
Abstract
Background
Speech and language therapy services for children with disabilities in Ireland have undergone a significant change in the recent past. There are many reports of parent views about access to interventions, but to date the perspectives of SLTs on their role has not been established.
Objective
This study aimed to gather the experiences of SLTs working in CDNTs regarding their ability to deliver interventions.
Method
We circulated an online survey to Irish clinicians and invited them to attend online focus groups or interviews to discuss their perspectives and experiences in delivering services and interventions within reconfigured services. The results were analysed quantitatively using descriptive statistics and qualitatively via thematic analysis.
Results
Twenty eight SLTs completed the full survey and five people took part in the focus groups/ interviews. The clinicians reported to be spending just a quarter of their time providing interventions, and most were not satisfied with their intervention provision. They discussed the challenging working environment, including large and varied caseloads, unclear policies, and a lack of clinical supervision which were impacting on their ability to provide a range of interventions, their relationships with parents and colleagues, and overall job satisfaction.
Conclusions
The study paints a picture of a very challenging work environment for SLTs in CDNTs. There remain significant challenges for how services are configured and delivered to retain staff and best serve families of children with disabilities. These need to be considered by those responsible for planning and organising disability services as a matter of urgency.
Background
Evolving population, clinical and societal needs are creating an impetus for healthcare reconfiguration across many countries (Martin et al., 2018). These changes are particularly pertinent issue for children’s disability services where the number of children requiring services is growing exponentially. For example, 42,000 Irish children required access to disability services in 2013, a figure that grew to 70,000 by 2023 (HSE, 2023). Globally, disabilities affect over 316 million children and adolescents worldwide (World Health Organization (WHO) & the United Nations (UN) Children’s Fund, 2023), approximately 13% of the child population (UNICEF, 2023). Contributing factors include increased survival of premature infants (Heuvelman et al., 2018) and knowledge of neurodevelopmental difficulties (Houtrow et al., 2014). Many of these children and young people will require regular and lifelong access to specialist healthcare services to reach their potential in terms of learning, independence and communication skills (WHO, 2011). In a review of services for children with speech, language and communication needs (SLCN) in the UK (Bercow, 2008), high variability and lack of equity in services was identified. Recommendations that followed including early identification and intervention, joint working, and a continuation of services around the family, particularly at key transition stages. The report was reviewed in 2018 amid a landscape of service reform in the UK (ICAN/RCSLT, 2018). Some of the positive changes that were noted at that time were increased evidence for SLCN through research, consistent funding to develop the workforce as well as a national AAC service. However, negative aspects included cuts to services and a loss of senior and specialist therapist roles. Overall, participants reported a poor experience of speech and language therapy (SLT) services which was reported to be based on resources rather than requirements. Although such a review has not taken place in Ireland, in 2001 the Bacon report (Bacon and associates, 2001) into labour market requirements for therapy services indicated that and 328% increase was needed in the existing supply of speech and language therapists by 2015. This report resulted in increased training places for SLTs in Ireland, some of whom went on to be employed in disability services.
A key recommendation of the Global Report on Children with Developmental Disabilities (WHO & UN, 2023) was the need to strengthen the capacity of disability services to provide responsive, inclusive and people-centred evidence-based care across countries. However, disability services do not exist in a vacuum and are impacted by events such as the 2008 international financial crisis and subsequent austerity measures many of which continue to have an impact on disability services in countries such as the United Kingdom and Ireland (Acheson, 2023). Looking at Ireland specifically, a programme of disability service reconfiguration was commenced in 2009. For context, Irish children’s disability services are provided by both the national healthcare provider, the Health Service Executive (HSE), and a range of non-statutory agencies. Historically, service provision has been piecemeal with service access determined by the nature of disability and geographical location, often described as a postcode lottery (HSE, 2023). To address these disparities, Progressing Disability Services for Children and Young People (PDS) was developed as a national programme of reconfiguration (Cantan & Bolger, 2017). Implementation commenced in 2009 and was completed in December 2021, with a total of 91 disability teams working as Children’s Disability Network Teams (CDNT) (Health Service Executive, 2023). Initiated in a financially austere climate, PDS aimed to reorganise existing staff and resources without any additional resourcing (National Disability Authority, 2015).
Since its initiation, several challenges have beset the process of reorganisation to CDNTs, including issues relating to clinical supervision and line management structures (Irish Association of Speech and Language Therapists (IASLT, 2022)), with an associated and pervasive challenge related to staffing and retention (HSE, 2023). Initially no additional resources or staffing were provided as part of the reconfiguration process and clinicians were assigned significantly larger caseloads with a much greater diversity in terms of clinical needs (Association of Occupational Therapists Ireland, 2023) . Insufficient resources, inadequate clinical supervision and unclear clinical pathways has led to lengthy waiting times for access to services and in some instances reduced access to services compared to before reconfiguration (Buckley et al., 2021). Allied professional bodies such as the Association of Occupational Therapists Ireland (2023) also reported that staffing and caseload numbers are negatively impacting occupational therapy practice in CDNTs. In late 2023, the HSE acknowledged difficulties recruiting staff, retaining staff and attrition of experienced staff as key factors impacting PDS (HSE, 2023). Staffing shortages included a national average vacancy of between 34% and 60% in CDNTs and anecdotal reports of ‘higher than usual turnover amongst CDNT experienced, highly skilled staff’ (Health Service Executive, 2023). It is likely that poor job satisfaction is associated with staffing problems for these healthcare professionals. Job satisfaction significantly impacts staff retention among healthcare professionals, especially for non-profit public services such as disability services, which are essential for a country’s provision of healthcare services and the population itself (Karaferis et al., 2022).
