
Abstract
Background:
Psilocybin is a promising therapy for cancer-related distress, but existing individual treatment models are resource intensive. In this study, we designed and tested a group model of psilocybin therapy for people with metastatic cancer and cancer-related anxiety and depression.
Method:
Eligibility criteria included metastatic cancer, moderate-to-severe symptoms of anxiety or depression without a pre-cancer mental health diagnosis, performance status adequate to attend a 3-day retreat that required self-care, and tapering of antidepressants. Exclusion criteria included enrollment in hospice. The design of the intervention included: two virtual preparatory sessions; a 3-day in-person retreat in a rustic setting that included the third prep session, the psilocybin session, and the first integration session; and two additional virtual integration sessions. Psilocybin was administered in oral capsules at 25 mg. A retreat team of four core facilitators and two backup facilitators conducted a series of eight retreats. The first retreat had five participants. For subsequent retreats, we used the primary safety outcome from each cohort, other safety outcomes, and qualitative feedback to make decisions to increase, decrease, or hold steady the participant number. The primary safety outcome was “unattended episodes of participant distress” during the psilocybin session requiring a backup facilitator. The primary exploratory efficacy outcome was reduction in anxiety and depression symptoms measured using the Hospital Anxiety and Depression Scale (HADS).
Results:
We enrolled 55 participants, of whom 3 withdrew prior to the retreat, leaving a total of 52. Their mean age was 53, and mean duration of living with cancer was 36 months, mean (range 5, 176); anticancer therapy was ongoing for 46 (88%); antidepressants were tapered for 18 (35%). The first retreat cohort had five participants, and the final retreat cohort had eight. For the primary safety outcome, there was not a single episode of unattended participant distress requiring a backup facilitator. The mean baseline at Day −14 (D −14) HADS total score was 17.5 (range 6–28); at D +28, the mean HADS total score was 10.2 (1–30), so the mean decrease in HADS from D −14 to D +28 was 7.3. (p < 0.0001).
Conclusion:
The Group Retreat Psilocybin Therapy was safe and well tolerated, and exploratory measures show efficacy that is promising. A group configuration of eight participants with four core facilitators can be safe for future studies with participants with serious medical illness.
Introduction
Psilocybin is a promising therapy for cancer patients with anxiety, depression, and existential distress.1,2 For patients with cancer, individual psilocybin therapy tested in randomized studies comparing psilocybin with placebo has shown efficacy in reducing symptoms of anxiety and depression.3–5 In these studies, treatment benefit appears to be greater than for individual psychotherapy, which current guidelines recommend as the standard of care. 6 However, the individual treatment model is resource intensive, requiring ≥ 16 h of therapist time per patient.
Group models of psilocybin therapy may offer an alternative with positive impact beyond resource use.7–8 These benefits may include peer support, social identity processes,9 group cohesion and trust,10,11 and ceremonial experiences of community. 12 In addition, cancer support groups without psilocybin have demonstrated efficacy for well-being.13,14
A review of the medical literature shows only two prior studies describing group psilocybin therapy for patients with cancer, and these studies emphasized group work in the preparation and integration phases but conducted the psilocybin session as individual.15,16 Agrawal et al. used psilocybin sessions that were conducted with one therapist and a video-monitoring therapist with one patient in an individual room15,17,18; Lewis et al. conducted psilocybin sessions with one therapist assigned to one patient in a chemotherapy suite with curtains separating participants. 16 A 2019 systematic review did not identify any studies using groups in studies of psilocybin for patients with cancer. 19
We developed a group model, called Group Retreat Psilocybin Therapy, where the psilocybin session itself was conducted in a room with all group members, in a rustic natural setting, with a multidisciplinary team of facilitators, who all interacted with each participant. Our experience with cancer support groups suggested that more than four participants per group, such as six to eight, would optimize the group process and foster participant peer support.
The objectives of this study were to assess the safety of this group format, especially regarding facilitator-to-participant ratio, and collect exploratory efficacy outcomes measuring symptoms and other aspects of group experience.
Methods
Trial design
This was a single arm, open-label trial of Group Retreat Psilocybin Therapy in which a fixed number of facilitators worked with a varying number of participants in each cohort. For all the cohorts, two facilitators conducted the virtual preparation and integration sessions, and four facilitators plus two backup facilitators conducted the 3-day retreat. The prespecified primary safety outcome was “unattended episodes of participant distress” during the psilocybin session that required involvement of a backup facilitator. Over a series of eight cohorts, we used the primary safety outcome from each cohort, other secondary safety outcomes, and qualitative reports from participants to make decisions about whether to increase, decrease, or hold steady the number of participants enrolled in the next cohort. A trial guidance committee, including experts other than the investigators, provided guidance. Exploratory efficacy outcomes were also collected at baseline (D −14) and following the psilocybin session (D 0) at D +7, D +28, D +56, D +84, and D +180.
Participants
The eligibility criteria included: a diagnosis of a metastatic solid tumor for which evidence-based curative therapy was not available, or incurable hematological malignancy; age 18–85; Eastern Cooperative Oncology Group (ECOG) performance status 0–2; acceptable organ and bone marrow function with creatinine ≤ 1.5x normal; liver function tests ≤ 1.5× normal, hematocrit ≥ 20, platelet count ≥ 20 K; >4 weeks after surgery or radiation; interest in participating in a group study; and screening Hospital Anxiety and Depression Scale (HADS) total score of > 11 (indicating clinically significant symptoms of anxiety and/or depression). No prior high-dose psychedelic session in the past year was allowed; microdosing was allowed but would need to be stopped 2 weeks prior to starting the study intervention. Participants were required to taper off antidepressants prior to starting the study preparation sessions (to make this study comparable with other published studies with cancer patients), and to taper off scheduled benzodiazepines and cannabis products prior to the retreat (which may confound the effect of psilocybin on outcomes). Participants could continue intravenous (IV) anticancer regimens but had to be off for at least 7 days prior to the first day of the retreat or enough time so that their oncologist did not expect them to be neutropenic (absolute neutrophil count < 1000 cells/microliter); oral anticancer regimens were handled individually, with most being held on the day of the psilocybin session. Opioid pain medications, including scheduled and breakthrough doses, were allowed on the psilocybin day.
The exclusion criteria included: enrollment in hospice, mental health diagnoses prior to the diagnosis of cancer requiring medication or clinical care (e.g., psychosis), family history of schizophrenia, and inability to self-care for the 3-day retreat.
Recruitment was done using a study website, clinicaltrials.gov, and social media.
Facilitators
Facilitators were selected for: experience working with cancer patients in a clinical setting, group facilitation experience, a personal contemplative practice, and personal experience with non-ordinary states of consciousness. The multidisciplinary facilitators included physicians, clinical psychologists, masters trained psychotherapists, advanced registered nurse practitioners, chaplains, registered nurses, and licensed counselors (Master of Social Work, Licensed Clinical Social Worker, or Licensed Mental Health Counselor), all trained to the study protocol.
Intervention design
The intervention components included: (1) two virtual preparatory sessions; (2) a 3-day in-person retreat that included the third prep session, the psilocybin session, and the first-integration session; and (3) two additional virtual integration sessions. All sessions were manualized (manual available from the corresponding author).
The physical setting was a rustic retreat center that has a 30-year history of doing cancer retreats, with individual rooms, shared bathrooms, a dining hall, a great hall for the group sessions, views of nature, short trails, and a labyrinth. Rescue medications were available (metoprolol, ondansetron, and lorazepam). At least one facilitator was Basic Life Support certified, and the retreat center had an automatic defibrillator adjacent to the room we used (which A.L.B. was trained to use). The retreat center was 20 min from the nearest Emergency Department.
