
Abstract
Commercial activities (eg, lobbying, water extraction) have important implications for population health and health equity. Identifying these activities can inform public health policy, practice, and surveillance. The aims of this study were to adapt a cross-industry typology of corporate activities (the HEALTH-CORP typology) to the Food & Beverage (F&B) industry and identify expert-informed measurement priorities for this industry. Activities within the HEALTH-CORP typology are categorized into domains of corporate influence (eg, political practices, environmental practices). Health experts (n = 22) rated the importance of measuring each domain on a 4-point scale (from ‘not important’ (0) to ‘very important’ (3)) and provided written feedback to guide the adaptation. We used qualitative and non-parametric quantitative techniques (eg, Mann-Whitney U tests) to analyze and implement participants’ feedback. The domain political practices received the highest mean importance rating (M = 2.95, IQR = 0); employment practices received the lowest (M = 2.14, IQR = 2). Ratings for some domains differed by whether experts reported employment in low-and-middle income countries. The resulting HEALTH-CORP-FB typology contains 89 F&B industry activities (eg, profiteering, child-appealing packaging). The typology provides a resource for policy makers and other stakeholders and the findings lend insight into measurement and monitoring priorities for this industry.
Keywords
Introduction
Over the last two decades, the concept of the commercial determinants of health (CDH) has emerged as a new lens to understand the causes of poor health and health inequity. The CDH have been defined as the “systems, practices, and pathways through which commercial actors drive health and equity.” 1 (p1195) Though less conceptually developed and globally recognized than the related concept of the social determinants of health (SDH), interest and attention to the CDH has been growing both within and outside of academia.2–5 By illuminating the role of market actors and market power in the development of adverse health outcomes, the concept of the CDH has the potential to direct policy makers towards underutilized solutions to addressing poor health and health inequity (eg, regulation of harmful commodities). 2
In an influential Lancet series on the CDH, Gilmore and colleagues proposed seven practices through which commercial entities can influence health. 1 These are: political practices, scientific practices, marketing practices, supply chain and waste practices, labour and employment practices, financial practices, and reputational management practices. The second article in this series provides a set of guiding questions that actors (eg, policy makers) can use to consider a company's engagement in these practices for the purposes of guiding their interactions with these entities or informing research and monitoring efforts (eg, “does the entity seek to influence global, supranational, national, or local policy development?”). 6
Our author team recently conducted a scoping review of CDH research describing corporate activities that can influence population health and health equity.7 We qualitatively synthesized the literature in this review to develop a typology (called the Corporate Influences on Population Health (HEALTH-CORP) typology) that describes 70 corporate activities that can influence population health and health equity across industries. Activities within the HEALTH-CORP typology are categorized across seven ‘domains of corporate influence’ (eg, political practices, products & services, environmental practices); these domains are conceptually-similar to the practices proposed by Gilmore and colleagues. 1 This work expands on the Lancet series by more comprehensively identifying the array of activities through which commercial entities influence population health (eg, lobbying, product accessibility, water extraction). 7
In this article, we describe a follow-up study that we conducted to adapt the cross-industry HEATH-CORP typology to the food and beverage (F&B) industry. The adaptation process involved the solicitation of input from health researchers and practitioners with relevant expertise (eg, nutrition, occupational health, environmental health). By integrating this feedback, we developed a F&B specific typology called the HEALTH-CORP-Food and Beverage typology (HEALTH-CORP-FB).
The primary aim of this study was to generate a typology that identifies the diverse range of activities through which the F&B industry can influence population health and health equity. Current frameworks designed to identify and/or monitor the practices of the F&B industry focus on specific practices and their health impact (eg, nutrition-related practices).8–11 Others consider a wider range of practices but do not focus specifically on practices that affect human health (eg, the World Benchmarking Alliance's Food & Agriculture Benchmark).12–14 The F&B industry exerts a significant impact on population health through a diverse set of mechanisms that include nutrition, environmental practices, and employment practices, among others.15–18 Developing a typology that captures the diverse range of practices through which this industry influences population health can support public health policy and practice by providing a resource for stakeholders (eg, policy makers, civil society actors) that play a role in monitoring and addressing these practices. It could also support existing monitoring initiatives by identifying activities that are not currently addressed by these frameworks.
The secondary aim of this study was to identify the practices of this industry that are deemed priorities for measurement and monitoring by public health experts. Effective monitoring of corporate practices is an important objective for the CDH field: longitudinal monitoring could be used to identify trends in corporate practices across time, industries, and regions, and illuminate areas in which stronger regulation is needed.19,20 In their recent review of frameworks describing the activities of the alcohol, tobacco, and ultra-processed food industries that influence human health, Bennett, Topp, and Moodie 19 suggested that government-led surveillance programs are unlikely to have the resources to monitor all corporate practices that affect health; therefore, a process of prioritization will be required. They remarked that: “since no explicit or relative justification for inclusion of certain corporate practices were made in any framework, [it] is not currently clear why some corporate practices should be prioritised for monitoring over others in any given setting.” 19 (p.11) Therefore, we sought to leverage our adaptation process to provide initial insight into expert-informed monitoring priorities for this industry.
In the next sections, we describe our process for adapting the HEALTH-CORP typology to the F&B industry, including our methods for eliciting relevant input from experts. We report key findings from this feedback, including the domains that experts felt were important to measure and monitor. We also report the ways in which experts’ responses differed as a function of the income level of the countr(ies) in which they were employed, suggesting contextual differences in the perceived importance of measuring certain corporate activities. Finally, we discuss the findings in relation to the two aims of this study, the strengths and limitations of the typology in comparison to other frameworks, and its potential uses for supporting policy, practice, and surveillance of F&B industry practices.
Methods
Our methodological approach was inspired by a Delphi design and altered for feasibility. Delphi designs involve the participation of experts in a series of feedback rounds with the goal of gaining consensus on a particular issue. 21 In a fully implemented Delphi study, participants are provided with the results of previous rounds, which they can use to reflect on other participants’ perspectives and change their own views accordingly, ultimately facilitating the development of consensus. In this study, we used a series of prompts to solicit structured feedback (ie, Likert-scale data, written responses) from public health experts on ways to adapt the HEALTH-CORP typology so that it reflects the specific activities of the F&B industry. For feasibility reasons, we were not able to engage the experts in multiple rounds of feedback.
For the purposes of this study, we defined the F&B industry as comprising entities that are involved in agriculture, F&B manufacturing, processing, wholesaling, retailing, marketing, and service provision (adapted from Mialon and colleagues). 22 Companies primarily involved in the processing or sale of alcohol and tobacco and/or that receive less than half their revenue from F&B products were not considered to be a part of this industry.
Ethics Approval
This study was reviewed by the Yale Institutional Review Board (Protocol ID #2000034281) and received approval as exempt research. Standards of research ethics were followed in the conduct of the study, such as requiring participants to provide written consent to participate and putting in controls to prevent breaches in confidentiality (eg, secure data storage).
Participants & Recruitment Strategy
Public health professionals and health researchers with expertise in topics relevant to the F&B industry were recruited via purposive and snowball sampling techniques. 23 Specifically, we identified potential participants by reviewing the author lists of relevant journal articles, asking participants and colleagues for referrals, and conducting internet searches. Invitations to participate were sent via email or LinkedIn direct message by the first author (RB). Recruitment occurred from May 8 to July 5, 2023.