Providing intervention is a core area where clinicians use their professional skills and clinical autonomy to meet the needs of children on their caseloads. Intervention is a broad term and can be conceptualised across different tiers or levels. For current purposes the definitions developed by Ebbels et al. (2019) is used to illustrate the different levels: • Tier 1: training parents and/or teachers to provide intervention designed to promote the development of all children (universal) • Tier 2: training provided to parents or teachers of children who have identified risk factors (targeted) • Tier 3(a): individualised intervention designed by the clinician and delivered by parents and/or teachers with coaching from the clinician (e.g. Parent–Child Interaction Therapy (PCIT), • Tier 3(b): individualised direct intervention by the clinician supported by collaboration with parents and/or teachers (specialist)
Post reconfiguration it has been indicated that much of the intervention provided is at tier 2 and 3a, but limited in terms of individualisation and direct clinician-child interaction (Inclusion Ireland, 2022). This lack of direct intervention is most likely due to large caseloads, staffing issues, limited experiences for building collaborative relations (Carroll, 2009) and flaws in understanding and implementing the CDNT model. An exacerbating factor is that many services were reconfigured during the COVID-19 pandemic with resultant deployment of clinicians and restricted services leading to a significant backlog from the beginning. Several parents have vocalised their dissatisfaction with the reconfiguration of children’s disability services (Dwyer, 2022); however, the views of clinicians working in the area have not been documented. Based on their own professional and clinical experience, the authors identified speech and language therapists (SLTs) working in children’s disability teams as one population who could provide an insight into this area. Moreover, establishing the views of SLTs currently working in the area could help to identify the issues that are affecting staff recruitment and retention, and develop potential solutions to this problem. Therefore, this research firstly aimed to establish the views of SLTs working in CDNTs around their work-related activities, and more specifically their views on their intervention provision.
Research Questions
1. How are speech and language therapists currently working in CDNTs allocating their time across different work-related activities? 2. How satisfied are they with their time for intervention? 3. How do SLTs perceive the effectiveness of their intervention delivery in CDNTs and how satisfied are they with their intervention provision overall?
Methods
This study used a sequential, mixed methods design, whereby data was initially collected via a survey (quantitative and qualitative data) with subsequent focus group and interviews (Ivankova et al., 2006) . The survey sought to establish both quantitative and qualitative data around time allocation to clinical tasks and these aspects were further explored through invitation to take part in focus groups or interviews. These tools are provided in Supplemental Information 1 and 2. Ethical approval was granted by the [removed for anonymisation]. We followed the consolidated criteria for reporting qualitative studies (COREQ, Tong et al, 2007) as outlined in the Supplemental Table 1.
Sampling and Recruitment
Purposeful and snowball sampling was used as recruitment materials were sent to relevant gatekeepers such as the IASLT and shared on these and personal social media platforms (i.e. X and Instagram) using relevant tags. SLTs currently working in a CDNT or who had left within the last 12 months were eligible to participate.
Data Collection
Phase one involved a bespoke questionnaire, with items informed by relevant literature, health service knowledge and clinical experience. The questionnaire was piloted with a clinician who had worked in CDNT services in the past, and small changes to clarify the wording of questions were added. The questionnaire comprised closed and open-ended questions and was open for a 2-week period hosted via Survey Monkey. The data from this phase informed the topic guide for phase two which was a qualitative study that aimed to expand upon the data provided in Phase 1. All participants who completed the survey were invited to take part in phase two which involved online focus groups and individual interviews (through Microsoft Teams) which were audio recorded and run separately by both authors. These lasted for approximately 60 minutes. The authors are female academics working in Irish Universities with PhD qualifications. Both had worked in children’s disability services in Ireland prior to moving into academia. Their previous experience and current education of clinicians who are/will be employed in CDNTs lead to their interest in researching this topic. The researchers knew the participants on a professional capacity but had not established a relationship prior to the study. Both authors have extensive experience in completing interviews and focus groups from their academic work.
Data Analysis
Quantitative questionnaire data was analysed via descriptive statistics. Focus group and interview data was analysed via the six-phase process of thematic analysis as outlined by Braun and Clarke (2021) by both authors who are experienced qualitative researchers that have taught and used qualitative methodologies. Both authors transcribed the interviews verbatim and re-read the transcripts. They then used an inductive approach by openly coding the statements and recording this in NVivo 12 software to support transparent and collaborative data analysis, with clear audit trails. To promote credibility and rigour, we used cross coding whereby both authors independently coded one focus group interview each and then compared them for consistency of coding. After this, the second author coded the final interview. Both authors generated initial codes and grouped these into themes based on agreed patterns relating to ideas. Themes and subthemes were then identified across the data and their core meaning agreed before looking for patterns in the data. At this stage, themes that overlapped were merged to identify more selective and meaningful themes, resolving any disagreements that emerged through discussion. Once the core set of themes and subthemes were agreed, the first author analysed the qualitative comments in the questionnaire data via content analysis using the coding framework identified in the focus groups and interview as the data was not sufficiently in-depth to justify thematic analysis (Vaismoradi et al., 2013). This was reviewed by the second author to ensure that the quotes were appropriate for the existing framework. All of the data was then integrated to develop an overall set of findings which best reflected participant experiences, weaving quantitative and qualitative data together into a cohesive narrative (Fetters et al., 2013).
Results
Participants
Although 107 people opened the survey, a total of 28 participants completed the full survey (26% completion rate). Most of the SLTs had worked in disability services for between one and three years (39%, n = 11); followed by more than 10 years (29%, n = 8); 5–10 years (21%, n = 3) and 3–5 years (11%, n = 3). More than half the group (61%) had worked in disability services prior to reconfiguration. There was variation in the length of time SLTs had worked in a reconfigured CDNT ranging from one month to eight years with an average of 2.5 years. All the SLTs worked with children aged 5–12 and almost all with children aged birth to five (96%, n = 27) and with children aged 12–18 (93%, n = 26) reflecting the extensive age group on their caseloads.