The facilitation model (described in Group Retreat Psilocybin Therapy for People with MetastaticCancer with Anxiety and Depression: A Rite of Passage Facilitation Model for a Phase1/2 Study) considered the entire intervention to be a rite of passage with three phases, as described by van Gennep 20 : (1) separation phase, (2) liminal phase, and (3) reincorporation phase. Our preparation sessions corresponded to “separation” (leaving one’s normal routine); the psilocybin session corresponded to the “liminal” phase; the integration sessions corresponded to the “reintegration” phase. To enact the rites of passage facilitation model, the intervention included brief ritual elements that signaleded each phase, such as an opening circle poem to mark stepping away from one’s usual routine; having participants bring symbolic objects to the psilocybin session that represented people or things that would remind them even while in a liminal space of why they choose to be in the study; and integration activities that reminded participants to bring their psilocybin session experiences and learnings back into their day-to-day life. Ritualized framing has been described in prior clinical trial contexts and therapeutic settings as a means of fostering psychological safety, promoting reflective states of mind, and enhancing engagement.21–23 The facilitation model and ritual elements were intended to invoke a contemplative, secular, person-oriented (rather than medically oriented) set and setting.
The first preparation session began developing the mental “set” for the participants. The high-level objectives for preparation were to introduce group members to each other, articulate reasons for wanting to participate, discuss cancer-related experiences, and provide psychoeducation for the psilocybin experience. The group interaction for most sessions was based on Council practice, a structured form of group dialogue, 24 and prior clinical trials of cancer support groups.11,25–27 In the version of Council used in this study, participants and providers convened on zoom or sat in a circle, used a talking piece (a physical object passed around a group to regulate the pace of conversation in a circle that encourages speakers and listeners to be more mindful, more reflective, and more self-aware), and responded to prompts given by facilitators (which are available in the Supplementary Data). Council differs from group psychotherapy in several important respects: as a modality is not designed to provide diagnosis, interpretation, or treatment of psychological disorders. Instead, it emphasizes equal participation, reflective listening, and speaking from personal experience in a non-hierarchical circle. Facilitators serve as guides for the process rather than as therapists analyzing content. Thus, we describe this intervention as “Group Retreat Psilocybin Therapy” rather than “group psychotherapy” or “assisted psychotherapy.”
The preparation also included practical and individual elements. Participants arrived at Day 1 of the 3-day retreat, for lunch, had group sessions that included psychoeducation about “what to expect,” and a 30-min individual session to discuss anything they did not wish to bring up in the group, describe touch preferences, and have a suicidality assessment; this was followed by a group dinner and an evening session to get accustomed to their mattress, eye shade, and music, and to practice raising a hand for assistance.
The psilocybin session, on Day 2, was designed to support participants for an experience of liminality which included uncertainty, emotional moments, and unexpected experiences. In the morning, there was a guided labyrinth walk, and then when they arrived at the hall, vital signs were taken, and psilocybin 25 mg oral capsules (Filament Health, Vancouver, BC) were administered in a brief ritual where participants spoke their intentions aloud. Blood pressure was measured pre-psilocybin and 1 h later, and followed if elevated. A playlist curated for this study (Wavepaths) was played over speakers. The facilitators moved around the room during the 7-h session to support all participants during the course of the day and provided support in response to explicit requests. (Participants were trained to raise their hand to request support and practiced this on Day 1.) Touch was offered according to the participant’s preferences using previously published study guidelines. 28 A study assistant tracked all interactions between facilitators and patients on a structured form. The psilocybin sessions were videorecorded for potential review if any incidents of compromised safety occurred. At the end of the session, snacks were offered followed by a brief closing circle. Participants were assessed before or after dinner to ascertain if extra attention was needed and had the phone number of a facilitator who was staying in the building on-call through the night.
The integration sessions began formally on Day 3 of the retreat, when participants had a private session with a facilitator to tell the story of their psilocybin session, a group circle to share whatever part of their psilocybin experience they felt ready to talk about, a psychoeducation session about returning home, a session about how to continue integration at home, and a second brief private session for a safety check prior to leaving the retreat center. Following the retreat, there were two virtual integration sessions, designed to fulfill the “reincorporation” phase of a rite of passage, to enable participants to bring their insights into their everyday lives.
Safety and efficacy measures
The primary safety outcome was “unattended episodes of participant distress,” defined as a time period of any length during the group psilocybin session when four participants required 1:1 support simultaneously while another participant was experiencing distress that was unattended. The study assistant, who was trained to track interactions and record them on a structured form, watched for instances when a participant in a psilocybin session appeared to need 1:1 assistance, was not receiving it, and was becoming more distressed. All psilocybin sessions were videotaped so that these instances could be reviewed (this was not necessary). This outcome was measured with a study staff who logged all facilitator interactions with participants in real time. These time-motion logs were converted to visual diagrams showing interaction in 15-min blocks during the 7-h psilocybin session.
The secondary safety outcomes were five questions that we developed after the first retreat and began using starting with the second retreat. The questions were: (1) Were there ever times when you felt you did not get the attention from the facilitators you needed to be safe?; (2) Were there ever times when you were having difficulty and the facilitators did not respond adequately?; (3) Were there ever times when a facilitator talked to you in a way that you found intrusive or unwanted?; (4) Were there ever times when a facilitator touched you in a way that you found confusing or unwanted?; and (5) As you look back now, do you feel that other participants were supported adequately by the facilitators? These questions were administered in person by a facilitator during a private meeting with the participant on the morning after the psilocybin session so that if a participant answered “yes” to any question, we could ascertain details of the event.
Adverse events were collected using the National Cancer Institute Common Terminology Criteria for Adverse Events at the retreat, and facilitators continuously observed participants for adverse events, reporting them at twice-daily facilitator meetings. After the retreat, participant adverse events were collected after virtual integration sessions and as reported during interactions for measurement collection.
The primary efficacy outcome was symptoms of depression and anxiety measured by the HADS. 30 The HADS is a 14-item measure chosen because it was used in prior studies of psilocybin therapy for cancer, has been extensively validated in patients with cancer, and avoids somatic symptoms that could overlap with cancer-related fatigue. A decrease in HADS scores indicates improvement. The Demoralization Scale II (DS-II) is a 16-item self-report instrument designed to assess demoralization30,31; each item is rated on a 3-point Likert scale, with total scores ranging from 0 to 32, where higher scores indicate greater demoralization. The Death and Dying Distress Scale (DADDS) is a 15-item measure used to assess distress related to thoughts of death and dying 32 ; each item is rated on a 6-point Likert scale, ranging from 0 (“no distress”) to 5 (“extreme distress”), with total scores ranging from 0 to 75, where higher scores indicate greater distress. The National Institutes of Health Healing Experience of All Life Stressors (NIH-HEALS) was used to assess psychosocial and spiritual healing 33 ; each item is rated on a 5-point Likert scale, with higher scores indicating greater well-being. The Functional Assessment of Cancer Therapy—General (FACT-G) is a 27-item measure used to assess quality of life that has been widely used in cancer studies. 34 These measures were collected on a secure mobile app (Quantified Citizen) from baseline D −14 to 6 months D +180.
Additional exploratory measures of the psilocybin experience were administered on paper on the morning of Day 3: Mystical Experience Questionnaire 30 (MEQ30), a 30-item self-report measure with scores from 0 to 150, with higher scores indicating greater mystical experience intensity 35 ; the Challenging Experience Questionnaire, a 26-item self-report measure with scores from 0 to 130 with higher scores indicating more challenging experiences 36 the Emotional Breakthrough Inventory (EBI), a 6-item measure with scores from 0 to 600, with higher scores indicating more profound emotional breakthroughs 37 ; and the Communitas scale, a 10-item measure with scores of 10–70 with higher scores indicating stronger group bonding. 12
In addition to standardized quantitative outcomes, participants were invited to provide brief written reflections about their experience, and their Day 3 individual sessions were audio-recorded. A selection of quotes is presented alongside the retreat process quantitative results to provide an illustration of how these numerical results were experienced by participants, even though these do not represent a formal qualitative analysis.
