
Abstract
Background
Children with neurodevelopmental disabilities (NDDs) have complex therapeutic needs which require tailored models of service delivery.
Objective
To profile the characteristics of the optimal service for children with complex neurodevelopmental disabilities in policy and professional guidelines in addition to the empirical literature.
Methods
An integrative review was conducted. A systematic search of electronic databases (n=4) for Ireland, New Zealand and Finland and a manual search of policy and professional guidelines for Ireland was completed in October 2023. A total of 18 papers were included in the analysis. Qualitative content analysis was undertaken independently by two researchers.
Results
Five descriptive categories were identified across the dataset: (i) Person-centred, (ii) Empowering, (iii) Evidence-based, (iv) Accountable, and (v) Safe.
Conclusions
A coherent vision of the optimal services for children and young people with complex NDDs is evident across policy, professional guidelines and empirical literature. Currently there is a discord between this vision and the realities of service delivery in the Irish healthcare context. Implementation science theories and frameworks have the potential to bridge the research-practice gap and improve services for this vulnerable population.
Keywords
Introduction
Neurodevelopmental disabilities (NDDs) include conditions such as communication disorders, specific learning disorders (American Psychiatric Association 2013; Thapar et al., 2017), autism, attention deficit hyperactivity disorder (ADHD), and motor disorders. Children with NDDs can experience difficulties developing speech, language and communication, as well cognitive skills, motor, sensory and emotional behavioural skills. For many children, these needs co-occur (Hughes et al., 2017; Larson et al., 2011; Thapar et al., 2017). Children with NDDs have been shown to have poorer long-term outcomes in terms of educational attainment, employment, and mental health (Danielsson et al, 2024), as well as being at increased risk of co-occurring chronic health needs in adulthood (McCarron et al, 2017; Torr et al, 2010).
Findings from international studies report that between 12 and 15% of the childhood population presents with one or more NDD (Atladottir et al., 2015; Grandjean & Landrigan, 2014). In 2022, there were 131,764 children with an NDD in Ireland, accounting for 10.8% of the child population (the Department of Children, Equality, Disability, Integration and Youth, 2023). Irish population-based data also shows that from 2011 to 2016, the number of children aged 3–5 with NDDs has increased (Whelan et al., 2021).
Children with one or more NDD are often referred to as having complex needs, as they may require several therapeutic services to meet their needs across the lifespan including speech and language therapy, occupational therapy, physiotherapy, and psychological supports in addition to medical and social care. In the Irish context, complex needs are defined as needs arising from a disability where one or more impairments ‘contribute to a range of significant functional difficulties that require the services and support of an interdisciplinary disability team’ (Health Service Executive [HSE] 2019, p.13) There is significant evidence to suggest that the earlier therapeutic interventions are delivered, the better the long-term outcomes for this population (Boccaccio et al., 2023; Colizzi et al., 2020; Morgan et al., 2021). However, addressing the needs of children with multiple NDDs presents health services with unique challenges, in part because for supports to be effective they must be delivered in an integrated way across health, education and social care (Thapar et al., 2017).
In Ireland, services for children with complex NDDs have undergone significant changes in recent years. Traditionally, service provision was delivered by both statutory bodies, such as the Health Service Executive (HSE), and non-statutory organisations, including the Brothers of Charity and Enable Ireland. How services were structured resulted in disparities in access to supports and resulted in differences in outcomes for the population nationally. In 2009, a health service restructuring programme, Progressing Disability Services for Children and Young People (PDS) was launched which aimed to address healthcare inequity and to improve outcomes for all children with complex NDDs across Ireland (Cantan & Bolger, 2017). It was informed by a number of key pieces of legislation and policy such as the Disability Act (2005), Education of Persons with Special Needs Act (2004), and the Sláintecare policy (2017). By December 2021, the reconfiguration of services was considered complete, with 91 disability teams operating under the new framework. These teams referred to as Children’s Disability Network Teams (CDNT) were tasked with providing holistic, family-centred support using an interdisciplinary approach, with optimal resource utilisation (HSE 2022a). In the last three years, however, it is has become increasingly apparent that many stakeholders are not satisfied with the new model of services for children with complex NDD in Ireland. Although limited objective robust service data exists nationally, data published in 2023 by the HSE itself (HSE 2023) showed large numbers of children (over 16,500) awaiting their first appointment with a CDNT with an additional 70,000 children awaiting intervention.