We sought to recruit a diverse sample of participants in terms of age, race/ethnicity, region of employment, type of employment (academic or professional), and type of expertise (topics & regions), such that the resulting typology reflected the activities of F&B companies across multiple contexts and from multiple perspectives. To recruit a diverse sample, we asked for referrals from colleagues working in various capacities in different regions of the world. We also conducted targeted internet searches on Google and LinkedIn.
Given the extensive CDH research documenting the negative influence of industry on health researche.g.,, 24 participants were not eligible to participate if they reported significant conflicts of interest with the F&B industry (eg, receive research funding from the industry), which the research team assessed prior to their participation.
Procedure
Before participating, potential participants were asked to fill out an intake form using Qualtrics survey software. 25 This form asked participants for written consent and collected information on their gender, race/ethnicity, age, employer, region of employment, employment position, topics of expertise, and the geographic foci of their public health work. We also screened for potential conflicts of interest (COIs) via two open-ended questions: Are you or a close family member/spouse currently receiving financial or non-financial benefits from the F&B Industry, or have you received such benefits in the past five years?; and Does the organization or academic center in which you are employed receive financial or non-financial support from the F&B Industry?. Participants who answered “yes” were asked to describe the benefits received.
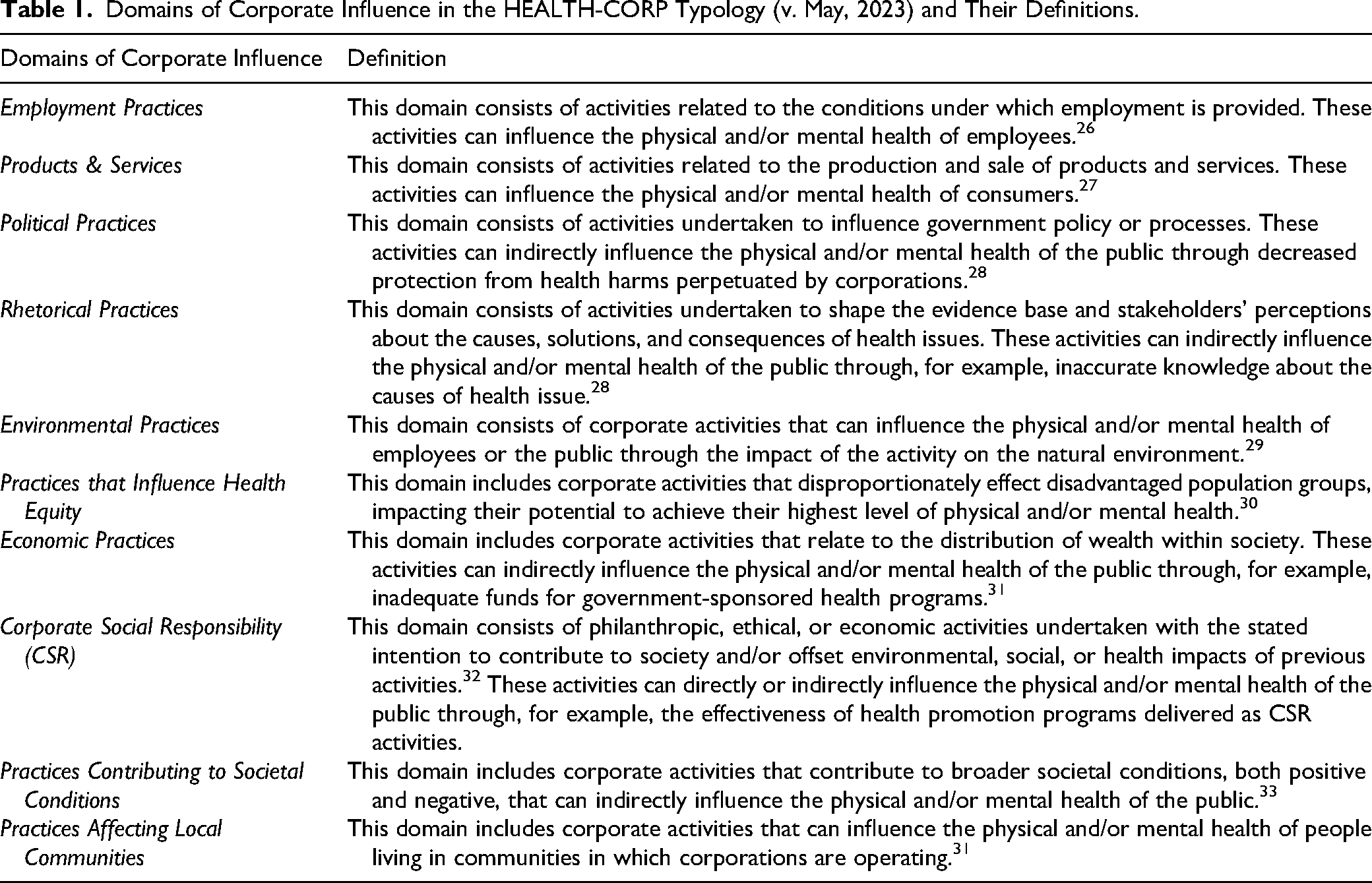
Eligible participants were provided with a draft of the HEALTH-CORP typology. The draft was up to date as of May 2023 and did not reflect later revisions made to the HEALTH-CORP typology during the publication process. The draft typology provided to participants contained 91 corporate activities (eg, use harmful chemical and pesticides, engage in political financing) that can influence population health across industries. These activities were categorized into ten domains of corporate influence (Table 1) (Appendix 1).
Domains of Corporate Influence in the HEALTH-CORP Typology (v. May, 2023) and Their Definitions.
Participants were also provided with an instructional document that described the purpose of the study, our definition of the F&B industry, and four feedback prompts (Table 2). The prompts were designed to elicit feedback that would a) guide us in effectively adapting the HEALTH-CORP typology to the F&B industry, and b) lend insight into the F&B industry practices that should be prioritized for measurement and monitoring. The prompts are similar to those employed by others to identify monitoring priorities for the tobacco industry.34,35
The Four Pieces of Feedback Requested from Participants.
