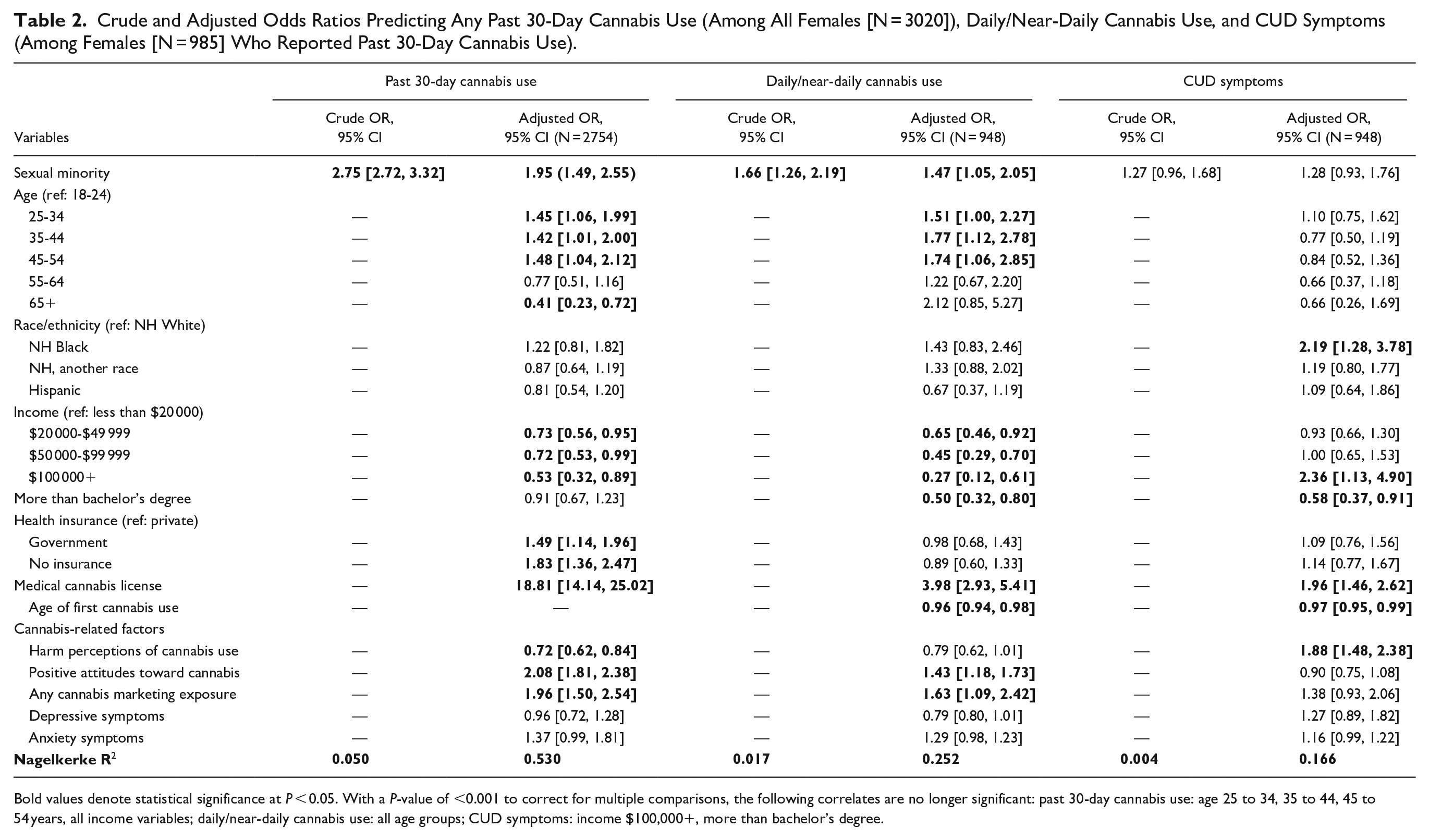
Bold values denote statistical significance at P < 0.05. With a P-value of <0.001 to correct for multiple comparisons, the following correlates are no longer significant: past 30-day cannabis use: age 25 to 34, 35 to 44, 45 to 54 years, all income variables; daily/near-daily cannabis use: all age groups; CUD symptoms: income $100,000+, more than bachelor’s degree.
Cannabis-Related Factors and Cannabis Use Among Males
Among males, 10.1% identified as SM, 89.9% as heterosexual, and 36.2% reported past 30-day cannabis use (Table 3). A greater percentage of SM (vs. heterosexual) males were younger, reported lower income (i.e., less than $20 000), and were unemployed. A lower percentage of SM males reported having at least a bachelor’s degree. Additionally, a greater percentage of SM (vs. heterosexual) males reported depressive and anxiety symptoms, past 30-day cannabis use, and daily/near-daily cannabis use.
