
Abstract
Background:
Concurrent substance use among adolescents has been associated with an increase in physical and mental health problems. These outcomes tend to be exacerbated among adolescents of color in underserved urban settings. The purpose of this study was to understand alcohol and concurrent drug use patterns among adolescents in an underserved urban community to provide targeted prevention and treatment recommendations.
Method:
This study examined data among adolescents in an underserved urban community (N = 1789; 56.90% female; 70.86% Hispanic/Latino/a; meanage = 15.96 ± 1.56). Using latent class analysis (LCA) and multinomial logistic regression modeling, analyses identified independent correlates of latent class membership.
Results:
Five latent classes (LC) were identified including LC group 1: Predominant alcohol use and limited to no concurrent-drug use (n = 213; 11.9%); LC group 2: Concurrent drug and alcohol use including methamphetamine, marijuana and synthetic marijuana use, and alcohol use (n = 74; 4.2%); LC group 3: Concurrent drug and alcohol use, with no marijuana use (n = 204; 11.39%); LC group 4: High Concurrent drug use and alcohol use (n = 204; 11.40%); and LC group 5: Concurrent drug use without alcohol use (n = 1101; 61.52%). Significant between group differences were noted between latent class groups and sociodemographic characteristics. Multinomial logistic regression models identified the associations between sociodemographic characteristics and corollary clinical features of substance use on latent class groupings of alcohol and concurrent drug use.
Conclusion:
Understanding concurrent substance use LC groups among adolescents is essential to providing targeted interventions and treatment programs, as well as early intervention programs that may help reduce substance use during adolescence.
Introduction
Drug and alcohol use have been linked to long-term cognitive and behavioral dysfunction among adolescents. 1 According to the Substance Abuse and Mental Health Services Administration (SAMHSA) 2020 National Survey on Drug Use and Mental Health, 13% (or 3.4 million) of adolescents (12-17 years old) used an illicit drug in the past year. 2 Further, 16.1% (or 6.0 million) of people under 21 years of age used alcohol during the past month and 4.1% (or 1.0 million) adolescents engaged in binge drinking. 2 The proportion of adolescents who used drugs in 2020 was higher among American Indian or Alaska Native (32%) adolescents, those adolescents who identified as multiracial (30%), and Black or African American adolescents (24.33%), when compared to non-Hispanic White adolescents (22%). 2 Similar proportional differences have also been noted on alcohol use between adolescents of color and their non-Hispanic White adolescent counterparts. 2 Based on these prevalence rates, it is critical to better understand the correlates of substance use among adolescents, especially the ethnic/racial minority youth population, in order to mitigate behavioral risk.
In the last two decades, there has been an increase in concurrent substance use in the United States among adolescents. 3 Concurrent substance use is defined as the use of multiple licit and illicit substances often to modify or enhance the effects of a single substance or compensate for the effects of one substance by taking another.4 -6 Concurrent substance use may also be an unintentional mixing of drugs.4,5 Regardless of the mechanism or reason for use, concurrent substance use has been linked with negative treatment outcomes, poor treatment retention, higher chances of relapse, and higher mortality rate, 4 highlighting the critical need to understand associations of concurrent substance use among youth.
Dangers related to concurrent substance use are numerous. People engaged in concurrent substance use are at an increased risk of health problems such as brain injury, liver damage, heart attack, and stroke, as well as overdose and ultimately death. 5 In addition to health risks, engagement in concurrent substance use has been linked to other mental health problems such as suicidal thoughts, suicidal attempts, and aggressive behaviors. 7 These mentioned health-related outcomes due to concurrent substance use tend to be exacerbated among adolescents of color in urban settings.
While there are some differences in the use of alcohol and drugs among adolescents of color, youth living in urban settings tend to experience more negative consequences than their non-Hispanic White adolescent counterparts, including more long-term negative health effects, more difficult pathways to recovery, and negative long-term economic outcomes. 8 Underserved urban communities tend to also have numerous ecological factors that place youth in at-risk circumstances, which increases the probability of alcohol and drug use, binge drinking, and smoking. 9 For instance, recent studies have shown that numerous ecological factors increase the likelihood of substance use including income inequality, lack of community prevention-intervention resources 10 and increased density of alcohol outlets,11,12 tobacco outlets,13,14 as well as access to illicit drugs. 15 These combinations of multi-system ecological factors influence the concurrent use of drugs and alcohol among adolescents of color. To gain a deeper understanding of concurrent substance use patterns and their correlates among urban youth, this study employed a person-centered approach utilizing latent class analysis (LCA). This approach enabled an exploration of nuanced substance use patterns.
There is a need in the adolescent substance use literature to further understand Latent class (LC) group membership characteristics of concurrent substance use among adolescents living in under-served urban communities. Primary aims for this study were to: 1. Use LCA to identify and investigate patterns of concurrent substance use among adolescents from an under-served urban community in the northeastern United States. 2. Examine corollary clinical features of substance use with LCA patterns of concurrent substance use among adolescents of color.
LCA was used to examine subpopulations of adolescents who demonstrated distinct patterns of concurrent substance use. Between-group analyses examined differences among sociodemographic correlates and identified concurrent substance use LC groups. Multinomial logistic regression analysis was used to investigate LC group membership representation based on clinically relevant correlates including depression and anxiety symptoms, suicidal ideations, access to alcohol, marijuana and other drugs, and risk perception. Examining the association between corollary clinical features and LC groups of concurrent substance use among adolescents could further inform substance use prevention initiatives to reach those youth who are the greatest risk. Such research could also provide important clinical considerations for treating youth engaged in concurrent substance use.