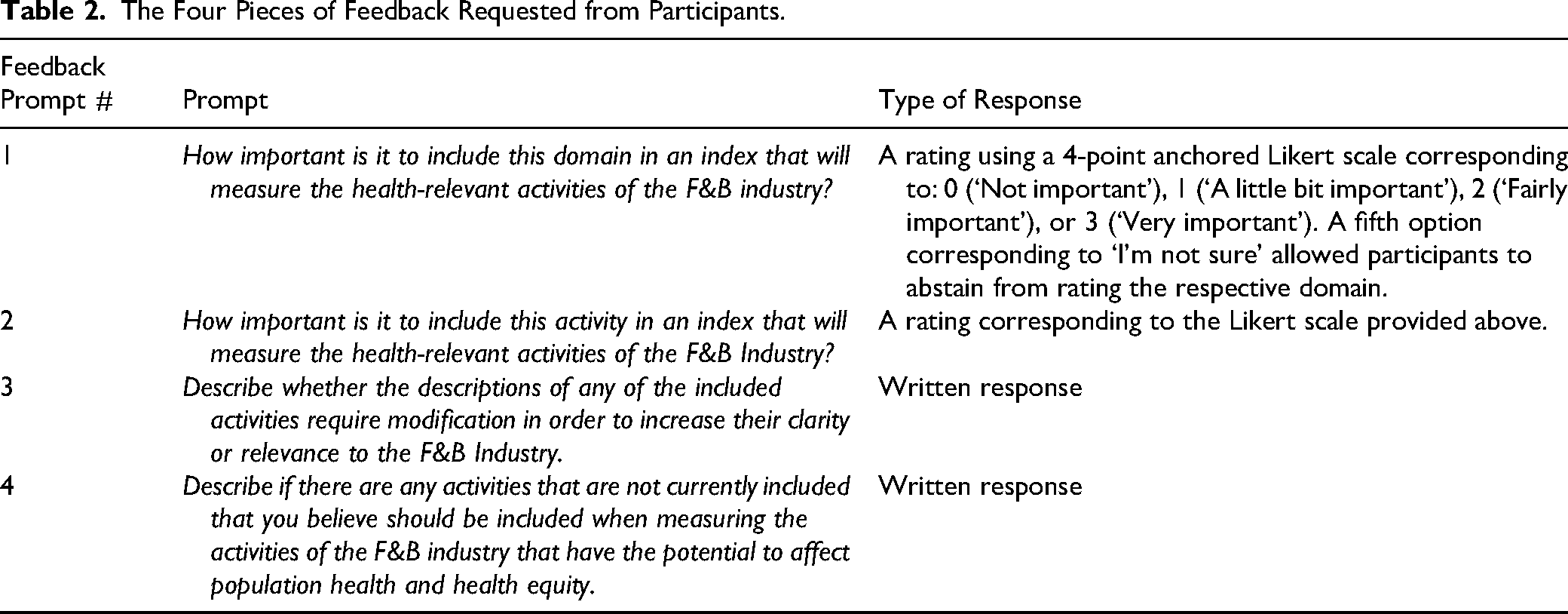
Participants recorded their responses in an individual Microsoft Excel 36 spreadsheet. The instructions were piloted for clarity with two individuals prior to data collection. For Feedback #1, participants were asked to rate each of the ten domains on a scale of 0 (corresponding to “not important” to 3 (corresponding to “very important.”) An additional response category of “I’m not sure” allowed participants to abstain from rating that particular domain (Table 2). For Feedback #2-4, participants were assigned to 2-4 domains based on their areas of expertise as indicated by their professional biographies, academic publications, and responses to the Qualtrics intake form. At least three participants were assigned to each of the ten domains. Participants received $40 USD as compensation for their participation in the task.
Analytic and Adaptation Process
We performed a series of techniques to summarize the Likert data and qualitative feedback received and implement the recommended adaptations. Our analytical strategy was based on recommendations by Beiderbeck and colleagues for the analysis of data from Delphi studies. 37
Quantitative Analysis
First, we computed descriptive statistics for the domain ratings (Feedback Prompt #1) (mean, inter-quartile range) and activity ratings (Feedback Prompt #2) (mean). Ratings in the category “I’m not sure” were excluded from all calculations as non-responses. Activities that received relatively low mean ratings (<2) by the expert participants were excluded from the typology.
Next, we assessed the overall level of agreement between experts (ie, inter-rater reliability) for the domain and activity ratings by computing Gwet's AC2 statistic. AC2 was chosen due to its ability to assess the inter-rater reliability of ordinal data effectively when percent agreement is high. 38 We interpreted the value of AC2 by benchmarking the result to the Landis-Koch scale 39 using the benchmarking method recommended by Gwet. 40 According to this scale, AC2 values between 0.61 and 0.8 indicate ‘substantial’ agreement, whereas values between 0.81 and 1.0 indicate ‘almost perfect’ agreement.
We then further analyzed the domain ratings for instances of dissent between experts. First, we tabulated the frequency of responses in each response category to understand the spread of scores across response categories. We checked for opposing groups of experts by visually inspecting domain response histograms and flagging divergent responses (defined as
Descriptive statistics and Mann-Whitney U tests were computed using IBM SPSS Statistics version 29.01.0 41 and Gwet's AC2 statistic was computed using the R package ‘irrCAC’ 42 in RStudio 43 version 2022.12.0 + 353.
Qualitative Analysis
The first author (RB) iteratively analyzed and implemented the participants’ written feedback in Microsoft Excel 36 based on the principles of qualitative manifest content analysis.44,45 That is, the goal of the analytic process was to extract the explicit meaning of the text (ie, participants’ recommendations) without engaging in significant inference. 45 The process was conducted in three cycles. In the first cycle, responses were reviewed line-by-line to identify and highlight the appropriate modifications recommended for individual activities within each domain. Once all of the recommended modifications had been identified with respect to a specific activity, the activity was revised accordingly. At the same time, activities that were recommended for addition by participants were flagged and a list of these activities was compiled for each domain. Recommended activities were added to the typology if they could be reasonably linked to impacts on human health and to the actions of the F&B industry. This process involved extensive consultation of relevant literature to better understand the nuances of participants’ comments and the potential health implications of recommended activities. The relevant participant was contacted for clarity or elaboration if needed. In the second cycle, the investigator re-reviewed all responses to ensure they had been appropriately captured in the revised typology and addressed any remaining comments. In the third cycle, higher-level insights about the typology were extracted, such as general feedback about the content, tone, or structure of the typology.
Results
Participant Characteristics
Many of the expert participants were employed in academic teaching or research roles (n = 15, 68%) on related topics such as the CDH, the food industry, food systems, nutrition, occupational health, environmental health/sustainability, and health/food policy. Some participants were employed in professional or mixed roles (ie, a combination of professional and academic roles) (n = 7, 32%), such as working for public health organizations focused on obesity reduction and nutrition. Overall, participants most often had expertise in nutrition (n = 15), the socioeconomic determinants of health (n = 14), or marketing, corporate political activity, corporate involvement in health research, and corporate social responsibility practices (ie, CDH topics) (n = 11). Fewer had expertise in environmental health (n = 4) and occupational health or related topics (n = 3). Two participants did not have specific expertise in the F&B industry but were recruited for their expertise in relevant topics (ie, occupational health, environmental health) (Table 3).
Summary of Participant Characteristics (n = 22).