There were two online focus groups (two participants in each) and one individual online interview. The SLTs in the first focus group had worked in disability services for eight and 15 years, respectively, the latter having taken a career break in the last 12 months. The second focus group involved two SLTs, one who was working in disability for over 20 years the other for 18 months. The SLT who took part in the individual interview had been working in disability services for over 20 years before moving to private SLT work in the previous 12 months.
We will summarise our results by first presenting the quantitative data from the survey, followed by the results from the qualitative analysis.
Time Allocation
We first profiled the time SLTs reported to be spending on various clinical tasks over a typical month and the responses are contained in Figure 1. Percentage of time spent on tasks per month.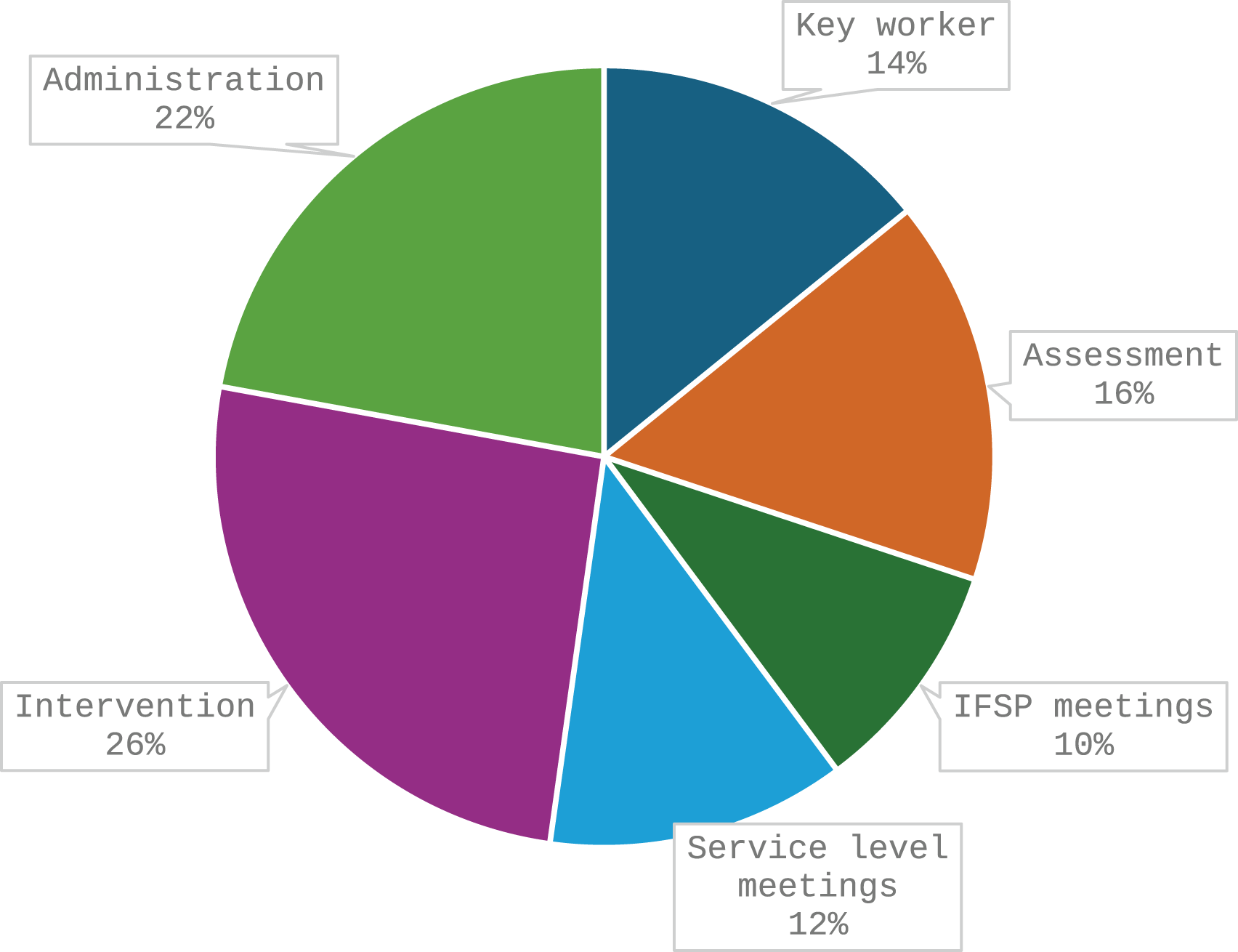
As can be seen, the SLTs reported spending about 25% of their time providing interventions, and 22% on administration tasks. An average of 16% of their time was spent on assessment, followed by key worker/ contact tasks (14%) and 22% combined attending Individual Family Service Planning (IFSP) and service level meetings. The respondents indicated that about 42% of time was spend on indirect and 32% on direct interventions.