Analysis
Safety outcomes
Descriptive statistics were used to describe all safety outcomes, including “unattended psilocybin-related distress”; these outcomes were tabulated from the interaction worksheet immediately after each group intervention.
Facilitator interactions
Descriptive statistics were used for facilitator interactions, which were coded during analysis as “simple” or “complex” using a definition developed during the course of the study. The data were visualized using Tableau software.
Efficacy outcomes
For the primary exploratory efficacy measure of HADS total score, a pre–post strategy was used to compare the mean change from D −14 to D +28 using a 1-sample t-test. Mean changes (and standard deviation of the mean change) in HADS total score from D −14 to D +7, D +28, D +56, D +84, and D +180 after the psilocybin session (D 0) were also summarized. Mean changes from D −14 to D +28 for other measures were also summarized and assessed with 1-sample t test, and mean changes (with standard deviation of the mean change) from D −14 to other timepoints are presented descriptively.
Human subjects
This study was reviewed and approved by the Federal Drug Administration, the Fred Hutch Cancer Center Scientific Review Committee, and the Fred Hutch Internal Review Board. No information about study participation was entered into the University of Washington electronic medical record, and a Certificate of Confidentiality was obtained. This trial was registered at clinicaltrials.gov (NCT05847686).
Results
Participants
Demographics
We enrolled 55 participants who committed to start the intervention and attend a retreat. Of those, 52 (90%) attended the retreat to which they were assigned (Fig. 1). Of the treated participants, 32 (61%) were female, 6 (12%) self-reported race or ethnicity other than White, and mean age was 53 years (range 26–81). Mean duration of living with cancer at study entry was 36 months (range 5, 176). Additional details are in Table 1.
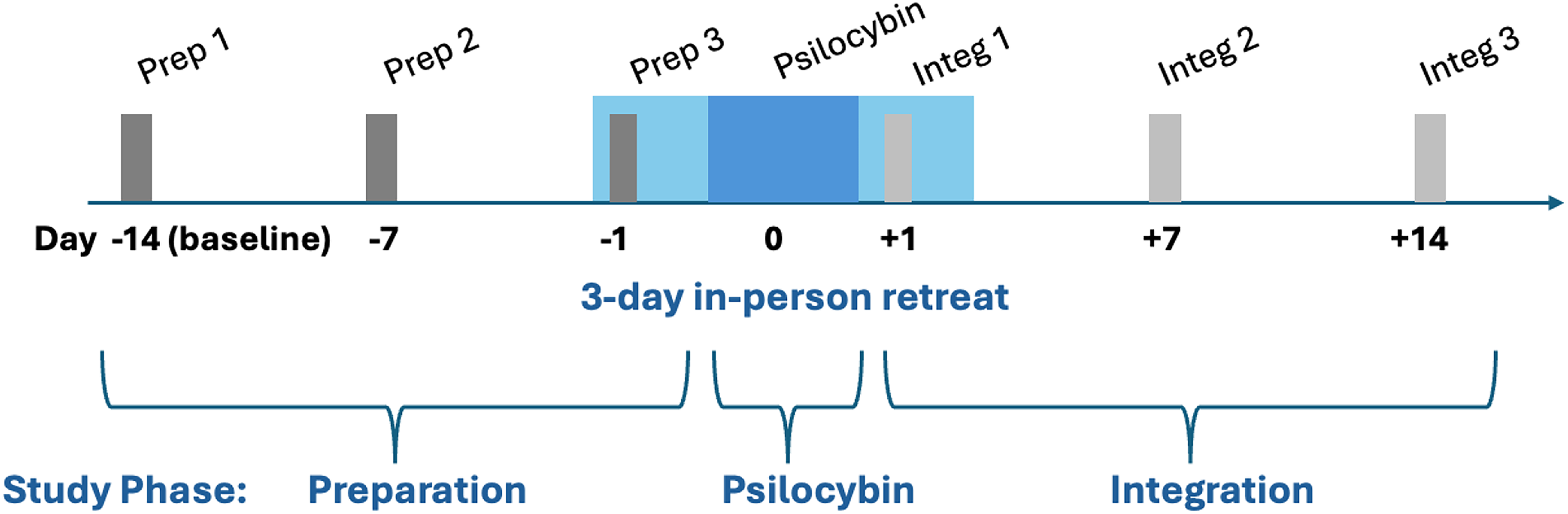
Structure of the Group Retreat Psilocybin Therapy. The three preparation sessions, all 90 min, are shown by dark gray bars. Preparation sessions 1 and 2 were virtual. The three integration sessions, all 90 min, are shown by light gray bars. Integration sessions 2 and 3 were virtual.
Demographics and Baseline Characteristics
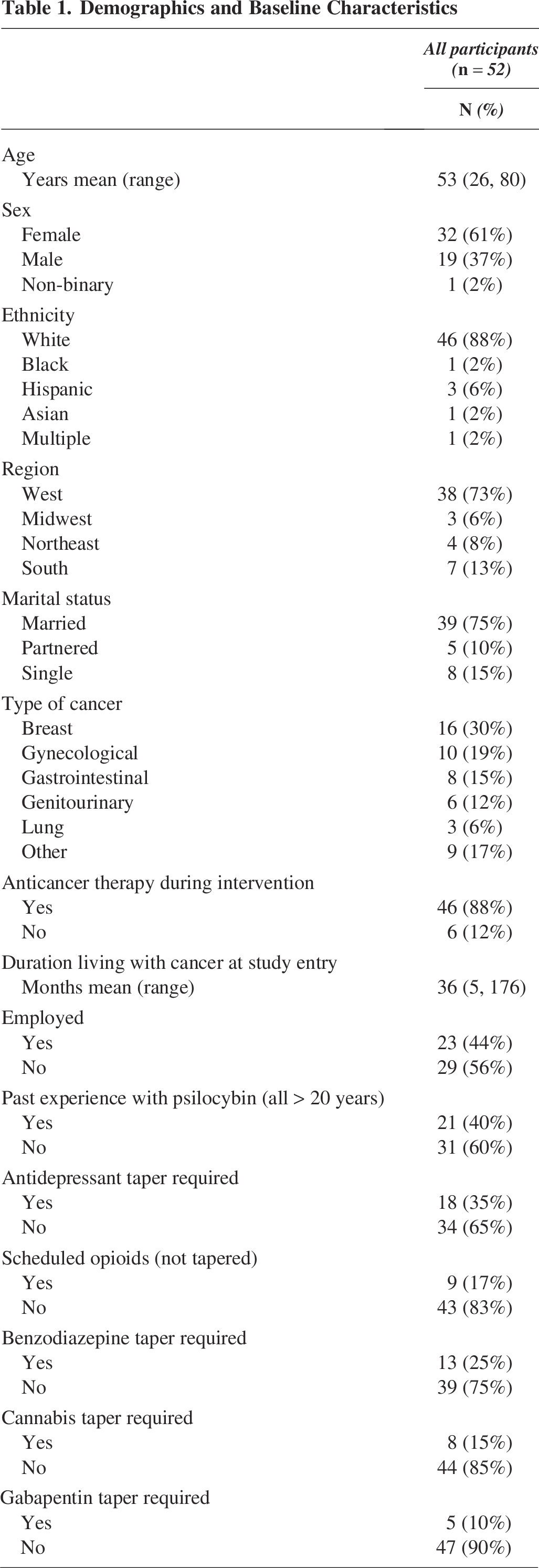
Anticancer therapy was ongoing for 46 (88%) participants, and included oral targeted therapy (23), IV targeted therapy (5), oral chemotherapy (3), IV chemotherapy (9), immunotherapy (7), and oral anti-hormonal therapy (10). Two patients had previously treated brain metastases (one with gamma knife and one with whole brain radiotherapy). Psychological or spiritual care had been provided by a palliative care clinician or counselor for 45 participants (74%). None were enrolled in hospice at study entry. Participant performance status was ECOG 0 for 5 (10%) participants, ECOG 1 for 43 (83%) participants, and ECOG 2 for 4 (8%) participants.