The HSE cite several contributory factors including long waiting lists, staffing vacancies, and growing service demand as well as the assessment of need (AON) under the Disability Act 2005. This Act provides for a legal right to assessment for people suspected of having a disability born on or after 1st of June 2022. There was a 20% increase in AON applications in June 2023 compared with the previous year (HSE 2023). This assessment process has impacted significantly on the delivery of therapeutic services. Increased demand for assessment and therapeutic services is not limited to Ireland. For example, in the United Kingdom new autism referrals increased by 27% in 2023 compared with the previous year (Child of the North Initiative & & Centre for Young Lives, 2024). In the United States, Chen et al., 2023) found in excess of a 2-year waitlist from first screening to autism diagnosis.
The current system of service provision for children with complex NDDs does not align with the World Health Organisation’s (WHO, 2010) definition of quality care which describes quality care as the degree to which health services for individuals and populations increase the likelihood of desired health outcome.
An integrative review of empirical and theoretical literature, as well as national policy and professional guidelines was undertaken to gain a greater understanding of an optimal service for children with complex neurodevelopmental disabilities.
This research addressed the following question: What are the characteristics/features of the optimal service for children and young people with complex neurodevelopmental disability as described in literature including empirical and policy/professional guidelines?
Methods
Positionality Statement
The research team included six White able-bodied females. Two researchers were students on a professional qualification programme, one (NW) in occupational therapy and the other (HS) in speech and language therapy. The remaining four researchers were qualified speech and language therapists (SLTs) previously in practice and at the time of the study in academic roles. These researchers were acting in the capacity of research supervisors. Three of these research supervisors had direct practice experience working in services for children with complex neurodevelopmental needs when practising as SLTs. It can be said that the research team were positioned as insiders in relation to the research undertaken. Being an insider requires additional consideration with regards to rigour when planning and undertaking a study. To this end, all search strings were developed with external advice from library specialist in health sciences, screening of papers were undertaken by two reviewers, analytical coding was undertaken by two researchers independently and using a qualitative database to track decisions, field notes were kept by the primary coders, and findings were presented and discussed at three research meetings with academic supervisors throughout the analytical phases to consider other possible conceptual mapping of the dataset.
Study Design
Given our aim was to conduct a comprehensive review of policy and empirical literature, we chose to undertake an integrative review. An integrative review is a well-established method of answering research questions which span policy and practice as it allows for different search strategies (systematic and/or purposive), different inclusion criteria and diverse quality appraisal tools as needed to enable the identification, inclusion and analysis of disparate sources of literature (Souza et al., 2010). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in reporting the results of the searches (Moher et al., 2009).
Searching the Literature
Search Strategy (Empirical/Theoretical Literature)
A systematic electronic search was conducted to retrieve empirical and theoretical literature using the elements Sample - Phenomenon of Interest (SPI) from the SPIDER framework (Cooke et al., 2012) with the support of an information specialist in Education and Health Sciences. Search strings were developed by HS and NOL. The population of interest was children and young people with childhood onset developmental disabilities. The situation was health services delivery models and the countries of interest included Ireland, New Zealand, and Finland. The latter two countries were selected due to their similar population sizes and cultural affinities with Ireland. Electronic search strings were developed in the first instance with key words from relevant literature known to the research group. Specific thesaurus terms related to each electronic database were then added. Final electronic searches were completed in October 2023 by HS and NOL. The following four databases were searched PsycINFO, Scopus, Medline, and CINAHL. Papers were restricted to after the WHO published indicators for a quality health service in 2010 (Appendix 1 for a sample electronic search string).
Manual Searches
Manual searches were conducted by NW and another researcher and were completed in August 2023. Documents from government departments, non-governmental organisations, and healthcare professional associations in Ireland were searched. Manual searches were recorded in relation to date of search, website link, and number of documents yielded.
Identifying the Included Papers
Inclusion and Exclusion Criteria
Empirical publications were included if they met the following criteria: • Related to children and young people with neurodevelopmental disabilities. • Related to health service/care delivery models. • Included detailed description of the characteristics of a service/ healthcare model. • Peer-reviewed publication.
Papers were excluded if they: • Did not relate to children and young people with neurodevelopmental disabilities. • Did not relate to health service/care delivery models in Ireland, Finland or New Zealand. • Did not have data related to the characteristics of a service/ healthcare model. • Not peer-reviewed. • Published before 2010.
Screening the Literature
When final electronic searches were completed, papers were exported and uploaded to Rayyan (Ouzzani et al., 2016). Rayyan is an online screening tool which allows researchers to track all inclusion and exclusion decisions and to note rationale for each decision. Screening for title and abstract was conducted by HS and NOL. Where lack of agreement between reviews decisions arose, these were referred to NW. Most discrepancies were related to diverse nature of terminology in relation to the population of interest. In relation to policies and professional guidelines, many documents retrieved were not in the format of academic papers with a sufficiently detailed title and abstract by which to screen. A preliminary read of the executive summaries was then undertaken by NW and another researcher independently to ascertain relevance prior to including for a full text review.