Satisfaction With Intervention
The first set of survey questions asked participants how satisfied they considered themselves to be with various aspect of intervention provision (see Figure 2). To summarise responses, we combined results for those who selected ‘very dissatisfied’ with ‘dissatisfied’ and ‘very satisfied’ with ‘satisfied’. Participant satisfaction with various aspects of intervention.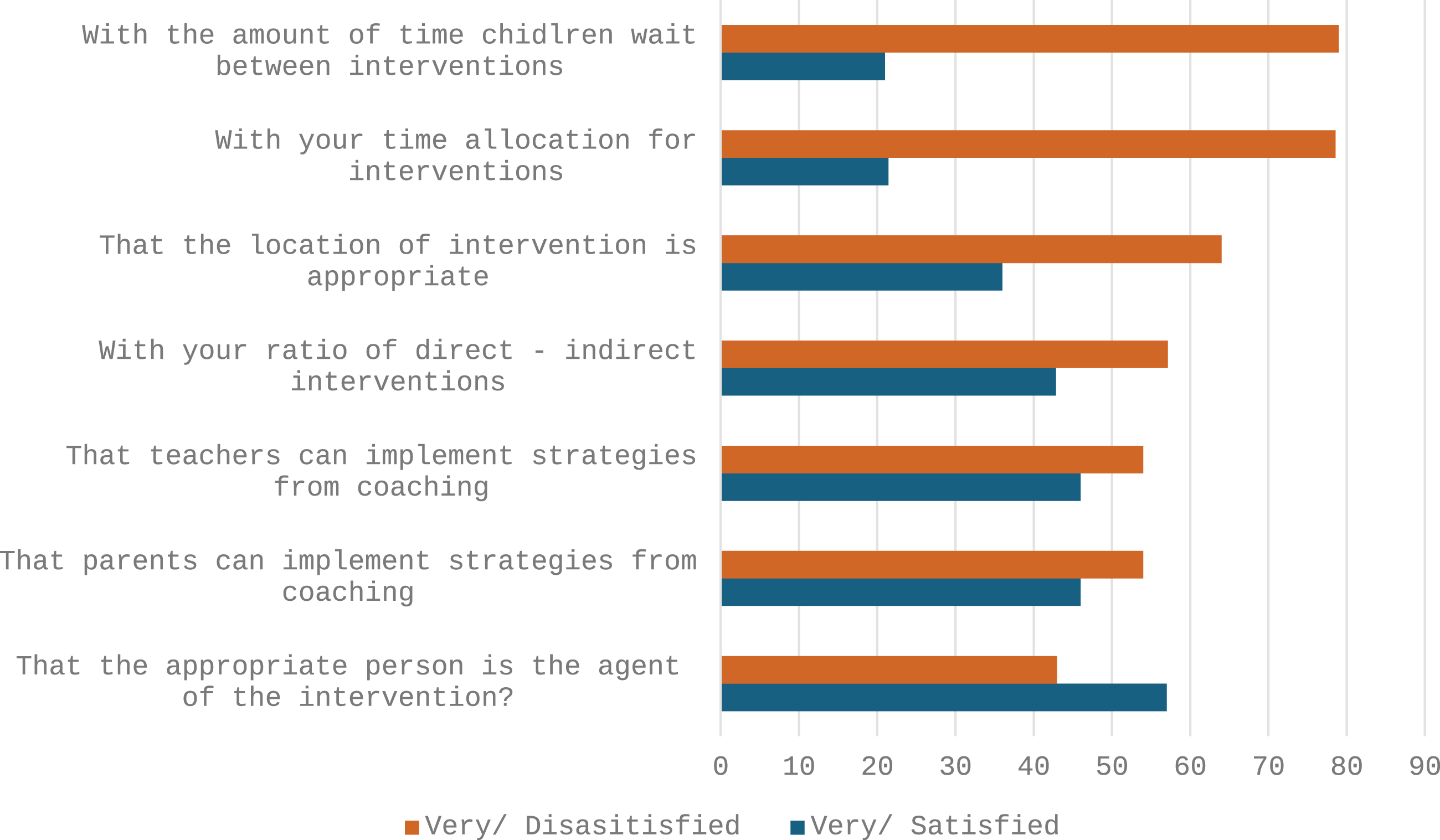
Most participants were very dissatisfied or dissatisfied with the waiting times between interventions (79%, n = 22), with their time allocated for interventions (79%, n = 22) and with the location of the intervention (64%, n = 18). Just over half of therapists were not satisfied with their ratio of direct to indirect interventions (57%, n = 16) while some were happy with this (43%, n = 12). Similarly, just over half of SLTs were not satisfied (54%, n = 15) that teachers or parents could implement intervention strategies although slightly fewer were satisfied (46%, n = 13). On the other hand, more respondents were ‘satisfied’ (57%, n = 16) than ‘not satisfied’ (43%, n = 12) that the appropriate person was the agent of the intervention.