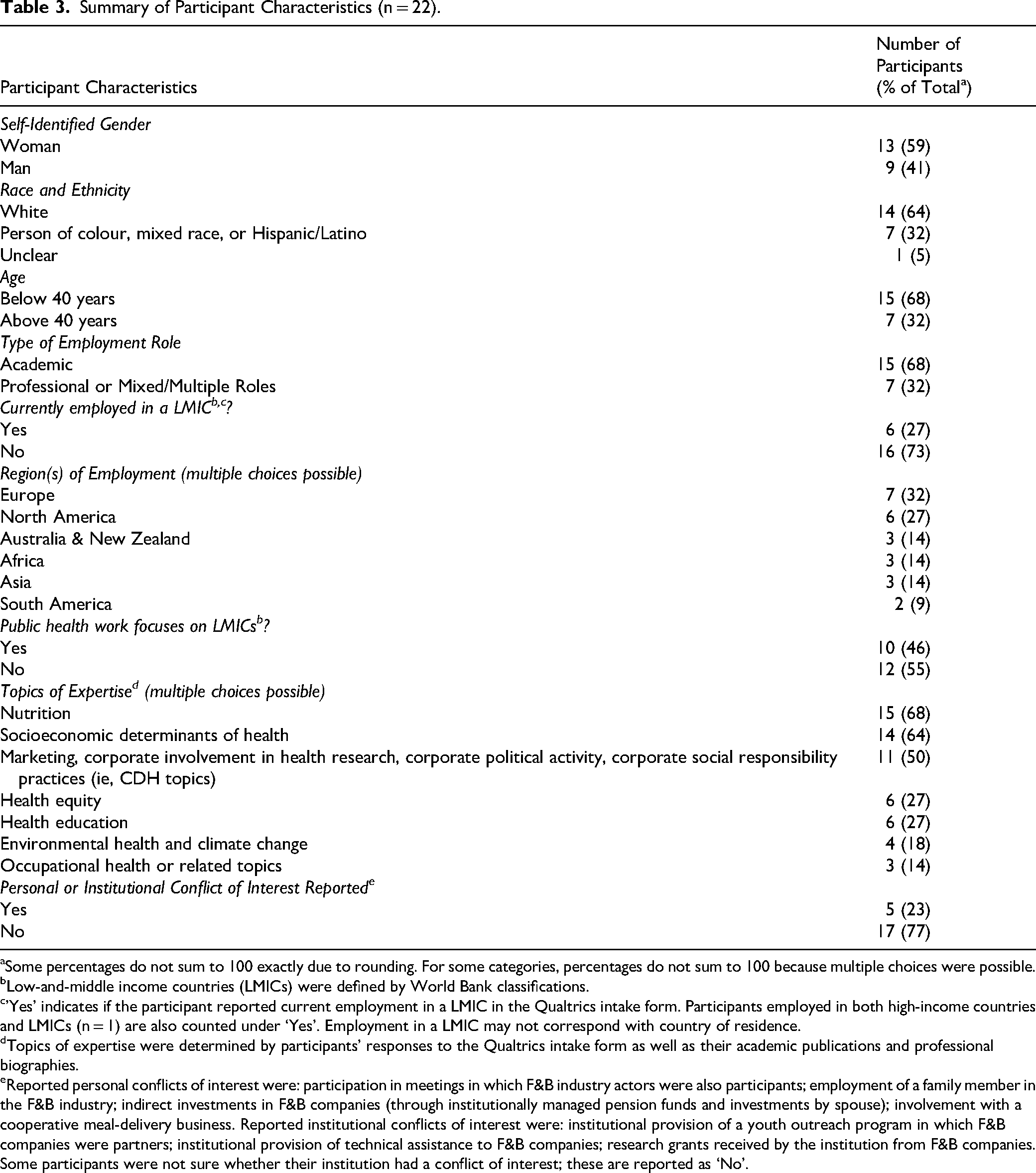
aSome percentages do not sum to 100 exactly due to rounding. For some categories, percentages do not sum to 100 because multiple choices were possible.
Low-and-middle income countries (LMICs) were defined by World Bank classifications.
’Yes’ indicates if the participant reported current employment in a LMIC in the Qualtrics intake form. Participants employed in both high-income countries and LMICs (n = 1) are also counted under ‘Yes’. Employment in a LMIC may not correspond with country of residence.
Topics of expertise were determined by participants’ responses to the Qualtrics intake form as well as their academic publications and professional biographies.
Reported personal conflicts of interest were: participation in meetings in which F&B industry actors were also participants; employment of a family member in the F&B industry; indirect investments in F&B companies (through institutionally managed pension funds and investments by spouse); involvement with a cooperative meal-delivery business. Reported institutional conflicts of interest were: institutional provision of a youth outreach program in which F&B companies were partners; institutional provision of technical assistance to F&B companies; research grants received by the institution from F&B companies. Some participants were not sure whether their institution had a conflict of interest; these are reported as ‘No’.
Participants were employed across six different continents (Table 3), including Africa (n = 3, 14%), Asia (n = 3, 14%) and South America (n = 2, 9%). Sixteen (73%) were employed (or studying) in high-income countries (HICs), while six (27%) were employed in low-and-middle-income countries (LMICs) or a combination of HICs and LMICs. Demographically, just over half of the participants identified as women (13, 59%), approximately one third identified as a person of colour, mixed race, or Hispanic/Latino (n = 7, 32%), and about two thirds of participants were below the age of 40 years (15, 68%).
Four participants were existing colleagues, eleven responded to initial contact from the investigator, and seven were referred by other participants or colleagues. Of the 68 individuals contacted, 22 (32%) agreed to participate and returned the questionnaire. Three individuals filled out the intake form but did not return the questionnaire and two others responded positively to the recruitment message but did not complete an intake form. One participant returned the questionnaire partially incomplete (only two of the domains were rated); this individual's responses were included in the dataset.
Five participants reported a personal or institutional conflict of interest. None of the reported COIs were deemed severe enough (ie, potential to influence participant responses in a way that is favourable to the interest) and therefore these individuals were not excluded from participation (Table 3).
Quantitative Findings
Descriptive Statistics
The domain political practices received the highest mean importance rating (
Descriptive Statistics of the Importance Ratingsa for the Domains of Corporate Influence.
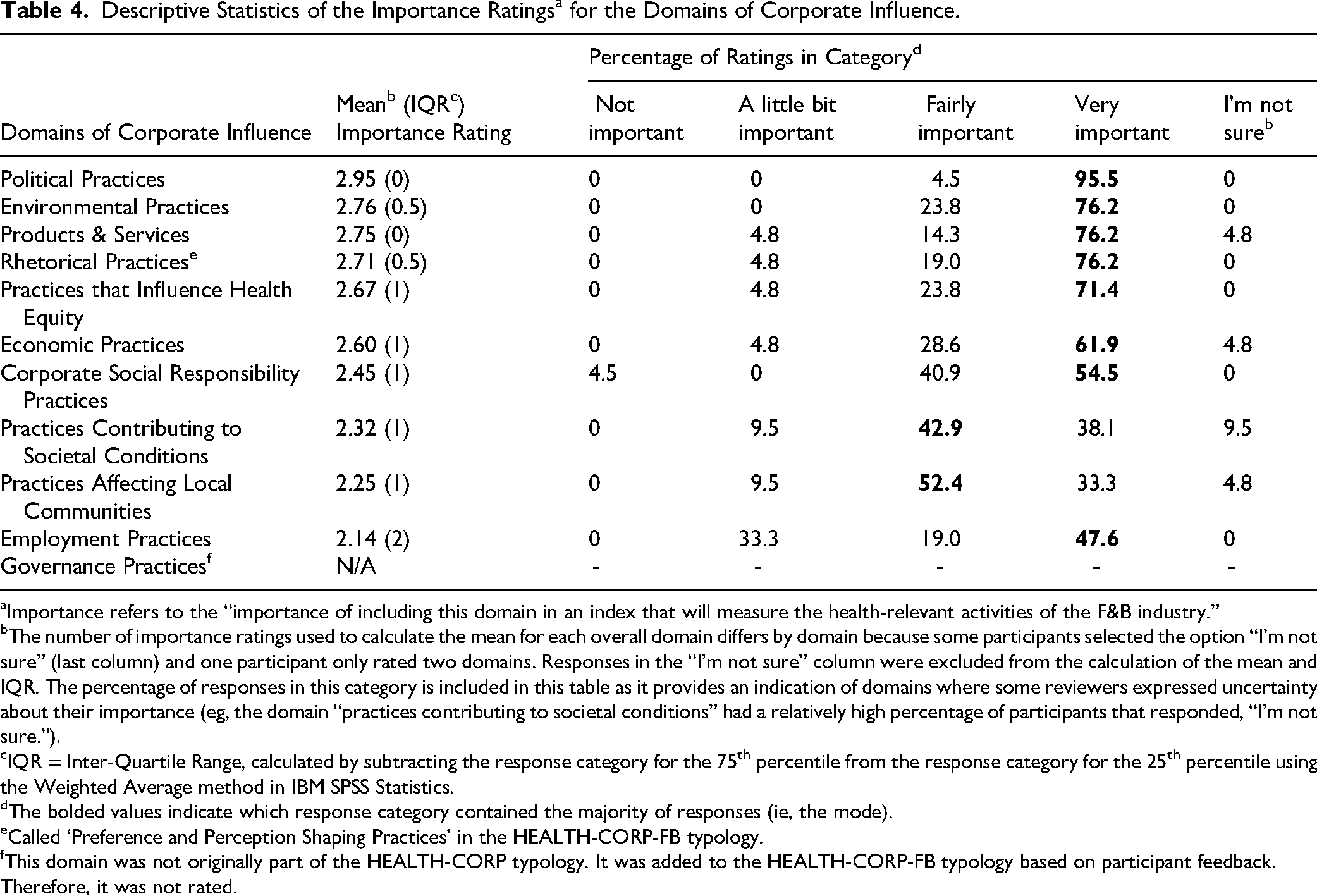
Importance refers to the “importance of including this domain in an index that will measure the health-relevant activities of the F&B industry.”