Analysis
Once final included papers were identified, these were imported into NVivo software package (version 14) for analysis (Dhakal, 2022). NVivo is a data management system which allows for the recording of decisions during qualitative analysis. A guiding analytical framework informed by a preliminary scoping of health service improvement documents was used in initial stages of coding. Deductive content analysis was used to analyse the qualitative data. Descriptive categories were then developed once a final list of initial codes had been identified. Two research meetings were held to interrogate the data and coding during the process of analysis to ensure other plausible lines of argument were explored and discounted.
Results
Search Results
See Figure 1 for further details. The final dataset following full text screening resulted in eleven papers from the electronic search and seven documents from manual searches. Of the empirical papers, most were qualitative studies (n=8), two papers reported a mixed-methods design (one sequential mixed-methods design and one embedded design), and one paper reported a quantitative study design. Of the seven papers retrieved from the manual searches and screening these included one national policy, four professional/national guidelines, one government reports, and one survey. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram (Page, 2021)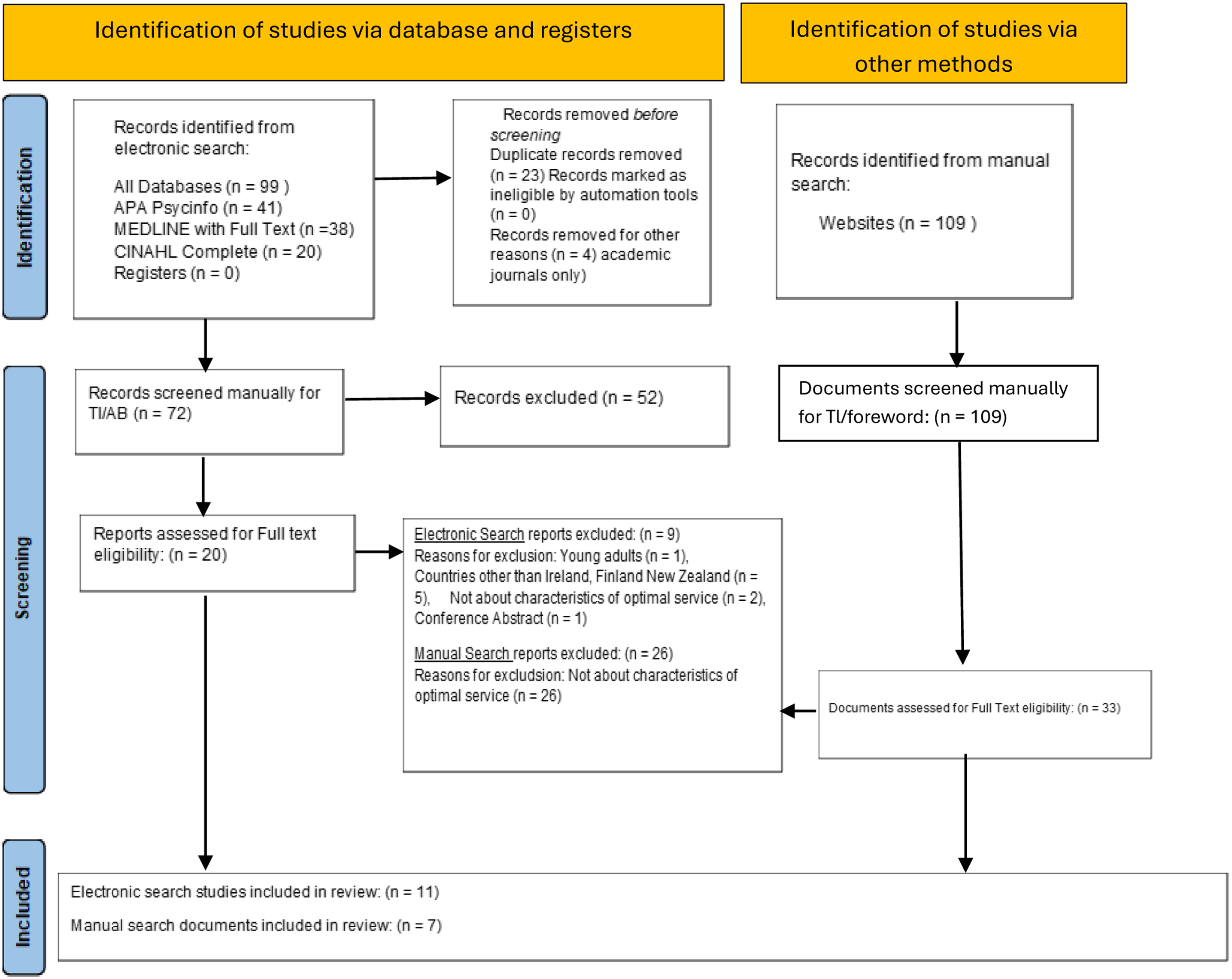
Characteristics of Included Empirical Papers
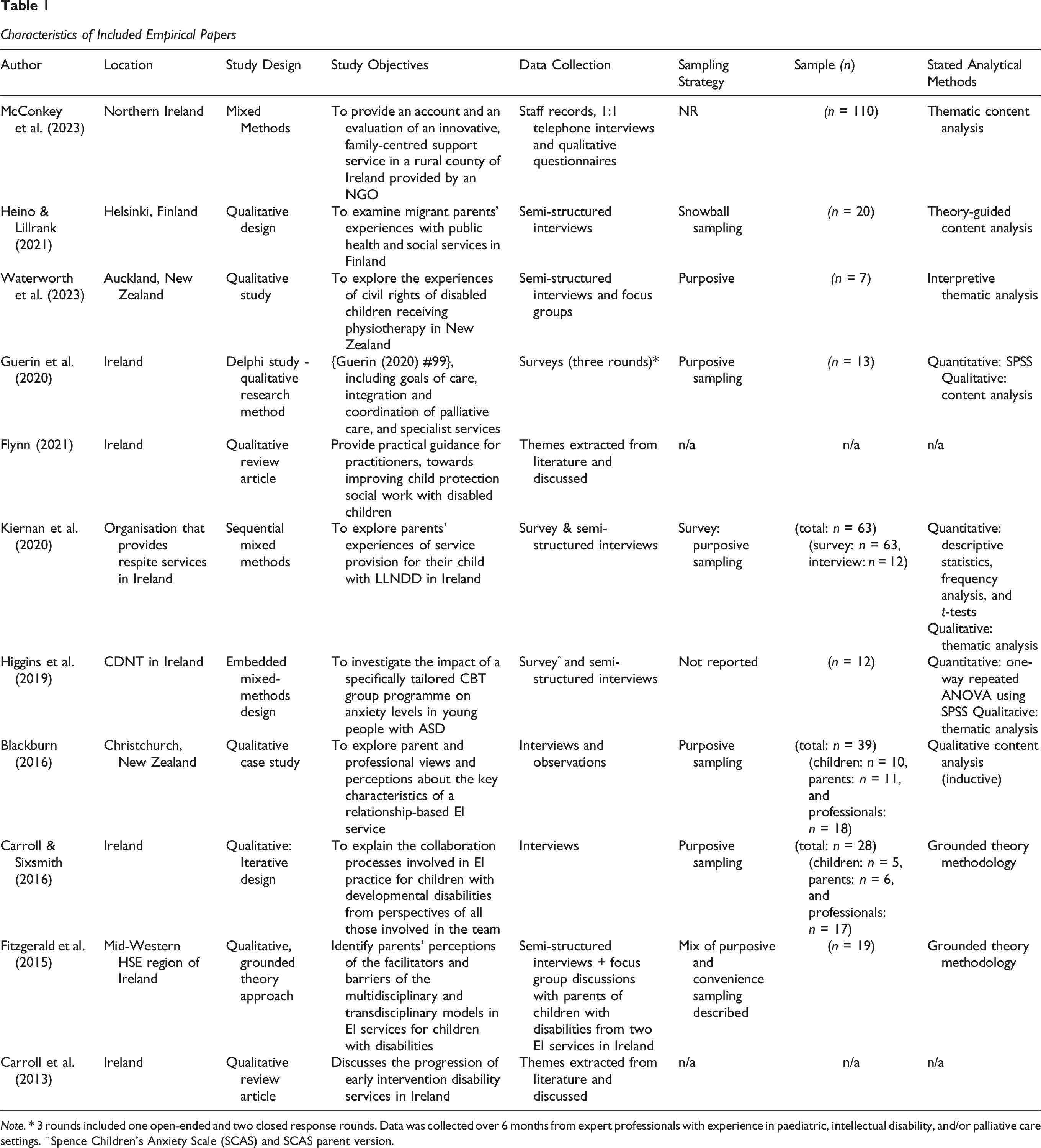
Note. * 3 rounds included one open-ended and two closed response rounds. Data was collected over 6 months from expert professionals with experience in paediatric, intellectual disability, and/or palliative care settings. ^ Spence Children’s Anxiety Scale (SCAS) and SCAS parent version.