Participant Characteristics and Bivariate Analyses Examining Differences Between Males Identifying as Sexual Minority Versus Heterosexual, n = 2279.
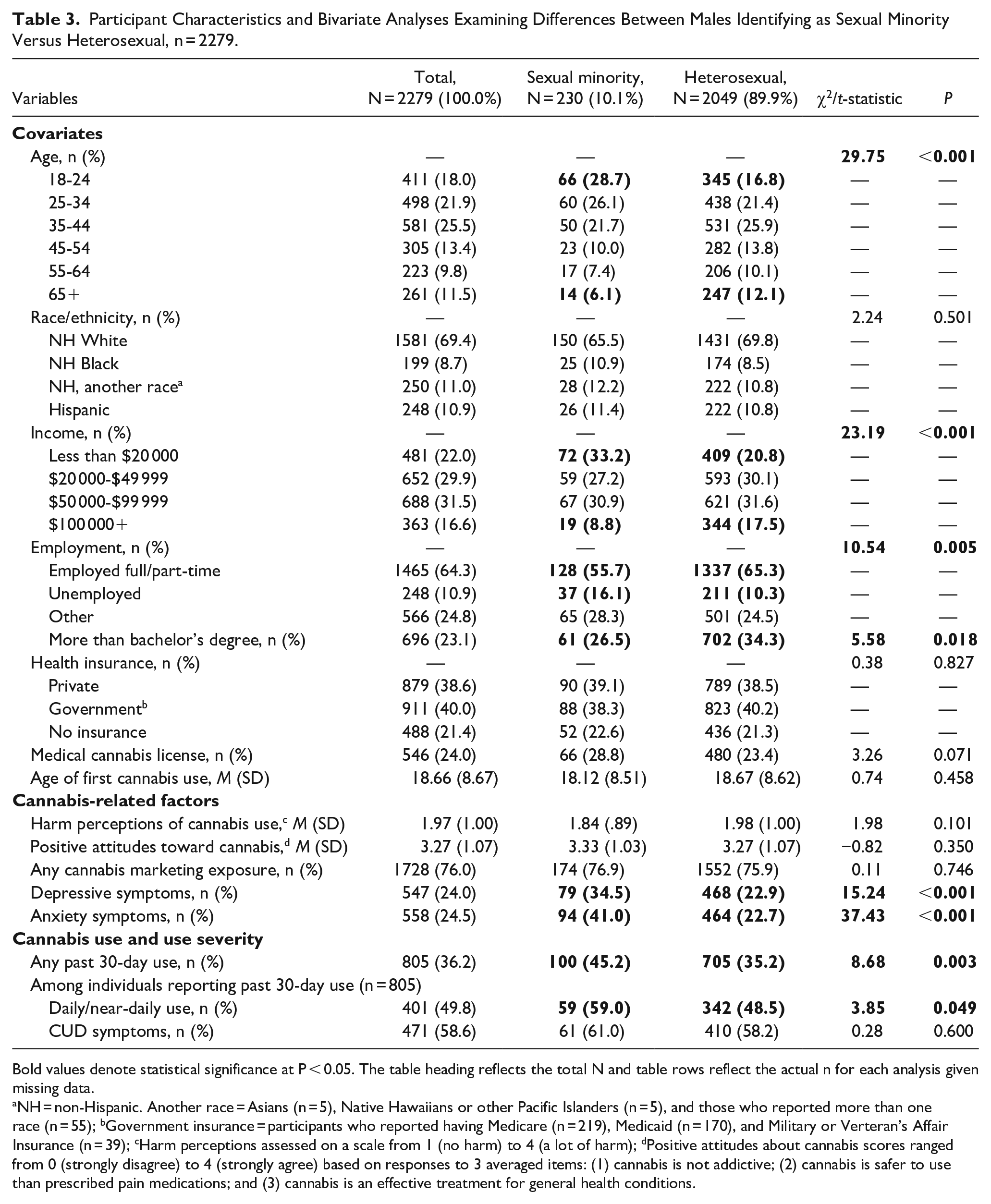
Bold values denote statistical significance at P < 0.05. The table heading reflects the total N and table rows reflect the actual n for each analysis given missing data.