Satisfaction With Time Allocated to Interventions
The SLTs then responded to questions about their satisfaction with the regularity they get to work with children, parents and teachers as summarised in Figure 3. Participant satisfaction with time allocation.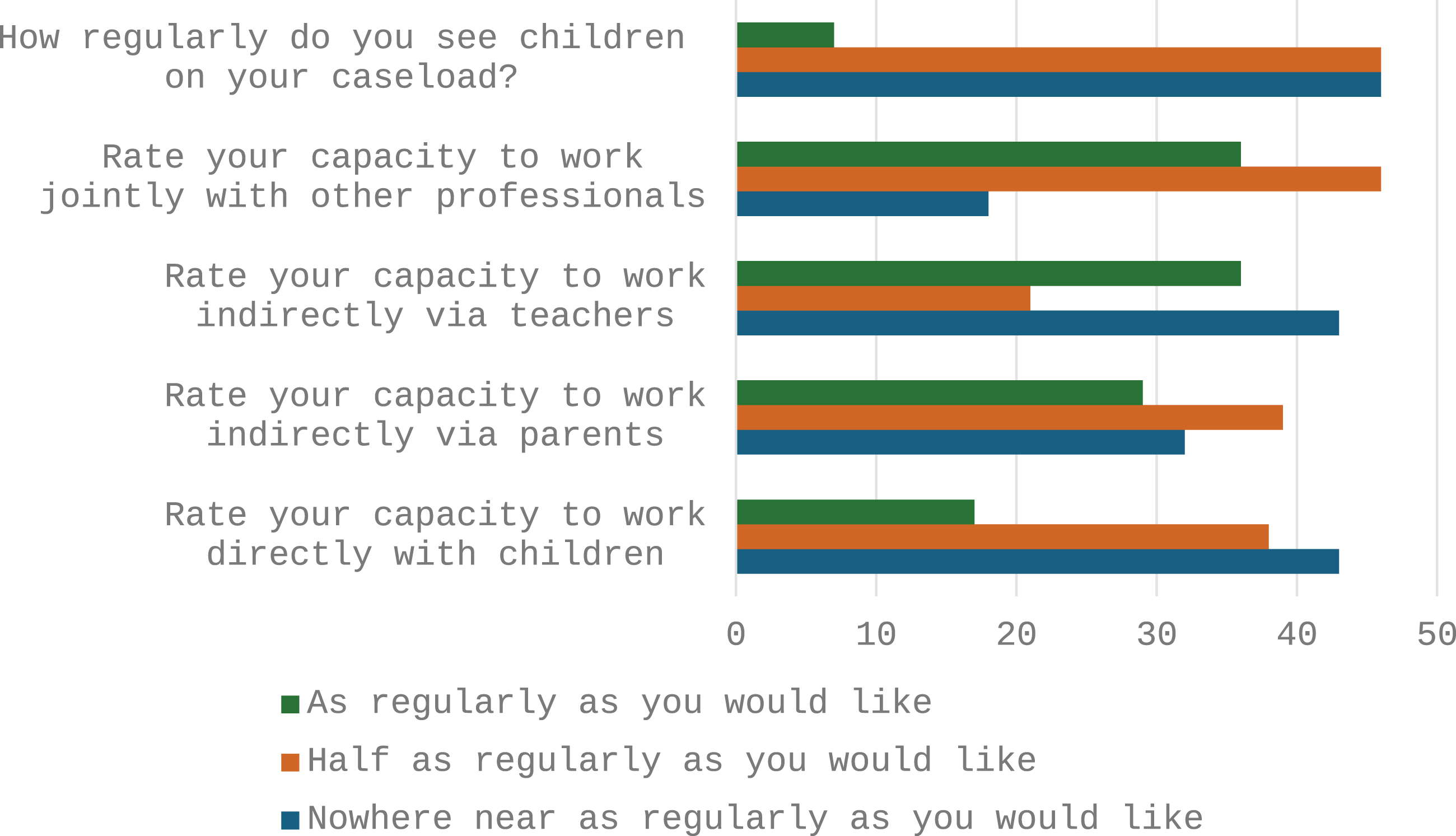
As can be seen, the majority of SLTs felt that they get to see children half (46%, n = 13) or nowhere near (46%, n = 13) as regularly as they would like. Just two SLTs (7%) considered that they saw children as regularly as they would like. When asked to rate their capacity to work directly with children, many SLTs (43%, n = 12) reported that they did not work with children as regularly as they would like and 39% (n = 11) half as regularly as they would like. We also asked about the time the SLTs had to work indirectly with parents to coach them on delivering interventions. Most SLTs reported that they did not work with parents as regularly as they would like (39%, n = 11) or nowhere near as regularly (32%, n = 9), although 29% (n = 8) were doing this as regularly as they would like. Similar responses were noted for working indirectly via teachers where the majority felt that this work was nowhere near (43%, n = 12) or half as regularly as they would like (21%, n = 6). Finally, when asked about how regularly they get to work jointly with other professionals, most felt this was not as regularly as they would like (46%, n = 13) and some nowhere near as regularly (18%, n = 5) while 35% (n = 10) did work with others as regularly as they would like.
Qualitative Data
Themes, Subthemes and Illustrative Quotes From Qualitative Data
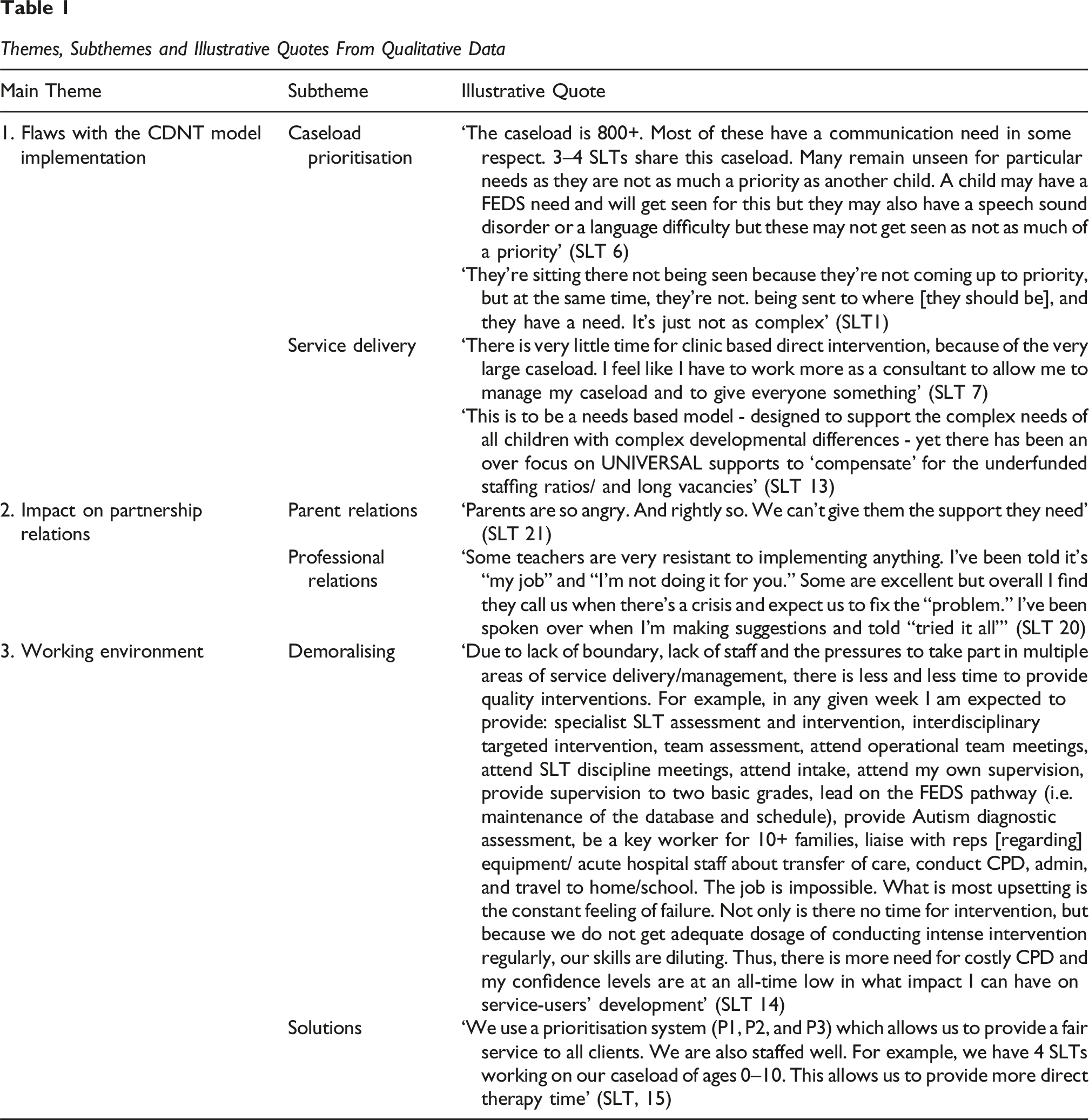
The first major theme related to the
The lack of clarity meant that a significant amount of time was wasted identifying whether a child should be on a Primary Care or a CDNT caseload. The SLTs felt that there was a lack of understanding at a policy and managerial level about what it means to have a child with complex needs, and how it is a lifelong disability. Therefore, the prioritisation and pathways model taken from HSE primary care services were not fit for purpose. One SLT said ‘The way policies have been developed, it’s been very much, that primary care model, statistics, how many families can you see, what’s the outcome? And in disability those type of structures can’t be applied because it’s so dependent on the individual child and family’ (SLT 3). Another SLT agreed when she said ‘even the ministers or politicians who are working within disability roles would go back to that very primary care model of “Oh, just get them their block of therapy and they’ll be happy, you know”… But it’s just putting a plaster over a massive wound. Like it doesn’t make sense’ (SLT 4). SLTs noted that children with Feeding, Eating, Drinking and Swallowing (FEDS) difficulties and AAC devices were considered ‘top priority’, but those with other communication difficulties including speech sound disorders were not, even though as one SLT put it ‘when we did speech work, we did have significant improvement’ (SLT 2). As well as being complex, they spoke about how broad their caseloads were. One SLT noted ‘Before [reconfiguration] you had a specific kind of case load with specific needs. Now it’s 0–18 and it can be in any area and we all know SLT is so broad and there’s no way you can be specialist, in every area’ (SLT 2).
The second subtheme around the contextual environment related to their description of the
The therapists also reflected on multidisciplinary working, which was inconsistent across teams and dependent on staffing levels. One SLT noted that before reconfiguration there had been time to provide a good MDT service in special schools, but as the change to the CDNT model did not come with a corresponding increase in staffing it meant that ‘we’ll give the same service to everybody, but it’ll be a watered down version and nobody will get anything of significance’ (SLT 2). Another SLT noted that ‘We have the capacity for joint working but it is very different to pre [reconfiguration], not a lot of sessions and it feels like therapists don’t get fully invested and keep things to generic discussions and quickly move to written recommendations for home rather than direct intervention’ (SLT 8).
The second major theme was the
The therapists also spoke of how the reconfiguration of services is affecting their
The third theme related to
During the discussions, the SLTs suggested
Discussion
The findings of this research paint a picture of a challenging work environment for SLTs working in children’s disability services. Clinicians who responded to our survey reported that they only spent one quarter of their time providing interventions, while almost half of their time was spent attending meetings and on administrative tasks. This time allocation to clinical tasks is unlike other studies of SLT practice, including a national survey in the United Kingdom that found SLTs there spent over half their time giving therapy (both indirect and direct; Pring et al., 2012). Most of the SLTs were dissatisfied with many aspects of CDNT model, including prioritisation, waiting times, time allocation, and location of services. When providing indirect therapy as a key aspect of their role, they were not satisfied that they could individualise it to children and their families or allocate sufficient time to deliver it. They reported that they did not have enough time to intervene with the children, work with parents or teachers or their colleagues in other disciplines which one of the key aspects of the reconfiguration of disability services (Cantan & Bolger, 2017).