Methods
Participants and Procedures
This study used data from a Substance Abuse and Mental Health Services Administration (SAMHSA), Drug Free Communities (DFC) grant initiative. Part of this grant initiative assessed current beliefs, perceptions, and rates of substance use among a large cohort of adolescents from an under-served northeastern United States urban community. Data collected informed environmental prevention strategies. Students were sampled through their high school physical education and health classes in grades 9 through 12. Students who returned parental informed consent and student assent forms were given the opportunity to complete the questionnaire during these periods. The study procedures and protocol were approved by Montclair State University Institutional Review Board (IRB).
Students completed self-reported surveys in Qualtrics using Google Chromebooks® that were encrypted and locked to the school district virtual private network (VPN) within their physical education and health classes. Approximately, 4161 students were given the opportunity to participate in the parent study. Of these students, 2118 were recruited to complete the survey in the parent study (response rate of 50.90%). For the current study, participant responses were restricted to those who responded to questions on alcohol, marijuana, and other drug use (N = 1789; 84.46% of parent study). Among the delimited sample, less than 30% of data were missing and related to depression and anxiety. To preserve observations, we used multiple imputation based on multivariate imputation by chained equations. 16 Assessment of missing data were conducted using the mice package in R. 17
Statistical power and sample size requirements are understudied in LCA, but generally less concerning among robust sample sizes (n > 1000). 18 As a probabilistic or model-based technique, and variant of traditional cluster group analysis, simulation studies support that minimal power (0.70-0.80) is needed to correctly determine the number of classes. 18 Power estimates for this study were obtained using a two-tailed simple logistic regression formula in G*Power 19 resulting in conservative power estimates. To achieve 0.80 power based on an expected odds ratio of 2.00, inclusion of a minimum of 3 covariates with moderate associations (0.50) to LC membership groups with a value equal to 0.13, and 0.05 error, a sample of 400 is adequate, with estimates ranging from 0.75 (n = 200; odds ratio = 2.00) to 0.95 (n = 450; odds ratio = 2.40). While multinomial logistic regression does not necessitate a specific sample size, 20 power analyses indicate that this study’s current sample (N = 1789) makes it well-powered to identify appropriate odds ratios in multinomial logistic regression models.
Latent Class Group Membership Variables
This study focused on multiple variables from the parent study survey tool. Alcohol and concurrent drug use latent classes were derived from items from the Alcohol, Tobacco, and Other Drug Use (ATOD) scale of the Youth Risk Behavior Surveillance Survey. 21 The ATOD scale examined 30-day substance use with responses ranging from 0 to 30 days. 21 Items examined from the ATOD scale included marijuana, heroin, ecstasy, prescription drugs, synthetic marijuana, methamphetamine, and alcohol. Cocaine use was not included due to zero participants identifying use. Tobacco use was not included in these analyses given the focus on alcohol use and illicit drug use. For the purposes of LCA, responses that ranged from 0 to 30 days were re-coded as a dichotomous response option with 0 days coded as “No” (0) and 1 to 30 days coded as “Yes” (1). These questions were used to create LC groups.
Corollary Clinical Indicators of Latent Class Group Membership
Depressive and anxiety symptoms were derived from the Child Behavior Checklist.22,23 Depressive symptoms were examined using 5-items (sample items: “Sometimes I think that life is not worth it”; “All in all, I am inclined to think that I am a failure.”) and anxiety symptoms using 5-items (sample items: “I feared thinking or doing something bad”; “I felt nervous, high strung, or tense.”). Student responses were recorded using a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Responses were summed to reflect higher composite scores of depressive symptoms (M = 10.28 ± 2.46; Cronbach’s α = .90) and anxiety symptoms (M = 13.06 ± 2.72; Cronbach’s α = .89).
Quartiles were calculated to examine continuous variable distribution and identify appropriate cut-off scores to create dichotomized (0.00 or 1.00) score for subsequent analysis. Depression symptom scores ≥25% quartile cut-off (scores ≥9.00) were recoded as 1.00 (“Yes”) with all scores <9.00 recoded as 0.00 (“No”). The original continuous measure was highly correlated with the recoded dichotomized outcome (r = .89, P < .001). Anxiety symptom scores ≥25% quartile cut-off (scores ≥11.54) were recoded as 1.00 (“Yes”) with scores <11.54 recoded as 0.00 (“No”). The original continuous measure was highly correlated with the recoded dichotomized outcome (r = .80, P < .001).
Suicidal ideations was assessed using a single item from the Youth Risk Behavioral Surveillance Survey (item: “During the past 12 months, did you ever seriously consider attempting suicide?”). 21 Responses were recorded dichotomously (Yes = 1; No = 0). Approximately, 13.79% of students experienced suicidal ideations.
Access to alcohol, tobacco, marijuana, and other drugs was assessed using 6 items from the Communities that Care (CTC) survey 24 (sample items: “If you wanted to get beer, wine, or hard liquor (vodka, whiskey etc.), how easy would it be for you to get?”; “If you wanted to get a drug like cocaine, LSD, or amphetamines (or Meth), how easy would it be for you to get?”). Student responses were recorded using a 4-point Likert-type scale (1 = very hard to 4 = very easy). Student responses were summed to reflect increased access to alcohol, tobacco, marijuana, and other drugs (M = 12.84 ± 5.92; Cronbach’s α = .83).