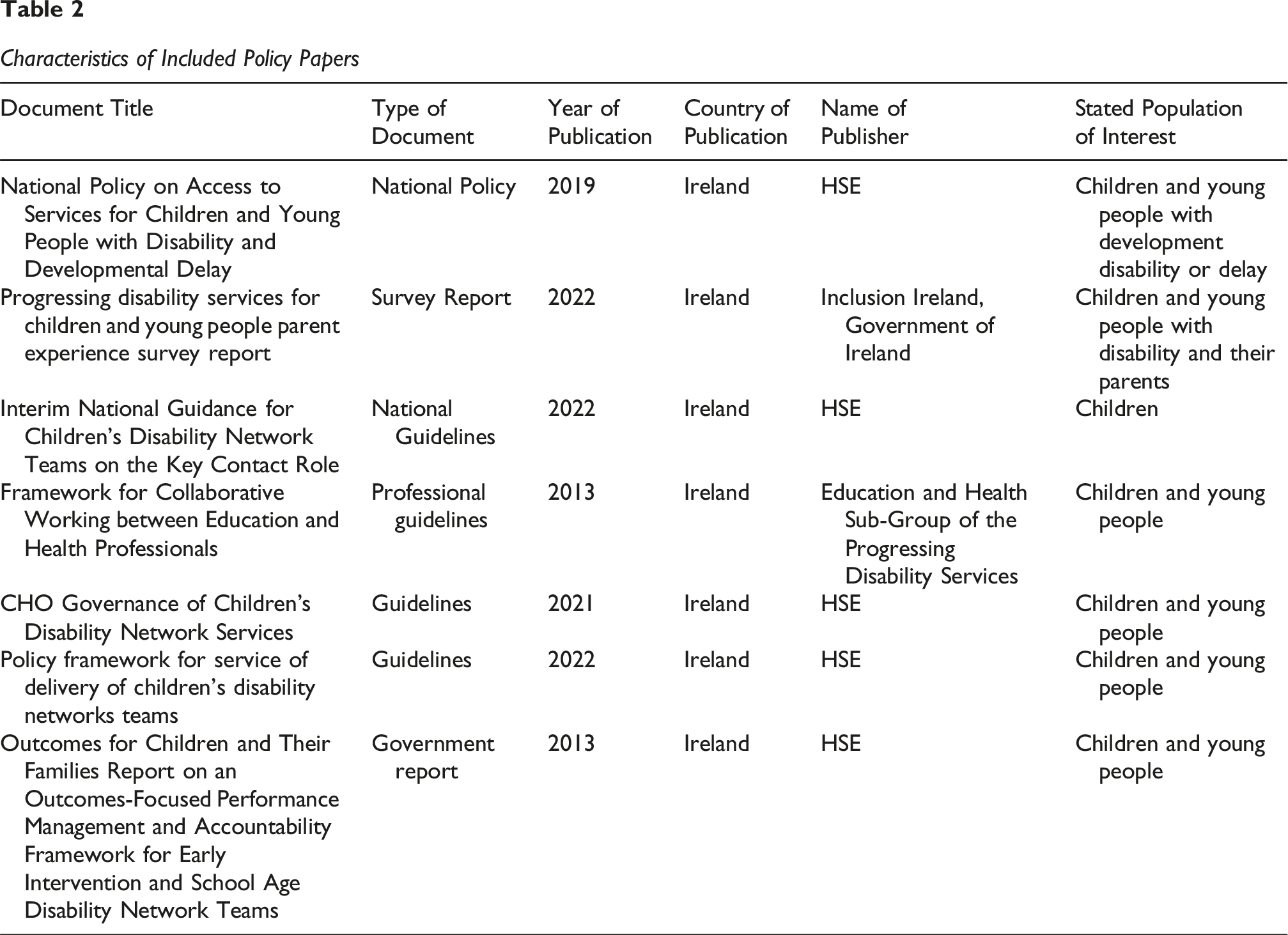
Characteristics of Included Policy Papers
Analysis
We present a summary of our findings in Figure 2. We then describe the findings from our deductive content analysis under five descriptive categories (i) Person-centred, (ii) Empowering, (iii) Evidence-based, (iv) Accountable, and (v) Safe in order from the most frequently coded concepts to the least coded. Characteristics of the Optimal Service for Children and Young People With Neurodevelopmental Disabilities
Description Category 1: Person-Centred
A Responsive and Accessible Service With Shared Decision-Making
This descriptive category includes four subcategories: (i) a tailored service responsive to the needs of the individual, (ii) family involvement, (iii) the voice of the child as a participant, and (iv) timely and accessible services.