The therapists spoke of the flaws in how the CDNT model was being implemented that affected their clinical decision making. For example, they reported that managing their caseloads was a major challenge, due to the overlapping factors of large caseload numbers and poorly articulated definition of ‘complex needs’. The 2009 ‘Report of the National Reference Group on Multidisciplinary Disability Services for Children aged 5–18’ defines a CDNT as being for ‘children who have complex ongoing needs and require an interdisciplinary team service’ (Health Service Executive, 2009, p. 13). However, this definition is unclear in practice as the SLTs reported spending a considerable amount of time deciding whether a child was sufficiently ‘complex’ to need a CDNT or whether they should be referred to primary care for services. There were no clear pathways or policies around prioritisation and disparities within and across teams, leading to variable and inconsistent access to disability services. More than anything, clinicians spoke of large and unsafe caseloads and a lack of understanding from policy makers around the lifelong needs of those with disabilities. They argued that traditional HSE models of service delivery where children are offered relatively short periods of weekly on/off ‘blocks’ of intervention regardless of their level of need were not appropriate or effective for these children and their families. Research has shown that traditional approaches to intervention delivery that apply a universal treatment dosage such as the ‘6-week block’ for all children is not in line with evidence-based practice (Justice et al, 2017). Moreover, the changes required to successfully implement such service reconfiguration require clear leadership and management (Barry et al, 2021) with supportive appropriate clinical supervision (O’Keefe et al, 2014).
Large caseloads were also a significant barrier for providing safe and effective interventions according to our findings, although there are currently no recommended caseloads sizes for SLTs. For example, the American Speech-Language Hearing Association (ASHA, 2002) no longer recommend a maximum caseload number as they argue that agencies need to consider the amount of time a clinician has available and how this can be divided across services to children. They discuss the difference between a ‘caseload’ and ‘workload’ model, and how additional workload tasks including preparing reports, meetings, and other administrative tasks mean that there will be a necessary reduction in direct SLT interventions (Farquharson et al., 2022). ASHA argue that SLTs working with children with complex needs might have smaller caseloads due to the necessity for intensive direct and indirect services. Moreover, children with complex disabilities require longer assessment time due to the necessity of non-standardised methods and require the coordination of educational and health services. ASHA recommend setting caseload standards based on an analysis of overall workload to ensure that children receive appropriate and adequate services. In our survey and focus groups, the SLTs noted how children with FEDS needs and AAC devices were generally prioritised over those needing interventions for speech sound disorders for example, even though this disorder could present equally significant challenges for a child and their ability to communicate, socialise and learn. To our knowledge, there are no policy guidelines for CDNTs stating that FEDS and AAC should be prioritised on an SLT’s caseload, although it is known that both areas of work are very time intensive and increases SLTs workloads significantly (Farquharson et al, 2022; Yoshimatsu et al., 2024). Moreover, studies of SLT practice in the area of AAC has found that generalist SLTs do more maximal assessments and consider more irrelevant factors and so having more specialist SLTs clinical areas could enhance efficiency and quality (Dietz et al., 2012).
The challenges of providing a full tiered model of service delivery were also raised by clinicians. The SLTs reported that they were not able to use all tiers as they had to focus on giving ‘everyone something’ in largely group-based interventions at tier 2 (targeted) due to unmanageable caseloads and staff shortages. Even when they were able to provide interventions at Tier 3, this was only indirectly via parents and teachers, but again without sufficient time for individualisation and coaching. Direct interventions at tier 3 were rarely provided by SLTs, apart from AAC or FEDS needs as previously discussed. Previous research has found that a clinician’s ability to apply all tiers of intervention is affected by caseload size. In a review of how 575 SLTs working in the US can apply the tiered model, Swaminathan and Farquharson (2018) identified that those smaller caseloads of 40 children or less were more likely to be able to implement a multi-tiered approach than those with larger caseload (60 or more). It is therefore not surprising that the clinicians report that their caseload size impacts on their service delivery decisions. Pring et al. (2012) reviewed working practices of SLTs in the UK and noted similar stresses in terms of lack of time to use evidence-based practice, contribute to research and an increasing trend towards indirect therapy by educators and others. They also found that the SLTs were unhappy with the amount for direct therapy in particularly and with the amount of time dedicated to administrative tasks. The clinicians in our study also spoke of having to ‘water down’ their interventions due to caseload size. Regardless of whether an intervention is delivered indirectly by parents and/or teacher or directly by a clinician, it needs to be delivered at the appropriate dosage according to the evidence-based. Dosage relates to the intensity (time per session), frequency (number of treatment sessions) and duration (length of treatment) of any intervention (Farquarson et al., 2022). For children with intellectual disability, metanalyses of systematic reviews for indirect interventions have indicated that they ‘may require more intensive and longer-term language intervention to ensure improvements in their functional and social communication measured across context and over time’ (Roberts & Kaiser, 2011, p. 308).
The SLTs noted the effect that reconfiguration was having on relationships with parents and other professionals. The large caseloads meant that the SLTs didn’t know the families they were working with or have sufficient time to intervene. Parents were angry and unsatisfied with the services they were receiving. Many of the clinicians spoke about how they used Parent-Child Interaction Therapy (PCIT), whereby clinicians train parents on how to facilitate language and communication in everyday environments (O’Toole et al., 2021). PCIT is an evidence-based and important part of early SLT interventions, but must be delivered in a manner whereby parents achieve a shared understanding of communication and language and their role in developing this. In a qualitative evidence synthesis of 27 studies around parental experiences of PCIT, O’Toole et al. (2021) found that the ultimate success of PCIT interventions will depend on parental engagement, individually tailoring the intervention to family circumstances and whether there is a trusting relationship with the clinician. Parents need to be guided into, through and out of intervention and know about the next steps for their child’s intervention, including direct intervention from SLT. Clinicians in our survey expressed a desire to deliver PCIT intervention in this way, but were unable to do so. Collaborative relationships with colleagues in education and healthcare also affect the outcomes for children with disabilities meaning that broken relationships will have long lasting impacts (Carroll, 2009). It was evident from our study that multidisciplinary working was not uniform across teams and was largely due to staffing levels and vacancies. This was a similar finding to a study of how special education teachers in Ireland perceived collaboration around AAC following the move to CDNTs where collaboration was inconsistent leading to feelings of isolation and lack of support (Moore Ramirez & Lynch, 2024). Moreover, in the current study relationships with educators were particularly affected as SLTs were no longer working directly in schools. Interprofessional collaborative working is complex to achieve but co-practice and relationships are essential for service delivery for children with communication needs. These relationships are built on trust, reciprocity and negotiated practice both at the ground level at higher levels of service governance (McKean et al., 2017). It was evident from our data that SLTs were not able to develop these relationship and trust with their education colleagues to achieve effective co-practice.