Risk perception was assessed using 8-items from the YRBS that examined students’ perception of risk of using alcohol, tobacco, marijuana, and other drugs (sample items: How much do you think people risk harming themselves physically or in other ways if they use marijuana once or twice a week? How much do you think people risk harming themselves physically or in other ways if they use prescription drugs (eg, Vicodin, OxyContin (OCY), Hydrocodone, and Percocet) that are not prescribed to them?). 21 Student responses were recorded using a 4-point Likert-type scale (1 = No risk to 4 = Great Risk). Student responses were summed to reflect more perceived risk of using alcohol, tobacco, and other drugs (M = 30.39 ± 8.14; Cronbach’s α = .93).
Covariates
Several sociodemographic covariates were tested as statistical controls. Covariates were included in LCA and retained based on performance in the model. These covariates included gender identity, sexual-orientation identification Lesbian, gay, bisexual, questioning, and any other identities not encompassed under this acronym (LGBQ+), race-ethnicity, education level, and age in years. Gender identity was categorized using 3 separate response options (1 = Male; 2 = Female; and 3 = Gender non-conforming/non-binary). Sexual orientation-identification (LGBQ+) was categorized dichotomously (Yes = 1; 0 = No). Race-ethnicity was categorized dichotomously (Yes [to identified ethnicity] = 1, No [to identified ethnicity] = 0) using several questions that asked participants their race-ethnicity including American Indian/Native American, Asian, Black/African American, Hispanic/Latino/a, White non-Hispanic, and Native Hawaiian/Pacific Islander. Education level was categorized using five separate response options (9th grade = 1; 10th grade = 2; 11th grade = 3; 12th grade = 4; and not currently enrolled in school = 5). Age was measured in years.
Data Analysis
All analyses were conducted in R. 25 Following the examination of descriptive statistics, Latent Class Analysis (LCA) was used to identify distinct subgroups based on measures of heroin use, other opioid and prescription drug use, methamphetamine use, ecstasy use, marijuana and synthetic marijuana use, and alcohol use. LCA identifies unobserved subgroupings based on specific indicators. LCA was conducted in R using the proLCA package. LCA is a person-centered analysis that allows the researcher to categorize and uncover participation within subgroups and examine how groups of individuals function relative to others within the same population. 26 Eight Latent Class (LC) groups were modeled, and indices were retained as dichotomous response scales. 26
Using indices of model fit, a data driven approach was used to identify the best fitting and most parsimonious LC membership model, as well as the model that captured the largest number of total associations between observed indicators. Membership in LC groups are independent in that individuals cannot belong to more than one class group. Membership probabilities and item-response probabilities are used to assess and ensure that each class is distinguishable.27,28 Item-probabilities approaching 1.00 suggests higher certainty of class contribution and membership (see Figure 1).27,28
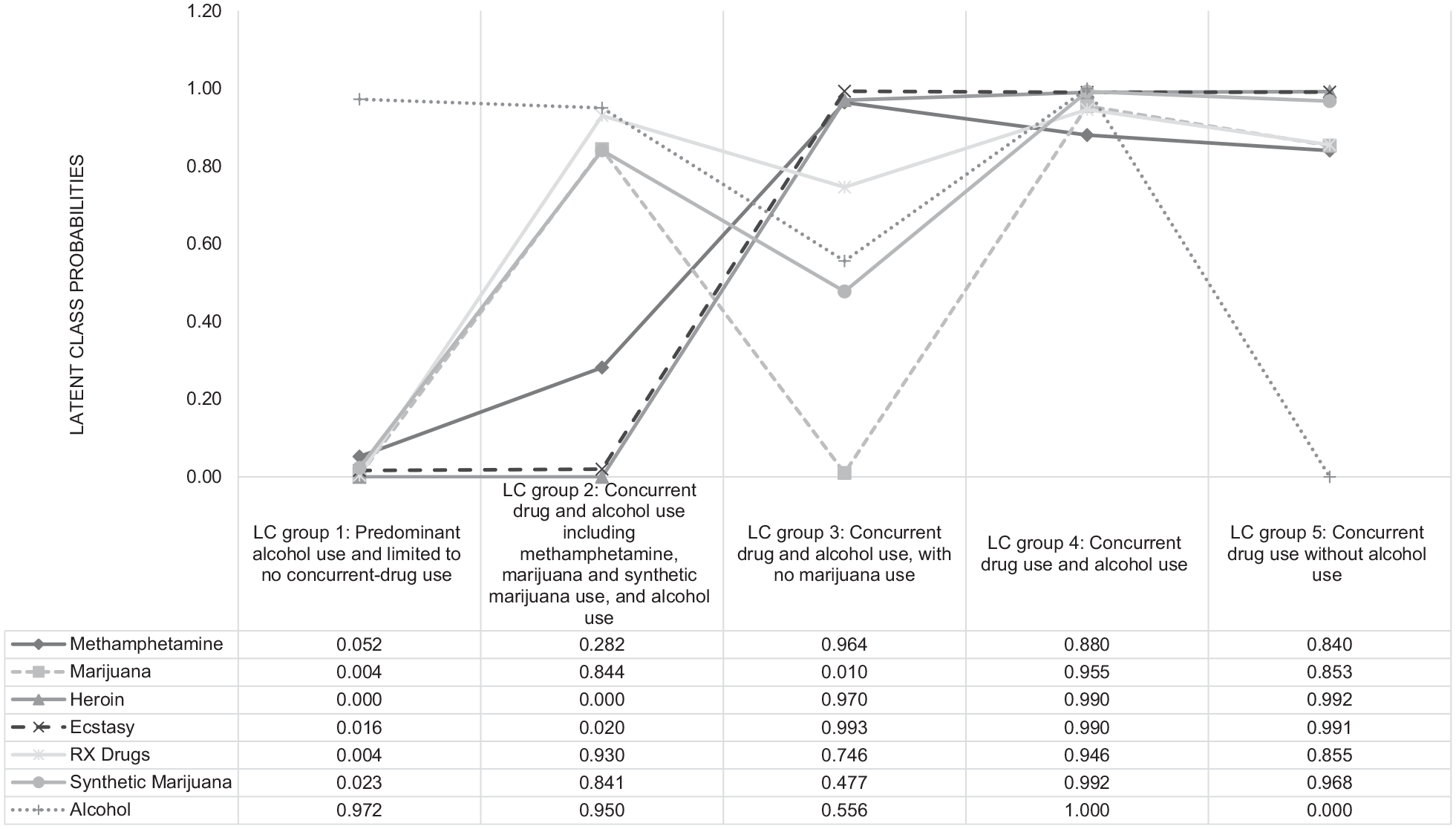
Latent class group membership probabilities.