In relation to tailored services, almost all papers highlighted the importance of a flexible, responsive, adaptable approach to cater for individual needs of the child and family (n=17): ‘Each child’s session was different, as therapists worked on children’s individual learning targets that valued family practices and children’s interests and preferences’ (Blackburn, 2016, p. 339).
A significant number of studies highlighted the importance of family involvement in an optimal service (n=16). This included taking the family into consideration and enabling them to be part of the design and decision-making process. In addition, some studies identified the need for families to be treated with respect, to be listened to, and their circumstances acknowledged throughout: ‘Parents know their child better than anyone else and should be treated by professionals as equal partners given the expertise they have in the care of their child. […] A child’s need for services does not exist in isolation from their other needs and from the needs of their family’ (HSE, 2021b, p. 4) .
The voice of the child and their involvement in decision-making was referenced in some papers (n=6). An optimal service that respected and valued the child’s opinion was referenced throughout. It enables the child to be an active participant in their care and allows them to make informed decisions.
Multiple papers also identified the importance of a responsive, accessible service that takes place during the early developmental years (n=15): ‘Children with disabilities need and deserve to access comprehensive, consistent support from as early as possible for as long as they require’ (Inclusion Ireland, 2022 p. 20).
Description Category 2: Empowering
Empowering Service Users as Partners
This descriptive category includes three subcategories: (i) empowering parents and families, (ii) networks, and (iii) participation.
Family training, education and provision of information, capacity building, and upskilling were heavily referenced across many papers as being important components of parent empowerment (n=11). This involved linking families to relevant supports and resources, facilitating parent and family training, and equipping them with skills and strategies. Several articles referred to facilitating parent empowerment: ‘Families are empowered and enabled to engage at the level that is comfortable and appropriate for them according to their own psychobiology’ (Blackburn, 2016 p.340).
The importance of having a support network was referenced across some of the papers, which included supportive relationships between children with disability and their family/community (n=8). This also included the importance of supportive professionals with expertise: ‘One of the legacies of a time-limited engagement with families by professional services is helping them to build ongoing support networks among family and friends’ (McConkey et al., 2023 p. 9 ).
Participation was a key idea within better health and wellbeing. This involved opportunities for families to engage socially in community activities. Providing opportunities for development of knowledge/skills and capacity building were also referenced in some papers within participation (n=6). This included functional development and learning daily living skills: ‘Offering programmes that support the development of skills for daily living, participation in pre-school and school as appropriate and information for families on local activities, social, sporting and cultural opportunities’ (HSE, 2022b, p.8).
Description Category 3: Effective
Evidence-Based Interventions and Meaningful Outcomes
This descriptive category includes three subcategories: (i) ensuring evidence-based services, (ii) ensuring that interventions target appropriate/meaningful outcomes for the child, and that (iii) services have mechanisms allowing for quality improvement and monitor effectiveness:
In relation to evidence-based services, the importance of ensuring that practice was informed by recent research was most commonly discussed as a component of optimal service (n=14). This incorporated ideas such as the importance of early interventions, the amount of therapy given, and the frequency of sessions. It also indicated in some papers that the skills and expertise of staff should be informed by evidence-based practice: ‘[E]nsure the highest possible quality of service based on current knowledge and evaluated practice by keeping up to date with the latest research’ (HSE, 2013b, p. 19).
In terms of meaningful outcomes, several papers discussed the significance of working towards functional goals (n=10). This reflected an outcome focused delivery of care. Accountability, planning, and regular monitoring were referenced in a few papers. Clarifying expectations between stakeholders was also referenced in a few papers. This allowed parents and staff a greater understanding and enabled them to collaborate effectively: ‘To maintain a focus on desired outcomes for the individual child and the family through a process of clarifying expectations’ (HSE, 2013b, p 15).
Quality improvement involved ongoing, flexible evaluation. Some papers identified the need for optimal services to have mechanisms that allow for quality improvement and to monitor effectiveness (n=8). This could include audits and reviews as well as consistency and continuity of services: ‘Services are regularly monitored and reviewed with the involvement of service users […] in line with best practice’ (HSE, 2013b, p.19).
Description Category 4: Accountable
Team Working for an Equitable and Accountable Service
This descriptive category includes three subcategories: (i) effective communication, (ii) equitable access to services, and (iii) governance that monitors the outcomes and results of the interdisciplinary process.
In relation effective communication, families identified collaboration of professionals as significant in providing quality care (n=13). These incorporated professionals learning from each other and communicating effectively; integral aspects of coordinated care: ‘They’ve all seen the child. Somebody will have a little piece that they would never put in a report, but somebody else will have a little piece and suddenly there’s a synergy of understanding’ (Blackburn, 2016, p.337).