Finally, the clinicians spoke about the work environment which was demoralising. Previous research has found that staff tend to become dissatisfied when the actual work situation does not align with the idealised work situation (Samadi et al., 2023), which can include caseload size, clinical autonomy, and opportunities to use professional skills (Ewen et al., 2021) all of which were evidence in our data. Participants also reported dissatisfaction with the loss of clinical specialisms they had developed prior to reconfiguration. Concerns here were twofold. First the challenge of providing interventions across the age span from 0 to 18 with a range of physical, sensory and cognitive disabilities. Second, the personal sense of disenfranchisement of no longer working in their chosen area of clinical specialism. Pring et al. (2012) and Bercow (2008) also noted that clinicians in the UK were dissatisfied working with a wide age band and range of communication difficulties and recommended providing a more specialised service as a more efficient way of delivering services and developing greater expertise. As healthcare professionals, SLTs are susceptible to occupational stress and burnout which can be exacerbated by ‘stressful working conditions, professional devaluation, occupational overload, poor management, and other situations that can have a significant impact on psychological and emotional well-being’ (Brito-Marcelino et al., 2020, p. 218). The conditions described by participants in this study show that SLTs in disability services are experiencing many of these risk factors for burnout. Moreover, there is a strong relationship between caseload size or manageability and job satisfaction (Farquharson et al., 2022) with a knock-on effect on the quality of therapy provision (Biancone et al., 2014). These factors have cascading effect as it is evident that smaller caseloads result in a more manageable workload for clinicians, which improves their job satisfaction and the quality of services they are able to provide and in turn results in improved child outcomes.
The clinicians suggested some potential solutions to the issues currently facing them. Firstly, increased staffing would mean that the workload would be more manageable, they would be able to provide more intense, individualised and higher quality services for all. One participant mentioned successful implementation of the CDNT model, but in an environment of a manageable caseload with appropriate clinical supervision. Their comments highlighted that ring-fenced workloads and a recognition of specialisms across age or area of practice with a defined career progression from staff to senior and specialist grades would ensure both efficient service delivery and career satisfaction. They suggested how some roles such as key worker roles could be led by administrative staff, thereby freeing up their time to provide clinical interventions. They also pressed the need for more clear prioritisation and clinical pathways for all children and all communication and FEDS needs and stressed the urgency for clinicians to be located in schools for effective collaborations and therapy delivery in schools. Finally, appropriate supervision and line management structures are needed so that clinicians are guided by those with a knowledge and understanding of their specific professional scope of practice (RCSLT, 2017).
Limitations of the Current Study
A limitation of this study was the small sample size. Only 28 SLTs completed the survey and there was a completion rate of just 26% for those who opened or started the survey. Although this could have been due to participants not meeting the inclusion criteria, it could also have been that the survey was too long. With this small sample represented in our data there is always the possibility that this can lead to bias on who chose to take part.
Conclusions and Recommendations
The results of this study suggest that the role of SLT in disability services is in crisis. Neither clinicians, families nor colleagues in health and education are currently satisfied with the intervention provision for children with disabilities. Overwhelmingly large caseloads, staff shortages, unclear pathways and insufficient time for interventions are resulting in demoralisation and burnout. Anecdotally it is known that experienced therapists working in disability services are leaving the profession, taking career breaks or pursuing employment in different areas including private practice. Many of the SLTs mentioned how private practice was a more attractive workplace due to defined and controlled workload and some had already moved. Increased private practice will ultimately grow a two-tiered therapy service if the public sector continues to be underfunded and children with disabilities do not receive the interventions they need. Speech and language therapy, if delivered correctly, is known to be a cost-effective intervention that will ultimately improve the social and academic outcomes for children with disabilities and their ability to live and work independently as adults, reducing the burden on state and families to care for them (Marsh et al, 2010). It is therefore imperative that the state invests in more posts that have ring-fenced workloads, appropriate supervision and mentoring and clinical specialities with career progression as a matter of urgency if they are to attract and retain these skilled clinicians. These posts need to be supported with effective policies to protect staff such as a clear definition and prioritisation of children that need this to attend CDNTs and clinical pathways in order to provide timely and appropriate services. Clinicians should be empowered to exercise their own clinical autonomy, provide direct intervention where needed and be supported to do so through appropriate clinical supervision and support.
Supplemental Material
Supplemental Material - Speech and Language Therapists Experiences of Delivering Interventions Across Disability Services in Ireland: The Move to Child Disability Network Teams (CDNTs)
Supplemental Material for Speech and Language Therapists Experiences of Delivering Interventions Across Disability Services in Ireland: The Move to Child Disability Network Teams (CDNTs) by Ciara O’Toole and Noreen O’Leary in Advances in Communication and Swallowing
Footnotes
Acknowledgements
The authors would like to thank the therapists who gave their time to complete the survey and take part in our focus groups and interviews and share their at times difficult experiences.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.