Model fit indices include the likelihood ratio chi-square statistic (L2) Bayesian Information Criterion (BIC), Akaike Information Criterion (AIC), number of parameters, and classification error were used as comparative indicators to assess model fit. Larger L2 values and the associated degrees of freedom (df), as well as a significant bootstrap P-value, indicate poor model-to-data fit, or more highly negative than maximum precision can indicate, rendering values meaningless. Smaller BIC and AIC in relation to a smaller L2 and a nonsignificant bootstrap P-value, indicate good model-to-data fit. Entropy R2 was also considered when choosing the most parsimonious and best-fitting LC model for subsequent analyses. The maximum number of iterations through which the estimation algorithm will cycle was set at 5000 iterations, which is considered robust.26,29
After completing LCA models, multinomial logistic regression models were used to identify independent predictors of latent class membership. Log odds and adjusted odds ratios and corresponding 95% confidence intervals (CI) were presented. Multinomial logistic regression was conducted using the multinom function in the nnet package. 30
Results
Sociodemographic Characteristics
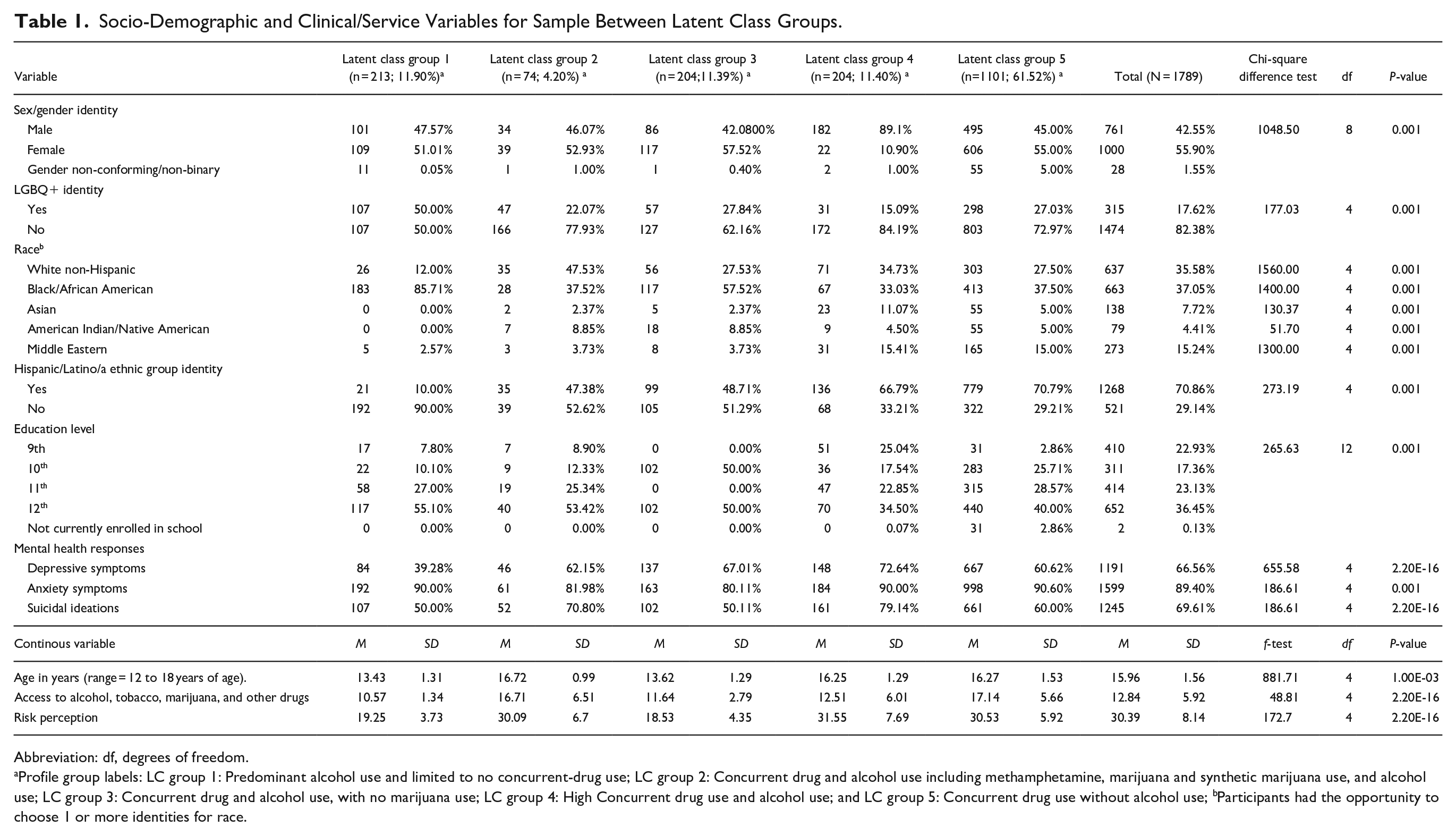
Sample characteristics are presented in Table 1. Participants in the total sample were 12 to 18 years of age (M = 15.96 ± 1.56), predominantly female (n = 1000; 55.90%), non-LGBQ+ (n = 1474; 82.38%), and identified with a racial category of either Black/African American (n = 663; 37.05%) or White non-Hispanic (n = 637; 37.58%); however, 70.86% (n = 1268) identified as ethnically Hispanic/Latino/a. Most students in the sample were in either 11th grade (n = 414; 23.13%) or 12th grade (n = 652; 36.45%).