The number of importance ratings used to calculate the mean for each overall domain differs by domain because some participants selected the option “I’m not sure” (last column) and one participant only rated two domains. Responses in the “I’m not sure” column were excluded from the calculation of the mean and IQR. The percentage of responses in this category is included in this table as it provides an indication of domains where some reviewers expressed uncertainty about their importance (eg, the domain “practices contributing to societal conditions” had a relatively high percentage of participants that responded, “I’m not sure.”).
IQR = Inter-Quartile Range, calculated by subtracting the response category for the 75th percentile from the response category for the 25th percentile using the Weighted Average method in IBM SPSS Statistics.
The bolded values indicate which response category contained the majority of responses (ie, the mode).
Called ‘Preference and Perception Shaping Practices’ in the HEALTH-CORP-FB typology.
This domain was not originally part of the HEALTH-CORP typology. It was added to the HEALTH-CORP-FB typology based on participant feedback. Therefore, it was not rated.
Individual activities that received high mean importance ratings included the healthiness of product offerings (
Agreement, Dissent, and Subgroup Differences
Overall, inter-rater agreement on domain and activity ratings was “substantial” (Domain AC2: 0.80 [95% CI 0.69 0.91]; Activity AC2: 0.76 [95% CI: 0.69 0.82]). However, the distribution of responses differed by domain (Table 4). The domains employment practices and practices contributing to societal conditions received divergent responses, with the former receiving a high frequency of responses at the extremes (Table 4; Appendix 2).
Thus, we conducted stakeholder group analyses on these two domains as well as the domains practices affecting health equity and practices affecting local communities, which we hypothesized would be the most likely to differ between groups of participants. Importance ratings for the domains employment practices and practices affecting local communities were statistically significantly higher (employment practices: U = 71.0, z = 2.195, p = 0.028; practices affecting local communities: U = 70.0, z = 3.188, p = .001) for individuals reporting current employment in an LMIC than those not reporting current employment in a LMIC (mean ranks for employment practices: employed in LMIC = 15.33, n = 6, not employed in LMIC = 9.27, n = 15) (mean ranks for practices affecting local communities: employed in LMIC = 17.0, n = 5, not employed in LMIC = 8.33, n = 15). No other significant differences were found, though some tests were close to significance (Appendix 3).
Qualitative Findings
We received a total of 324 comments (mean: 14.7 comments per participant) in response to Feedback Prompt #3 and 4. Below, we describe the nature of participants’ comments about specific activities and report general feedback that was received about the typology.
Nature of Participants’ Comments
In general, participants’ responses included comments related to increasing the specificity or clarity of the described activities (eg, “It's important to define what (and WHO is defining) you mean by “healthy"…”), expanding their scope (“this could also include global pre-emption (eg, trade, Codex Alimentarius, etc)”), combining or splitting activities that reflected similar or different constructs, respectively (eg, “Block, weaken and delay [health policy] are of course different but probably could be combined…”), or suggesting that certain activities fit better under a different domain (eg, “Doesn't reformulation/product design fit under products and services?”). Many comments related to general modifications to improve the activity descriptions (eg, “You could add ‘and voluntary policies/codes’” [self-regulation]) while others recommended modifications specific to the F&B industry (eg, “Activity 1 description needs to include the [F&B industry's] involvement in providing simple and accurate nutritional quality information”). Some participants contextualized their responses by providing examples in particular contexts, which was particularly useful for understanding corporate involvement in LMICs (eg, “because of comprehensive labour legislation, employees in [LMIC] in a formal work environment in large corporations have guaranteed safety nets… But, it is the abuse of migrant workers in the supply chains (mining, agriculture, etc) where the abuse is significant.”)
General Comments About the Typology
General comments about the typology from participants included one suggestion that activities could be framed more neutrally to capture positive impacts (n = 1). Another participant suggested that the acceptability of certain corporate activities (eg, providing health education in schools) depends on the characteristics of industry involvement (eg, whether the health education materials contained product marketing). One participant indicated that corporate activities (eg, deforestation) should not be confused with associated outcomes (eg, contributions to greenhouse gas emissions). A few participants (n = 3) described how the importance of certain domains and activities were dependent on the strength of relevant institutions (eg, government, civil society), as these actors can mitigate the impact of some corporate activities.
Summary of Adaptations to HEALTH-CORP Typology
Below, we summarize the changes we made to the HEALTH-CORP typology to adapt it to the F&B industry.
Adaptations to Descriptions of Corporate Activities
In total, we added 25 corporate activities (eg, level of product processing) to the previous, cross-industry HEALTH-CORP typology based on participant recommendations and participant-recommended literature (Appendix 4 contains the activities we added). We removed 20 activities for the following reasons: low participant ratings of importance (11 activities), a lack of clarity or differential interpretations of the activity from participants (2), activity is an outcome (6), the activity has an unclear link to human health (1) (Appendix 5 contains the activities we removed). In addition, many activities were combined because they reflected similar constructs. Minor modifications were made to almost all the activities for the purposes of clarity, scope, and relevance. Where possible, we also refined the descriptions of activities for greater neutrality.
Adaptations to Domains of Corporate Influence
We added a new domain called governance practices to capture recommended activities that did not fit in other domains (eg, “structure of the company in terms of how power and economic resources are distributed”). We removed the domain corporate social responsibility practices as relevant activities were consolidated with activities in other domains. Finally, we removed practices affecting local communities, practices influencing societal conditions, and practices affecting health equity and distributed the associated activities across the remaining domains as relevant. We did this to better align the HEALTH-CORP-FB typology with newer drafts of the HEALTH-CORP typology and because the activities in these domains were related to other domains (eg, disproportionate marketing to disadvantaged populations is an element of marketing, which is a preference and perception shaping practice).
The resulting HEALTH-CORP-FB typology consists of 89 activities categorized into seven domains of corporate influence (governance practices, political practices, preference and perception shaping practices, economic practices, employment practices, products and services, and environmental practices) (Appendix 7 provides definitions).