Medications requiring taper
Eighteen (35%) participants were taking antidepressants for cancer-related depressive symptoms and tapered prior to the retreat. Three patients were taking medications for Attention Deficit / Hyperactivity Disorder (ADHD), which they stopped 1 day prior to the retreat. Seven (13%) participants reported some use of cannabis products and were advised to discontinue them. Among cannabis users, all five reported using it for sleep. One participant began using high-dose cannabis in the month prior to the retreat because of worsening anxiety after tapering their sertraline, without informing the investigators.
Medications allowed for symptoms
Participants’ ongoing treatments for pain included: opioid-responsive pain, for which scheduled and breakthrough opioids were used by 9 (17%), allowed during the psilocybin session and not tapered; neuropathic pain for which a gabapentoid was used and tapered, 5 (10%); 2 had been treated with lutetium radioligand therapy more than 4 weeks prior to study entry.
Past experience with psilocybin included 21 (40%), who reported using “magic mushrooms” as young adults in high school or college. No participant reported a psilocybin experience within the past 15 years, including microdosing, or since their cancer was diagnosed (Fig. 2).
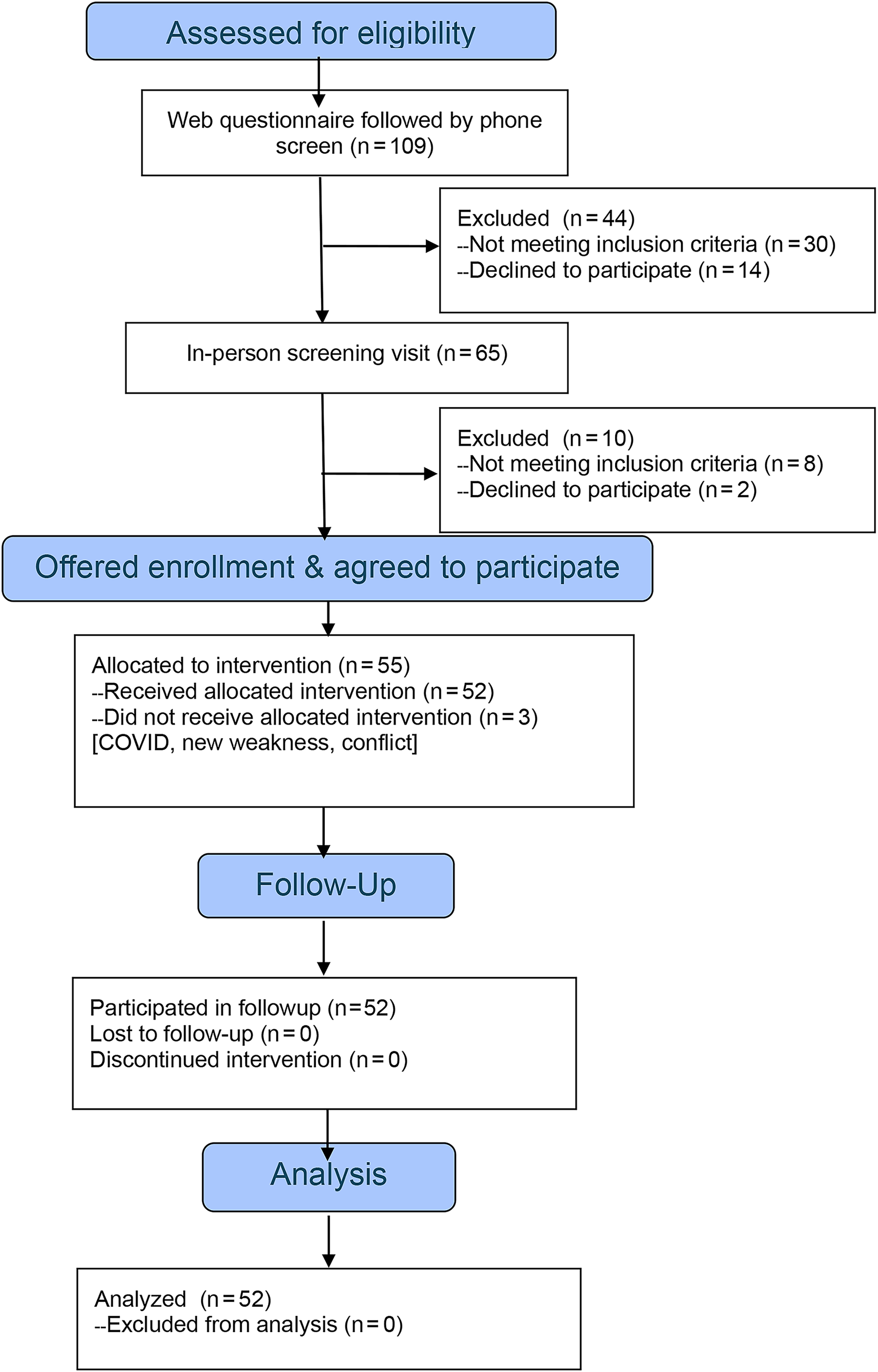
CONSORT (COnsolidated Standards Of Reporting Trials) diagram.