Socio-Demographic and Clinical/Service Variables for Sample Between Latent Class Groups.
Abbreviation: df, degrees of freedom.
Profile group labels: LC group 1: Predominant alcohol use and limited to no concurrent-drug use; LC group 2: Concurrent drug and alcohol use including methamphetamine, marijuana and synthetic marijuana use, and alcohol use; LC group 3: Concurrent drug and alcohol use, with no marijuana use; LC group 4: High Concurrent drug use and alcohol use; and LC group 5: Concurrent drug use without alcohol use; bParticipants had the opportunity to choose 1 or more identities for race.
Latent Class Analysis of Concurrent Substance Use
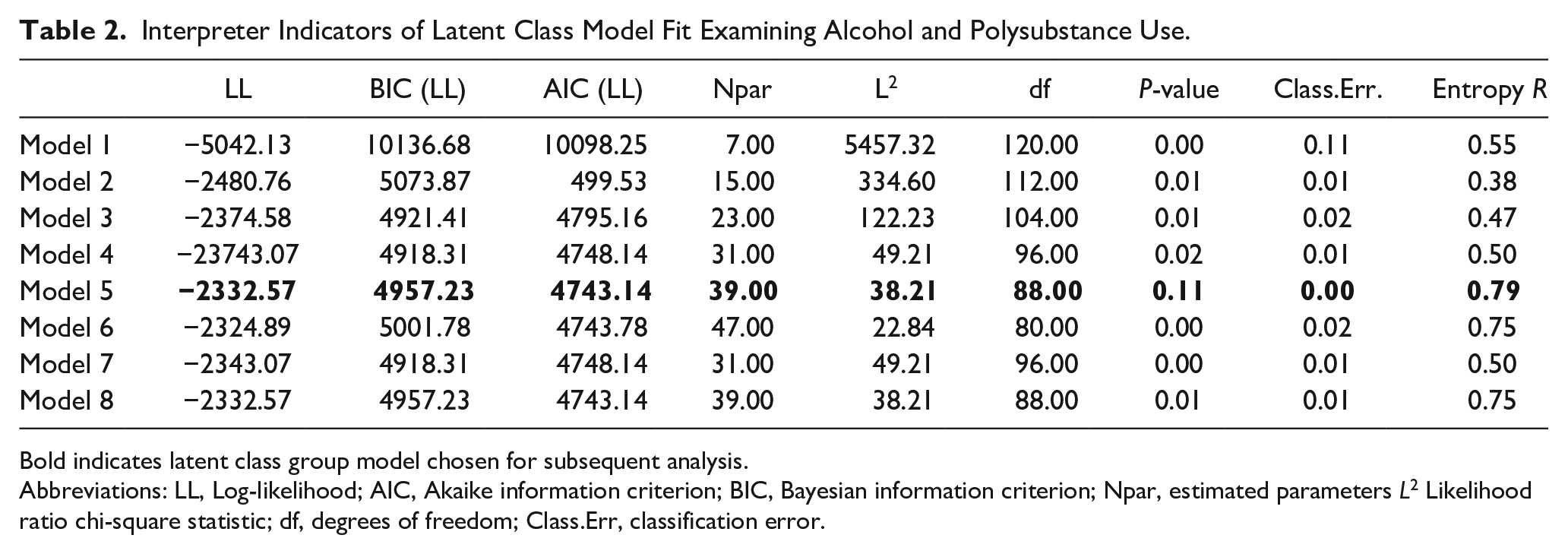
Interpreter indicators of model fit (Table 2) were examined. Individual cases were assigned to LC groups using standard modal classification (n = 1789). Potential covariates were included in the initial LCA modeling strategy but not retained due to no improvements in model-to-data fit; however, these same covariates were tested later in regression modeling. Results showed that the five LC group model provided optimal model-to-data fit to the sample data. LC group 5 showed the best model-to-data fit. Fit statistics for the best-fitting 5-class model were as follows: L2 = 38.21, BIC = 4957.22, AIC = 4957.22, and the bootstrap L2 P-value = .11. The five group LC model provided an entropy R2 value of .79. LC group probabilities were also within reasonable ranges to ensure classes represented a distinguishable LC group (see Figure 1).
Interpreter Indicators of Latent Class Model Fit Examining Alcohol and Polysubstance Use.
Bold indicates latent class group model chosen for subsequent analysis.
Abbreviations: LL, Log-likelihood; AIC, Akaike information criterion; BIC, Bayesian information criterion; Npar, estimated parameters L2 Likelihood ratio chi-square statistic; df, degrees of freedom; Class.Err, classification error.