In Figure 1, we organized the domains based on their proximity to health outcomes (ie, distal to proximal), as is done within the HEALTH-CORP typology. 7 Specifically, distal domains (eg, political practices) are those which exert important upstream influences on population health, while proximal domains (eg, products & services) have a more direct influence on population health. The double-headed arrow between the distal and proximal domains indicates the potential for proximal and distal domains to influence one another. For example, the political practices (eg, litigation) of the F&B industry enable the characteristics of the products (eg, portion size) they are able to sell. 47 Likewise, the environmental impact of a product (eg, greenhouse gas emissions) may influence how a company attempts to shape consumer preferences (eg, sustainability marketing of plant-based dairy alternatives), which further influence the company's pursuit of environmentally sustainable practices (eg, efforts to reduce packaging waste). 48
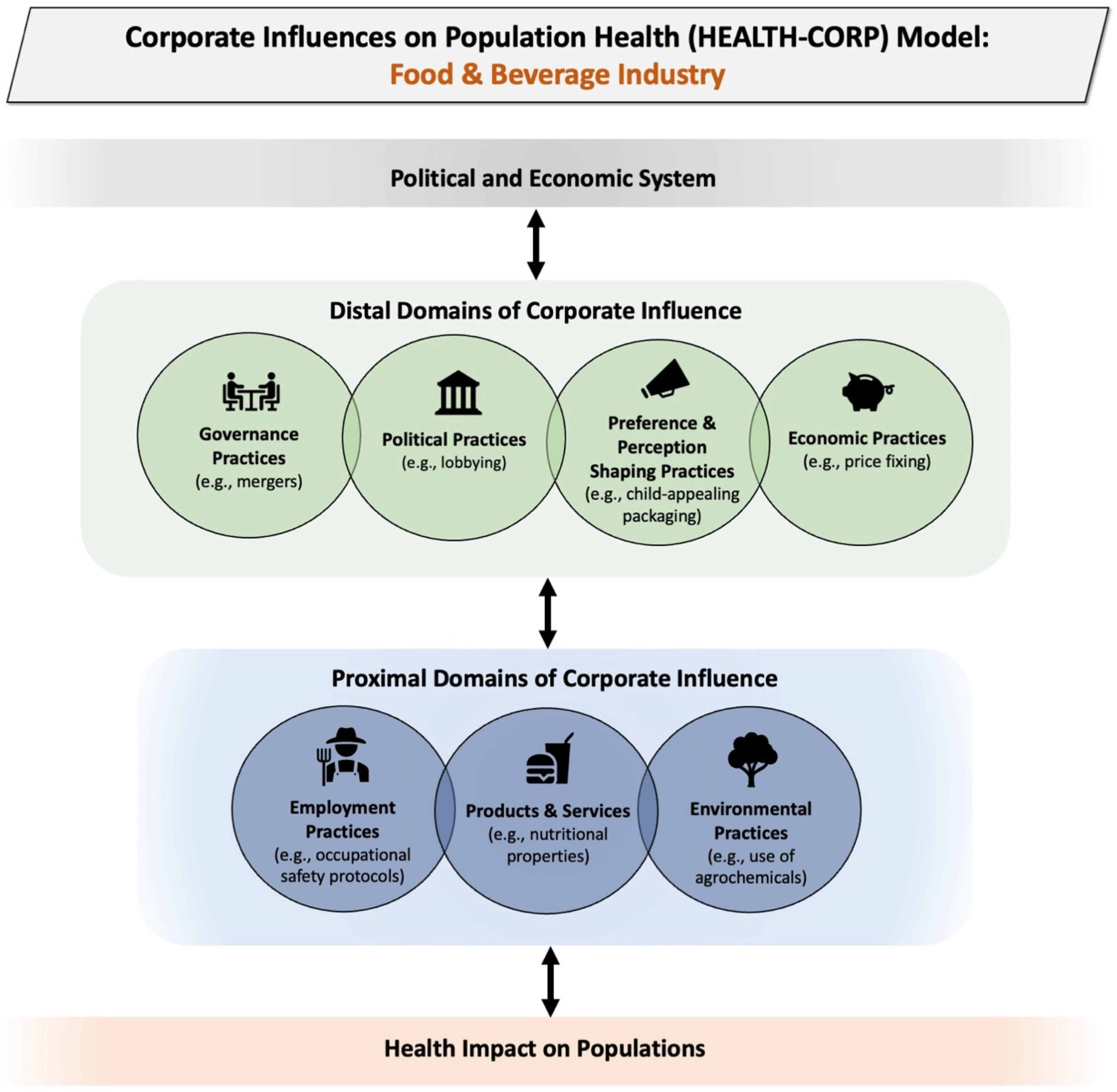
Depiction of the domains of corporate influence in the HEALTH-CORP-FB typology and examples of corporate activities included in each domain. Original figure published on Zenodo. 46
A two-way arrow between the domains and the ‘Health Impact on Populations’ box is intended to portray that corporate activities have an impact on the health of various populations, though these populations also have agency to shape corporate practices (eg, through litigation, boycotts, etc). 7 Similarly, the political and economic system both serves to shape the corporate activities that occur and is simultaneously shaped by these practices. 7
The HEALTH-CORP-FB typology (including the 89 identified corporate activities) is provided under a Creative Commons CC-BY-NC license on Zenodo to facilitate access and use by policy makers, public health units, and non-profit organizations. 46
Discussion
In this article, we report on the process of adapting the cross-industry HEALTH-CORP typology to the F&B industry. The resulting HEALTH-CORP-FB typology consists of 89 activities (eg, child-appealing packaging, profiteering) through which the F&B industry can influence population health and health equity, categorized across seven domains of corporate influence (eg, preference and perception shaping practices, economic practices). As part of this adaptation process, we obtained insight into the practices of this industry that experts identify as important to measure and monitor. We also observed that experts reporting current employment in LMICs assigned higher importance ratings to measuring the domains of employment practices and practices affecting local communities compared to experts that did not report current employment in LMICs, suggesting that context may influence experts’ perceived importance of measuring certain types of corporate practices.
The primary aim of this study was to produce a typology that identifies the diverse range of activities the F&B industry engages in that can influence population health and health equity. In comparison to previous typologies and monitoring initiatives that focus on certain types of practices (eg, nutrition-related practices)8–11 or capture a wider range of practices but without a specific focus on human health,12–14 the HEALTH-CORP-FB typology captures activities that this industry engages in across environmental, occupational, nutritional, and economic dimensions that have implications for population health (Appendix 8 indicates which HEALTH-CORP-FB typology activities are captured by existing frameworks).
Moreover, the broad definition of the F&B industry we employed in the development of the typology may allow it to facilitate an understanding of the practices of the F&B industry as a whole (ie, from field to fork). Our initial definition of the F&B industry focused on the food manufacturing, processing, and retailing sectors and did not include the agricultural sector (ie, food production). However, we received feedback from one participant (an expert in environmental health) suggesting that “we cannot dissociate agricultural practices from industrial practices that use agricultural products” and that excluding environmental practices related to the agricultural sector would preclude a systemic view of the supply chain. Based on this feedback and other participants’ comments about the importance of agricultural practices such as land use, we decided to expand the scope of the typology to include agriculture. As a result of this comprehensive definition of the F&B industry, the HEALTH-CORP-FB typology may encourage a non-reductionist perspective that facilitates consideration of the connections between different industry players and permits examinations of practices that influence health across the entire supply chain.