Cohort size
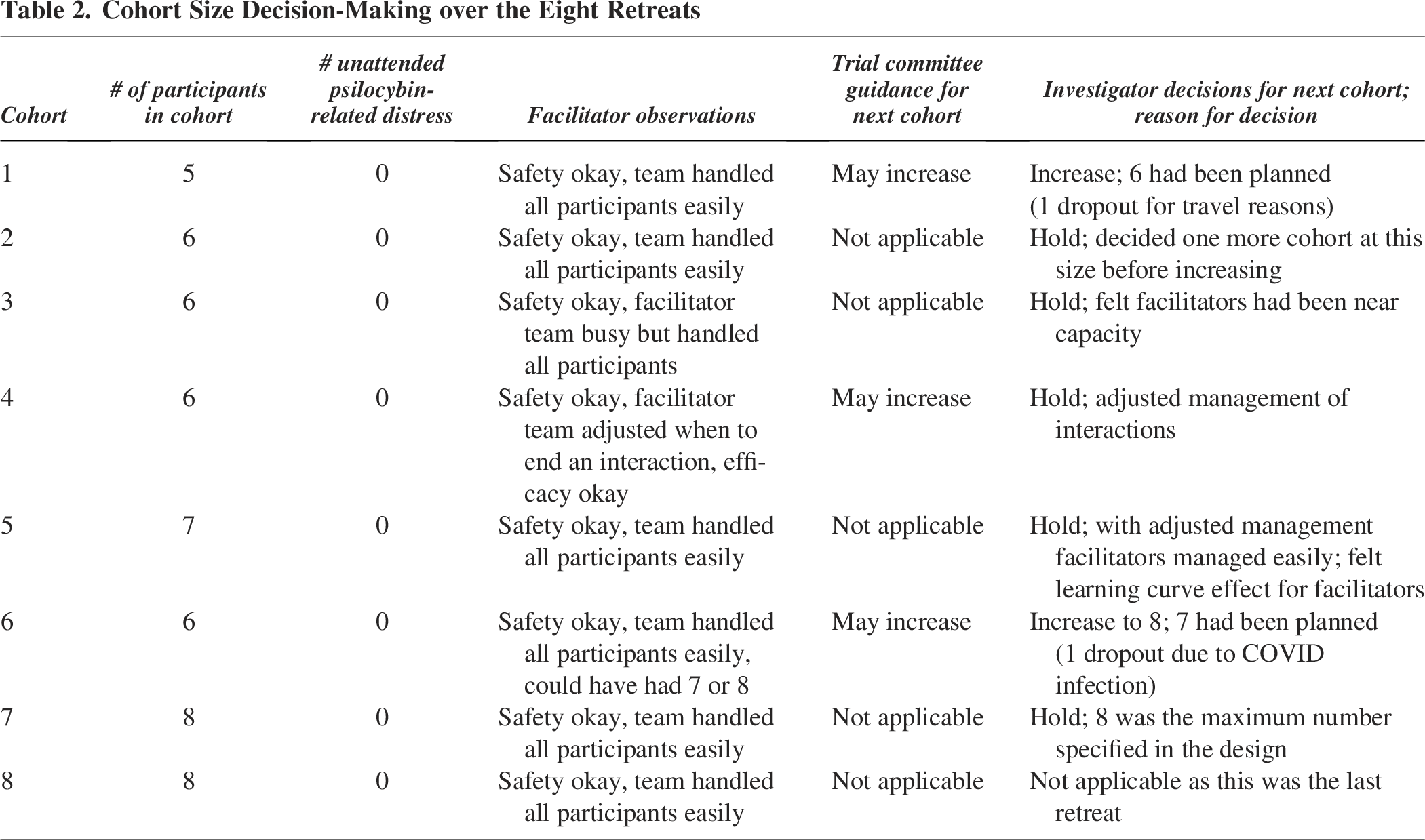
The trial design prespecified that all retreats would have four core facilitators and two backup facilitators, with the number of participants per cohort varying according to safety outcomes. Over the eight cohorts, the number of participants increased from five to eight (Table 2). The number of participants per cohort who actually attended a retreat was as follows: Cohort 1 (C1) = 5 participants; C2 = 6; C3 = 6; C4 = 6; C5 = 7; C6 = 6 (there was a last-minute dropout); C7 = 8; C8 = 8. Note that 55 participants enrolled, of whom 1 withdrew before the intervention started, 1 withdrew just before the Cohort 1 retreat, and 1 withdrew just before the Cohort 6 retreat, leaving 52 participants who completed the intervention.
Cohort Size Decision-Making over the Eight Retreats
Safety outcomes
Primary safety outcome
For the primary outcome of “unattended episodes of participant distress” during the psilocybin session, when more than four participants required core facilitator intervention, not a single instance was recorded.
Other safety outcomes
The questions regarding participants’ perceptions of facilitator availability and safety during the psilocybin session specifically were as follows: (1) Were there ever times when you felt you did not get the attention from the facilitators you needed to be safe? (No, 100%); (2) Were there ever times when you were having difficulty and the facilitators did not respond adequately? (No, 100%); (3) Were there ever times when a facilitator talked to you in a way that you found intrusive or unwanted? (No, 100%); (4) Were there ever times when a facilitator touched you in a way that you found confusing or unwanted? (No, 100%); 5) As you look back now, do you feel that other participants were supported adequately by the facilitators? (Yes, 100%).
Adverse events
There were no serious adverse events on the psilocybin day (Table 3), including for the two participants with brain metastases. Use of scheduled opioids did not result in adverse events. Of the two patients who experienced malaise as the psilocybin session ended, one was later found to be using high-dose cannabis until the day before, unreported to study staff, and one tested positive for Coronavirus (COVID) infection the following day (no other participants or study personnel acquired infections; all had a negative COVID test on arrival at the retreat). Of the two patients experiencing nausea, one was treated with ondansetron (an anti-nausea medication) with no benefit. On the day after the psilocybin session, one patient (with a history of migraines) had a migraine and used their prescribed sumatriptan with relief.
Adverse Events Not Tabulated in Table 2
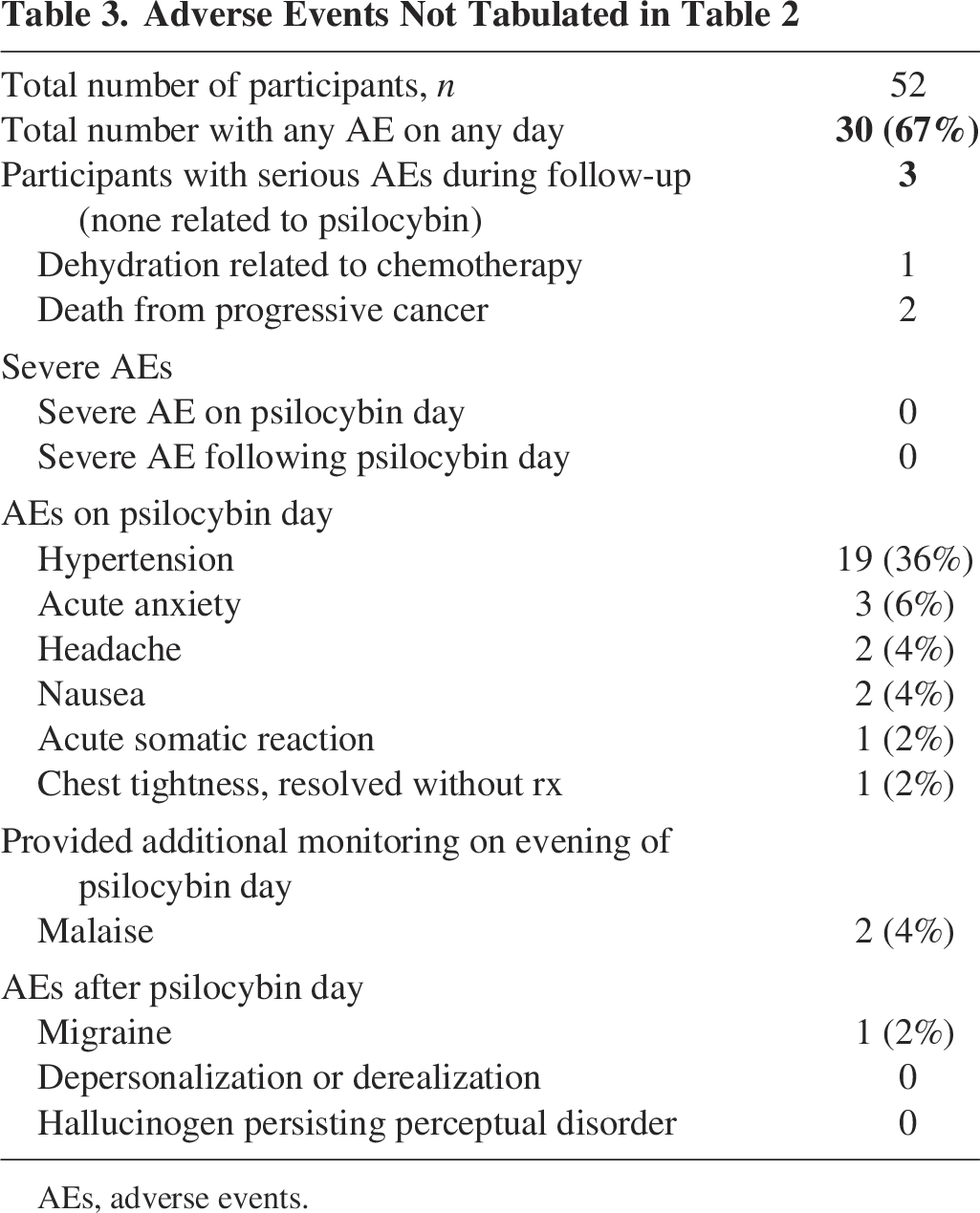
AEs, adverse events.