LC group probabilities are estimated for each observation. These LC probabilities were used to assign LC groups and assist in labeling LC groups. Of note, LC modeling does not assign individuals to classes, rather, LC modeling probabilities are generated for membership in identified classes. 31 Probability cut-offs were pre-determined to assign LC groups (>50% LC probability indicates meaningful contribution to LC group). The five identified LC groups included: LC group 1: Predominant alcohol use and limited to no concurrent-drug use (n = 213; 11.90%); LC group 2: Concurrent drug and alcohol use including methamphetamine, marijuana and synthetic marijuana use, and alcohol use (n = 74; 4.20%); LC group 3: Concurrent drug and alcohol use, with no marijuana use (n = 204; 11.39%), LC group 4: Concurrent drug use and alcohol use (n = 204; 11.40%), and LC group 5: Concurrent drug use without alcohol use (n = 1101; 61.52%).
Between Group Differences on Sociodemographic and Latent Class Groups
Next, LC group differences among sample sociodemographic characteristics were analyzed (see Table 1). Significant between group differences were noted among LC groups and sociodemographic characteristics (P < 0.001). Differences were also noted on mental health responses. For instance, LC group 3 (n = 137; 67.01%) and LC group 4 (n = 148; 72.64%) had proportionally the largest percentage of participants that identified with symptoms of depression; LC group 1 (n = 192; 90.00%), LC group 4 (n = 184; 90.00%), and LC group 5 (n = 988; 90.60%) displayed larger proportions of participants that identified symptoms of anxiety. Suicidal ideations were present across all groups with slightly larger proportions of students with identified suicidal ideations in LC group 2 (n = 52; 70.80%), LC group 4 (n = 161; 79.14%), and LC group 5 (n = 661; 60.00%).
Multinomial Logistic Regression Model Assessing Factors Associated With Latent Class Group Membership Among Adolescents of Color
Multinomial logistic regression models were used to identify association between sociodemographic characteristics with between group differences P ≤ 0.20, and independent predictors associated with concurrent drug and alcohol use, including depressive symptoms, anxiety symptoms, suicidal ideations, access to alcohol, tobacco, marijuana and other drugs, and risk perception. Covariates were retained in final multinomial logistic regression model based on statistical significance (P < 0.05). Log odds and 95% CI, along with adjusted odds ratios, are presented in Table 3. LC group 5 was used as the reference category.
Multinomial Logistic Regression Model Assessing Factors Associated With Latent Class Group Membership Among Youth of Color (N = 1,789).
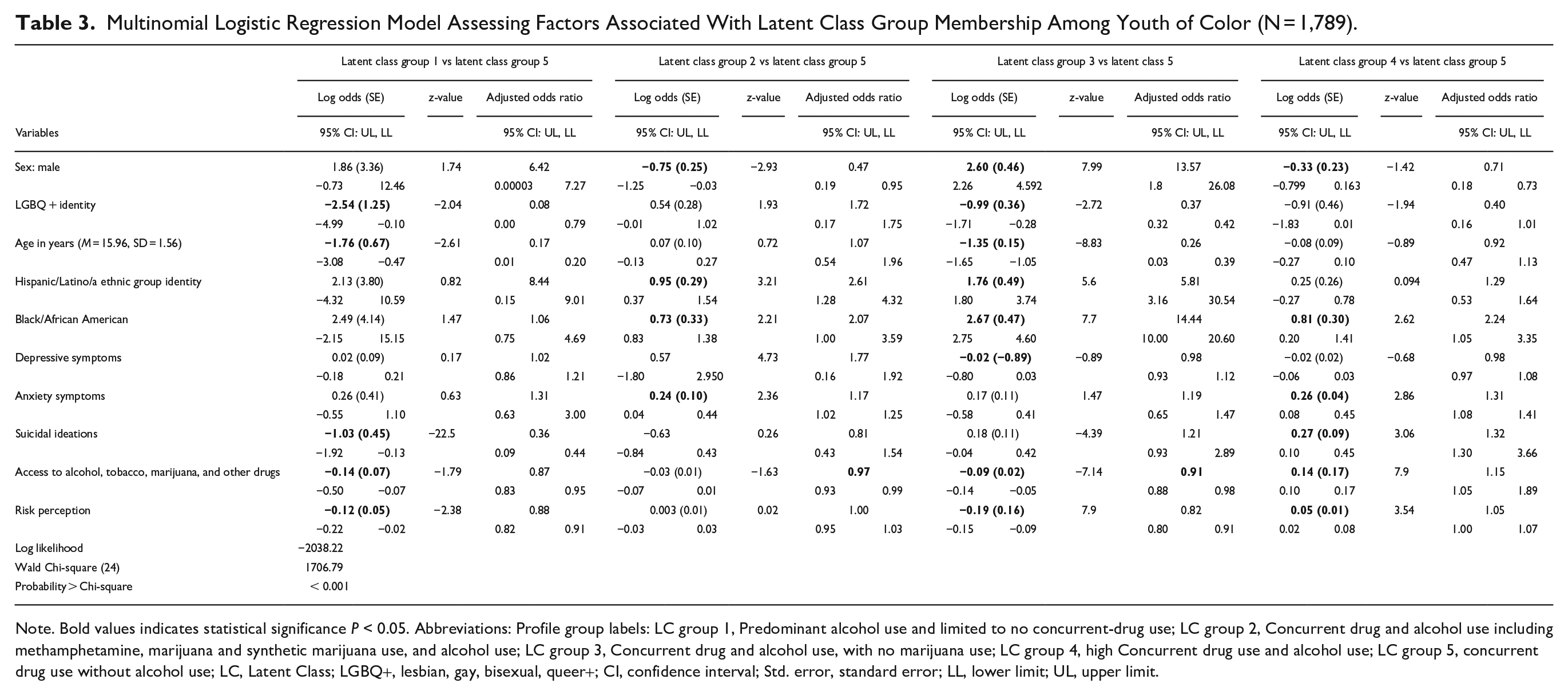
Note. Bold values indicates statistical significance P < 0.05. Abbreviations: Profile group labels: LC group 1, Predominant alcohol use and limited to no concurrent-drug use; LC group 2, Concurrent drug and alcohol use including methamphetamine, marijuana and synthetic marijuana use, and alcohol use; LC group 3, Concurrent drug and alcohol use, with no marijuana use; LC group 4, high Concurrent drug use and alcohol use; LC group 5, concurrent drug use without alcohol use; LC, Latent Class; LGBQ+, lesbian, gay, bisexual, queer+; CI, confidence interval; Std. error, standard error; LL, lower limit; UL, upper limit.