Other typologies and frameworks have taken different approaches. For example, the Access to Nutrition Initiative (ATNI)'s flagship Global Index seeks to benchmark the actions of large F&B manufacturers specifically. 8 ATNI also has separate indexes dedicated to assessing other sectors, such as the United Kingdom Retailer index, which benchmarks the actions of large food retailers in the United Kingdom. 49 The BIA-Obesity (Business Impact Assessment—Obesity and population-level nutrition) tool developed by the INFORMAS (International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support) monitoring initiative employs a similar strategy.9,50 Though the domains used to assess companies are the same across sub-industries (eg, nutrition labelling), the indicators used for evaluating companies are tailored based on whether the company is classified as a food manufacturer, food retailer, or supermarkets (eg, the placement of unhealthy items on displays is assessed for the supermarket sector). 9 Segmenting by different sectors is useful as it allows for the creation of sector-specific indicators and indicator weights, facilitates direct comparisons between companies in the same sector, and permits the analyst to make sector-specific recommendations. 9 The authors of the BIA-Obesity tool acknowledge, however, that there is significant variation in the characteristics of different companies even within these sectors. 9 Moreover, the existence of large F&B companies with extensive product lines, complex supply chains, and involvement across many sectors 51 may make this type of segmentation challenging and potentially hinder its usefulness as a benchmarking strategy.
The HEALTH-CORP-FB typology may support the advancement of F&B industry monitoring efforts by identifying activities that are not addressed within existing monitoring initiatives. For example, existing frameworks that we reviewed (Appendix 8) do not capture the industry's involvement in acts of profiteering and price fixing which have important implications for food security. 52 These activities may be particularly important to monitor given the economic inflation currently being experienced in many countries and the fact that several major F&B companies have recently been accused or found guilty of engaging in these activities.52,53 Similarly, few of the existing frameworks capture F&B companies’ pursuit of market power via mergers, acquisitions, and joint ventures; these pursuits have implications for the consolidation of the food system and related food security issues. 52 Finally, the frameworks that we reviewed did not capture the extent of processing a food product underwent; ultra-processed foods may have important implications for health via mechanisms that extend beyond their nutrient profile (eg, via the use of additives, ingredient fractionation). 54 The extent of food processing could be captured within existing monitoring initiatives by using the NOVA classification or by modifying the Health Star Rating nutrient profiling system already used by the Access to Nutrition Initiative.55,56 For the purposes of maintaining resource efficiency, indicators measuring these activities could replace indicators corresponding to activities that received low ratings of importance in this study (eg, employee wellness programs) or indicators that are deprioritized based on other evidence such as the magnitude of expected health impact.
The HEALTH-CORP-FB typology may also provide a useful resource for policy makers, civil society actors, and researchers that are interested in understanding the multi-faceted influence of this industry on population health. Prominent approaches to research and policy making such as One Health and the Sustainable Development Goals (SDGs) recognize the complex interdependence between environmental, health, and social issues.56,57 Transdisciplinary approaches may be particularly important for investigating and optimizing the global food system given the complex relationships between nutrition and climate change. 57 The HEALTH-CORP-FB typology may support transdisciplinary policy and research on the food system by illuminating the diverse mechanisms through which the F&B industry influences human health. Similar to Lacy Nichols and colleagues’ guiding questions, 6 the HEALTH-CORP-FB typology could also be used as a tool for policy makers and investors to evaluate F&B companies in order to understand the potential risks and benefits of interacting with these entities for the purposes of informing policy, agenda setting, and decision making. Socially-minded investors could similarly use the HEALTH-CORP-FB typology to consider the health impacts of F&B companies of interest. 6
Furthermore, the HEALTH-CORP-FB typology and model provide some insight into the potential interactions between the social and commercial determinants of health. In general, the relationship between the social and commercial determinants appears complex and has not been well-elucidated.2,58,59 Some of the corporate activities in the HEALTH-CORP-FB typology such as determining the adequacy of employee pay, using agrochemicals, and engaging in profiteering/price fixing likely contribute to social determinants of health (SDH) such as income, environmental exposure, and food security. 60 At the same time, it is also possible that corporate activities are the result of existing social structures.1,58 For example, socioeconomic stratification (ie, “society's categorization of its people into groups based on socioeconomic and other factors” 58 p.119) may create the conditions for and perceived acceptability of harmful corporate activities such as the exploitation of LMIC populations for cheap (and often unsafe) labour. In this way, social and commercial factors may be simultaneously interacting with one another to influence health outcomes. 58 These types of interactions should be further explored in future work.
The secondary aim of this study was to lend insight into the practices of this industry that are potential, expert-informed priorities for measurement and monitoring. The political practices, environmental practices, products and services, and preference and perception shaping practices of this industry received the highest mean importance ratings by experts in our study. The features of F&B products (eg, nutritional composition, accessibility) are monitored by civil society actors (eg, the Access to Nutrition Initiative)8,9 and environmental practices are monitored by both civil society12–14 and the financial industry (eg, Environmental Social Governance (ESG) rating systems). 61 Though these initiatives also seek to monitor the political practices of this industry (eg, lobbying activities, anti-bribery mechanisms), political practices are some of the most difficult activities to systematically track under current disclosure requirements.62,63 For example, although corporations conduct many of their political activities through trade associations, neither party is required to disclose its relationship to the other in the United States (U.S.). 64 Some of the preference and perception shaping practices of this industry, such as corporate involvement in and sponsorship of academic conferences, professional associations, and other key groups (eg, dietician ‘influencers’) are similarly obscure.22,65,66 To facilitate the measurement of these important practices, one solution could be to implement regulations on the disclosure of corporate funding to trade associations, professional associations, and other relevant organizations. This would serve to both increase transparency for stakeholders (eg, civil society organizations, investors) and provide an opportunity for systematic monitoring of these practices and their downstream impacts on health.
Though the aforementioned domains received the highest mean importance ratings in this study, it is important to note that mean ratings for all other domains were still greater than 2 (corresponding to ‘fairly important’). Moreover, the differences in importance ratings for some domains that we found between participants employed in LMICs compared to those who are not supports the idea that the corporate activities that are most important to measure and address likely differ based on the context in which they occur. 31
In this case, the fact that experts reporting employment in LMICs assigned greater importance to the measurement of employment practices and practices affecting local communities than experts not employed in LMICs makes intuitive sense when one considers conditions in LMICs. For instance, LMIC populations are often subjected to dangerous and insecure employment, driven in part by the ability of transnational corporations (including F&B companies) to exploit cheap labour in these contexts in order to maximize profits. 67 Moreover, as a result of weaker regulatory structures and power differentials with transnational corporations (TNCs), communities in LMICs may be more likely than communities in HICs to experience significant impacts from corporate operations, such as strain on the water supply.67,68 Therefore, these activities may still be important priorities for monitoring initiatives, particularly in certain contexts. This initial evidence suggests that future work to identify regional monitoring priorities would be valuable.
It is also important to note that this study relies on the opinions and perspectives of experts (ie, health researchers and public health professionals). These individuals may prioritize certain types of corporate practices (ie, political practices) because these are the types of practices they are often exposed to and/or study. In contrast, practices such as employment practices may be deemed lower priorities for measurement and monitoring by experts because they are not likely to have experienced first-hand the impacts of poor employment practices on health. In the future, follow-up studies could be conducted to elicit the perspectives of local communities, employees, and other key stakeholders in specific regions. It is entirely possible that these groups would prioritize different practices for measurement and monitoring purposes than experts. Likewise, the perspectives of other stakeholders could lend insight into other important activities of the F&B industry that were not identified in this study.