After the psilocybin session, there were three serious adverse events, none related to the Group Retreat Psilocybin Therapy: one patient was hospitalized for chemotherapy-related dehydration 7 days after the retreat; two patients died of progressive cancer before the last followup at D+180. There were no adverse events related to preparation or integration sessions. There were no instances of suicidality. There were no participants who experienced depersonalization, derealization, or hallucinogen persisting perceptual disorder.
Efficacy outcomes
Primary exploratory efficacy outcome: change in the mean HADS score
The mean (standard deviation) HADS baseline D −14 total score among all treated participants was 17.5 (5.99); at D +28, the mean HADS total score was 10.21 (6.31) with a mean decrease from D −14 to −7.29 (95% confidence interval, −9.33, −5.25; SD ± 7.33; p < 0.0001), indicating an improvement in symptoms of anxiety and depression. The mean change in HADS total score from D −14 to D +56 was −7.57 (6.95), to D +84 was −7.21 (6.90), and to D +180 was −6.49 (6.49).
Other exploratory efficacy outcomes
The DADDS mean D −14 total score was 35.1 (range, 3–70); at D +28, the mean DADDS was 21.1, with a mean decrease of −14.02, suggesting a decrease in distress related to thoughts of death and dying. The mean change in DADDS score from D −14 to D +180 was −13.19.
The NIH-HEALS mean D −14 score was 116.8 (range 86–153); at D +28, the mean NIH-HEALS was 130.4, with a mean increase of 13.28, suggesting an improvement in psychosocial function. The mean increase from D −14 to D +180 in the NIH-HEALS score was 13.28.
The DS-II mean D −14 score was 13.2 (range 2–32); at D +28, the mean DS-II was 6.8 with a mean decrease of −6.33, suggesting improvement in demoralization. The mean decrease from D −14 to D +180 in the DS-II score was −5.47.
The FACT-G mean D −14 score was 62.3 (range 33–93); at D +28, the mean FACT-G was 74.1, with a mean increase of 11.81, suggesting improvement in quality of life. The mean increase from D −14 to D +180 in the FACT-G score was 9.85.
Retreat experience process
To describe facilitator interactions, we developed a distinction during the study between “simple” and “complex” interactions. In a simple interaction, the participant maintains adequate self-regulation through a strong emotion or difficult experience, and the facilitator provides non-directive presence or empathic support. In a complex interaction, the participant shows impaired self-regulation, and the facilitator initiates directive intervention to support emotional expression, reduce distress, or ensure safety. The average number of simple + complex facilitator interactions per participant for all cohorts was 8.1, and most of those interactions were coded as simple (average 5.9). While 22 (42%) participants had zero complex facilitator interactions, 20 (38%) had at least one complex facilitator interaction lasting ≤ 45 min, and 10 (19%) had a prolonged complex facilitator interaction lasting > 45 min (with facilitators rotating about every 30 min). Figure 3 shows the average number of simple + complex facilitator interactions per cohort for all eight cohorts combined over each 15-min segment of their psilocybin session. Although the cohorts had different numbers of participants, the number of facilitators was fixed, so these numbers represent facilitator demand. The Supplementary Data include a heatmap showing simple + complex interactions for each cohort.
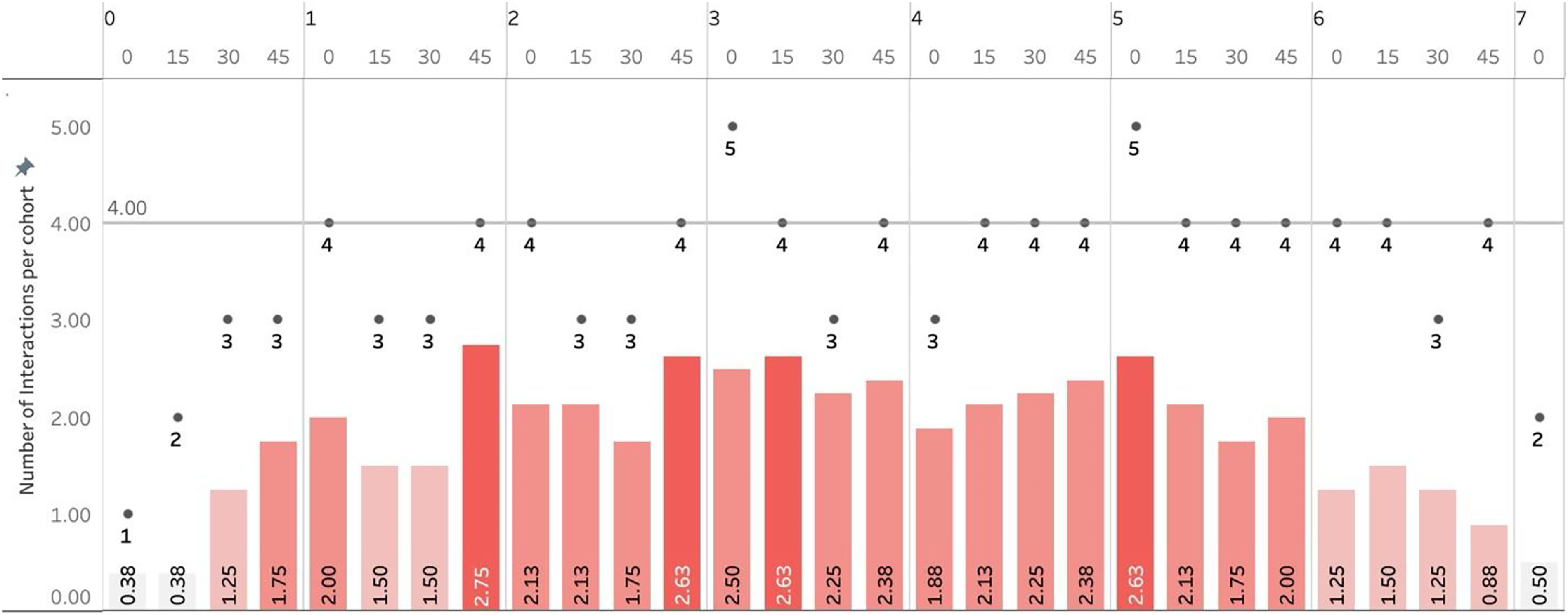
Facilitator interactions over time for all cohorts. Facilitator interactions for each 15-min interval during the psilocybin session. All sessions had four core facilitators and two backup facilitators. Each bar shows the average number of facilitator interactions per cohort for each 15-min segment of a psilocybin session, where time = 0 is when psilocybin was administered, and time = 7 h is the end of the session. The required blood pressure measurements are not included in these data. The color scale of the bars reflects the average number of facilitator interactions, where the color white indicates the lowest value, and the dark red indicates the highest value. The black dots represent the maximum number of facilitator interactions observed in all eight psilocybin sessions. Both instances where five facilitator interactions were recorded within a 15-min period did “not” qualify for the primary safety outcome because in both cases at least two of the facilitator interactions did not require the entire 15-min period, so that no backup facilitators were called in.
On the MEQ30, participants reported high levels of mystical-type psilocybin experiences. The mean (±SD) total MEQ30 score was 3.61 ± 0.97. Subscale means were: 3.55 ± 1.02 for Mystical, 3.57 ± 1.16 for Positive Mood, 3.81 ± 0.82 for Transcendence of Time and Space, and 3.63 ± 1.16 for Ineffability. Overall, 64.7% of participants met the criterion for a “complete mystical experience” as defined by Barrett. 36 The MEQ30 mean, raw total score was 108 ± 29.1. Participant reflection: “I wrestled with the idea of death and it didn’t seem possible to die. It felt like my body could die, but my feelings could never die and, I know this sounds silly but I realized that death is love.”