LC Group 1 versus LC Group 5. Suicidal ideations, access to alcohol, tobacco, marijuana and other drugs, and risk perception were negatively associated with membership in LC group 1 compared to LC group 5. LGBQ+ identity and age were also negatively associated with membership in LC group one compared to LC group five. LC Group 2 versus LC Group 5. Male identity was negatively associated with membership in LC group two compared with LC group five. Hispanic/Latino/a and Black/African American ethnic-racial identities were positively associated with membership in LC group two compared with LC group five. Anxiety was positively associated with membership in LC group two. LC Group 3 v. LC Group 5. Male identity, and both Hispanic/Latino/a identity and Black/African American ethnic-racial identities were positively associated with membership in LC group three compared with LC group five. LGBQ+ identity and age were negatively associated with membership in LC group three compared with LC group five. Both access to alcohol, tobacco, marijuana and other drugs, and risk perception were negatively associated with membership in LC group three compared with LC group five. LC Group 4 versus LC Group 5. Last, both Black / African American ethnic-racial identity and LGBQ+ identity were positively associated with LC group four compared with LC group five. Anxiety symptoms, suicidal ideations, access to alcohol, tobacco, marijuana and other drugs, and risk perception, were positively associated membership in LC group four compared with LC group five.
Discussion
The goal of this study was to utilize a person-centered approach (LCA) to identify subgroups of adolescent concurrent substance use. Additionally, we examined corollary clinical features of Latent Class (LC) group membership including depression and anxiety symptoms, suicidal ideations, access to alcohol, marijuana and other drugs, and risk perception. The results demonstrated that five meaningful groups emerged. Interestingly, alcohol use played an important role in group identification, as some adolescents used illicit drugs in combination with alcohol, while others used multiple illicit drugs without drinking alcohol and others primarily or exclusively engaged in alcohol use. While previous research has also identified groups of concurrent substance use in adolescence,32 -34 the inclusion of alcohol use is an important contribution of the current study. In addition, the broad age range of adolescents in this sample as well as the numerous drugs examined provides important considerations for clinical practice and programmatic initiatives. 33
This study also examined correlates of LC group membership and found that female and non-LGBQ+ identifying adolescents were more likely to engage in concurrent substance use without drinking alcohol. Racial/ethnic differences also emerged and suggested that there might be different patterns of substance use for adolescents depending on their race/ethnicity or cultural group membership. Adolescents who reported symptoms of depression were more likely to be in the LC group with high concurrent substance use and alcohol use, which is consistent with previous research linking depressive symptoms in adolescence to higher rates of substance use and problematic alcohol use.35 -37 Anxiety symptoms and suicidal ideations were associated with membership in LC group four: Concurrent drug use and alcohol use. These results highlight the strength of using a person-centered approach because specific mental illness indicators seem to be associated with specific patterns of concurrent substance use for adolescents.
This study extends existing research on concurrent substance use in adolescence and can inform targeted intervention and treatment. Most prior research on concurrent substance use has not considered alcohol use in combination with other substances among a sample of adolescents within an urban context.33,38 Examining adolescent alcohol use in the LCA added evidence that there are unique patterns of substance use occurring, including combinations of specific substances with alcohol. Of particular note, those in LC group 4 may have the greatest difficulty in treatment due to high rates of co-occurring drug and alcohol use, as well as greater odds of experiencing comorbid conditions such as anxiety and suicidal ideations. These groups might need specific intervention plans based on their environmental and psychological characteristics.
Substance use and mental health treatment have traditionally focused on treating either substance use or mental illness separately, and when engaged in substance use treatment, providers have conventionally focused on a singular substance.39 -41 Providers working with youth engaged in concurrent substance use, and likely with comorbid mental health conditions, need to utilize appropriate and comprehensive screening assessments to support appropriate multidimensional treatment planning. 6 As evident in our study findings, there are numerous pairings and patterns of concurrent substance use that may be more strongly associated with adverse outcomes or perceptions (e.g., those in LC group 4 with high rates of co-occurring drug and alcohol use, and having greater odds of experiencing comorbid conditions such as anxiety and suicidal ideations). Because of this, providers need to be able to implement effective strategies to manage clinical needs for those engaged in concurrent substance use. For instance, interventions that combine both pharmacotherapy with counseling and, or contingency management strategies may be effective for adolescent patients with psychiatric comorbidities and negative external antecedents (e.g., high density of alcohol and licit/illicit drug access).42,43 Furthermore, targeted prevention and treatment recommendations including early intervention programs such as Screening, Brief Intervention and Referral to Treatment (SBIRT) can delay or reduce substance use in adolescence. Yet, concurrent substance use and mental health treatment is complex and will likely need to include treatment support services from different provider settings (e.g., residential, outpatient, or therapeutic communities), as well as take an ecological approach to implementation—meaning, placing emphasis on systemic supports such as families, peers, and other social support systems.