As part of this interdisciplinary response to working, a key worker was identified in some papers as being part of an optimal service. This represented one point of contact for the family and coordinated the care through effective lines of communication: ‘The requirement for team members to act as Key Contact, key worker or support coordinator for children and families is a prominent feature in recommendations on family centred practice’ (HSE, 2022a, p.2).
In terms of access and equity, a clear pathway to interdisciplinary services and an individualised, easily accessible, needs-based service was referenced in some papers (n=7). ‘[T]he importance of the range of therapies being accessible to families in one location was noted […], as was the frequency of delivery and time given to children within their sessions’ (Blackburn, 2016, p.337).
Some papers identified the importance of governance under interdisciplinary working (n=8). This represents a level of accountability between interdisciplinary teams and provides a review of clinical standards: ‘For healthcare staff, this means specifying the clinical standards you are going to deliver and showing everyone the measurements you have made, to demonstrate that you have done what you have set out to do’ (HSE, 2021a, p.7).
Description Category 5: Safe
Do No Harm
This descriptive category includes three subcategories: (i) care that prevents harm, (ii) the importance of a safe spaces, and (iii) the need to protect vulnerable populations.
In relation to care that prevents harm, safeguarding and preventing harm from occurring was most commonly discussed within this domain (n=8). Clinical governance, accountability and clarity on management roles/responsibilities to ensure safe and quality care was also referenced. This incorporated ideas such as monitoring performance, specifying clinical standards, and the use of guiding principles to prevent harm from occurring: ‘There must be structures in place to support children disability network managers and staff and to respond to governance issues in a timely manner. This is to ensure safe processes and a safe working environment for all levels of staff’ (HSE 2021a, p.7).
In relation to the importance of ensuring a safe space, fostering a safe, welcoming and nurturing environment was referenced (n=3) This involved ideas such as ensuring safe spaces for children to speak out with safe adults and promoting safe school/work cultures and environments. Protecting vulnerable populations was referenced on one (n=1) occasion: ‘[T]he Centre director identified the structural processes that needed to be in place […] nurturing therapy spaces in a welcoming environment’ (Blackburn, 2016, p. 337).
Discussion
This integrative review of policy, professional guidelines, and empirical literature was conducted to gain a more comprehensive understanding of the characteristics of the optimal service for children with complex neurodevelopmental disabilities. A systematic search of electronic databases (n=4), and manual searches of policy and professional guidelines was undertaken. A total of 18 papers were included in the final analysis. Qualitative content analysis was employed across the dataset. Five descriptive categories were identified that describe the characteristic of the optimal service for children with complex neurodevelopmental needs.
A Coherent Vision
The findings of the review show a coherent vision of the components of the optimal service for children and young people with complex needs across policy, professional guidelines and the empirical literature. The optimal service is characterised as person-centred (responsive, tailored and adaptable to the individual needs of the family and the child), empowering (focused on equipping the child and family with the knowledge and skills to manage their own health and wellbeing), effective (using the best available evidence to achieve meaningful outcomes), safe and accountable, and delivered by a team of professionals who work effectively together towards the family’s goals and vision.
Many of these characteristics have been discussed in the literature for some time. For example, the notions of person-centred care was first discussed in the 1940s by Carl Rogers (Rogers, 1951) who proposed a shift from a disease-centred focus to an healthcare delivery approach based on the assumption that a person should be viewed as a whole and that their right to self-determination should be respected. Since that time concepts such as person-centred care, patient empowerment, and patient participation have received much attention in the literature bringing both conceptual clarity, and the development of practical tools to support the implementation of such participatory healthcare ideas in practice (Hakansson et al., 2019). The evidence-based medicine movement can be traced back to the early 20th century, and evidence-based decision-making has been fully integrated in health professional standards of practice internationally for decades (Ratnani et al., 2023).
Further, the principles of open science in the last twenty years have resulted in the widespread availability of synthesised and critically appraised evidence for clinical practice, reducing many of the perceived practitioner-level barriers to implementing evidence-based decision-making as routine practice. A similarly rich body of literature has explored the complexities of inter-professional care for several decades (see Baldwin, 2007 for a history of the concept) resulting in several frameworks and models to guide collaborative practice across a range of healthcare settings, including in the field of speech and language therapy related to school-aged children with speech, language, and communication needs (Gallagher et al, 2021).