On the Communitas Scale, participants reported strong feelings of collective connection and shared experience. The mean (±SD) total Communitas score was 56.5 ± 10.0. (The instructions for the Communitas Score instructed participants to rate only the psilocybin session.) Participant reflection about the group: “There is a lot to be gained…just being willing to engage and be vulnerable—this is awesome.” Another reflection: “I love the whole idea of the group and all that we went through and the intimacy that we had.”
On the Challenging Experiences Questionnaire (CEQ), participants reported moderate levels of difficult experiences. The mean (±SD) total CEQ score was 1.60 ± 0.93. Subscale means were 1.70 ± 0.99 for Fear, 1.38 ± 1.29 for Grief, 1.62 ± 0.84 for Physical Distress, 1.37 ± 1.21 for Insanity, 1.50 ± 1.24 for Isolation, and 2.61 ± 1.16 for Death. The mean, raw total score was 41.7 ± 24.1. Participant reflection: “I felt like I was twisting into the ground…I got scared, I was freaking out, I wasn’t ready yet…”
On the EBI, participants reported substantial emotional breakthrough, with a mean (±SD) score of 70.0 ± 23.0. Participant reflection: “I objectified my cancer and wanted to be angry at it and yell and scream and then started laughing at how absurd that was. So I gave it a hug and loved and forgave.”
While we did not have an instrument to measure the effect of ritual, many participants described the ritual elements as contributing to a sense of calm and shared purpose, which helped them feel prepared for their psilocybin experience and integration. Participant reflection: “I’ve always been, well, [the ritual elements] are a hokey kind of thing, right? But I really liked the exercise of putting what we wanted to leave behind in the rock.”
Discussion
We conducted this Phase 1/2 study of the Group Retreat Psilocybin Therapy to examine safety outcomes and exploratory efficacy outcomes using an intervention design that brings in elements of nature, ritual, and ceremony adapted for participants who are medically complex and largely psychedelic-naïve. In particular, we sought to identify a safe facilitator-to-participant ratio to be used in future studies that could potentially increase access, while taking safety, efficacy, and logistical considerations into account.
The safety outcomes were the most important, especially given the setting outside a medical facility, and demonstrate that Group Retreat Psilocybin Therapy is safe and feasible. Over the course of eight retreats, we encountered no serious adverse events attributed to the intervention, and not a single instance of “unaddressed psilocybin-related distress” was observed during a psilocybin session. The adverse events we did encounter during the psilocybin sessions were managed mostly with facilitator interactions. We did encounter a learning curve for the facilitator team, which is reflected in Table 2 showing how cohort numbers were increased.
The efficacy outcomes for the Group Retreat Psilocybin Therapy, while exploratory, are promising, even though our participant sample differs from other published studies with cancer patients. For example, the randomized study of psilocybin for cancer patients with anxiety and depression by Ross et al. 3 involved 29 patients, of whom 10 (34%) had stage IV cancer; in this study, 52 (100%) had metastatic cancer, with 2 dying of progressive cancer before the 6-month follow-up was complete. Ross et al. do not report how many participants had ongoing anticancer treatment; in this study, 88% were undergoing anticancer therapy that had to be paused or adapted so they could participate. Despite these differences, the efficacy of this study may be comparable. In Ross et al., the exact HADS total scores are not reported, but examination of the figures indicates that for participants who were randomized to receive psilocybin first, their HADS total scores were approximately 12.5 at baseline and 6.0 at the 6-week time point, for a change score of approximately −6.5 (Fig. 4). Our results using the same measure (HADS total) show a 4-week (D +28) change score of −7.3, similar in magnitude to Ross et al., although this is a historical comparison, and the study population in that study is not exclusively Stage IV metastatic. For the HADS, a minimally important difference (MID) of approximately −2.0 points has been established, indicating the threshold for clinically meaningful improvement.38,39 The estimated HADS total change score of approximately −6.5 in Ross et al. and the −7.3 change observed in our study at Day +28 both exceed this MID by more than threefold, supporting the conclusion that these reductions represent clinically significant improvement rather than solely numerical change. Although this comparison is historical and the Ross et al. population was not exclusively metastatic, the magnitude of improvement observed across studies is similar and clinically meaningful.
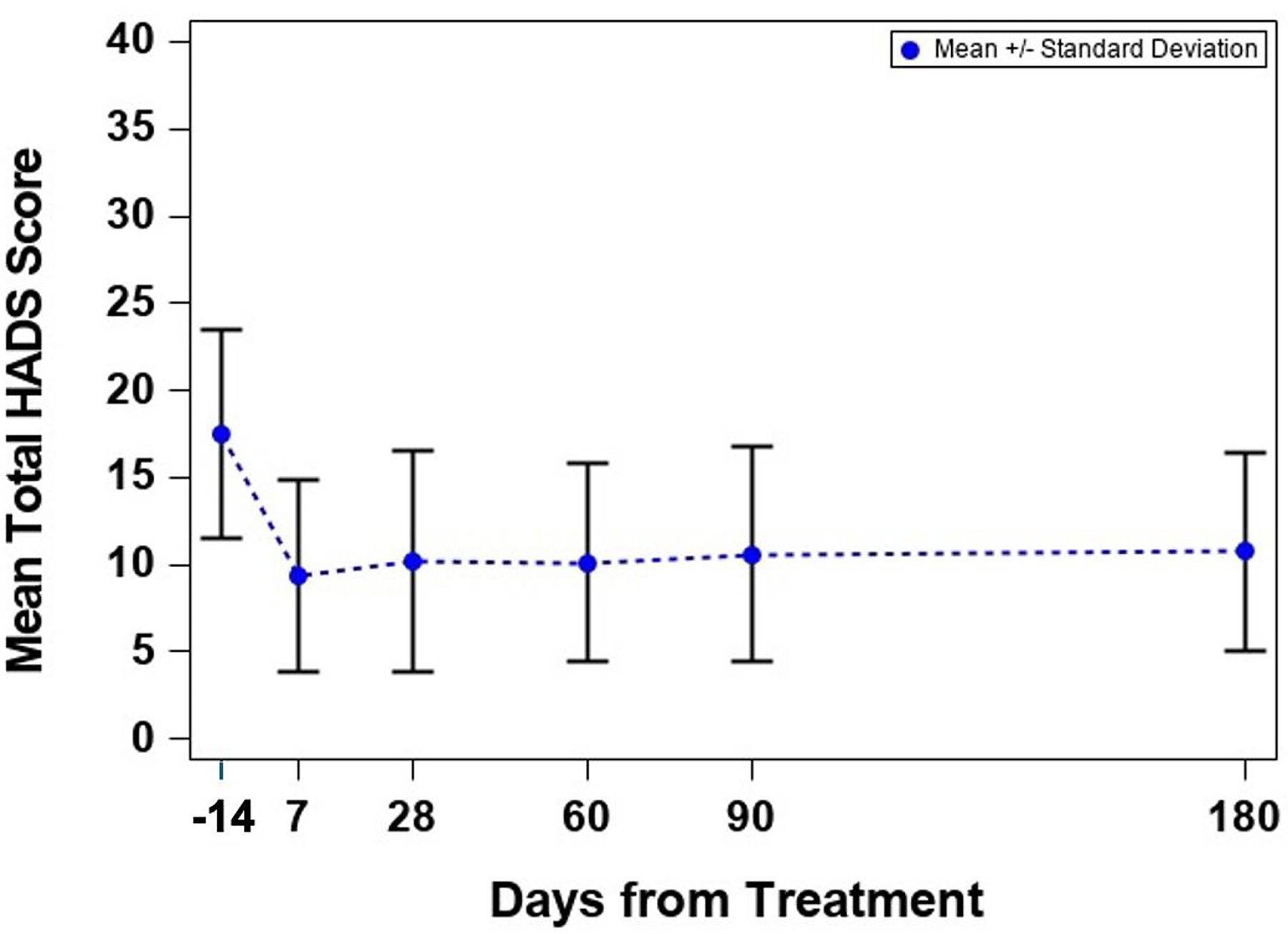
Primary exploratory efficacy outcome (HADS) for all participants (can be combined with 5 panels in Fig. 5 for one 6-panel figure). HADS, Hospital Anxiety and Depression Scale.