NH = non-Hispanic. Another race = Asians (n = 5), Native Hawaiians or other Pacific Islanders (n = 5), and those who reported more than one race (n = 55); bGovernment insurance = participants who reported having Medicare (n = 219), Medicaid (n = 170), and Military or Verteran’s Affair Insurance (n = 39); cHarm perceptions assessed on a scale from 1 (no harm) to 4 (a lot of harm); dPositive attitudes about cannabis scores ranged from 0 (strongly disagree) to 4 (strongly agree) based on responses to 3 averaged items: (1) cannabis is not addictive; (2) cannabis is safer to use than prescribed pain medications; and (3) cannabis is an effective treatment for general health conditions.
Multivariable logistic regression (Table 4) indicated that sexual identity was not associated with any past 30-day cannabis use after adjusting for covariates. However, greater positive attitudes toward cannabis, cannabis marketing exposure, depressive symptoms, and lower harm perceptions predicted greater odds of past 30-day use. SM males displayed greater odds of daily/near-daily cannabis use in both crude and adjusted models. Positive attitudes toward cannabis and lower harm perceptions predicted greater odds of daily/near-daily use. Greater harm perceptions, depressive symptoms, and anxiety symptoms predicted greater odds of CUD symptoms, whereas positive attitudes toward cannabis predicted lower odds of CUD symptoms.
Crude and Adjusted Odds Ratios Predicting Any Past 30-Day Cannabis Use (Among All Males [N = 2,279]), Daily/Near-Daily Cannabis Use, and CUD Symptoms (Among Males [N = 805] Who Reported Past 30-Day Cannabis Use).
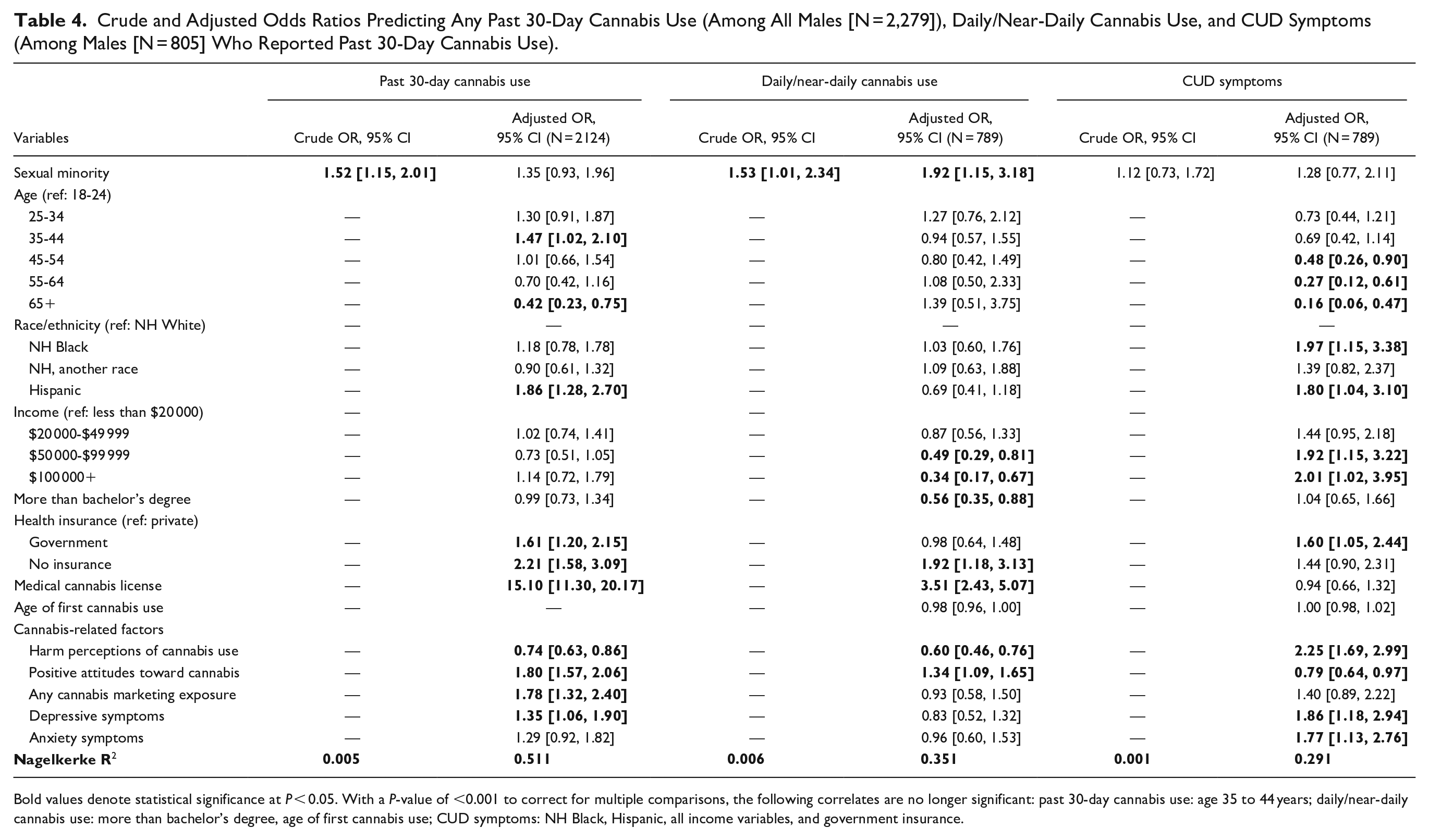
Bold values denote statistical significance at P < 0.05. With a P-value of <0.001 to correct for multiple comparisons, the following correlates are no longer significant: past 30-day cannabis use: age 35 to 44 years; daily/near-daily cannabis use: more than bachelor’s degree, age of first cannabis use; CUD symptoms: NH Black, Hispanic, all income variables, and government insurance.