Issues in Practice
Despite evidence of a coherent vision for services for children with complex NDDs, and a rich body of literature bringing conceptual clarity in relation to how such a vision might be translated into practice, implementation of a person-centred, empowering, evidence-based, accountable and safe service appears to present significant challenges in the context of the Irish healthcare system. For example, research suggests that children with NDDs in Ireland are facing significant challenges in terms of access to timely, responsive services (Blackburn, 2016; Carrol et al., 2013; Gonzalez et al., 2022; Wiley et al., 2022), with one commentator describing the current model as funding-centred, rather than family-centred (Fogarty, 2024 para.22). Rather than responding to the needs of families, other factors such as location appear to determine access. A national parent survey by Inclusion Ireland in 2022 reports those in urban settings receiving better services than those in rural areas and finding consistent with McConkey et al. in 2023. Regarding engaging families as partners, further issues are evident. There are reports that parents of children with complex needs feel forgotten about, ignored, and not consulted (English, 2024; Molloy, 2022). Such a lack of partnership between parents and professionals can lead to different expectations of treatment, which can reduce further cooperation and engagement with the service (Heino & Lillrank, 2021). In terms of effectiveness, there is some evidence to suggest that families who do receive intervention appear to be dissatisfied with the limited frequency and duration of therapy time which they believe negatively impacts outcomes for the child (Carroll & Sixsmith, 2016; Fitzgerald et al., 2015; Kiernan et al., 2020). Issues of safety have also been noted. In a joint submission to the HSE, Health and Social Care professionals have recently highlighted ‘serious concern with the current direction, impact and safety of Children’s Disability Services’. They cited systemic failures in the roll out of disability services which are ‘placing children, families, and Health and Social Care Professionals at risk’ (HSCP, 2024, p. 1).
Bridging the Gap
Although limited service and practice data exists in relation to services, it appears from the evidence available that there is a significant discord between the characteristics of the optimal service for children with complex NDDs in the literature and the practice reality in the Irish context. Such a gap calls for evidence-based methods of understanding. Using theories and frameworks from the field of implementation science when conducting research in this health services context can provide actionable knowledge to bridge the gap. Such an approach would allow for a thorough exploration of innovation related factors and how these are contributing to challenges in service delivery. This could result in guidance as to how the model could be improved. In addition to innovation level factors, such an approach can guide an exploration at an organisational level to provide recommendations to inform implementation strategies. Implementation science tools can also shed a light on the process of implementation, and how this may be improved. For example, we know that in order for any innovation to be successfully implemented, all stakeholders need to be engaged authentically and on an ongoing basis and that the innovation needs to align with their values and vision. Implementation science is a field of inquiry which allows the study of methods to support the systematic uptake of innovations such as new models of care such that they become normalised into routine practice (Durlak & DuPre, 2008) The method of inquiry provides a vast array of theories, models, and frameworks incorporating factors related to the innovation itself and those related to the inner and outer settings which influence implementation outcomes. (Damschroder 2022, May 2018).
It may be that changes implemented as part of Progressing Disabilities need to be re-examined in relation to their underpinning values. By taking the time to understand the implementation of the current model through a new lens, we may be better positioned to meet our obligations of quality care as recommended by the World Health Organisation (WHO, 2010). These obligations include ensuring that health services are effective, safe, person-centred, timely, equitable, integrated, and efficient. This consideration may lead to an improvement in long-term outcomes of educational attainment, employment, living independently as well as in the overall health and wellbeing for children with NDDs.
Strengths and Limitations
The use of integrative review methods allowed a systematic search of both manual and electronic searches. Having insight from policy documents as well as empirical literature enabled us to examine whether a coherent description of the optimal healthcare service existed. However, there are several limitations that need to be considered when considering the findings. There are well-documented differences in definitions and terminology in relation to neurodisabilities in the literature that may have negatively impacted the accuracy of our search strings. Furthermore, it was beyond the scope of this research to carry out searches on individual conditions which may have yielded additional data on those with complex needs. The research team may have benefited from having a member who identified as neurodivergent as this would have provided an additional lens on the research. In addition, for resource driven reasons, we were not in a position to conduct comprehensive searches of the grey literature around our focus of inquiry. These decisions may have resulted in important empirical studies being missed. A full critical appraisal of the studies was not undertaken. Therefore, it has not been possible to provide important information regarding the quality of the body of empirical literature included in the study nor to discuss these quality issues when interpreting the findings.
Conclusion
A coherent vision of the optimal service for children with complex neurodevelopmental needs was identified in this integrative review. The characteristics described have been a focus of inquiry in the healthcare literature for many decades. There appears to be a significant discord between the optimal service in the literature and the service that is currently being delivered in the Irish healthcare system. The need to understand more fully the discord between this policy vision and the practice reality using analytical methods from implementation science is proposed. This work is needed to ensure that we meet our obligations to ensure that Irish children and young people with complex needs are to be enabled, as is their right, to participate and achieve to their full potential.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.