This study utilized an approach involving the adaptation of a cross-industry typology of corporate activities to a specific industry. This type of approach may be a resource-efficient method for investigating the CDH. Research on corporate activities has consistently documented that various industries engage in similar practices (eg, intimidating critics, participating in policy development) that have implications for human health; these practices are referred to as the ‘industry playbook’.27,69,70 Despite the commonalities in practices across industries, most industries likely also have unique practices and features that require the attention of researchers and practitioners. 6 For example, the F&B industry has been observed to engage in practices (eg, creating doubt about product harms) employed by other industries (eg, tobacco). 70 However, it also has unique features, such as the resource-intensive nature of its activities and the provision of goods that are essential for maintaining human life.15,70 Starting with a core set of cross-industry practices which are supplemented and adapted via input from experts and key stakeholders (eg, community members, employees) may be an efficient way to identify the activities of various industries that affect health (eg, social media, health care). CDH researchers have employed similar strategies before; for example, Mialon and colleagues 10 developed a widely-used typology of the corporate political activity of the food industry based on previous work describing the use of these practices by the tobacco industry. 71 These type of approaches may help prevent the duplication of similar efforts and the development of disciplinary siloes. 19 Similarly, defining a core set of cross-industry indicators that are augmented by a smaller set of industry-specific indicators where needed may be an approach to the surveillance of corporate practices that maximizes available resources. This strategy may also lend insight into the common structures (eg, a focus on shareholder wealth maximization) and unique parameters (eg, production of health-harming goods) that dictate an industry's engagement in certain practices. 6
Strengths and Limitations of This Study
The major strengths of this study are that we were able to elicit qualitative and quantitative feedback from a diverse group of public health experts employed in various roles across six different continents to adapt the HEALTH-CORP typology to the F&B industry.
Our study also has limitations. The first is that feasibility issues prevented us from being able to engage participants in multiple rounds of feedback and achieve consensus on the activities that should be added or removed. Though we recruited a fairly diverse sample of experts, our study may have been improved with greater representation from certain types of participants (ie, those with environmental and occupational expertise and employed in LMICs). The extent to which the importance ratings obtained in this study are generalizable to other groups of relevant experts is unclear; the findings should be confirmed in larger samples. Likewise, the findings from this study suggest that socioeconomic context may be an important determinant of monitoring priorities. Our study was not adequately powered to detect differences in monitoring priorities within specific regions; however, this is an important area for future inquiry.
We did not seek participation from representatives of large F&B companies to avoid the potential for conflicts of interest to influence the development of the typology. As previously mentioned, we also did not include the perspectives of community members, employees, or other key stakeholders. Inclusion of these actors in future samples may yield new insights into corporate activities, their drivers, and their implications. It may also allow us to identify more ways in which F&B corporations contribute positively to population health, as the current iteration of the typology is focused primarily on negative impacts. Any attempt to include the perspectives of industry actors, however, should be done extremely carefully to avoid the potential for the typology to be revised in a way that serves industry interests over population health needs. 72
One of the strengths of the HEALTH-CORP-FB typology is its breadth. However, it was outside of the scope of this study to evaluate the strength of the relationship between each of the activities included in the HEALTH-CORP-FB typology and associated health outcomes. Moreover, increased breadth may come at the expense of depth for some topics. As discussed earlier, the broad definition of the F&B industry used in the development of the typology may not allow for tailored analyses of specific players (eg, retail stores) that are facilitated by other frameworks.8,9
Conclusion
In conclusion, the HEALTH-CORP-FB typology is a novel framework designed to identify the diverse set of activities through which F&B companies can influence population health and health equity. The findings from this study provide initial insight into key corporate practices that are prioritized for measurement and monitoring by health experts. The HEALTH-CORP-FB typology and the findings from this study may also support public health policy, practice, and resource-efficient monitoring of F&B industry practices that influence population health.
Supplemental Material
sj-docx-1-joh-10.1177_27551938261418656 - Supplemental material for Food & Beverage Industry Activities That Influence Population Health: Development of the HEALTH-CORP-FB Typology
Supplemental material, sj-docx-1-joh-10.1177_27551938261418656 for Food & Beverage Industry Activities That Influence Population Health: Development of the HEALTH-CORP-FB Typology by Raquel Burgess, Nicholas Freudenberg, Lawrence Grierson, Tanja Srebotnjak and Yusuf Ransome in International Journal of Social Determinants of Health and Health Services
Footnotes
Acknowledgments:
We would like to acknowledge Savas Kim, Kenneth Chen, and Naisha Dharia (McMaster University) for their assistance with extracting the information represented in Appendix 7. Naisha Dharia also provided assistance with collating participant responses. We would also like to thank each of the participants for their time and insights and acknowledge those who agreed to be named: Nabin Adhikari (Tribhuvan University), Mavra Ahmed (University of Toronto), Benjamin Allès (Sorbonne Paris Nord University and University of Paris), Adam Bertscher (University of Bath), Caroline Cerny (Bite Back), Yanaina Chavez-Ugalde (University of Cambridge), Eric Crosbie (University of Nevada Reno), Josefa Maria Fellegger Garzillo (University of São Paulo), Jenn Lacy-Nichols (University of Melbourne), Jane Martin (Food for Health Alliance), Elise Pauzé (University of Ottawa), Joelle Robinson-Oghogho (John Hopkins University), Paraskevi Seferidi (Imperial College London), and Namuna Shrestha (Dhulikhel Hospital-Kathmandu University Hospital). Yanaina Chavez-Ugalde also provided additional useful insights to inform the adaptation of the typology beyond her direct participation in the study.
Ethical Approval
This study was reviewed and received an exemption determination from the Yale Human Research Protection Program Institutional Review Boards (#2000034281).
Consent to Participate
Participants provided electronic consent to participate prior to participation.
Consent for Publication
Not applicable.
Author Contributions
Raquel Burgess: conceptualization, methodology, formal analysis, investigation, data curation, funding acquisition, original draft preparation, reviewing and editing. Nicholas Freudenberg: conceptualization, methodology, reviewing and editing. Lawrence Grierson: conceptualization, methodology, reviewing and editing. Tanja Srebotnjak: methodology, reviewing and editing. Yusuf Ransome: conceptualization, methodology, supervision, reviewing and editing.
Funding
Participant compensation was covered by a Seed Grant from the Yale Women Faculty Forum, awarded to RB. This study is part of RB's dissertation research, which was supported by a Canadian Institutes of Health Research (CIHR) Doctoral Foreign Study award. RB was also supported by a Scholar Award from the International Chapter of the Philanthropic Educational Organization (P.E.O.). The Yale Women Faculty Forum, P.E.O., and the Yale School of Public Health supported travel expenses for RB to present this research at Public Health 2025 (annual meeting of the Canadian Public Health Association) in April 2024. The funders did not plan any role in the study design, data collection and analysis, decision to publish, or preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Domain importance ratings are available on Open Science Framework (https://doi.org/10.17605/OSF.IO/T2MY7). The data has been de-identified to protect the confidentiality of the participants. The HEALTH-CORP-FB typology is provided under a CC-BY-NC license on Zenodo (https://doi.org/10.5281/zenodo.11164913) to facilitate use for public health policy and practice.
Supplemental Material
Supplemental material for this article is available online.