Discussion
The current study examined factors (i.e., cannabis-related perceptions, marketing exposure, mental health problems) related to differences in cannabis use and use severity (any past 30-day cannabis use, daily/near-daily cannabis use, CUD symptoms) among SM relative to heterosexual adults residing in Oklahoma. Roughly 18% and 10% of females and males identified as SM, respectively, which is higher than the national and state average.1,58 A greater proportion of SM females was younger, racially and ethnically diverse, unemployed, uninsured, reported lower education, and had a medical cannabis license relative to heterosexual females. Among SM males, a greater proportion was younger, lower income, unemployed, and reported lower education than heterosexual males. Findings highlight the differences between SM and heterosexual adults in relation to cannabis-related factors, which were associated with cannabis use and use severity.
SM (vs. heterosexual) females reported greater odds of past 30-day cannabis use and daily or near-daily use, consistent with previous literature.6 -11 SM females also reported lower cannabis-related harm perceptions and a greater percentage reported cannabis marketing exposure, depressive symptoms, and anxiety symptoms relative to heterosexual females. In contrast, SM males were more likely than heterosexual males to report daily or near-daily cannabis use in both crude and adjusted models, but were not more likely to report any past 30-day cannabis use after adjusting for other factors. While SM males displayed higher rates of depressive and anxiety symptoms relative to heterosexual males, they showed no differences in other factors.
Neither SM females nor SM males displayed greater odds of CUD symptoms relative to heterosexual individuals. While SM individuals report that cannabis helps to alleviate depressive symptoms, they also report concerns about developing CUD symptoms. 59 Thus, participants in the current study may have been using cannabis at elevated rates, but are mindful about the possibility of developing CUD symptoms. Interestingly, greater harm perceptions were associated with greater odds of CUD symptoms among both females and males, potentially suggesting that individuals with CUD symptoms are more likely to perceive cannabis as harmful once they have become dependent. However, future work exploring these phenomena is warranted.
Findings expand upon limited work regarding a range of factors that are related to cannabis use among SM relative to heterosexual individuals, including cannabis-related marketing exposure 34 and harm perceptions. 26 They are consistent with those found among adolescent and young adult samples34,35 and found in the tobacco literature,60,61 which demonstrate that SM young adults report greater tobacco marketing exposure due to targeted marketing efforts from the tobacco industry (e.g., at LGBTQ+ community events). SM females’ lower cannabis-related harm perceptions relative to heterosexual females may be due to multiple factors, including: (a) higher rates of recent cannabis marketing exposure (as marketing efforts often include health claims and few health warnings62 -64), particularly in places like Oklahoma with high levels of cannabis marketing exposure43,44; and (b) greater use within LGBTQ+ social networks, which may impact risk perceptions via social norms.65,66
Cannabis marketing exposure and lower cannabis harm perceptions were associated with greater odds of any past 30-day cannabis use and daily or near-daily cannabis use among females. Individuals with lower cannabis-related harm perceptions likely worry less about adverse effects of cannabis (e.g., mental health problems), leading to greater likelihood of current use. 67 Greater exposure to cannabis-related marketing is also associated with greater purchasing access (e.g., via dispensaries, online) and cannabis availability.37,40,41,68 Indeed, almost twice the proportion of SM females compared to heterosexual females in our sample reported having a current medical cannabis license. Findings are also consistent with the tobacco literature, which suggests that SM females are more receptive to tobacco marketing than heterosexual females.32,61
Greater proportions of SM females and males reported depressive and anxiety symptoms relative to their heterosexual peers. However, neither depressive nor anxiety symptoms were associated with cannabis use outcomes among females after accounting for other factors. Among males, depressive symptoms were associated with greater odds of past 30-day cannabis use. From the lens of Minority Stress Theory, results may be emblematic of multiple community-level factors, including experiencing discrimination and marginalization across multiple social institutions (e.g., families, peers, workplace, society) and residing in an unsupportive state policy context, driving depressive symptoms and, in turn, using compensatory cannabis to self-soothe from these stressors.69,70
Current findings have implications for future research, policy, and practice. Findings stress the importance of moving beyond the Minority Stress Model to identify additional correlates of SM cannabis use differences, such as industry-level influences (e.g., cannabis marketing and related harm perceptions). Future research should examine how and why SM females are more frequently exposed to cannabis marketing than non-SM, including whether cannabis industries are engaging in targeted marketing to these groups like the tobacco industry.29,71 Moreover, research examining the influences of cannabis-related social norms and social meanings of cannabis on cannabis use and use severity among SM groups is needed.