The strengths of this study are that the intervention was manualized, used facilitators with relevant experience, and followed a predefined scheme for increasing the number of participants per cohort. Another strength is the careful tracking and documentation of facilitator interactions. Finally, the exploratory efficacy outcomes used measures that are validated and being used in other studies, and the FACT-G provides a benchmark for comparisons to future studies.
Overall, Group Retreat Psilocybin Therapy merits further study. Compared with an individual setting, the group format makes different demands of participants: They need to listen to other patient's stories about living with metastatic cancer and facing mortality that are somewhat different than their own; they need to interact with the other participants; and they also need to interact with all the facilitators. An earlier individual study of psilocybin for patients with cancer reported mean MEQ scores of 60–70 (Fig. 5, exact scores not reported); in this study, mean MEQ score was 108. A study using the Communitas instrument in naturalistic settings with different populations reported a total score of 39.6 13 ; in this study, the Communitas score was 49.5. While these historical comparisons are not definitive, they suggest that this intervention offers an experience comparable in depth with individual psilocybin and a group experience comparable with what has been reported in naturalistic studies. However, there are likely patients for whom this group intervention or natural setting would not be suitable.
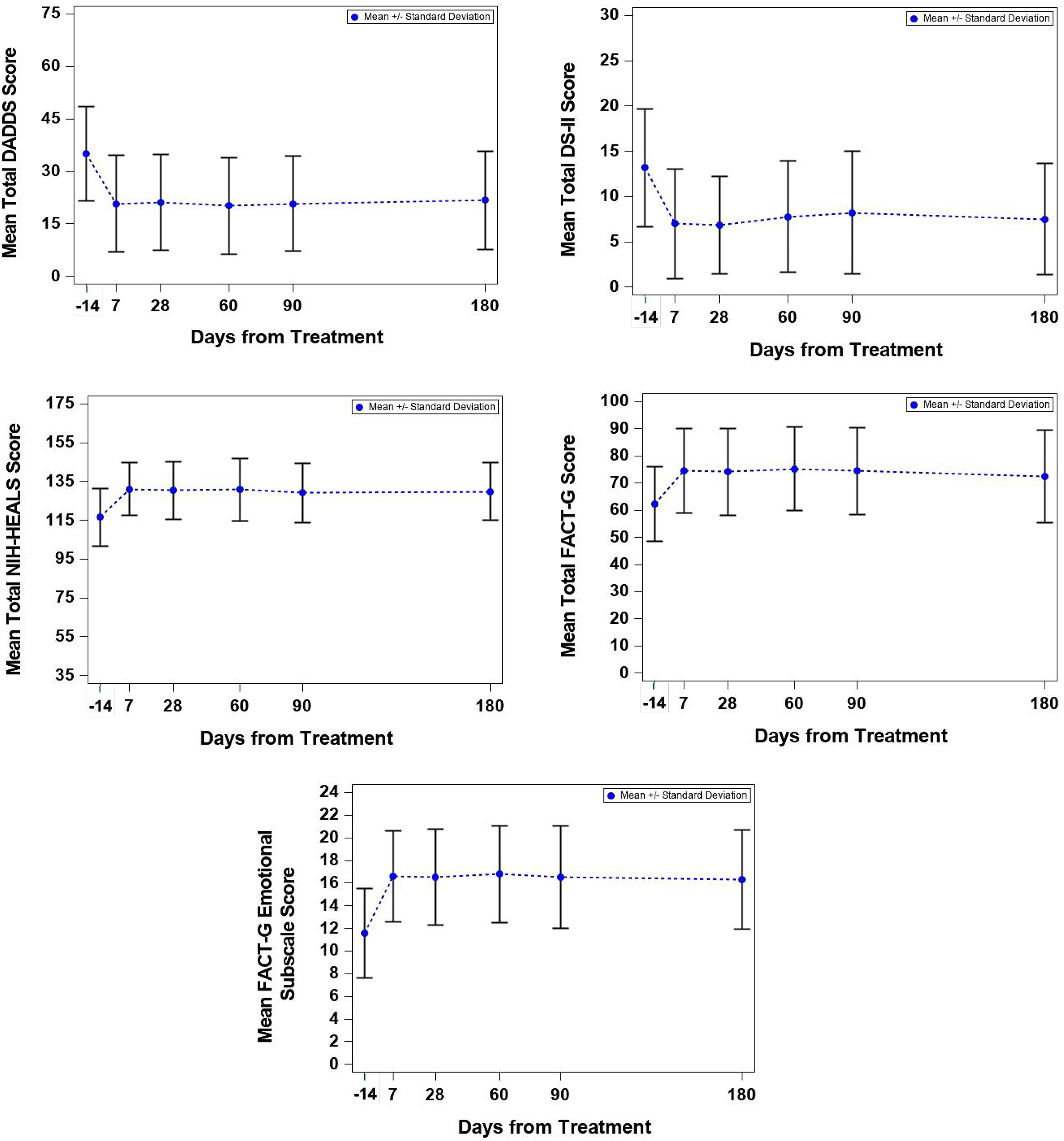
Exploratory efficacy outcomes for all participants.
This study also has limitations. The study involved a relatively small sample of patients with metastatic cancer, and there was no control group, so the generalizability of these findings is limited. Given the lack of safety data that exist for group psilocybin interventions, we felt it was important to establish safety as a first step. In addition, the study was conducted at a single site, with a cadre of facilitators who worked together repeatedly over a year. That may not be possible to replicate exactly, but we did manualize the study procedures and refine them continuously, so that materials have now been created to replicate and scale this intervention as well as train future facilitators. Finally, we acknowledge that the safety questions should be asked more than once after the retreat and that participants may have concerns about reporting safety issues to one of the facilitators. However, we now have data that the safety questions were clear and easily understood, and in future retreats, we will use them in an electronic format with additional timepoints.
Conclusion
Group Retreat Psilocybin Therapy was safe and well-tolerated, and exploratory measures show efficacy that is promising and merits further study. A group configuration of eight participants with four core facilitators can be safe for use in future studies with participants with serious medical illness.
Authors’ Contributions
A.L.B.: Conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—original draft and editing, supervision, funding acquisition. B.A.M.: Conceptualization, methodology, formal analysis, investigation, resources, writing—editing. L.L.T.: Investigation, data curation, project administration. K.B.: Formal analysis, editing. T.G.: formal analysis, editing. M.K.: Methodology. K.H.: Methodology, software, data curation. J.M.G.: Facilitation, editing. S.M.: Facilitation, editing. J.P.: Facilitation, editing. P.T.: Facilitation, editing. L.B.: Facilitation, editing. C.N.: Resources, facilitation, editing.
Footnotes
Acknowledgments
Patricia James. Maria Mangini ARNP. Sam Webster. Randy Morris, PhD. James Clifton. Nai Kaya. Daan Keiman, MA. Joan Halifax, PhD. David Hammond, PhD. Joong Kim, PharmD. April Cowgill, PharmD. Harmony Hill Retreat Center. Langley Fine Farms. Ripple Science. Reba Blissell. Amy Deyle, RN. Edward Gibbons, MD.
Author Disclosure Statement
No authors report conflict of interest.
Funding Information
The study was funded by the Steven and Alexandra Cohen Foundation (Grant number PSYCH36). Psilocybin was provided by Filament Health.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.