Child and adolescent mental health service agencies, youth addiction services and other health and social services, as well as prevention specialists and policy-makers need to take a multi-systemic ecological approach to both implementing and funding concurrent substance use and mental health treatment and prevention services. Treatment and prevention of concurrent substance use and mental health conditions can vary across geography, socioeconomics, culture, ethnicity, race, gender identity, and age. Therefore, treatment intervention and prevention programming that is culturally-sensitive, -responsive, and -appropriate can facilitate engagement and attendance and improve outcomes. 44 One such treatment recovery program that has displayed efficacy across geographic regions and among various racial-ethnic youth groups in the United States is the Adolescent Community Reinforcement Approach (A-CRA).45 -47 A-CRA seeks to support youth in recovery by increasing family, social, and educational/vocational reinforcement.45 -47
Future funding needs to be allocated to multi-systemic and ecologically-focused treatment, recovery, and prevention initiatives, as these programs may have increased effectiveness in the treatment of substance use disorders, promoting recovery, and preventing substance use among youth. 48 More importantly, funding priorities and Requests for Applications (RFA) need to emphasize the involvement of youth and other stakeholders in the development and delivery of comprehensive clinical mental health and substance use systems of care service approaches. One such example is the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Project AWARE (Advancing Wellness and Resiliency in Education) Grant Initiative (https://www.samhsa.gov/grants/grant-announcements/sm-23-001), which focuses on developing a sustainable infrastructure for school-based mental health and substance use programs and services. Importantly, there is an emphasis in these programs for the direct involvement of youth end-users and other stakeholders in the development of program services and sustainability. Funding and implementation of such programs alongside youth end-users and other stakeholders is critical to adequately addressing the needs of adolescents from complex and marginalized social and ecological backgrounds.
Limitations
The study has several limitations. First, the sample is limited to those students who were present in school for the survey. This does not account for students who are truant, have been suspended or expelled/no longer attending school. Therefore, these results may not be generalizable to all students within an urban community. Second, data were delimited to those student participants who responded to questions about alcohol, marijuana, and other drug use. While most non-responses were due to missing data, there is a potential for selection bias in those who did not respond to this question versus those who did respond to this question and were examined in this study. Yet, this cannot be fully known. Future research should examine issues of selection bias when attempting to uncover person-centered-specific differences related to concurrent substance use. Third, data were collected from a single state and urban community in the United States. This represents a small limitation when considered alongside the robustness of the sample. Nonetheless, future studies should draw samples from numerous urban communities to reflect and expand the diversity of possible participants. Fourth, while students may report symptoms of depression and anxiety, clinical presence of a mental health diagnosis was not verified by a trained clinical behavioral health provider, nor further verified against health records in school. This small limitation poses a need for future research to consider multiple methods of ensuring reliability and accuracy of findings related to mental health. Fifth, the route of drug use intake was not included in the survey, posing as a limitation. Future research should include questions on route of drug use, which will provide important information for precision-medicine, harm reduction, and other prevention-intervention programs for populations at-risk. Sixth, data were cross-sectional, which cannot address longitudinal, or time-order effects. Consequently, it may be difficult to draw generalizable conclusions from a cross-sectional sample. Yet, the size of the sample is a boon, making this a somewhat smaller limitation. Seventh, data were limited to questions required by the federal funding agency. Therefore, covariates of notable importance were not included in the initial survey but need to be considered in future studies. Covariates of particular interest that were not part of this current study survey included: socioeconomic status (SES) or a proxy for SES such as free/reduced lunch, experiencing racial discrimination, complex and community trauma, as well as others (see PhenX Toolkit (https://www.phenxtoolkit.org/) as an example of a comprehensive web-based catalog of recommended measurement instruments and protocols). Last, the sample size was robust (>1000 student participants) and sufficient for LCA based on simulation studies 18 and power analyses conducted for this study. However, some subgroups designated relatively smaller sample sizes proportion to the entire sample. The accuracy of both approaches depends on the strength of the correlations of the measures in a LC group. With strong enough correlations, LCA is capable of producing strong class structure based only on 30 observations.18,49,50 Strong associations were present between variables, and consistency with prior investigations is encouraging when considering relative stability of results.
Conclusion
Concurrent substance use during adolescence has innumerable unfavorable developmental outcomes. Our findings have important implications for both prevention and practice, and provide a step in understanding concurrent substance use and associations with mental health and other corollary clinical features. Recognizing patterns of alcohol and substance use in under-served communities can support interventions targeted to such groups without disregard for other environmental factors that promote the likelihood of access to substances.
Footnotes
Author contributions
DTL and AND originated the project manuscript and PGR and RJR obtained funding. DTL, AND, CSV, LC, and SM drafted the initial manuscript. AH, PGR, and RJR secured the data and DTL conducted the analyses. All authors participated in interpreting the results, contributed to the writing of the manuscript, provided critical feedback to the manuscript, and approved the final manuscript draft for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Substance Abuse and Mental Health Services Administration Grant to Drs. Robert J Reid and Pauline Garcia-Reid (Grant # SP082663)
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.
Consent to Participate
All procedures followed were in accordance with the ethical standards of the responsible committee on human subject’s research (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants for being included in the study.