Cannabis prevention messaging and cessation efforts should be tailored toward SM females and males, respectively, given different correlates of cannabis use among these groups relative to their heterosexual peers. Public health campaigns addressing cannabis-related harms may most effectively reach SM females in Oklahoma, whereas interventions focused on mental health symptoms along with the social conditions that perpetuate stigma and discrimination related to sexual identity may be most effective in reaching SM males in Oklahoma. We are unable to determine whether SM males and females in our sample were differentially exposed to cannabis-related targeted marketing, but this should be examined in future studies.
Limitations
The current study had several limitations. First, nearly one-third of our sample reported past 30-day cannabis use, which is higher than the 2019 to 2020 prevalence rate for Oklahoma (14.2%). 58 However, this could be because we asked respondents about both their medical and recreational cannabis use. Given limitations on recruiting such a large sample in Oklahoma, the sample was not fully representative of the state, although our demographics for age, sex, race/ethnicity, income, and insurance aligned with state estimates (within 3%-5%). 72 Because this study was conducted only in Oklahoma, findings should not be generalized to other states with varying legalized cannabis contexts. Second, the data were self-reported and cross-sectional, potentially leading to shared method variance and preventing our ability to examine causal or bidirectional associations among cannabis-related factors and cannabis use. Third, all SM females and males, respectively, were combined into a single group to increase sample size when making comparisons by cannabis-related factors and behaviors. Prior research has identified differences within the SM community (e.g., bisexual females have higher rates of substance use than lesbian females 73 ). Fourth, gender identity was not examined in the current study. Future research should examine patterns of cannabis-related factors and behaviors among specific SM-by-gender subgroups of adults. Finally, use of the PHQ-2, GAD-2, and CUDIT-SF prevented us from capturing a clinical diagnosis of depression, anxiety, or CUD.
Conclusions
The current study examined differences in a range of potential cannabis-related factors and behaviors among SM and heterosexual adults in Oklahoma. SM (vs. heterosexual) females reported higher rates of cannabis use, whereas SM (vs. heterosexual) females and males reported higher rates of daily/near-daily cannabis use. Among females, findings may be related to cannabis marketing exposure (for past 30-day and daily/near-daily use) and harm perceptions (past 30-day use), whereas past 30-day cannabis use among males may be related to depressive symptoms. With future replication, findings highlight important potential targets for reducing cannabis-related disparities among SM, relative to heterosexual females and males, respectively, living in places with legal medical cannabis retail markets, high structural stigma, and pronounced substance use. Public health campaigns aimed at correcting misinterpretations of harm that could emanate from marketing efforts by the cannabis industry may help reduce cannabis use among SM females, whereas SM males may be better reached by intervention efforts targeting mental health symptoms, as well as large-scale interventions that attend to the unjust social conditions that perpetuate stigma and discrimination related to sexual identity.
Footnotes
Author Contributions
All authors contributed to the conceptualization of the study and reviewed the article drafts. Data analyses were conducted by KFR. Initial article drafts were led by KFR and AMC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported in part by the National Cancer Institute Cancer Center Support Grant P30CA225520 awarded to the University of Oklahoma Stephenson Cancer Center, a seed grant awarded to AMC from the Oklahoma Tobacco Settlement Endowment Trust Contract # R22-03, and a career development award (K01DA055073) awarded to EAV from the National Institute on Drug Abuse. The content is solely the responsibility of the research team and does not necessarily represent the official views of the National Institutes of Health.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approvals were obtained from University of Oklahoma Health Sciences Center.